Mechanically Ventilated Broiler Sheds: a Possible Source of ...

Archives of Disease in Childhood, 1974, 49, 505.
Improved prognosis of infants mechanically ventilatedfor hyaline membrane disease
E. 0. R. REYNOLDS and A. TAGHIZADEHFrom the Departments of Paediatrics and Morbid Anatomy, University College Hospital and Medical School,
London
Reynolds, E. 0. R., and Taghizadeh, A. (1974). Archives of Disease inChildhood, 49,505. Improved prognosis ofinfants mechanically ventilated forhyaline membrane disease. The results of mechanical ventilation for severe
hyaline membrane disease (HMD), and the changes in technique which took place,during the 6-year period 1967-72 are described. A pilot study of the effect ofhydrocortisone among the most severely affected infants showed no benefit. After theintroduction at the beginning of 1970 of a regimen for ventilating the infants at lowpeak airway pressures, slow respiratory frequencies, and high inspiration: expirationratios, there was a sudden increase in survival rate which was largely accounted for by a
reduction in the incidence of bronchopulmonary dysplasia. Evidence is presentedthat in infants with HMD mechanical factors are more important than oxygen toxicityin the pathogenesis of this condition.
Mechanical ventilation has been widely used inthe management of HMD for the past 10 years(Thomas et al., 1965; Cooke et al., 1967; Adamsonet al., 1968; Heese et al., 1970; Linsao et al., 1970;Reynolds, 1970b; Stahlman et al., 1970; Stem et al.,1970; Daily, Sunshine, and Smith, 1971; Chernickand Vidyasagar, 1972; Cumarasamy et al., 1973).Our own interest in this form of treatment began atthe end of 1965, and from early 1966 onwards allinfants weighing more than 1000 g who were soseverely affected by the illness that their chances ofintact survival seemed severely jeopardized havebeen ventilated. During the years 1966-69 oursurvival rate for ventilated infants was low(Adamson et al., 1968; Reynolds, 1970b), and morethan half of those who died were found to have thechanges of bronchopulmonary dysplasia at necropsy(Hawker, Reynolds, and Taghizadeh, 1967;Northway, Rosan, and Porter, 1967). Frompathological studies (Hawker et al., 1967) it appearedpossible that at least two potentially preventablefactors might be involved in the pathogenesis ofbronchopulmonary dysplasia: mechanical trauma tothe lung from the use of very high peak airwaypressures and fast respiratory frequencies during thephase of surfactant deficiency, and pulmonaryoxygen toxicity. Experiments were therefore
Received 29 November 1973.
started in 1969 (Reynolds, 1971; Herman andReynolds, 1973) in order to find ways of ventilatingthe infants at lower peak airway pressures andoxygen concentrations reduced as far as possiblebelow 100%. After the application at thebeginning of 1970 of results from the first series ofexperiments, a sudden increase in survival rate tookplace, together with a diminution in the incidence ofbronchopulmonary dysplasia.The purpose of this report is to present our results
for the years 1967-72 and to analyse the factorswhich may have been responsible for this improve-ment in prognosis.
Material and methods
Population. During the years 1967 to 1972, 164infants who weighed more than 1000 g at birth wereadmitted to the Neonatal Unit of University CollegeHospital with a diagnosis of severe HMD. Smallerinfants have not been included in the analysis because ofdiagnostic difficulties and because they were notinvariably mechanically ventilated if they becameapnoeic, whereas infants weighing more than 1000 gwere. The diagnosis of severe HMD was based on thefollowing. (1) The presence at 4 hours of age or later ofat least 3 of these 4 abnormal physical signs: abnormalretractions of the chest wall during inspiration, cyanosisrequiring an increased inspired oxygen concentration forits relief, a respiratory frequency of 60 breaths/min or
505

506 Reynolds anmore, and expiratory grunting. (2) Persistence ofabnormal breathing beyond 72 hours of age. (3) Acharacteristic reticulogranular appearance of a chestx-ray (Peterson and Pendleton, 1955) obtained at 4 hoursof age or subsequently. (4) An arterial oxygen tension(Pao2) after the first 4 hours of life of less than 90 mmHgwhile breathing more than 60% oxygen. The diagnosisin infants needing mechanical ventilation from birth orshortly afterwards was based on criteria (2), (3), and (4).By considering only infants meeting these criteria wehope to have excluded mild cases of HMD in whom adefinite diagnosis is difficult or impossible to makeduring life, as well as infants with other respiratoryillnesses.
Management. The general management of infantswith HMD cared for at this hospital has been detailedelsewhere (Adamson et al., 1968; Reynolds, 1970a, b,1974) and is summarized as follows. Infants at risk bornin the hospital were carefully observed during labour inorder to minimize the chances of intrapartum hypoxia.Paediatricians were present at delivery, and rapidresuscitation using endotracheal intubation, intravenoussodium bicarbonate solution, and external cardiacmassage was performed as indicated. Infants trans-ferred from other hospitals were almost always collectedin a portable incubator by a member of the medical ornursing staff trained in resuscitation. Since early 1968the portable incubator was equipped with facilities formechanical ventilation in transit, should this provenecessary (Blake et al., 1970a).
After admission to the Neonatal Unit, the infants werenursed in incubators in a neutral thermal environment.Frequent arterial blood samples were obtained fromindwelling umbilical arterial catheters or by puncture ofperipheral arteries and measurements of Pao2, Paco2, pH,and base excess were made within the unit usingRadiometer equipment. The inspired oxygen con-centration was measured with a Beckman or Tekmaroxygen analyser and regulated to produce, if possible, aPao2 in the range 50 to 90 mmHg. If a substantialnegative base excess was found, it was partially or totallycorrected with intravenous 5% sodium bicarbonatesolution administered slowly through the arterial catheteror intravenously through an umbilical vein catheter or aperipheral vein.
All infants were carefully observed by nurses trained inendotracheal intubation. Cardiac ratemeters were usedfor monitoring, together with, from early 1969, apnoeaalarm mattresses (Blake et al., 1970b). Arterial bloodpressure was measured in some infants with a Sanbornstrain gauge transducer attached to the umbilical arterycatheter.
