Improving Self Care with Allergy New Zealand and ASCIA ... kylie morse... · Improving Self Care...
21
10/1/2012 1 Improving Self Care with Allergy New Zealand and ASCIA Resources Dr Kylie Morse, Wellington GP Allergy NZ Board Member Associate Member ASCIA 1 • Allergy New Zealand for providing the depth of information and support that many families need to manage allergies, including mine • My children, who have provided me with the impetus to improve allergy education, and not let multiple allergies affect their development • ASCIA for use of their slides and resources Acknowledgements 2
Transcript of Improving Self Care with Allergy New Zealand and ASCIA ... kylie morse... · Improving Self Care...
10/1/2012
1
Improving Self Care
with Allergy New Zealand
and ASCIA Resources
Dr Kylie Morse, Wellington GP
Allergy NZ Board Member
Associate Member ASCIA
1
• Allergy New Zealand for providing the depth of information
and support that many families need to manage allergies,
including mine
• My children, who have provided me with the impetus to
improve allergy education, and not let multiple allergies affect
their development
• ASCIA for use of their slides and resources
Acknowledgements
2

10/1/2012
2
• What patients want to know:
• What is allergy?
• Why is it increasing and changing?
• How to manage anaphylaxis – immediate and long
term
• Who would benefit from adrenaline auto-injectors?
• Action plans
• The role of the GP
• Further information, resources and training
Overview
3
Mechanism of IgE mediated allergy
4

10/1/2012
3
Signs and symptoms of mild or moderate allergic
reactions
• Swelling of lips, face, eyes
• Hives or welts
• Tingling mouth
• Abdominal pain, vomiting (these may be signs of anaphylaxis especially in insect allergy)
5
Any acute onset of hypotension or bronchospasm or upper airway obstruction where anaphylaxis is considered possible, even if typical skin features are not present
OR
Any acute onset illness with typical skin features (urticarial rash or erythema/flushing, and/or angioedema), PLUS involvement of respiratory and/or cardiovascular and/or persistent severe gastrointestinal symptoms
Ref: ASCIA 2010
What is anaphylaxis?
6

10/1/2012
4
Cutaneous symptoms
Urticaria, erythema and angioedema may be transient,
subtle and easily overlooked
In 1 out of 6 fatal food induced
anaphylaxis cases, severe
cardiovascular symptoms
developed without skin or
respiratory symptoms
Ref: Sampson et al. 1992; Brown, Mullins, Gold. 2006 7
Food allergy
Whilst 90% of food allergic reactions are caused by allergic reactions to
these foods, any food can cause an allergic reaction
8
10/1/2012
5
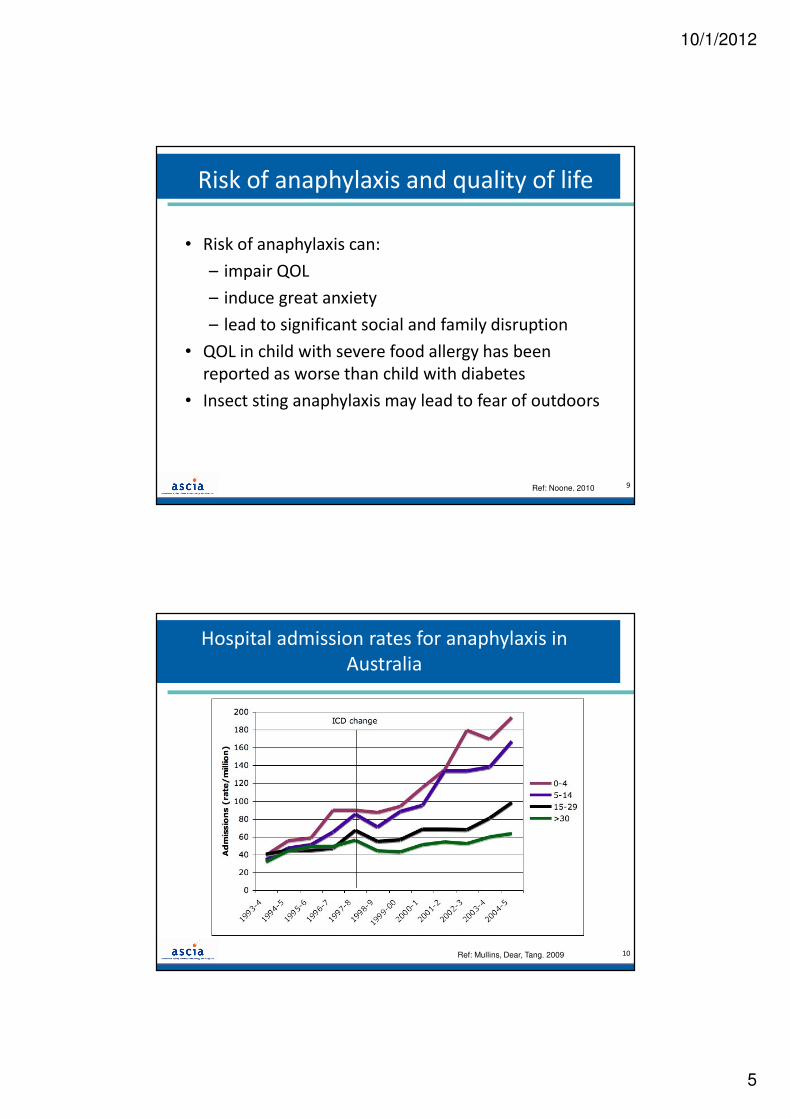
Risk of anaphylaxis and quality of life
• Risk of anaphylaxis can:
– impair QOL
– induce great anxiety
– lead to significant social and family disruption
• QOL in child with severe food allergy has been
reported as worse than child with diabetes
• Insect sting anaphylaxis may lead to fear of outdoors
Ref: Noone. 2010 9
Hospital admission rates for anaphylaxis in
Australia
Ref: Mullins, Dear, Tang. 2009 10

