Robyn Woidtke MSN,RN, RPSGT,CCP,CCSH OCTOBER 24 KASP 2014 Sleep in the Hospitalized Patient 1.

Improving Safe Sleep Practices for Hospitalized InfantsKristin A. Shadman, MD, a Ellen R. Wald, MD, a Windy Smith, RN, b Ryan J. Coller, MD, MPHa
aDepartment of Pediatrics, University of Wisconsin School
of Medicine and Public Health, Madison, Wisconsin; and bAmerican Family Children’s Hospital, Madison, Wisconsin
Dr Shadman conceptualized and designed the
study, designed the data collection instruments,
participated in the analysis and interpretation of
the data, and drafted the initial manuscript; Dr Wald
conceptualized and designed the study and critically
reviewed the manuscript; Ms Smith coordinated
and supervised data collection and critically
reviewed the manuscript; Dr Coller performed the
analysis, participated in the interpretation of the
data, and reviewed and revised the manuscript;
and all authors approved the fi nal manuscript as
submitted.
DOI: 10.1542/peds.2015-4441
Accepted for publication Apr 29, 2016
Address correspondence to Kristin A. Shadman, MD,
Department of Pediatrics, University of Wisconsin,
H4/468 CSC, 600 Highland Ave, Madison, WI 53972.
E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online,
1098-4275).
Copyright © 2016 by the American Academy of
Pediatrics
FINANCIAL DISCLOSURE: The authors have
indicated they have no fi nancial relationships
relevant to this article to disclose.
FUNDING: No external funding.
POTENTIAL CONFLICT OF INTEREST: The authors
have indicated they have no potential confl icts of
interest to disclose.
Despite declines in sudden infant
death syndrome (SIDS) during the
Back to Sleep Campaign through
2001, additional reductions have
not occurred, and SIDS remains the
leading cause of death in infants
beyond the neonatal period in the
United States. 1 In response to this
plateau, the American Academy
of Pediatrics (AAP) has expanded
recommendations for SIDS prevention
and addressed safe sleep practice
(SSP) in newborn nurseries and
NICUs. 2 Although >20% of all pediatric
discharges are among children <1
year of age, 3 SSP recommendations
in general inpatient settings have
not been established, and adherence
for hospitalized infants is not well
studied.
Hospitalizations offer unique
opportunities to provide education
abstractBACKGROUND AND OBJECTIVES: Adherence to the American Academy of Pediatrics
safe sleep practice (SSP) recommendations among hospitalized infants is
unknown, but is assumed to be low. This quality improvement study aimed
to increase adherence to SSPs for infants admitted to a children’s hospital
general care unit between October 2013 and December 2014.
METHODS: After development of a hospital policy and redesign of room setup
processes, a multidisciplinary team developed intervention strategies
based on root cause analysis and implemented changes using iterative
Plan–Do–Study–Act cycles. Nurse knowledge was assessed before and after
education. SSPs were measured continuously with room audits during
sleeping episodes. Statistical process control and run charts identified
improvements and sustainability in hospital SSPs. Caregiver home practices
after discharge were assessed via structured questionnaires before and
after intervention.
RESULTS: Nursing knowledge of SSPs increased significantly for each item (P ≤
.001) except avoidance of bed sharing. Audits were completed for 316 sleep
episodes. Simultaneous adherence to all SSP recommendations improved
significantly from 0% to 26.9% after intervention. Significant improvements
were noted in individual practices, including maintaining a flat, empty
crib, with an appropriately bundled infant. The largest gains were noted in
the proportion of empty cribs (from 3.4% to 60.3% after intervention, P <
.001). Improvements in caregiver home practices after discharge were not
statistically significant.
CONCLUSIONS: Sustained improvements in hospital SSPs were achieved
through this quality improvement initiative, with opportunity for continued
improvement. Nurse knowledge increased during the intervention. It is
uncertain whether these findings translate to changes in caregiver home
practices after discharge.
QUALITY REPORTPEDIATRICS Volume 138 , number 3 , September 2016 :e 20154441
To cite: Shadman KA, Wald ER, Smith W, et al.