Oral feeding with expressed breast milk was started assoon as possible, through a fine indwelling nasogastrictube. In most infants about half the fluid requirementfor the first 48 to 72 hours was supplied by this route andthe remainder as an intravascular infusion of electrolytesand 10% dextrose. Oral feeding was reduced orstopped in the most severely affected infants, and since1971 some of them have been partially or totally intra-
Id Taghizadehvenously fed via an indwelling silicon rubber catheter(Shaw, 1973). Blood glucose levels were determined,usually using Dextrostix, and any tendency towardshypoglycaemia was corrected with oral or parenteralglucose. Plasma bilirubin, calcium, and electrolytelevels were measured as indicated and abnormalitiescorrected. From 1967 until mid-1969 all infants weretreated with ampicillin and cloxacillin, but this policywas then stopped. Subsequently, kanamycin orgentamicin, together with penicillin or cloxacillin, havebeen the main antibiotics used and have been given onlyfor suspected or proven infection.We have always been concerned to avoid unnecessary
interference with infants suffering from HMD, believingthat it is very easy to precipitate a deterioration incondition or apnoea. When Gregory et al. introducedtheir technique of continuous positive airway pressurebreathing (CPAP) in 1971, we therefore initially used itonly for weaning infants from the ventilator. Afteracquiring experience with various forms of CPAP, westarted in May 1972 a controlled trial of 'early' inter-vention (Pao2 <60 mmHg while breathing more than95% oxygen) with CPAP using either an endotrachealtube or a negative pressure tank round the trunk. In1972, therefore, a few ventilated infants had previouslybeen treated by CPAP, whereas the others had not.
Indications for mechanical ventilation. Initially ouronly indications were apnoea or a deterioration in clinicalcondition accompanied by peripheral vasoconstriction, afall in heart rate or gasps superimposed on a slowingrespiratory frequency. More recently, since mid-1969,a further indication was added-Pao2 < 35 mmHg whilebreathing more than 95°h oxygen.
Method of ventilation. All infants meeting theseindications for ventilation were immediately intubated,usually by nursing staff. No infant was allowed todeteriorate into a severely compromised state beforeresuscitation was undertaken. Oroendotracheal tubes(Warne No. 12 or 14) were used and were fixed in placeby fitting them through a cut-off Portex tracheostomytube tied to a gauze hat. Bennett PR2 machines wereused exclusively until September 1972; subsequently amodified Draeger Spiromat 662 ventilator has beenemployed. Because infants with HMD normallybreathe very fast, we initially decided to mimic theirpattern of spontaneous breathing as closely as possible.The machine was therefore set at a frequency of 60 to 80cycles/min. At this frequency the Paco2 could easily bekept normal, but the Pao2 was often too low (we aimedfor 50-90 mmHg) unless we used a very high peak airwaypressure (35-60 cm li2O). During late 1969, experi-ments were performed (Reynolds, 1971) which showedthat by using a pressure wave-form resembling a squarewave, a slow respiratory frequency (30/min), and a highinspiration:expiration ratio (3 1:1), adequate oxygena-tion could be achieved at a much lower peak airwaypressure (about 25 cmH]2O). From the start of 1970,therefore, it was possible to ventilate the infants at amuch lower peak airway pressure and respiratory

Improved prognosis of infants mechanically ventilated for hyaline membrane disease 507
frequency than in previous years. From the end of1970, the usefulness of a high inspiration :expiration ratioin improving Pao2 was exploited in order to reduce theinspired oxygen concentration, as well as reduce peakairway pressure. In 1971 and 1972 a further series ofexperiments (Herman and Reynolds, 1973) showed thatthe use of a positive end-expiratory pressure was alsoeffective in improving Pao2, and this manoeuvre has beenused routinely since mid-1972, mainly to help reduce theinspired oxygen concentration. CPAP has been usedfor weaning the infants from the ventilator since April1971.
Bronchial suction and lavage were performed atintervals which depended on the amount of secretionsproduced by the infant. Cultures of endotrachealsecretions were examined daily. Prophylactic anti-biotics (ampicillin, cloxacillin, kanamycin, or colistin)were administered both systemically and down theendotracheal tube until the end of 1970. This practicewas then abandoned and subsequently antibiotics(kanamycin and cloxacillin or gentamicin and penicillin)have been given systemically only in the presence ofclinical or bacteriological evidence or suspicion ofinfection.
Steroid trial. Because of evidence that steroidswere capable of stimulating the production of pulmonarysurfactant in fetal lambs (Liggins, 1969), a pilotcontrolled trial of hydrocortisone (10 mg/kg per 24 hr, in3 divided doses intramuscularly) was started among themost severely affected infants in September 1970.Infants were entered into the trial if the severity of theirpulmonary illness was such that they requiredmechanical ventilation within 24 hours of birth. Theinfants were assigned to the treatment or nontreatmentgroup from sealed envelopes. Treatment was continueduntil death, or until the infant had breathedspontaneously for 24 hours. ACTH was then given, 10units on the 1st, 2nd, and 4th days after stoppinghydrocortisone. The trial continued until December1971, when there were 8 infants in each group.
Necropsy. A full necropsy was performed between 4hours and 2 days after death in 53 of the 60 infants whodied. One lung, usually the right, was sectioned andpieces from each lobe were fixed in formol saline; the restwas fixed in formol calcium. The other lung was
inflated by air at 20 to 60 cmH2O pressure, the exactpressure depending on that used terminally in life. Theinflated lung was then fixed by formol calcium injectioninto the pulmonary artery until the solution running fromthe pulmonary veins was free of blood, after which it wassuspended in a similar solution. Paraffin and frozensections were prepared from inflated and noninflatedlungs and stained with a variety of stains. In many cases
a needle biopsy of the lung was obtained immediatelyafter death, fixed in glutaraldehyde, and prepared forelectron microscopy. Further details of the methodsemployed in examining the lungs are given elsewhere(Taghizadeh and Reynolds, 1975).
ResultsBecause a sudden change in our methods of
setting the ventilator occurred at the beginning of1970, the results are presented in two 3-year periods,1967-69 and 1970-72, so that comparisons can bemade. Most of the data were collected during theinfant's admission to the unit. The significance ofdifferences between proportions, including thedistribution of birthweight by 500 g groups andgestation by 3-week periods, was analysed using X2,with Yates's correction when appropriate.Student's 't' test was used to test the differencebetween mean values.