10/1/2012
6
11
Why the rise in food allergy?
Proposed explanations include:
• Hygiene hypothesis
• Delayed versus early
introduction of allergenic foods
• Methods of food processing
• Development of allergy to food
by skin exposure (especially in
severe eczema)
This area requires further research
Fatal anaphylaxis - associations
• Asthma
• Delayed or no administration of adrenaline
• Age:
– Teenagers and young adults (food allergy)
– Adults (insect and drug allergy)
• Upright posture during anaphylaxis
• Food allergic individuals eating away from home
• Initial misdiagnosis
• Systemic mastocytosis
Previous mild/moderate reactions may not rule out subsequent severe or fatal reactions
Ref: Bock. 2010; Liew, Williamson, Tang. 2008; Bock. 2007; Pumphrey. 2003; Bock. 2001 12

10/1/2012
7
Cause of Allergic ReactionPercent
Peanut 60% 0.190968 37
Tree nut 27% 0.087742 17
Fish 2% 0.005161 1
Milk 8% 0.025806 5
Shrimp 3% 2
62
0% 10% 20% 30% 40% 50% 60% 70%
Peanut
Tree nut
Fish
Milk
Shrimp
Percent of Cases
Cause of Fatal Anaphylaxis
Common causes of fatal food anaphylaxis
Ref: Pumphrey, Garland. 2007 13
Shrimp (prawn)
Key information that assists diagnosis:
• Nature of symptoms
• Exposure to potential triggers
• Timing of reaction in relation to exposure
• Response to treatment
Clinical history
14
10/1/2012
8
Allergy testing: use and limitations
Use:
• Useful to confirm clinical suspicions
• Single allergen testing; avoid mixes
Limitations:
• Positive test alone does not = allergy
• Does not correlate well with severity
• Not available for all triggers (e.g. ticks, NSAID, most
antibiotics, anaesthetics)
• SPT – false positives and negatives may occur
15
Allergic reactions may occur on the first
known exposure
Sensitisation may occur through:
• Oral exposure in other foods
• Cutaneous exposure - creams containing unrefined
nut oils, direct contact of food to skin especially in
children with eczema
16

10/1/2012
9
Serum tryptase
Ref: Simons, Camargo. 2010; Yunginger, Squillace et al. 1989; Sampson, Menderson et al. 1992.
• Serum tryptase should be measured within 4 hours after anaphylaxis
• Serum tryptase is often normal after food anaphylaxis
17
Action for anaphylaxis in clinical settings
• Remove allergen (if still present)
• Call for assistance
• Lay patient flat (if breathing difficult allow to sit but not
stand or walk)
• Give IMI ADRENALINE without delay– 1:1000 IMI into mid lateral thigh
– Repeat every 5 minutes as needed
– If multiple doses required or a severe reaction consider adrenaline
infusion if skills and equipment available
• Call ambulance to transport patient,
state “anaphylaxis need adrenaline”
18

