IMPAIRMENT OF PHONETIC READING IN DYSLEXIA AND ITS PERSISTENCE BEYOND CHILDHOOD—RESEARCH NOTE
18
/. Child P^yM. P>Mkl. Vnl, 23, Nc. 4. pp. 459-475, 1982. TO21-9630/8'2/U4O159-17 |(i:i.0O/U Ptint"! inCreai Brilain. Pcrsanum Press Ltd. © 1982 Assmiaiiuri lur Ghild Psyihology and Paythiatr), IMPAIRMENT OF PHONETIC READING IN DYSLEXIA AND ITS PERSISTENCE BEYOND CHILDHOOD—RESEARCH NOTE GERALD Ru.ssELL Department of Psychiatry, Institute oi Psychiatry, University of London, London, England INTRODUCTION IN A previous review of the history of writing, it was shown that over the course of some 3500 years, most forms of writing developed along a similar pathway. There was a gradual simphfication ofthe graphic symbols and they became progressively more phonetic in their representation (Russell, 1982). As the written seripts came to represent more faithfully the sounds ofthe spoken language, there is evidence that reading and writing became more widely available to the masses of the people. It was therefore postulated that as the wider dissemination of writing was dependent on its progressive phonetisation, the latter was a process which was adaptive to man's cognitive and linguistic abilities. While this process was generally an adaptive one, it was further postulated that for a minority of children the decipherment of a highly phonetic script would present unusual obstacles, with the result that they would find learning to read an impossible or extremely arduous task. They would be the children who suffer from reading disorders. The aim of this study is to test the hypothesis that dyslexic subjects find it difficult to process spoken sounds, and that this difficulty contributes to their reading disorder. In recent years, enquiries into the nature of reading disorders have veered towards a closer examination of the operation of reading itself and the linguistic abilities of dyslexic subjects. This is in contrast with earlier approaches. The first reports of children with inexplicable reading difficulties spoke of an underlying 'derangement of visual memory' and proposed the descriptive term 'congenital word blindness' (Pringle Morgan, 1896; Hinshelwood, 1895, 1917), a term which has persisted until recently (Lancet, 1966). In the absence of evident structural cerebral changes, Critchley (1970) put forward a developmental delay or 'maturational lag' of a functional nature, and favoured the terms 'developmental dyslexia' or 'specific dyslexia'. There has also been a long-standing debate on the contribution of uncertain cerebral dominance to reading disorders, a concept of direct relevance because of hemispheric specialisation for language. The origin of this concept goes back to Orton (1937), who was more concerned with the possible interference between oppositely oriented engrams in the two hemispheres as an explanation for the disabled readers' proneness to mistake some letters for their mirror images (e.g. b for d, and Based on an Inaugural Lecture at the Institute of Psychiatry, London: 16 January, 1980. Requests for reprints to: Professor Gerald Russell, Department of Psychiatry, Institute of Psychiatry, De Crespigny Park, Denmark Hill, London SE5 8AF, England. Accepted manuscript received 2%July 1981 459
-
Upload
gerald-russell -
Category
Documents
-
view
216 -
download
0
Transcript of IMPAIRMENT OF PHONETIC READING IN DYSLEXIA AND ITS PERSISTENCE BEYOND CHILDHOOD—RESEARCH NOTE