Population and overall survival rate. Thetotal number of infants admitted who fulfilled ourcriteria for a diagnosis of severe HMD, the numbersborn in this hospital and those transferred fromother institutions, and the mean birthweights,gestational ages, and survival rates for each categoryof infant are given in Table I. As expected, there
TABLE IBirthweight, gestational age, sex ratio, and survivalratefor infants admitted with severeHMD in 1967-69
and 1970-72
1967-69 1970-72
Total no. of infants withsevere HMD 69 95Birthweight (g) 1700 (1020-3200) 1690 (1045-3572)Gestation (wk) 33 (27-37) 32 (27-39)Sex ratio M:F 47:22 62:33Survived 38 (55%) 66 (69%)
Born in this hospital 39 (56%) 54 (57%)Birthweight (g) 1520 (1020-3200) 1700 (1045-3572)Gestation (wk) 32 (27-37) 33 (27-39)Sex ratio M:F 25:14 38:16Survived 22 (56%) 40 (74%)
Born elsewhere 30 (44%) 41 (43%)Birthweight (g) 1900 (1150-3105) 1640 (1100-3130)Gestation (wk) 34 (27-37) 32 (27-37)Sex ratio M:F 22:8 24:17Survived 16 (53%) 26 (63%)
Note: Median values and ranges are shown.
were more boys than girls (P <0 * 05). Nosignificant differences were found between the two3-year periods for birthweight, gestational age, sexratio, or for the proportion of infants admitted fromoutside the hospital. Though the survival rate ofinfants born in the hospital increased significantlyfrom 56% in the first period to 74% in the second(P <0 05), the change in overall survival rate from55 to 69% did not quite reach significance(P <0-10).

508 Reynolds and TaghizadehTABLE II
Details of infants treated by mechanical ventilation (MV), and comparison between 1967-69 and 1970-72
1967-69 1970-72 P
No. of infants treated by MV 35 57% of total admitted with severeHMD 51 60 NS
Birthweight (g) 1470 (1020-2807) 1540 (1045-2890) NSGestation (wk) 31 (27-37) 32 (27-37) NSSex ratio M:F 26:9 36:21 NSSurvived 4 (11% of MV) 28 (49% of MV) <0c001
Born in this hospital 20 27% of infants admitted with severeHMD 51 50 NS
Birthweight (g) 1300 (1020-2126) 1530 (1045-2638) <0 005Gestation (wk) 29 (27-34) 31 (27-37) <0 05Sex ratio M:F 14:6 20:7 NSSurvived 3 (15% of MV) 12 (44% of MV) <0-025
Born elsewhere 15 30% of infants admitted with severeHMD 50 73 <0*05
Birthweight (g) 1820 (1280-2807) 1620 (1100-2890) <0 05Gestation (wk) 33 (28-37) 32 (27-37) NSSex ratio M:F 12:3 16:14 NSSurvived 1 (7% of MV) 16 (53% of MV) <0 001
Note: Median values and ranges are shown.
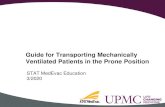
Proportion of infants mechanicallyventilated and ventilator survival rate. TableII gives figures for the numbers of infants ventilatedtogether with their birthweights, gestational ages,sex ratio, and survival rates. The birthweights andgestational ages of infants born in this hospital werehigher in the second 3-year period, the birthweightsof infants admitted from other hospitals were lower,and the proportion of infants admitted from outsidewho were ventilated was higher, but no significantdifferences were found when the population wasconsidered as a whole with respect to birthweight,gestational age, sex ratio, or the proportion of infantssubjected to mechanical ventilation. The survivalrate of ventilated infants increased, however, from11% in 1967-69 to 49o% in 1970-72 (P <0 001).The Fig. shows survival by birthweight for thesecond period.
Time of starting and duration ofmechanicalventilation. Ventilator variables. Table IIIsummarizes data from the ventilated infants.Striking changes in ventilator settings occurredbetween the two 3-year periods. Peak airwaypressure, the number of infants ventilated with peakairway pressures of 35 cmH2O or more, and therespiratory frequency were all much reduced in thesecond period. Altering the length of inspiration asone means for regulating Pao2 was used only 3 timesin 1967-69, but it was a routine part of managementin 1970-72. A positive end-expiratory pressure wasused in a small, but significant number of infants in1970-72.
35 - t5)
30-
6425
20 90
015-E
U1 1 1 i 8910 ~~~~~~~~100
5
01000 1500 2 2500 3000 3500
Birthweight 9
FIG.-Infants with severe HMD, divided into birthweightgroups, admitted during the years 1970-72. Thepercentage of infants surviving is given at the head of eachcolumn. D survived without mechanical ventilation, ,
survived after mechanical ventilation, died aftermechanical ventilation.
CPAP. CPAP was frequently used to weaninfants from the ventilator in the second 3-yearperiod (Table III).
Oxygen therapy. The inspired oxygen con-centration during mechanical ventilation, thenumber of infants who breathed more than 80%oxygen for more than 100 hours (whether breathingspontaneously or during mechanical ventilation),
r-

Improved prognosis of infants mechanically ventilatedfor hyaline membrane disease 509TABLE III
Age at the start and duration of mechanical ventilation; details of ventilator variables, the numbers of infantstreated by CPAP, and details of oxygen therapy
1967-69 1970-72 P
No. of infants treated by MV 35 57Age at start (hr) 16-2±5-2 22-0+3-2 NSDuration (hr) 139*6±23*1 89*7±12*6 <0c025Duration in survivors (hr) 88-7+20-9 68-6±15-5 NS
Ventilator variablesPeak airway pressure (cmH.O) 36-0±1-3 26-2+2-9 <0 001Peak airway pressure 935 cmH20 (no. of infants) 30 (86%) 15 (26%) <0c001Respiratory frequency (per min) 64 5±29 33 1±0 5 <0c001Inspiration: expiration ratio used to regulate Pao2
(no. of infants) 3 57 <0c001Positive end-expiratory pressure used (no. of
infants) 0 8 <0*01CPAPUsed before MV (no. of infants) 0 3 <0 05Used during illness (no. of infants) 0 23 <0-001Used during weaning in survivors (no. of infants) 0 16 <0 01
Oxygen therapyInspired 02 concentration during MV (%) 86-94+0-03 78-96±0-02 <0-01Inspired 02 concentration 380% for 3100 hr
(no. of infants) 16 (46%) 11 (19%) <0 0125Time until surviving infants were breathing room
air (dy) 45-5+10 9 17-1 ±3-5 <0 001
Note: SE of mean values is shown.
and the time taken until the surviving infants werebreathing room air were all less in the second period(Table III).