Improving Safe Sleep Practices for Hospitalized
Infants. Pediatrics. 2016;138(3):e20154441
by guest on January 10, 2021www.aappublications.org/newsDownloaded from

SHADMAN et al
and role modeling to families
and providers. Studies have
demonstrated that supine position
and bed sharing at home are both
positively and negatively influenced
by SSP modeled in the newborn
nursery 4, 5 and sleep advice provided
by health care professionals. 6 –8
Given this influence of SSP modeling
from the newborn nursery, we
were concerned about potentially
negative influence of unsafe sleep
practices modeled in inpatient
settings. Parents of hospitalized
infants encounter unsafe practices,
such as leaving personal care items
in the crib, elevating the head of
the bed (HOB), or using towel rolls
to position the child. Despite the
risk of SIDS associated with such
practices 9 –13 our experience suggests
they commonly occur in inpatient
settings. This practice counters a
professional responsibility to follow
established guidelines intended to
reduce preventable sleep-related
deaths regardless of the setting. 4, 14, 15
Previous quality improvement work
in other settings demonstrated
the value of various approaches to
improving SSP: providing nursing
education, using visual cues for
families and providers, auditing
cribs, and surveying parent-reported
practices. 14, 16 Such strategies were
therefore anticipated to provide
a framework on which additional
improvement activities might be
added.
To address concerns about
nonadherence and poor modeling
of SSP at our children’s hospital,
we used quality improvement
methods to enhance knowledge,
attitudes, and practices related to
the SSP recommendations issued
by the AAP. Our specific aim was
to increase the number of infants
sleeping in complete adherence
to the AAP SSP guidelines to 90%
within 12 months. We hypothesized
that workflow redesign, nurse
education, and reinforcement
through infant room audits during
sleep episodes with just-in-time
feedback would result in improved
adherence to recommended SSP. We
also hypothesized that caregivers
would report increased knowledge
and adherence to the AAP sleep
recommendations at home after
discharge.
METHODS
Context
The American Family Children’s
Hospital is a medium-sized, urban,
academic children’s hospital where
the majority of infants are admitted
to 1 of 3 mixed medical and surgical
units. There is no birthing service
at the hospital. Hospital medicine,
subspecialty, and surgical attending
physicians staff these units, supervise
pediatric and surgical residents, and
collaborate with nursing colleagues.
Planning the Intervention
We chose SSP as an area for
improvement after the release of the
2011 AAP infant sleep environment
recommendations. 2 This work
paralleled our community hospital
advocacy task force initiative to
improve the safety of home sleep
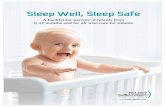
practices. Figure 1 provides an
overview of the hospital quality
improvement project.
A multidisciplinary stakeholder team
of nurses, attending and resident
physicians, a surgical advanced
practitioner, and a hospital quality
and patient safety officer gathered
before the intervention. This group
defined the ideal hospital SSP based
on AAP guidelines for the home
sleeping environment adapted to the
inpatient setting by using local expert
opinion and best practice sleep
policies from 3 other institutions.
A baseline assessment of hospital
SSP was conducted via a Web-
based audit tool on the intervention
unit and included rooms of all
hospitalized infants <12 months of
age, regardless of underlying medical
condition, length of stay, or acuity of
illness. Rooms were excluded if they
were located outside the primary
intervention unit.
Improvement Activities
After the baseline assessment, a
fishbone diagram (Supplemental
Figure 3) was constructed to
identify important candidate causes
of nonadherence with SSP in the
hospital; improvement activities
were then designed to address these
causes. We developed a hospital
policy statement for SSP, a process
map of standard infant room setup
on admission, followed by a redesign
to eliminate both placement of
extraneous items in the crib and
provision of excessive linens for
bundling. Our final activity at the
start of the project was development
of a computer-based education
module outlining SSP. Hospital staff
nurses and nursing assistants from
all units completed this education
module during their annual
education review in 2014.
Data from Web-based room audits
were reviewed by a smaller unit-
based workgroup every 2 weeks.
Additional improvement activities
targeted adherence to SSP by using
iterative Plan–Do–Study–Act cycles.