10/1/2012
10
Is it anaphylaxis or asthma?
If patient is known to be at risk of anaphylaxis and is
unsure if they are experiencing anaphylaxis or asthma
follow their ASCIA Action Plan for Anaphylaxis:
• Give adrenaline autoinjector first
• Then give asthma reliever medication
• Call ambulance
• Continue asthma first aid
19
Why is adrenaline effective?
• Inhibits the release of inflammatory mediators
• Reverses the physiological effect of mediators by:
– Reducing airway mucosal oedema
– Inducing bronchodilatation
– Inducing vasoconstriction (thus increasing HR & BP)
– Increasing strength of cardiac contraction
Lasts ~ 15-20 minutes; repeated doses may be needed after 5 minutes if no response
Ref: Tole, Lieberman. 2007 20

10/1/2012
11
IMI into outer mid thigh is recommended
• IMI into mid-anterolateral thigh provides rapid plasma
and tissue concentrations of adrenaline
• IM formulation of adrenaline contains 1 mg/mL and may
also be labelled as 1:1000 or 0.1%
• If using adrenaline ampoules ensure appropriate needle
length for IMI
21
Adrenaline ampoule dosages
Dose 0.01 mg per kilogram (up to 0.5 mg per dose)
Source: Adapted from the Australian Immunisation Handbook 9th Edition22
10/1/2012
12
Adrenaline - possible adverse effects
• Well tolerated in children as well as adults
• Transient adverse effects include anxiety, fear, restlessness, headache, dizziness, palpitations, pallor and tremor
IV boluses of adrenaline are NOT recommended
23
Medical observation
• Relapse, protracted and/or biphasic reactions may occur
• Observe patient for at least 4 hours after last dose of adrenaline
• Observe overnight if patient:– had a severe reaction (hypotension or hypoxia) or– required repeated doses of adrenaline or – has a history of asthma or biphasic/protracted
anaphylaxis or– has other concomitant illness or– lives alone or is remote from medical care
24
10/1/2012
13
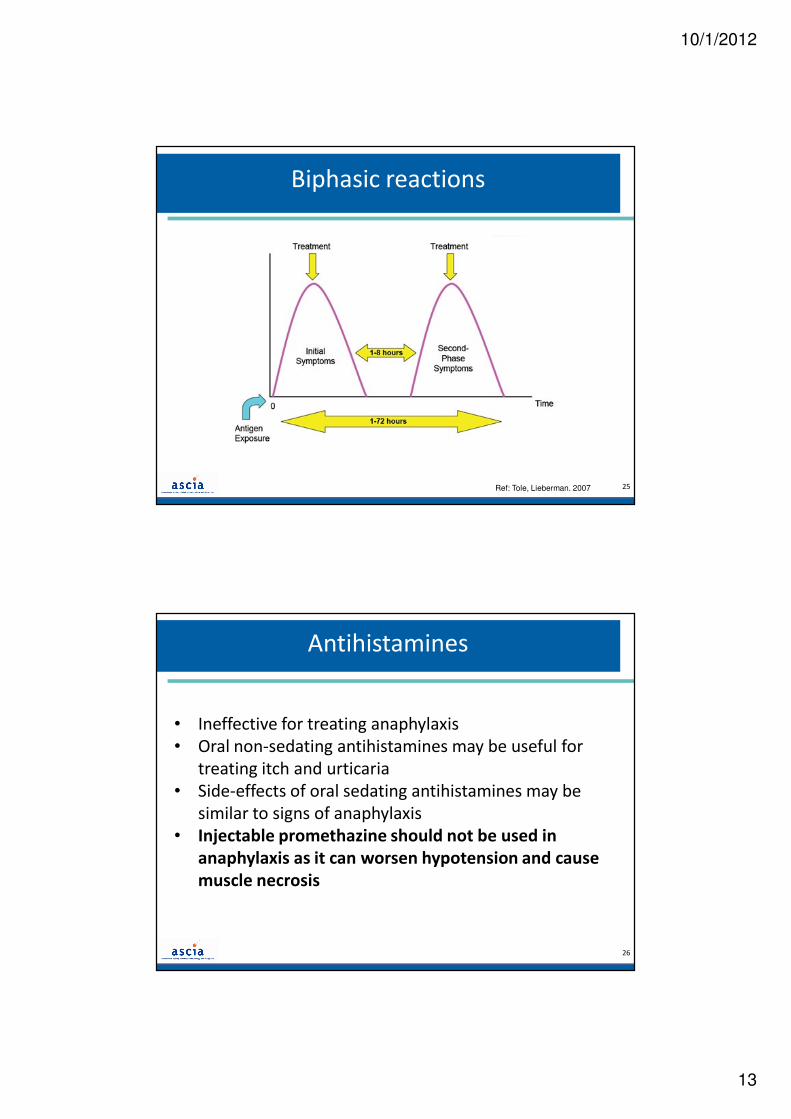
Biphasic reactions
Ref: Tole, Lieberman. 2007 25
Antihistamines
• Ineffective for treating anaphylaxis
• Oral non-sedating antihistamines may be useful for
treating itch and urticaria
• Side-effects of oral sedating antihistamines may be
similar to signs of anaphylaxis
• Injectable promethazine should not be used in
anaphylaxis as it can worsen hypotension and cause
muscle necrosis
26