Pneumothorax. In 1967-69 pneumothoraces,sometimes together with pneumomediastinums,occurred in 6 infants (17%) during mechanicalventilation; 3 other infants developed spontaneouspneumothoraces before ventilation started and 1additional infant had pneumothoraces due to beingintubated and connected directly to an oxygencylinder in another hospital before transfer. Allthese infants died.
In 1970-72, 8 infants (14%) developed pneumo-thoraces with or without pneumomediastinumsduring ventilation; 3 infants developed spontaneouspneumothoraces and 1 infant a spontaneousmediastinum before ventilation started, and 1 otherinfant a spontaneous pneumothorax 2 weeks aftersuccessful weaning from the ventilator. 7 of thetotal of 12 infants with pneumothoraces or pneumo-mediastinums survived. The incidence ofpneumo-thorax was not significantly different in the two3-year periods. The mean peak airway pressure atwhich rupture of the lung occurred was 33 cmH2O(range 17-50 cmH20).
Endotracheal cultures. Positive bacterialcultures were obtained from endotracheal aspirate in10 infants (28%) in 1967-69 and 11 infants (19%) in
1970-72. These numbers are not significantlydifferent. The organism most frequently en-countered was Klebsiella aerogenes; other organismsincluded Pseudomonas pyocyanea, Esch. coli, Citro-bacter freundii, and Candida albicans. Presence oforganisms was not usually associated with any otherevidence of infection.
Intravenous feeding. 7 infants were fedintravenously during 1970-72. 5 lived and 2 died.
Steroid trial. The median birthweight of the 8infants treated with steroids was 1680 g (range1420-2330 g), and of the 8 controls, 1580 g (range1160-2520 g). The median gestational ages were33 weeks (31-36 weeks) and 32 weeks (27-35 weeks),respectively. In each group 6 infants were boys and2 were girls. 3 of the 8 infants survived in eachgroup. The mean age at which ventilation started,duration of ventilation, and age at death were similarin the two groups. This pilot study of the effect ofsteroids in the most severely affected infants,therefore, showed no significant benefit of treatmentand it was abandoned.
Necropsy. Detailed description of the necropsyfindings will be published separately (Taghizadehand Reynolds, 1975).
Pulmonary pathology. Table IV summarizes thepulmonary pathology. HMD was diagnosed when

Reynolds and TaghizadehTABLE IV
Pulmonary pathology
1967-69 1970-72 P
Total infants MV 35 57Deaths without BPD 14 17(% of MV) 40 30 NSTotal deaths with BPD 17 12(% of MV) 49 21 <0*01Early deaths with BPD (<28 dy) 15 7(% of MV) 43 12 <0*001Late deaths with BPD (> 28 dy) 2 5(% of MV) 6 9 NS
MV, mechanically ventilated; BPD, bronchopulmonary dysplasia.
atelectasis was present, and eosinophilic hyalinematerial lined distended terminal airways. Noattempt was made to diagnose bronchopulmonarydysplasia in infants who died earlier than 5 daysfrom birth because of difficulties in distinguishingthis condition from the normal repair processes ofthe lung. The diagnosis of bronchopulmonarydysplasia was made when the regeneration andrepair of tissue showed evidence of interference withlung structure and development. Epithelial hyper-plasia with or without foci of squamous metaplasiawas found in large bronchi, together with obliterativegranulation and young fibrous tissue in smallerbronchi, and peribronchiolar fibrosis whichextended into the lobules and distorted theirstructure. In later stages this fibrosis and excessivecollagen and elastic fibres round the air sacs led todeficient development and to alternating areas ofcollapse and emphysema. Hypertrophy of the wallsof small arteries was also present.Among the 7 infants in whom permission for
necropsy was refused, bronchopulmonary dysplasiawas diagnosed from the characteristic x-rayappearance (Northway et al., 1967) in 3 who died
aged between 13 and 30 days. The remaining 4infants without necropsies died within 78 hours ofbirth.The number of infants dying without broncho-
pulmonary dysplasia, when expressed as a per-centage of the total number ofventilated infants, wassimilar in 1967-69 and 1970-72. A strikingreduction occurred, however, in the proportion ofventilated infants dying with bronchopulmonarydysplasia in the second period (Table IV).Evidence oflung infection was present at necropsy
in only 4 infants (8%) during the 6 years 1967-72.Table V summarizes the birthweights, gestationalages, and details of mechanical ventilation andoxygen therapy in the infants who died with andwithout bronchopulmonary dysplasia. Similar datafrom survivors are shown for comparison. Themedian age at death in the infants without broncho-pulmonary dysplasia was 41 hours (range 9 hours-10days) and in those with this condition, 11 days(range 5 days-13 months).
Larynx and trachea. Though superficial damageto the epithelium and oedema of the larynx werecommon, ulceration was present in only 5 infants, 4of whom had been ventilated for more than 5 days.1 infant had a perforation ofthe trachea. Subglotticstenosis was not found.