A summary of activities included the
following:
1. Recruitment of nurse and nursing
assistant safe sleep champions
2. Auditing of infant rooms
weekly by champions with
the development of scripts for
champions to provide feedback to
colleagues after room audits
3. Distribution of commercial sleep
sacks to intervention unit and
families
4. Incorporation of a visual cue in
infant rooms based on the US
Department of Health and Human
Services Safe to Sleep educational
campaign material 1
e2 by guest on January 10, 2021www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
5. Designation of space for the
infant’s personal care items
6. Delivery of grand rounds to
physician and nursing providers
by a national expert
Results of key measurements and
targets for improvement were added
to the unit’s publicly posted quality
scorecard.
Study of the Improvement
Nurse Knowledge
Nurses’ knowledge of AAP SSP
was assessed immediately before
and after the module via a Web-
based questionnaire designed for
this project. Key hospital SSPs
queried included maintaining a flat
HOB, absence of items in the crib,
appropriate bundling (sleeper alone,
single blanket or sleep sack), and
supine sleep position in the crib. Self-
reported comprehension of the AAP
sleep recommendations was also
assessed.
Hospital SSPs
SSP room audits were conducted
via a structured Web-based audit
tool designed for this study. The
tool included items that assessed
infant sleep location (crib or other),
infant sleep position (supine, side,
or prone), HOB position (elevated
or flat), number of items per crib,
and appropriate bundling (sleep
sack, single blanket, sleeper
alone). Complete adherence to
SSP was defined as presence of all
recommendations simultaneously
(sleeping in a crib, supine,
appropriately bundled with a flat
HOB and no items in the crib).
Nurses from the safe sleep
workgroup collected baseline data
by using the Web-based audit
tool between October 2013 and
November 2013, from a convenience
sample of rooms of sleeping
infants, with a goal of 10 room
observations per week. Safe sleep
champions collected ongoing data
during the intervention period,
typically overnight from infant sleep
episodes on the intervention unit
through December 2014. Champions
continuously reviewed the audit tool
with the supervising nurse manager.
Caregiver-Reported Practices at Home
The home sleep practices of
discharged infants <6 months of
age were assessed via a structured
data collection tool during the
preintervention phase, October 2013
through January 2014, and in the
postintervention period, February
through April 2014. Discharges from
the intervention unit in the previous
month were obtained weekly from
administrative data, and a research
e3
FIGURE 1Hospital-based SSP implementation timeline of data collection and interventions, July 2013 through December 2014.
by guest on January 10, 2021www.aappublications.org/newsDownloaded from

SHADMAN et al
nurse attempted phone contact ≤2
times. Caregivers were excluded if
they did not speak English, they were
inaccessible by phone, or the child
was in foster care.
As in the room audit tool, measures
of SSP included infant sleep location,
sleep position, HOB position, and
appropriate bundling. In addition,
we inquired about bed sharing,
and caregivers were queried for
recollection of sleep education by
hospital staff. We did not inquire
about the number of items in the
crib, because we thought this would
be an unreliable question to recall.
The definition of complete adherence
to SSP otherwise paralleled that for
inpatient SSP. Clinical characteristics
we hypothesized to influence SSP at
home were also assessed: history of
reflux, apnea or cardiorespiratory
monitor use, assisted respiration, and
tube feeding.
Analysis
Differences in nurse knowledge,
hospital practices, and caregiver
practices at home before and after
the improvement interventions
were assessed with χ2 tests for
categorical variables and t tests
for continuous variables. A P value
<.05 was considered significant.
Statistical process control (SPC)
p-charts and run charts were used
to monitor changes in hospital SSPs
using established rules for identifying
special cause variation. 17, 18 We
considered 8 consecutive points
above or below the centerline and
any points outside the control
limits to represent special cause
variation and prompt a change in the
centerline. 19, 20 Such observations
happen <0.4% of the time by chance
and are therefore conventionally
accepted as suggesting statistically
significant changes.21
Human Subjects Protection
This quality improvement initiative
was considered exempt by the
University of Wisconsin School
of Medicine and Public Health’s
Institutional Review Board.
RESULTS
Nurse Knowledge
Nursing staff completed 289
preeducation knowledge assessments
and 315 posteducation assessments.
Staff were primarily full-time
registered nurses with >5 years of
experience, nearly half of whom
had children of their own ( Table 1).
Preeducation and posteducation
results of SSP knowledge are
presented in Table 1. Staff
demonstrated increased knowledge
of appropriate sleep position, crib
items, HOB position and bundling,
and self-rated comprehension of
the AAP SSP recommendations
(P ≤ .001).