10/1/2012
14
Adrenaline autoinjectors...
• are spring-loaded automatic injector devices
• contain a single pre-measured fixed dose of adrenaline
• are designed for self-injection or bystander use
• should be injected into the outer mid-thigh muscle
• can be administered through a single layer of clothing
• should be stored in easily accessible, unlocked location with ASCIA Action Plan for Anaphylaxis
27
How to give EpiPen with orange needle end and blue safety
release
28

10/1/2012
15
How to give Anapen or Anapen Junior
29
Availability of adrenaline autoinjectors to patients
EpiPen and Anapen:
• Are not currently reimbursed by Pharmac in NZ
• are available without a prescription at full retail price
• are available on PBS authority prescription in Australia
• have different administration techniques and are not
brand substitutable
30
10/1/2012
16
Guidelines for prescribing an adrenaline autoinjector
Always recommended if…
• History of anaphylaxis (and continued risk)
• These patients should be referred to a clinical immunology/allergy
specialist
May be recommended if…
• History of a generalised allergic reaction and one or more risk factors:
– Asthma
– Age (children >5 yrs, adolescents, young adults)
– Specific allergic triggers
– Co-morbidity (e.g. ischaemic heart disease)
– Geographical remoteness from emergency medical care
• These patients should be referred to a clinical immunology/allergy
specialist31
ASCIA Action Plans:
Should be:
• provided to each patient who is prescribed an adrenaline autoinjector
• completed and signed by the doctor
• reviewed annually or if patient’s medical condition changes
• stored with adrenaline autoinjector
Can be printed in colour from ASCIA or Allergy New Zealand websites or colour hard copies ordered from ASCIA
Advise patient to keep their Action Plan with their autoinjector and provide a copy to their school, childcare or workplace
32
10/1/2012
17
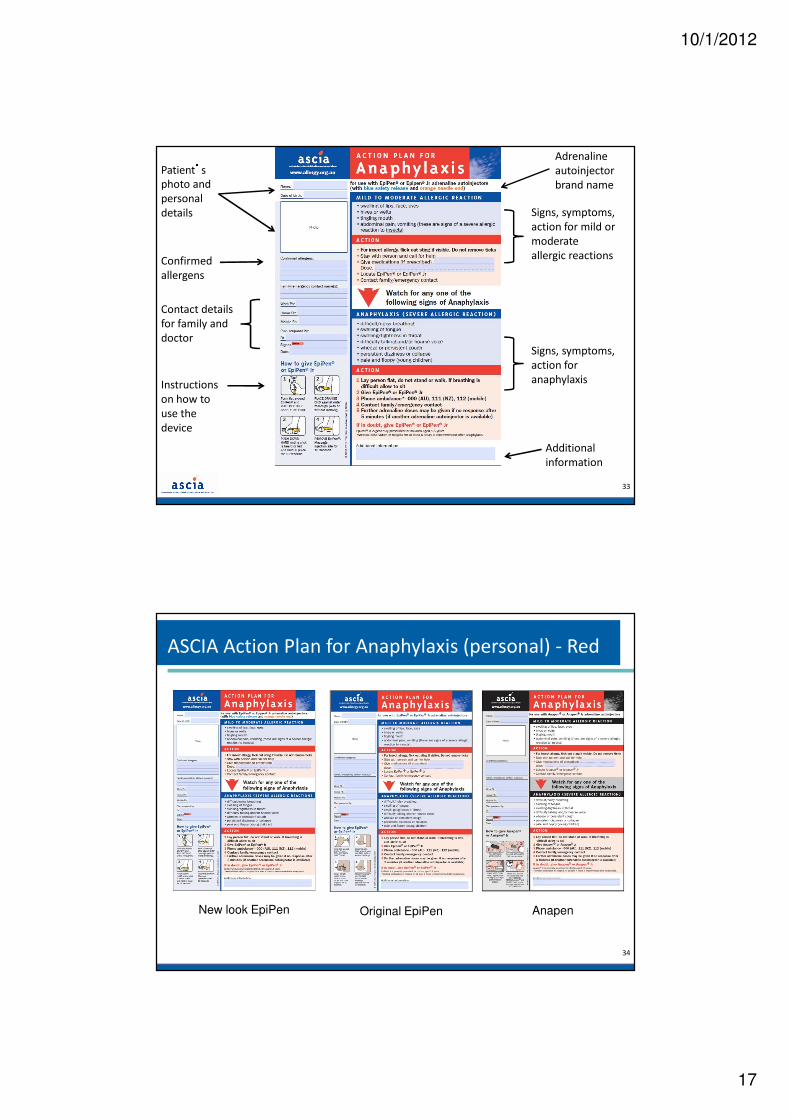
Patient’s
photo and
personal
details
Confirmed
allergens
Contact details
for family and
doctor
Adrenaline
autoinjector
brand name
Signs, symptoms,
action for mild or
moderate
allergic reactions
Instructions
on how to
use the
device
Signs, symptoms,
action for
anaphylaxis
Additional
information
33
ASCIA Action Plan for Anaphylaxis (personal) - Red
Original EpiPenNew look EpiPen Anapen
34

