Improving health care for immigrant and minority populations in the US
30
Improving health care for immigrant and minority populations in the United States Using practice, policy, and strategic alliances to drive change Julia Puebla Fortier Resources for Cross Cultural Health Care
-
Upload
guest1a0563 -
Category
Health & Medicine
-
view
1.910 -
download
1
description
Using practice, policy, and strategic alliances to improve access to and quality of care for diverse populations
Transcript of Improving health care for immigrant and minority populations in the US

Improving health care for immigrant and minority populations in the United States
Using practice, policy, and strategic alliances to drive change
Julia Puebla FortierResources for Cross Cultural Health Care

Resources for Cross Cultural Health Care
Policy development National CLAS Standards
Research Research agenda on cultural and linguistic
competenceEducation
Biennial conference seriesInformation dissemination
Newsletter and DiversityRx websiteProfessional networking and support
CLAS-talk listserv and ‘Your Voice’ project

Outline Financing and access to health services in
the U.S. Key forces and players Role of service delivery innovation Research on disparities and barriers to care Policy structures and models Non-profit and for-profit sector contributions Role of strategic alliances

Health care insurance in the U.S.
(Employment-based) private insurance Through networks of government and
private providers Government insurance
Medicare (elderly, disabled) Medicaid (low-income) Through participating providers

No insurance
Government/NGO clinics and hospitals Sliding scale fees ‘Charity’ care as part of mission
Private providers Self-pay Unreimbursed care (loss)

Refugees and health/social services
Government-funded resettlement program Local/regional health departments Voluntary Agencies Mutual Assistance Agencies
Community clinics/hospitals Private practitioners

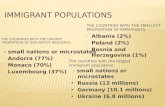
Immigrants and health/social services May have employment-based health
insurance Sometimes have Medicaid Use of community clinics, hospitals Often self-pay Immigration status
Legal – government program eligibility Undocumented – neither public nor private
insurance

Key forces in improving access and quality of care for immigrants and minorities
Minority health and civil rights Cultural and linguistic competence Health disparities reduction Quality improvement The ever-elusive goal of cost-
effectiveness

Key players Minority and civil rights leaders State and local health departments Front-line providers in diverse communities Health services researchers State and national policy leaders
Federal government National health professional and quality
organizations Private foundations

Service innovation:Community oriented providers
Community health centers Public hospitals Public health departments Health education programs run by
community based organizations

Service innovations for diverse populations Medical interpretation and translation services
—on-site and telephone Cultural competence training Use of cultural mediators/community health
workers Patient/community involvement in governance
and planning Technical assistance to other health care
organizations on health/social/cultural/linguistic issues specific to ethnic minority populations

Power of service innovations
Community-oriented providers had legal mandates to be responsive to the needs of underserved populations
They inspired and raised the performance bar for other providers
They drove the development of policy: gov’t requirements/programs need models and a track record of success

Policy framework
Minority health agenda (programmatic)
Refugee resettlement programs Civil rights laws State laws and regulations National CLAS Standards Minority health disparities reduction Quality improvement agenda

Offices of Minority Health Legislation to strengthen and expand the
scope of the federal Office of Minority Health and related programs (1990-) Additional funding More specificity about language and cultural
issues Increase number of minority health
professionals Support for state Offices of Minority Health

Development of National CLAS Standards
CLAS: Culturally and Linguistically Appropriate Services in Health Care
Research on model programs and policies Identification of common elements Draft standards—aimed at health care
organizations National public comment period Publication in the Federal Register

CLAS Standards: Categories of interventions Culturally Sensitive Interventions
Cultural competence education Race, ethnic and linguistic concordance Cultural mediators, community health
workers and culturally competent health promotion
Language Assistance Bilingual services, oral interpretation,
translated written materials

CLAS Standards: Categories of interventions
Organizational Supports for Cultural Competence Management and policy strategies Community engagement Information and data for planning and
evaluation Appropriate ethics and conflict
resolution processes

Unexpected impact
Highly symbolic impact Raised profile of the issue Spurred discussion, controversy,
refinements Offered an organizing framework Prompted action

NGOs and research, policy development, and advocacy Research and tool development to
enhance knowledge and good practice Consensus-building to advance key
issues State and federal policy analysis and
policy formulation Awareness-raising and advocacy to
improve practices and policy structures

Research on disparities and barriers to care Government and foundation funding for
research on minority/immigrant populations Barriers to care Comparative health status Effectiveness of targeted interventions
Institute of Medicine Report: “Unequal Treatment”
New government initiatives to address health disparities

Role of Strategic Alliances
Decision to reach beyond traditional ‘advocates’ to mainstream health stakeholders
Key role of money and convening power of foundations and government health agencies
Demonstrate the relationship between emerging national health agendas and this population

Synergy and support
Identify who has the power in health policy making
Bring them to the table Show how their agenda can’t
succeed unless these concerns are integrated
In time, they become your allies

State and Federal policy level States: coalitions of community clinics, ethnic
community organizations, civil rights advocates working with sympathetic health department officials and elected representatives
National: data from state and local programs, combined with national ethnic organizations, elected representatives and their staff. Federal health agencies not so sympathetic at first, except at Office of Civil Rights

Examples: language access
1995 briefing on language access –first time non-traditional stakeholders to the table
NHeLP language access coalition – informational at first, now working together for policy points in health care reform

Key issues and stakeholders Patient centered care: medical societies Quality of care: accreditation agencies,
hospital associations Patient safety/medical errors: risk
managers/legal departments Disparities reduction: NIH, AHRQ Effectiveness/cost containment: public
and private insurance agencies

Influence of quasi-regulatory agencies
Initiatives from key health care quality and accreditation organizations: The Joint Commission National Committee for Quality
Assurance The National Quality Forum

Role of for-profit sector
Service provider financial support for language and cultural
services Uncompensated care
Companies that provide interpretation and translation services
Consultants who do training and program support

Foundations
Major players The Robert Wood Johnson Foundation The Commonwealth Fund The WFF Kellogg Foundation The California Endowment Regional and community foundations

Final thoughts Policy statements are not enough
Funding for demonstrations, evaluations, research, technical assistance
Impact of success Awareness raising and advocacy to a
broad and influential audience Integration of the needs of diverse
populations into broader health priorities

For more information
Julia Puebla Fortier, Director Resources for Cross Cultural Health Care
[email protected] www.diversityRx.org