Hospital Safe Sleep Practices
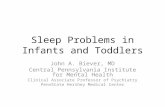
Changes in SSP by audits (n =
316) are shown in Table 2 and
the Fig 2 SPC charts. Baseline data
demonstrated that >96% of cribs
contained ≥1 item (mean 4.4 items
per crib), 40% had an overbundled
infant, and almost 20% were not
flat. Significant implementation
improvements were observed
in the number of crib items and
the proportions of cribs with no
items, flat HOB, and appropriate
bundling (P < .001). Initially, no sleep
episodes were completely adherent
to recommendations, although this
number increased to 26.9% after
implementation (P < .001). Supine
e4
TABLE 1 Nurse Knowledge Before and After Safe Sleep Education Intervention
Preeducation, n = 289 Posteducation, n = 315 P
n % Correct n % Correct
Sleep position .001
Supine 275 95.8 310 99.7
HOB position <.001
Flat 220 76.1 299 95.5
Appropriate bundling 242 83.7 290 92.7 .001
Items in crib <.001
None 210 72.7 277 87.9
AAP bed-sharing policy 283 100 309 99.7 .34
Refl ux and sleep position knowledge 89 30.9 188 60.0 <.001
Self-rated comprehension (4-point Likert scale) <.001
Highest category 66 23.2 147 47.4
Years of nursing experience .97
0–2 79 27.4 85 27.7
3–5 53 18.4 54 17.6
6–10 59 20.5 60 19.5
>10 97 33.7 108 35.2
Have their own children 139 48.4 150 48.7 .95
Occupation .90
Registered nurse 252 87.5 274 88.7
Nursing assistant 24 8.3 23 7.4
Work effort < 50% 36 12.6 32 10.4 .38
by guest on January 10, 2021www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
sleep position of an infant in a
crib (location) had high baseline
performance (>75% adherent)
without significant increases after
implementation.
Similarly, under established run chart
rules 19, 20 SPC charts demonstrated
statistically significant improvement,
that is, special cause variation as
defined in the Methods section,
shortly after the implementation
began and was sustained for all
measures except supine sleep
position and crib sleep location
(Supplemental Figure 4). Special
cause improvement in crib sleep
location was briefly noted after the
educational intervention, although
this improvement was sustained for
only ~2 months before returning to
baseline levels.
Caregiver-Reported Practices at Home
Table 3 highlights the characteristics
of infants included in the caregiver
surveys. A total of 56 caregivers
before nurse SSP education and 48
caregivers after the education were
surveyed (46% response rate). There
were no differences in age or clinical
characteristics between infants of
caregivers surveyed before and
during implementation.
The reported increase in SSP
education received by caregivers
during implementation was not
statistically significant. None of the
measures we included demonstrated
an increase in the implementation
compared with preimplementation
periods. However, caregivers
did report a high rate of crib
sleeping both before and during
implementation (85.7% and 93.8%,
respectively) and absence of bed
sharing (>94% in both cases). They
simultaneously reported a high use
of alternative sleep locations at least
once per day in both before- and
during-implementation periods
(62.5% and 66.7%, respectively).
DISCUSSION
We conducted a multifaceted
quality improvement project
incorporating workflow redesign,
nurse education, and audit and
feedback, which increased nurse
knowledge of SSP and improved
adherence to individual components
of SSP, including maintaining a flat,
empty crib with an appropriately
bundled infant. Adherence to SSP by
caregivers at home was unchanged.
Although we did not reach our
aim of 90% adherence within 12
months, we did achieve significant
improvement in complete adherence
to SSP recommendations. Whereas
previous improvement studies have
focused on infant SSP in newborn
nurseries and NICUs, 14, 16, 22 this is
the first study to our knowledge in a
general inpatient setting.
Our work in this setting complements
and extends previous research
describing the influence of modeling
SSP in the newborn on home
sleep environments. 14, 23 Previous
quality improvement efforts have
demonstrated improvement
in adherence to individual SSP
components 14 or a more limited
assessment of complete adherence
to SSP guidelines (eg, sleeping alone,
supine, and in a crib). 16 We sought
to investigate a more comprehensive
assessment of adherence to all SSP
recommended by the AAP.