Cerebral bleeding. Cerebral bleeding was equallycommon in infants who died in 1967-69 and1970-72. Among infants dying without broncho-pulmonary dysplasia it was found in 16 (55%) of thenecropsied infants, and was shown by needling theventricles of 2 others in whom necropsies were notdone. Cerebral bleeding occurred, then, in 18(58%) of the 31 infants for whom information wasavailable, and was intraventricular in 13, sub-
ILE VVentilator variables in survivors and in infants dying with and without bronchopulmonary dysplasia (BPD)
Age at startDuration ~~~Inspired 0,1Sex ratio Birthweight Gestation Age at start Duration PAP f concentration(M:F) (g) (wk) of MV of MV (cmH,O) (per min) during MV
I --(r-(hr (%)Ventilator survivors 21:11 1605t 32* 32*9±+49* 71*2±13*8t 24*6±0i5* 34*5+13* 69*41 ±3*02*
(no. = 32) (1090-2780) (28-37)Ventilator deaths 41:19 1495t 31* 12*8+2 3* 128*7+16*3t 32*7±0i9* 50*6±6 3* 88*72±1 46*
(no. = 60) (1020-2890) (27-37)Without BPD 22:9 1470 31 11*3±3*3 50*0±9 8* 30.7±1.0* 49*6±3*9 89*03±0*02(no. = 31) (1150-2807) (27-37)With BPD 19:10 1515 31 14-4+3-3 212-0±23-7* 34-8±1-5* 51-6±3-6 88-37±0-09
(no. = 29) (1020-2890) (27-36)
Note: Median values and ranges, or means and SE, are shown.MV, mechanical ventilation; PAP, peak airway pressure; f, respiratory frequency.*P <0-02,tP <0-0125,*P <0-001.
510

Improved prognosis of infants mechanically ventilatedfor hyaline membrane diseasearachnoid in 4, and into the brain substance in 1.Cerebral bleeding was also common in infants dyingwith bronchopulmonary dysplasia, being present in12 (46%) of the 26 necropsied infants. Separateintraventricular and subarachnoid haemorrhageswere present in 2 infants; isolated intraventricularhaemorrhages in 6, and isolated subarachnoidhaemorrhages in 2.
Comparison between 1969 and 1970. Theincrease in survival rate of ventilated infants, and thereduction in the incidence of bronchopulmonarydysplasia occurred between 1969 and 1970. Nofurther statistically significant changes took placeafter that year, in spite of continuing modificationsof treatment. We have therefore analysed in detailthe changes in ventilator management occurringbetween these 2 years.
The total number of infants admitted with severe
HMD was 22 in 1969 and 31 in 1970. The infants'sbirthweights in the 2 years (median 1690 g, range
1020-3200 g, and median 1710 g, range 1150-3350 g)and gestational ages (median 33 wk, range 27-37 wkand median 33 wk, range 27-39 wk) were similar, as
were the proportions of infants admitted from otherhospitals. The overall survival rate increased,however, from 50% in 1969 to 77% in 1970(P <0 05).The age of starting mechanical ventilation
(24 6±7.9 hr and 24 0±5 9 hr) and its duration(167-2±54-3 hr and 99-4±22 5 hr) were notsignificantly different in the 2 years. Table VIshows the proportion of infants ventilated, thesurvival rate, ventilator variables, and details ofoxygen therapy. 1 ventilated infant (8%) survived
in 1969, whereas 9 ventilated infants (56%) survivedin 1970 (P <0 005). Highly significant reductionsin peak airway pressure and respiratory frequencyoccurred between 1969 and 1970, but there were no
significant alterations in inspired oxygen concentra-tion on the ventilator, or in the number of infantswho breathed an inspired oxygen concentrationgreater than 80% for more than 100 hours, thoughboth tended to be less in 1970.
The number of ventilated infants who died is toosmall for statistical differences to be evident betweenthe 2 years, but it is noteworthy that, in 1969, 6(50%) out of 12 ventilated infants died frombronchopulmonary dysplasia, whereas the numberof deaths with this condition in 1970 was 3 (19%)out of 16 ventilated infants.
Follow-up. At ages between 1 and 7 years allexcept 2 of the surviving infants appear to beprogressing normally. These 2 infants, whoweighed 1090 and 1260 g at 28 and 30 weeks'gestation, have developmental and neurologicalhandicaps, 1 severe, and the other mild. Nosurviving infant has evidence of trauma to the upperairway or of pulmonary insufficiency.
DiscussionReasons for alterations in ventilator
management. The first aim of the alterations inventilator management which took place at the endof 1969 was to reduce the incidence of broncho-pulmonary dysplasia, which was killing many of ourventilated infants. Our preliminary pathologicalevidence tentatively implicating mechanical trauma
TABLE VIComparison of ventilator variables and oxygen therapy between the years 1969 and 1970
1969 1970 p
No. of infants treated by MV 12 16% of total with severe HMD 55 51 NSBirthweight (g) 1450 (1020-1700) 1470 (1150-2500) NSGestation (wk) 31 (27-34) 31 (28-37) NSSex ratio M:F 9:3 9:7 NSSurvived 1 (8%) 9 (56%) <0 005
Ventilator variablesPeak airway pressure (cmH2O) 31*8±1i 7 25 66±0*5 <0*001Peak airway pressure 935 cmH.0 (no. of
infants) 9 (75%) 2 (12%) <0-01Respiratory frequency (per min) 52*4±4*9 321 ±0*8 <0 001Inspiration: expiration ratio used to regulate
Pao, (no. of infants) 3 (25%) 16 (100%) <0-005Oxygen therapy
Inspired 02 concentration during MV (%) 84-50±0 05 79 06+0t05 NSInspired 0 concentration 380% for 9 100 hr
(no. of infants) 6 (50%) 5 (31%) NS
Note: Median values and ranges, or means and SE are shown.MV, mechanical ventilation.
511

Reynolds and Taghizadehto the lung, as well as oxygen toxicity, in thepathogenesis of bronchopulmonary dysplasia(Hawker et al., 1967) has subsequently beenamplified and is detailed elsewhere (Taghizadeh andReynolds, 1975). Two overlapping types of lesionswere identified. The first type was found whenpeak airway pressures of 35 cmH2O or more hadbeen used. Gross bronchial damage was present,and in the later stages there was marked hypertrophyof bronchial muscle. Peribronchiolar fibrosis wasconfined to the centre of the lobule without involve-ment of peripheral acini except in occasional caseswhere fibrosis replaced the whole of some lobules.The other type of lesion was associated with the useof very high inspired oxygen concentrations, usually100%, for 5 days or more. The changes in thebronchi were less marked, but subepithelialcongestion round air sacs, progressing later tofibrosis, was particularly obvious. Poorlybranching air sacs, variable in size, suggestedreduced alveolization. These changes could not bereliably separated from the repair processes of thelung, but some of them looked similar to the effectsof pulmonary oxygen toxicity in experimentalanimals (Robinson et al., 1967; deLemos et al.,1969).