10/1/2012
18
Provided to
patients with
known mild to
moderate allergies
who have NOT
been prescribed an
adrenaline
autoinjector
ASCIA Action Plan for Allergic Reactions - Green
35
• Provides
documentation for
patient to carry
adrenaline
autoinjector in
aircraft cabin
• Can be printed from
the ASCIA website
ASCIA Travel Plan for Anaphylaxis
36

10/1/2012
19
Role of GP after INITIAL allergic
reaction/anaphylaxis
• Provide specialist referral
• Prescribe initial adrenaline autoinjector if required• Provide ASCIA Action Plan
• Educate patient/carers in recognition/management of reactions• Advise on appropriate allergen avoidance measures
• Teach patient/carer how to use adrenaline autoinjector using trainer
– Demonstration results in 5-fold increase in ability to use the device
– Training must be brand specific as the devices have different methods of administration
• Educate patient on carrying and storage of adrenaline autoinjector• Review and optimise asthma management
• Provide resource materials
37
• Be aware of NZ Allergy Guidelines for Schools 2011. All school and ECE
children should have an appropriate action plan completed and education
around this
• Ensure yearly follow up, update Action plans, medications, education, +/-
allergy tests (to assess if they have grown out of some of the allergies)
• Look for and treat other atopic co-morbidities
-optimising allergic rhinitis Mx improves asthma
-treating eczema and improving the skin barrier function reduces
sensitisations
- improves QOL: “no one would hold my hand”, nasal congestion
• Be aware of immune dysregulation: offer varicella vaccination, be alert for
eczema herpeticum, recurrent staph and widespread molluscum
• Support family teaching how to be safe but not anxious, letting go.
Encourage them to join Allergy New Zealand for support and education.
Role of GP in long term management
38

10/1/2012
20
Eczema and allergic rhinitis plans
39
Further Information – Allergy NZ
41

10/1/2012
21
Further information - ASCIA
Australasian Society of Clinical Immunology and Allergy
The peak professional body of allergy and clinical immunology
specialists in Australia and New Zealand
ASCIA website www.allergy.org.au
Includes:
• Anaphylaxis resources (ASCIA Action Plans, Travel Plans,
FAQ, Guidelines), other Action Plans, Immunotherapy
treatment plans
• ASCIA education resources and patient information
(including allergen avoidance strategies)
• ASCIA anaphylaxis, food allergy and allergic rhinitis and immunotherapy e-training (CME being applied for)
39
• Goodfellow Allergy Toolkit under development
• NZ Paediatric Allergy Management guidelines
• Graduate Certificate in Allergic Diseases via
University of Western Sydney for GPs and
Paediatricians2 year mainly online part time course with a practical component in
second year working with Immunologists in NZ
• Professional Certificate of Allergy Nursing,
University of south Australia 16 week online course and 1 week clinical
Further Resources and Training
42