Similar to other studies, 24, 25 we
found high levels of nurse knowledge
about SSP, particularly regarding
supine position. The significant
improvement we observed in
knowledge of recommendations
for flat HOB, empty cribs, and
appropriate bundling after education
was also consistent with previous
work. 22 These gains in knowledge
were encouraging because our
baseline audits demonstrated poor
adherence to these specific practices.
Despite these gains, however,
half of the nurses did not rate
their own comprehension of SSP
recommendations at the highest
level. This might suggest a need to
expand the scope of educational
content or to build nurse confidence
in their knowledge. Although
the training module delivered
fundamental information, time
constraints, and its “just-in-time”
nature limited an in-depth discussion
of the rationale behind the SSP
recommendations.
Preimplementation measurement
confirmed our assumption that
adherence to SSP recommendations
was generally low. Most notably, no
cribs had complete adherence to SSP.
As in other studies, 14, 16 implementing
room audits demonstrated overall
improvements, with larger gains
in a subset of practices. Complete
adherence remains challenging,
probably because of the need for
unique solutions for different
components of a safe sleep
environment. Certain SSPs are
probably more responsive than
others to our intervention strategies.
In particular, we observed no
improvements in rates of appropriate
e5
TABLE 2 Audits of Hospital Practices Among Sleeping Infants
Preimplementation (n =
59), n (%)
Implementation (n = 257),
n (%)
P
Sleep location (crib) 46 (78.0) 215 (83.7) .30
Sleep position (supine) 47 (81.0) 215 (84.3) .54
HOB (fl at) 26 (44.1) 187 (73.3) <.001
Appropriate bundling 24 (40.7) 141 (56.0) .03
Items in crib, mean (SD) 4.4 (3.3) 0.9 (1.5) <.001
Cribs with 0 items 2 (3.4) 155 (60.3) <.001
Complete adherencea 0 (0) 69 (26.9) <.001
Age in months, mean (SD) 4.7 (2.9) 5.1 (3.5) .48
a Complete adherence indicates following all recommendations simultaneously (sleeping in a crib, supine, appropriately
bundled, with a fl at HOB and no items in the crib).
by guest on January 10, 2021www.aappublications.org/newsDownloaded from

SHADMAN et al
sleep location or supine position,
potentially explained by a lack of
emphasis in the training module
because initial rates were higher than
most measures.
Inconsistencies between
improvements in nurse knowledge
of a recommendation and changes
in practice for that recommendation
were observed. Improvement in
knowledge of SSPs through Web-
based education has been shown to
be achievable; however, increased
knowledge does not necessarily
translate into practice. 24 Some of
this apparent discrepancy may
be explained by a gap between
knowledge and firmly established
beliefs. For example, despite
knowing correct sleep position,
nurses may maintain the view that
supine position increases the risk
for aspiration. 24 – 26 Nurses may
believe that cardiorespiratory
monitors or frequent vital sign
checks reduce the need to worry
e6
FIGURE 2SSP adherence. Rooms with infant (A) sleeping fl at, (B) appropriately bundled, (C) with no items in crib, (D) with average number of items per crib, and (E) completely adherent.
by guest on January 10, 2021www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
about safe sleep. Families may hold
similar beliefs about SSP, 7, 24 creating
a secondary barrier to adherence
in the hospital. Parental preference
has also been demonstrated to
be a barrier to perfect practice
of sleep recommendations 23 and
may contribute to the lack of
improvement in some measures.
For example, our observed rates
of supine sleep positioning mirror
national rates of supine sleep
positioning in the home, 8 suggesting
to us that future Plan–Do–Study–
Act cycles will need to incorporate
consideration of current caregiver
practices into the development of
improvement activities.
Clinical situations may also influence
practices, even in the presence of
correct information. For example,
despite the lack of evidence, elevating
the HOB is often used as a strategy
for improving respiratory function
in infants admitted with respiratory
illness. Even if nurses know flat HOB
is the “correct answer, ” they may be
inclined to elevate the HOB of infants
admitted with respiratory problems.
Similarly, although evidence for
elevating the HOB in infants needing
nasogastric feeds or continuous
gastrostomy tube feeds is lacking,
there is confusion or disagreement
about positioning the HOB in these
infants.