Since the most severely damaging lesions, whichappeared early in the course of ventilator therapy,appeared to be associated with the use of high peakairway pressures and fast respiratory frequencies, wefirst tried to find means for ventilating the infants atlower pressures and lower frequencies. The use ofa slow respiratory frequency together with a longinspiratory phase in order to maintain alveolarinflation for a large part of each breath enabled us toventilate most infants at peak airway pressures ofabout 25 cmH2O, much less than had been ourprevious experience. Since the acute experimentswhich showed this technique to be effective inachieving good gas exchange at a low peak airwaypressure were performed in 1969, it was possible toadopt a new regimen of ventilator management fromthe start of 1970, when all infants were ventilated ata respiratory frequency of about 30/min, a peakairway pressure of about 25 cmH2O, and aninspiration: expiration ratio of 1:1 or more (TablesIII and VI). Initially, we continued to use veryhigh concentrations of oxygen, but subsequently,from the beginning of 1971, the effect of a longinspiratory phase in improving Pao2 was employedto reduce the inspired oxygen concentration to a lesstoxic level. Further developments since that timehave included the use of a positive end-expiratorypressure during ventilation, in order to retard orprevent alveolar collapse during expiration, and
the introduction of CPAP during spontaneousbreathing.
Change in survival rate. Criteria for thediagnosis of HMD vary widely in differentinstitutions, and figures for survival rate are verysensitive to the number of mildly affected infantsincluded in the analysis. Indications for initiatingmechanical ventilation also vary, so that a highventilator survival rate may merely reflect a lowthreshold for using this form of therapy. We havetherefore not attempted to compare our results withthose from other units. In order to find out if thesurvival rate of infants with HMD in our own unitchanged after the introduction of differenttechniques for mechanical ventilation, we adoptedstringent diagnostic criteria, and defined infantsmeeting these criteria as suffering from 'severe'HMD. A comparison was then made between the3 years which preceded and the 3 years whichfollowed this alteration in management.The overall survival rate of infants with severe
HMD was 55% in the first 3-year period, 1967-69,and 69% in the second period, 1970-72 (Table I).The survival rate of mechanically ventilated infantsincreased from 11% in 1967-69 to 49% in 1970-72(Table II). During 1970-72 only 3 infantsweighing more than 2000 g died from HMD (Fig.),2 of these also had severe rhesus isoimmunization(one ofwhom was born without a heart beat) and theother also had an intrauterine infection with Esch.coli.The increase in the survival rate of ventilated
infants cannot be attributed to a changingpopulation, since the birthweight, gestational age,sex ratio, and the number of admissions from otherhospitals did not differ significantly in the two 3-yearperiods (Table II). Also, the proportion of infantssubjected to mechanical ventilation was similar eventhough our indications for using this form oftreatment had relaxed slightly in the second period.Since the care of the infants was under the closesupervision of the same senior medical and nursingpersonnel throughout all 6 years, uniformity ofmanagement was assured.
Cause of death. Table IV shows that theincrease in survival rate of ventilated infants waslargely accounted for by a reduction in the pro-portion of infants dying with bronchopulmonarydysplasia. The high incidence of intraventricularhaemorrhage in infants who died with or withoutthis condition was similar to that described by others(Harrison, Heese, and Klein, 1968; Fedrick andButler, 1970).
512

Improved prognosis of infants mechanically ventilatedfor hyaline membrane diseaseReasons for increased survival rate and
reduced incidence of bronchopulmonarydysplasia. The increase in survival rate of ourventilated infants and the fall in the incidence ofbronchopulmonary dysplasia occurred at preciselythe time when we introduced our regimen forventilating the infants at low peak airway pressures,slow respiratory frequencies, and high inspiration:expiration ratios. An attempt to start a controlledtrial of our new methods for setting the ventilatoragainst the previous regimen was rapidly abandonedwhen it became clear that oxygenation could morereadily be achieved using the new technique, so thatwe cannot state with complete certainty that thealterations in ventilator management were definitelyresponsible for the improved prognosis of theinfants. Nevertheless, it is extremely difficult toattribute so sudden a change to anything else.
Since the increase in survival rate was largely dueto a reduction in the incidence of bronchopulmonarydysplasia, we believe that our hypothesis thatmechanical trauma is an important factor in thepathogenesis of this condition has received strongsupport. Most authorities have considered thatbronchopulmonary dysplasia was due largely to theuse of high inspired oxygen concentrations, but thecondition has yet to be described in infants who havenot been treated by mechanical ventilation, and thedifficulties of separating the effect of ventilation fromthe toxic effects of oxygen have repeatedly beenpointed out (Becker and Koppe, 1969; Pusey,Macpherson, and Chernick, 1969; Banerjee,Girling, and Wigglesworth, 1972; Mikity andTaber, 1973). By comparing data for the year 1969with 1970 (Table VI), it is apparent that our changein survival rate and incidence of bronchopulmonarydysplasia occurred in association with a reduction inpeak airway pressure and respiratory frequency, andbefore a significant reduction in inspired oxygenconcentration had been achieved. Further evidencesuggesting that oxygen breathing is not the mostimportant factor in the pathogenesis of broncho-pulmonary dysplasia comes from the finding that 7nonventilated infants in the present study breathedoxygen concentrations greater than 80% for 5 daysor more, yet made a rapid and complete recovery,whereas 6 ventilated infants breathing similarconcentrations of oxygen died at 5 days of age frombronchopulmonary dysplasia.Even though it seems likely from our data that
mechanical trauma to the lung is importantlyinvolved in the pathogenesis of bronchopulmonarydysplasia, there is little doubt that oxygen toxicityalso has a role in causing or exacerbating thecondition (Robinson et al., 1967; deLemos et al.,
1969; Stern, 1973). The fact that the survival ratein the last year of the study was the highest (15,63%, out of 24 ventilated infants survived and theoverall survival rate for infants with severe HMDwas 76%), and that there was only 1 death frombronchopulmonary dysplasia might suggest that thereduction in inspired oxygen concentration whichoccurred after 1970 was responsible. We cannot,however, be sure about this, particularly since otherimportant alterations in management took place atthe same time (Table III), including the use of apositive end-expiratory pressure as well as a highinspiration:expiration ratio for maintaining alveolarinflation, the introduction of CPAP duringspontaneous breathing, and the use of parenteralnutrition.We do not wish to imply that mechanical trauma
to the lung and damage due to breathing highconcentrations of oxygen are the only causes of lungfibrosis in mechanically ventilated infants. Wehave observed it in other infants usually born after28 weeks' gestation or less who have neededmechanical ventilation because of 'apnoea ofprematurity'. When ventilation was continued formany weeks at low airway pressures and low inspiredoxygen concentrations, some of these infantsdeveloped fibrotic lesions which seemed to be due touneven airways obstruction, possibly due toinspissated secretions, with consequent atelectasisand fibrosis.
