Improving Care and Generating ROI: A Davies Story...1 Improving Care and Generating ROI: A Davies...
41
1 Improving Care and Generating ROI: A Davies Story Session 95, March 6, 2018 Anupam Goel, MD, VP Clinical Information, Advocate Health Care Angela Diop, ND, CHCIO, VP of Information Systems, Unity Health Care Andrew Robie, MD, Chief Medical Information Officer, Unity Health Care Organization logo(s) may be placed on this slide
Transcript of Improving Care and Generating ROI: A Davies Story...1 Improving Care and Generating ROI: A Davies...

1
Improving Care and Generating ROI: A Davies StorySession 95, March 6, 2018
Anupam Goel, MD, VP Clinical Information, Advocate Health Care
Angela Diop, ND, CHCIO, VP of Information Systems, Unity Health Care
Andrew Robie, MD, Chief Medical Information Officer, Unity Health Care
Organization logo(s) may be placed on this slide

2
Anupam Goel, MD MBA
Angela Duncan Diop, ND, CHCIO
Andrew Robie, MD
Have no real or apparent conflicts of interest to report.
Conflict of Interest

3
AgendaTranscription costs (Advocate Health Care)
• Technology and behavior change
• Workflow considerations
• Results
• Next steps
Leveraging health IT to improve care of hypertensive patients (Unity Health Care)
• Change management
• How Health IT was used
• Results
• Lessons learned

4
Learning Objectives• Describe the financial and workflow considerations when migrating
from a telephone transcription to voice-to-text physician documentation model
• Apply metrics to help track expected financial savings when migrating from one physician documentation model to another
• Formulate a comprehensive approach that engages, staff and patients to significantly improve blood pressure control in a patient population
• Identify the components of a change management system that will help you repeatedly deliver meaningful and lasting organizational change to support your quality initiatives

5
Using Technology to Address Transcription Costs

6
Technology and behavior change• Facilitating factor: innovation benefits
• Limiting factors: design, technical concerns, familiarity with technology, time
Gagnon et al. Systematic Review of Factors
Influencing the Adoption of Information and
Communication Technologies by Healthcare
Professionals, J Med Sys 2012. 36:241-77.

7
Environment and context• iPhone adoption among independent provider community
• Improvements in voice recognition technology
• EMRs and clinician burnout

8
https://www.ncbi.nlm.nih.gov/pmc/articles/P
MC3889939/pdf/11606_2013_Article_2597.

9
Workflow considerations• Operative reports
• H&Ps, consults
• Progress notes
• Discharge summaries

10

11

12
Stopped progress
note telephone
transcription at most
sites
13
Results• We ended 2015 with $2.24 M transcription spend (over 50%
reduction from January’s annualized estimates)
• In August 2017, we were on track for annual spend of $1.8 M

14
Key lessons• Engage senior clinical and financial leadership early
• Identify clinical champions to create testimonials
• Work with site leaders and demonstrate the technology with opportunities for users to try it out
• Provide feedback reports regularly to target users who might benefit
• When the majority of users have made the switch, institute a hard stop to force the technology adoption

15
Next steps• Voice recognition to natural language processing
• Prompting users before document signature
– Missing data elements (compliance)
– Suggested diagnoses (clinical pathways)
– Suggested treatments (real-time decision support)

16
Federally Qualified Health Center
District of Columbia
Over 106,000 patients and 500,000
visits each year
Promoting healthier communities through compassion and
comprehensive health and human services,
regardless of ability to pay.
Unity Health Care

17
HIMSS Davies Application Team• Catherine Anderton, Associate Director for Quality Improvement and Research
• Angela Diop, VP of Information Systems
• Marcia Hinkle, Assistant Director Social Services: Behavioral Health
• Cherie Jones, Information Systems Manager
• Andrew Robie, Chief Medical Information Officer

18
Unity Sites and Services
Sites
10 Community Health Centers
10 Medical Sites in Homeless
Shelters
2 School-Based Health Centers
Homeless Outreach and
Mobile Van
Health Services in DC Jail
Services
•Primary care and specialty care
•Dental care
•Behavioral health care
•Care to people experiencing
homelessness, HIV, returning
citizens, Title X

19
Change Management
Robust system
of change
management
helps to
develop and
adopt well
thought-out
changes in an
organized
manner.
From Unity’s change management Guidelines for
Electronic Health Records ~2016

20
EHR Governance Teams
20
Stakeholders
• Approve major changes to EHR and workflows and assign resources needed for change.
Implementation Team
• Track issues and changes to resolution. Assign to teams for solution. Implement and communicate changes.
EHR Support Team
• Manage ongoing maintenance, upgrades and implementations and interface with EHR vendor.
Joint Training Team
• Develop EHR and PM training. Train staff.
Reports Team
• Develop reports.
Optimization Team
• Manage major configuration and content changes to EHR.

21
Our Approach
Develop Workflows
Modify EHR
Train Staff
Change

22
Workflow Development
Groups Developing the Workflows• QI Department• QI Working Groups• Optimization Team
In collaboration with Health Information Technology Team (HIT) and Reports Team.

23
Disseminating Change
Change is developed
Working Groups develop training
Multi-disciplinary team-based training is conducted
Measure ResultsTraining is reinforced CHANGE!