Lastly, a lack of nurse empowerment
may explain gaps between
knowledge and practice. The
education module did not train
nurses to have skills to address
parent beliefs or practices that
conflicted with recommendations. At
times, nurses may not have known
how to mediate a nonadherent
environment when pressured by
parents. Furthermore, because staff
were not continually present in the
room, families may intentionally or
unintentionally have deviated from
desired SSP.
To address these potential gaps
in knowledge and practice, future
efforts to improve SSP may
need to include training staff to
collaboratively resolve differences
with parents. Although informal
caregiver education occurred
at the bedside, future efforts
should be enhanced. Examples
of potentially effective strategies
include structured programs that
combine modeling with caregiver
education videos and SSP-specific
discharge instructions mirroring
efforts from newborn nurseries and
ICUs. 14, 16, 23
Despite significant improvements in
nurse knowledge and many hospital
practices, reported adherence of
caregivers to SSP recommendations
at home did not demonstrate
significant changes after our
implementation of SSP. Several
potential explanations exist for this
finding. First, posteducation surveys
were conducted shortly after the
nursing education intervention,
corresponding to a time in which
our hospital-based adherence to
e7
TABLE 3 Caregiver-Reported Sleep Practices at Home After Hospital Discharge
Preimplementation, n = 56 Implementation, n = 48
n (%) n (%) P
Hospital care team discussed safe sleep
Yes 15 26.8 17 35.4 .34
Sleep location
Crib 48 85.7 45 93.8 .18
Sleep position
Supine 50 89.3 45 93.8 .42
HOB position
Flat 38 79.2 29 65.9 .15
Appropriate bundling
Yes 42 76.4 42 87.5 .15
Items in crib
None 45 80.4 38 79.2 .36
Complete adherencea
Yes 23 41.1 22 45.8 .63
Bed sharing
No 53 94.6 46 95.8 .78
Alternative sleep locationb >1 per wk
Yes 43 76.8 41 85.4 .27
Alternative sleep locationb >1 per d
Yes 35 62.5 32 66.7 .66
Age in mo, mean (SD) — 3.0 (1.7) — 3.2 (1.8) .54
History of refl ux 5 8.9 8 16.7 .23
Apnea or cardiorespiratory monitor 2 3.6 2 4.2 .88
Assisted respiration 3 5.4 1 2.1 .39
Tube feeding 7 12.5 4 8.3 .49
a Complete adherence indicates following all recommendations simultaneously (sleeping in a crib, supine, appropriately bundled, with a fl at HOB and no items in the crib).b Alternative sleep location indicates location other than crib.
by guest on January 10, 2021www.aappublications.org/newsDownloaded from

SHADMAN et al
SSP was at its lowest. Repeated
evaluation of caregiver practices
during a period of more robust
adherence might provide better
assessment of their influence on
caregiver practice. Second, small
sample sizes limited our power to
detect changes in parent-reported
behaviors. Finally, most education
was done informally at the bedside,
which may have been less influential
in changing home sleep practice
and resulted in fewer caregivers
who recalled SSP education. Nurses
were instructed to provide SSP
education when they found the crib
to be in a state of nonadherence,
although this was at the discretion
of the nurse, and our intervention
did not allow us to systematically
evaluate these interactions. Nurses
may have provided inconsistent
education or failed to fully take
advantage of educational tools.
Improved implementation of
nurse–caregiver education may be
necessary to create changes in SSP
after discharge.
This work has several limitations.
First, we allowed infants to
be resampled because our
measurement unit of interest was
the sleeping episode rather than
patient. Though not completely
independent, each sleep occurrence
represented a new opportunity to
adhere to SSP recommendations.
We never resampled infants during
the same day or same sleep episode.
Second, the cross-sectional nature
of our nursing assessment makes
it unclear how long the increase in
knowledge was sustained. Future
efforts will retest nurse knowledge
at an interval farther from training.
In addition, we did not attempt to
link education of particular nurses
with their practice. Furthermore,
recall and response biases may
have influenced caregiver answers.
Third, our project included
assessment of supine sleep
position in some infants who
were developmentally able to
roll, although the findings did not
change when we excluded infants >6
months of age from analyses.
Lastly, we did not have complete
infant and staff demographic
data; therefore, the influences of
sociodemographics or education
could not be evaluated.