Effect of steroids. The reason for undertakinga pilot study of the effect of cortisol on the mostseverely affected infants was that Liggins (1969) andothers (deLemos et al., 1970; Motoyama et al., 1971)had shown that steroids were capable of potentiatingsurfactant production in the lungs of fetal animals.It seemed possible that a similar effect might occurafter birth and diminish the length of time that theinfants were exposed to mechanical ventilation andoxygen breathing. Our failure to show any benefitfrom steroids is in keeping with the much largerstudy of Baden et al. (1972).
Place of mechanical ventilation in manage-ment of HMD. With recent advances in themanagement ofHMD, such as prenatal detection ofinfants at risk (Gluck and Kulovich, 1973) and thepossibility of the stimulation of surfactantproduction before delivery (Liggins and Howie,1972), together with the use of CPAP duringspontaneous breathing, it is very much hoped thatthe need for mechanical ventilation will steadilydiminish. Nevertheless, the most severely affectedinfants continue to require this form of treatment
513

514 Reynolds and Taghizadehand it is therefore important that methods ofventilation should be available which give a goodprospect of recovery without damage to the brain orlungs. The use of methods which allow the infantsto be ventilated at low peak airway pressures andoxygen concentrations below 100% seem to providesuch a prospect.
Intraventricular haemorrhage. Intraventri-cular haemorrhage is now the most important causeof death in our ventilated infants. Ifmethods couldbe developed for its prevention probably few but thevery smallest infants would die. An associationbetween the occurrence of intraventricularhaemorrhage and hypoxia is well known (Harrison etal., 1968; Fedrick and Butler, 1970), and the mostimportant part ofthe mechanism of the haemorrhagemay be that an asphyxial episode causes heart failurewith a large rise in venous pressure and rupture ofthe terminal vein, which is the usual site of bleeding(Cole et al., 1974). Very careful monitoring andmanagement aimed at the avoidance of any asphyxiawhether or not the infant is being treated bymechanical ventilation are likely to be the mostimportant means of preventing this type ofhaemorrhage.
We are grateful to Professors L. B. Strang and J. F.Smith for their help and encouragement, to the medicaland nursing staff of the Neonatal Unit for their devotedcare of the infants, and to Mr. C. M. J. Bright fortechnical assistance.
REFERENCESAdamson, T. M., Collins, L. M., Dehan, M., Hawker, J. M.,
Reynolds, E. 0. R., and Strang, L. B. (1968). Mechanicalventilation in newborn infants with respiratory failure. Lancet,2, 227.
Baden, M., Bauer, C. R., Colle, E., Klein, G., Taeusch, H. W., Jr.,and Stern, L. (1972). A controlled trial of hydrocortisone ininfants with respiratory distress syndrome. Pediatrics, 50, 526.
Banerjee, C. K., Girling, D. J., and Wigglesworth, J. S. (1972).Pulmonary fibroplasia in newborn babies treated with oxygenand artificial ventilation. Archives of Disease in Childhood, 47,509.
Becker, M. J., and Koppe, J. G. (1969). Pulmonary structuralchanges in neonatal hyaline membrane disease treated with highpressure artificial respiration. Thorax, 24, 689.
Blake, A. M., Collins, L. M., Durbin, G. M., Hunter, N. J.,MacNab, A. J., Reynolds, E. 0. R., and Sellens, G. (1973).Simplified mechanical ventilation for hyaline-membrane disease.Lancet, 2, 1176.
Blake, A. M., Collins, L. M., Langham, J., and Reynolds, E. 0. R.(1970a). Portable ventilator-incubator. Lancet, 2, 25.
Blake, A. M., Collins, L. M., Langham, J., and Reynolds, E. 0. R.(1970b). Clinical assessment of apnoea-alarm mattress fornewborn infants. Lancet, 2, 183.
Chernick, V., and Vidyasagar, D. (1972). Continuous negative chestwall pressure in hyaline membrane disease: one year experience.Pediatrics, 49, 753.
Cole, V. A., Durbin, G., Olaffson, A., Rivers, R. P. A., Reynolds,E. 0. R., and Smith, J. F. (1974). Pathogenesis of intra-ventricular haemorrhage in newborn infants. Archives ofDisease in Childhood, 49. (In the press.)
Cooke, R., Lunding, M., Lomholt, N. F., Yssing, M., Zachau-Christiansen, B., and Friis-Hansen, B. (1967). Respiratoryfailure in the newborn. Acta Paediatrica Scandinavica, 56,498.
Cumarasamy, N., Nussli, R., Vischer, D., Dangel, P. H., and Duc,G. V. (1973). Artificial ventilation in hyaline membranedisease: the use of positive end-expiratory pressure andcontinuous positive airway pressure. Pediatrics, 51, 629.
Daily, W. J. R., Sunshine, P., and Smith, P. C. (1971). Mechanicalventilation of newborn infants. Anesthesiology, 34, 132.
deLemos, R. A., Shermeta, D. W., Knelson, J. H., Kotas, R., andAvery, M. E. (1970). Acceleration of appearance of pulmonarysurfactant in the fetal lamb by administration of corticosteroids.American Review of Respiratory Diseases, 102, 459.
deLemos, R., Wolfsdorf, J., Nachman, R., Block, A. J., Leiby, G.,Wilkinson, H. A., Allen, T., Haller, J. A., Morgan, W., andAvery, M. E. (1969). Lung injury from oxygen in lambs: therole of artificial ventilation. Anesthesiology, 30, 609.