24
Hypertension Case Study
25
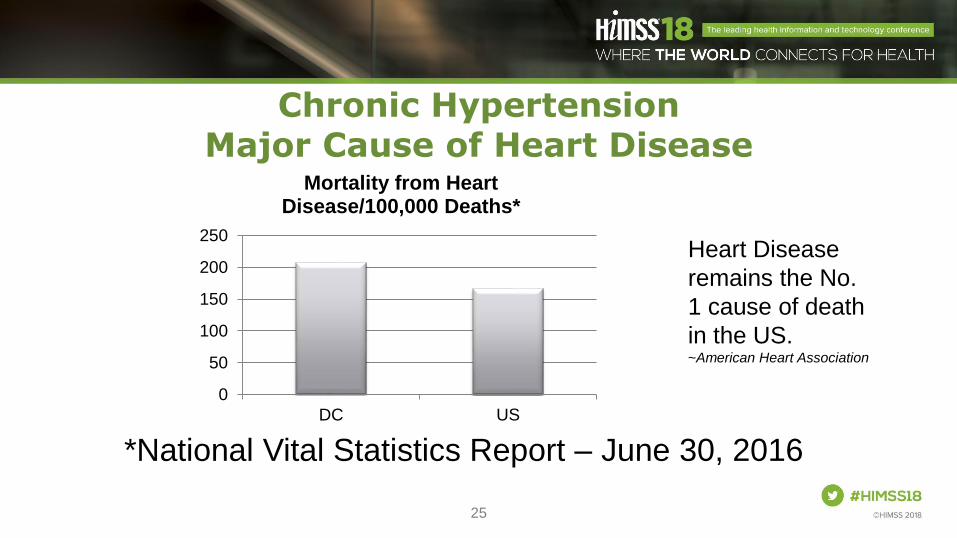
Chronic Hypertension Major Cause of Heart Disease
*National Vital Statistics Report – June 30, 2016
0
50
100
150
200
250
DC US
Mortality from Heart Disease/100,000 Deaths*
Heart Disease
remains the No.
1 cause of death
in the US. ~American Heart Association

26
Unity’s Patients and Hypertension
• Our number one diagnosis
• >20,000 hypertensive patients annually
• Affects >20% of our adult patients

27
Hypertension Goal
• Increase the percentage of patients with hypertension whose blood pressure is controlled
• Baseline December 2013: 54% of patients diagnosed with hypertension were considered controlled with a blood pressure reading less than 140/90

28
How Health IT Was Used

29
EHR Modifications/Set-up
• Alerts
– Reset BP alert to turn red at 140/90
– Alerts for medication-allergy and medication-medication interaction were enabled
– The EHR automates formulary checks helping providers reduce barriers to medication adherence
140/90

30
EHR Modifications/Set-up
• Clinical Decision Support for Providers
– Hypertension progress note based on JNC-8
– Structured preventive medicine documentation populates visit summary with patient education and goals

31
EHR Modification/Set-up
• Created a new visit type, “Nurse BP Follow-Up Visit”
• EHR template supports clinically comprehensive visit, nurse decision points on referral back to provider, patient education, and correct documentation, including coding
• Preventive medicine section in nurse visit documentation reiterates goal BP

32
Measuring Progress
• Reports were generated from the EHR
• Progress was reported to health center leadership at QI meetings
Increases in repeat BPs up to 60%

33
Team Training
• Staff trained in teams
– Review of HTN
– Workflows
– Proper measurement
– Documenting follow-up
• Training was recorded, placed on learning management system
• Compliance with training was tracked

34
Engaged Staff
• Healthy Competition
• Created the Heart of Gold award (HOG)
Columbia Road Health Services, first winner of
the Heart of Gold Award

35
Engaged Patients
• Follow-up patients within 30 days when BP not at goal
• Easy for them to make a Nurse Visit appointment for repeat BP check
• Automated reminder calls
• Shared goals with patients
• Preventive medicine section provided in the visit summary
• QI posters at the sites

36
Value Derived

37
Results
48%
50%
52%
54%
56%
58%
60%
62%
64%
66%
2013 2014 2015 2016
Controlled Hypertension <140/90
Blood pressure control improved by 9.3 percentage points

38
ROI
Hard ROI
• $415,000 due to increased revenue from hypertension nurse visits
Soft ROI
• Increased access because of nurse visits
• Increased provider satisfaction
• Expansion of the role of medical assistants and nurses
• Growth/expansion in team based care resulting in more efficiency
0
1000
2000
3000
4000
HTN Nurse Visits
Number of Visits
2013
2014
2015
2016

39
Lessons Learned
• We can significantly impact HTN control (improving 5-10%) by using multidisciplinary teams throughout all phases of the project
• Don’t just plan training; also plan how to reinforce it
• Think broadly about which team members will be affected by the changes. Often change impacts people on the team that seem to have nothing to do with the project

40
Questions
• Please complete online session evaluation
Contact information
Anupam Goel MD, Advocate Health
•@anupam1623
•LinkedIn: goelanupam
Angela Duncan Diop, ND, CHICIO
• @AngelaDiop
• LinkedIn: AngelaDiop
Andrew Robie, MD
• LinkedIn: AndrewRobieMD
• www.unityhealthcare.org
• @UnityHealthCare