CONCLUSIONS
This project illustrates
our institution’s approach
to implementing the AAP
recommendations for infant SSP
in the hospital setting. Although
previous improvement interventions
have been successful in the NICU
and nursery setting, our findings
show that interventions may
also be successful in a general
inpatient setting, where providers
may have less expertise and focus
on safe sleep practices. Several
improvement strategies translated
well to this more heterogeneous
population, including nurse
education and audit and feedback.
This work identified elements of
SSP that are more challenging to
achieve in the hospital setting,
particularly eliminating items in the
crib, flattening the HOB, avoiding
overbundling, and completely
adhering to recommendations for
SSP. Future research should explore
root causes of nonadherence in
these areas and continue to examine
the potential influence of education
regarding SSP from the nonbirth
hospital on caregiver practices at
home.
ACKNOWLEDGMENTS
We thank Jody Belling, RN, and
Andrea Blom, RN, for their assistance
with caregiver interviews. We also
acknowledge the American Family
Children’s Hospital Safe Sleep
workgroup for their support in
designing the intervention. We thank
the safe sleep nurse champions for
their enthusiastic involvement in this
initiative.
ABBREVIATIONS
AAP: American Academy of
Pediatrics
HOB: head of bed
SIDS: sudden infant death
syndrome
SPC: statistical process control
SSP: safe sleep practice
REFERENCES
1. Safe to Sleep Public Education
Campaign. Available at: www. nichd. nih.
gov/ sts/ Pages/ default. aspx. Accessed
September 1, 2014
2. Moon RY; Task Force on Sudden Infant
Death Syndrome. SIDS and other sleep-
related infant deaths: expansion of
recommendations for a safe infant
sleeping environment. Pediatrics.
2011;128(5):1030–1039
3. Agency for Healthcare Research and
Quality. HCUPnet: Healthcare Cost and
Utilization Project (HCUP). 2006-2009.
Available at: http:// hcupnet. ahrq. gov/ .
Published 2015. Accessed December 7,
2015
4. Colson ER, Bergman DM, Shapiro E,
Leventhal JH. Position for newborn
sleep: associations with parents’
perceptions of their nursery
experience. Birth. 2001;28(4):249–253
5. Colson ER, Joslin SC. Changing nursery
practice gets inner-city infants in the
supine position for sleep. Arch Pediatr
Adolesc Med. 2002;156(7):717–720
6. Colson ER, Willinger M, Rybin D, et al.
Trends and factors associated with
infant bed sharing, 1993–2010: the
National Infant Sleep Position Study.
JAMA Pediatr. 2013;167(11):1032–1037
7. Von Kohorn I, Corwin MJ, Rybin
DV, Heeren TC, Lister G, Colson
ER. Infl uence of prior advice and
beliefs of mothers on infant sleep
position. Arch Pediatr Adolesc Med.
2010;164(4):363–369
8. Colson ER, Rybin D, Smith LA,
Colton T, Lister G, Corwin MJ.
Trends and factors associated
with infant sleeping position: the
National Infant Sleep Position Study,
e8 by guest on January 10, 2021www.aappublications.org/newsDownloaded from

PEDIATRICS Volume 138 , number 3 , September 2016
1993–2007. Arch Pediatr Adolesc Med.
2009;163(12):1122–1128
9. DelRosso LMA. A 3-month-old infant
with recurrent apparent life-
threatening events in a car seat. Chest.
2015;147(4):e152–e155
10. Côté A, Bairam A, Deschenes M,
Hatzakis G. Sudden infant deaths
in sitting devices. Arch Dis Child.
2008;93(5):384–389
11. Tonkin SL, Vogel SA, Bennet L, Gunn
AJ. Apparently life threatening events
in infant car safety seats. BMJ.
2006;333(7580):1205–1206
12. Ahlers-Schmidt CR, Kuhlmann S,
Kuhlmann Z, Schunn C, Rosell J.
To improve safe-sleep practices,
more emphasis should be placed
on removing unsafe items from
the crib. Clin Pediatr (Phila).
2014;53(13):1285–1287
13. Colvin JD, Collie-Akers V, Schunn C,
Moon RY. Sleep environment risks for
younger and older infants. Pediatrics.