Fedrick, J., and Butler, N. R. (1970). Certain causes of neonataldeath. II. Intra-ventricular haemorrhage. Biology of theNeonate, 15, 257.
Gluck, L., and Kulovich, M. V. (1973). Fetal lung development.Current concepts. Pediatric Clinics of North Amnerica, 20, 367.
Gregory, G. A., Kitterman, J. A., Phibbs, R. H., Tooley, W. H., andHamilton, W. K. (1971). Treatment of the idiopathicrespiratory-distress syndrome with continuous positive airwaypressure. New England Journal of Medicine, 284, 1333.
Harrison, V. C., Heese, H. de V., and Klein, M. (1968). Intra-cranial haemorrhage associated with hyaline membrane disease.Archives of Disease in Childhood, 43, 116.
Hawker, J. M., Reynolds, E. 0. R., and Taghizadeh, A. (1967).Pulmonary surface tension and pathological changes in infantsdying after respirator treatment for severe hyaline membranedisease. Lancet, 2, 75.
Heese, H. de V., Harrison, V. C., Klein, M., and Malan, A. F. (1970).Intermittent positive pressure ventilation in hyaline membranedisease. Journal of Pediatrics, 76, 183.
Herman, S., and Reynolds, E. 0. R. (1973). Methods for improvingoxygenation in infants mechanically ventilated for severe hyalinemembrane disease. Archives of Disease in Childhood, 48, 612.
Linsao, L. S., Aharon, A., Levison, H., and Swyer, P. R. (1970).Negative pressure artificial respiration: use in treatment ofrespiratory distress syndrome of the newborn. CanadianMedicalJournal, 102, 602.
Liggins, G. C. (1969). Premature delivery of foetal lambs infusedwith glucocorticoids. Journal of Endocrinology, 45, 515.
Liggins, G. C., and Howie, R. N. (1972). A controlled trial ofantepartum glucocorticoid treatment for prevention of therespiratory distress syndrome in premature infants. Pediatrics,50, 515.
Mikity, V. G., and Taber, P. (1973). Complications in the treat-ment of the respiratory distress syndrome: bronchopulmonarydysplasia, oxygen toxicity, and the Wilson-Mikity syndrome.Pediatric Clinics of North America, 20, 419.
Motoyama, E. K., Orzalesi, M. M., Kikkawa, Y., Kaibara, M., Wu,B., Zigas, C. J., and Cook, C. D. (1971). Effect of cortisol onthe maturation of fetal rabbit lungs. Pediatrics, 48, 547.
Northway, W. H., Rosan, R. C., and Porter, D. Y. (1967).Pulmonary disease following respirator therapy of hyaline-membrane disease: broncho-pulmonary dysplasia. NewEngland Journal of Medicine, 276, 357.
Peterson, H. G., and Pendleton, M. E. (1955). Contrastingroentgenographic pulmonary patterns of the hyaline membraneand fetal aspiration syndromes. American Journal ofRoentgenology, 74, 800.
Pusey, V. A., Macpherson, R. I., and Chernick, V. (1969).Pulmonary fibroplasia following prolonged artificial ventilationof newborn infants. Canadian Medical AssociationJournal, 100,451.
Reynolds, E. 0. R. (1970a). Hyaline membrane disease. AmericanJournal of Obstetrics and Gynecology, 106, 780.
Reynolds, E. 0. R. (1970b). Indications for mechanical ventilationin infants with hyaline membrane disease. Pediatrics, 46, 193.
Reynolds, E. 0. R. (1971). Effect of alterations in mechanicalventilator settings on pulmonary gas exchange in hyalinemembrane disease. Archives of Disease in Childhood, 46, 152.

Improved prognosis of infants mechanically ventilatedfor hyaline membrane disease 515Reynolds, E. 0. R. (1974). Pressure wave-form and ventilator
settings for mechanical ventilation in very severe hyalinemembrane disease. International Anesthesiology Clinics. (Inthe press.)
Robinson, F. R., Harper, D. T., Jr., Thomas, A. A., and Kaplan,H. P. (1967). Proliferative pulmonary lesions in monkeysexposed to high concentrations of oxygen. Aerospace Medicine,38, 481.
Shaw, J. C. L. (1973). Parenteral nutrition in the management ofsick low birthweight infants. Pediatric Clinics of NorthAmerica, 20, 333.
Stahlman, M. T., Malan, A. F., Shepard, F. M., Blankenship, W. J.,Young, W. C., and Gray, J. (1970). Negative pressure assistedventilation in infants with hyaline membrane disease. journalof Pediatrics, 76, 174.
Stern, L. (1973). The use and misuse of oxygen in the newborninfant. Pediatric Clinics of North America, 20, 447.
Stern, L., Ramos, A. D., Outerbridge, E. W., and Beaudry, P. H.(1970). Negative pressure artificial respiration: use in treat-ment of respiratory failure of the newborn. Canadian MedicalAssociation journal, 102, 595.
Taghizadeh, A., and Reynolds, E. 0. R. (1975). Pathologicalchanges following mechanical ventilation for hyaline membranedisease. Submitted for publication.
Thomas, D. V., Fletcher, G., Sunshine, P., Schafer, I. A., and Klaus,M. H. (1965). Prolonged respirator use in pulmonary in-sufficiency of newborn. Journal of the American MedicalAssociation, 193, 183.
Correspondence to Dr. E. 0. R. Reynolds,Department of Paediatrics, University College Hospital,Huntley Street, London WC1E 6AU.
AddendumSince the completion of this study a further increase in
the survival rate of infants mechanically ventilated forHMD in our unit has occurred (Blake et al., 1973, Lancet,2, 1176.

本文献由“学霸图书馆-文献云下载”收集自网络,仅供学习交流使用。
学霸图书馆(www.xuebalib.com)是一个“整合众多图书馆数据库资源,
提供一站式文献检索和下载服务”的24 小时在线不限IP
图书馆。
图书馆致力于便利、促进学习与科研,提供最强文献下载服务。
图书馆导航:
图书馆首页 文献云下载 图书馆入口 外文数据库大全 疑难文献辅助工具