2014;134(2). Available at: www.
pediatrics. org/ cgi/ content/ full/ 134/ 2/
e406
14. Gelfer P, Cameron R, Masters K,
Kennedy KA. Integrating “Back to
Sleep” recommendations into neonatal
ICU practice. Pediatrics. 2013;131(4).
Available at: www. pediatrics. org/ cgi/
content/ full/ 131/ 4/ e1264
15. Lesko SM, Corwin MJ, Vezina RM,
et al. Changes in sleep position
during infancy: a prospective
longitudinal assessment. JAMA.
1998;280(4):336–340
16. Mason B, Ahlers-Schmidt CR, Schunn
C. Improving safe sleep environments
for well newborns in the hospital
setting. Clin Pediatr (Phila).
2013;52(10):969–975
17. Schondelmeyer AC, Simmons JM,
Statile AM, et al. Using quality
improvement to reduce continuous
pulse oximetry use in children with
wheezing. Pediatrics. 2015;135(4).
Available at: www. pediatrics. org/ cgi/
content/ full/ 135/ 4/ e1044
18. Dandoy CE, Davies SM, Flesch L, et al.
A team-based approach to reducing
cardiac monitor alarms. Pediatrics.
2014;134(6). Available at: www.
pediatrics. org/ cgi/ content/ full/ 134/ 6/
e1686
19. Benneyan JC. Use and interpretation of
statistical quality control charts. Int J
Qual Health Care. 1998;10(1):69–73
20. Benneyan JC, Lloyd RC, Plsek PE.
Statistical process control as a
tool for research and healthcare
improvement. Qual Saf Health Care.
2003;12(6):458–464
21. Provost L, Murray S. The Health Care
Data Guide: Learning From Data for
Improvement. San Francisco, CA:
Jossey-Bass; 2011
22. Price SK, Hillman L, Gardner P, Schenk
K, Warren C. Changing hospital
newborn nursery practice: results
from a statewide “Back to Sleep”
nurses training program. Matern Child
Health J. 2008;12(3):363–371
23. Goodstein MH, Bell T, Krugman
SD. Improving infant sleep safety
through a comprehensive hospital-
based program. Clin Pediatr (Phila).
2015;54(3):212–221
24. Fowler AJ, Evans PW, Etchegaray JM,
Ottenbacher A, Arnold C. Safe sleep
practices and sudden infant death
syndrome risk reduction: NICU and
well-baby nursery graduates. Clin
Pediatr (Phila). 2013;52(11):1044–1053
25. Grazel R, Phalen AG, Polomano
RC. Implementation of the
American Academy of Pediatrics
recommendations to reduce sudden
infant death syndrome risk in neonatal
intensive care units: An evaluation of
nursing knowledge and practice. Adv
Neonatal Care. 2010;10(6):332–342
26. Barsman SG, Dowling DA, Damato
EG, Czeck P. Neonatal nurses’ beliefs,
knowledge, and practices in relation
to sudden infant death syndrome
risk-reduction recommendations. Adv
Neonatal Care. 2015;15(3):209–219
e9 by guest on January 10, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-4441 originally published online August 1, 2016; 2016;138;Pediatrics
Kristin A. Shadman, Ellen R. Wald, Windy Smith and Ryan J. CollerImproving Safe Sleep Practices for Hospitalized Infants
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/138/3/e20154441including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/138/3/e20154441#BIBLThis article cites 22 articles, 7 of which you can access for free at:
Subspecialty Collections
http://www.aappublications.org/cgi/collection/hospital_medicine_subHospital Medicinesubhttp://www.aappublications.org/cgi/collection/quality_improvement_Quality Improvement_management_subhttp://www.aappublications.org/cgi/collection/administration:practiceAdministration/Practice Managementfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on January 10, 2021www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-4441 originally published online August 1, 2016; 2016;138;Pediatrics
Kristin A. Shadman, Ellen R. Wald, Windy Smith and Ryan J. CollerImproving Safe Sleep Practices for Hospitalized Infants
http://pediatrics.aappublications.org/content/138/3/e20154441located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2016/07/28/peds.2015-4441.DCSupplementalData Supplement at:
by the American Academy of Pediatrics. All rights reserved. Print ISSN: 1073-0397. the American Academy of Pediatrics, 345 Park Avenue, Itasca, Illinois, 60143. Copyright © 2016has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on January 10, 2021www.aappublications.org/newsDownloaded from