/. Child P^yM. P>Mkl. Vnl, 23, Nc. 4. pp. 459-475, 1982. TO21-9630/8'2/U4O159-17 |(i:i.0O/UPtint"! inCreai Brilain. Pcrsanum Press Ltd.
© 1982 Assmiaiiuri lur Ghild Psyihology and Paythiatr),
IMPAIRMENT OF PHONETIC READING IN DYSLEXIA AND ITSPERSISTENCE BEYOND CHILDHOOD—RESEARCH NOTE
GERALD Ru.ssELL
Department of Psychiatry, Institute oi Psychiatry, University of London, London, England
INTRODUCTION
IN A previous review of the history of writing, it was shown that over the course ofsome 3500 years, most forms of writing developed along a similar pathway. Therewas a gradual simphfication ofthe graphic symbols and they became progressivelymore phonetic in their representation (Russell, 1982). As the written seripts came torepresent more faithfully the sounds ofthe spoken language, there is evidence thatreading and writing became more widely available to the masses of the people. Itwas therefore postulated that as the wider dissemination of writing was dependent onits progressive phonetisation, the latter was a process which was adaptive to man'scognitive and linguistic abilities. While this process was generally an adaptive one, itwas further postulated that for a minority of children the decipherment of a highlyphonetic script would present unusual obstacles, with the result that they wouldfind learning to read an impossible or extremely arduous task. They would be thechildren who suffer from reading disorders. The aim of this study is to test thehypothesis that dyslexic subjects find it difficult to process spoken sounds, and thatthis difficulty contributes to their reading disorder.
In recent years, enquiries into the nature of reading disorders have veered towardsa closer examination of the operation of reading itself and the linguistic abilities ofdyslexic subjects. This is in contrast with earlier approaches. The first reports ofchildren with inexplicable reading difficulties spoke of an underlying 'derangementof visual memory' and proposed the descriptive term 'congenital word blindness'(Pringle Morgan, 1896; Hinshelwood, 1895, 1917), a term which has persisted untilrecently (Lancet, 1966). In the absence of evident structural cerebral changes,Critchley (1970) put forward a developmental delay or 'maturational lag' of afunctional nature, and favoured the terms 'developmental dyslexia' or 'specificdyslexia'. There has also been a long-standing debate on the contribution of uncertaincerebral dominance to reading disorders, a concept of direct relevance because ofhemispheric specialisation for language. The origin of this concept goes back toOrton (1937), who was more concerned with the possible interference betweenoppositely oriented engrams in the two hemispheres as an explanation for the disabledreaders' proneness to mistake some letters for their mirror images (e.g. b for d, and
Based on an Inaugural Lecture at the Institute of Psychiatry, London: 16 January, 1980.Requests for reprints to: Professor Gerald Russell, Department of Psychiatry, Institute of Psychiatry,De Crespigny Park, Denmark Hill, London SE5 8AF, England.
Accepted manuscript received 2% July 1981
459

460 G. RUSSELL
p for q). Belmont and Birch (1965) could not find a higher frequency of mixedcerebral dominance as judged by preferred hand- or eye-usage. More relevant to thecerebral lateralisation of spoken language, however, is the determination of ear-preference by the technique of dichotic auditory stimulation which has revealed left-ear preference in dyslexic children more frequently than in normal readers (Sparrowand Satz, 1970; Thomson, 1976). A mismatching between hemispheric specialisationfor language and structural asymmetry of cerebral hemispheres has been suggestedfrom the application of computerised brain tomography. This technique has revealeda tendency for dyslexic subjects to show a reversal ofthe pattern of cerebral asym-metry found in normal right-handed subjects (Hier et ai, 1978). More direct, butvery tentative, evidence of structural abnormalities in Wernicke's auditory speecharea has come from a single post-mortem examination of a dyslexic subject(Galaburda and Kemper, 1979).
More pertinent to the present study are the contributions from educational psycho-logy and linguistics. Credit should go to Elkonin (1963, 1973) for his originalresearch into the operation of reading. He proposed that the basis of successful readingof an alphabetical writing system is the analysis ofthe sound formation of words, nomatter how the written word is perceived visually. Before learning to read, a childshould be able to discriminate auditorily between the basic sound units of language(phonemes). Whereas the child will easily divide words into syllables (units ofpronunciation), he will find it more difficult to analyse words into their separatephonemes. He should learn how language is constructed frt>m these sound unitsbefore learning the alphabetical characters as symbols for sounds. Elkonin views thewritten word not as a symbol but as a model ofthe sound form ofthe word: readingis thus the creation of the sound form of the word according to its graphic model.
Mattingly (1972) regarded reading as a language-based skill, written language beingessentially moulded on the spoken sounds. He also quotes Liberman as observing that"reading is parasitic on language" (in Kavanagh, 1968). Reading is hard whencompared with listening: it has to be deliberately acquired and is dependent onwhat he calls "the speaker-hearer's linguistic awareness". By this, he means theawareness of certain aspects of linguistic activity, associated with an internal imageof utterances which owes more to the phonological than any other level of represen-tation. When we read we rely on this awareness to synthesise actively the linguisticprocess common to both reading and speech, thus enabling us to understand themeaning of the written text. Shankweiler and Liberman (1976) also speak of theprimacy of spoken language and the derivative nature of reading and writing. Theystress that children need to acquire an explicit knowledge ofthe phonetic structure ofboth the spoken and the written word to enable them to establish a link betweenalphabetical symbols and spoken sounds: "the phoneme is the principal point atwhich the writing system meshes with the reading system." Reading disorders maythus result from a defective appreciation of the phonetic structure of language,this failure occurring at a relatively high level of linguistic processing. In contrast,a more basic impairment of auditory discrimination of spoken sounds has beenproposed by Wepman (1961), such as difficulty in distinguishing between 'cat' and'cap', which he found to be associated with lower reading attainments. This work

IMPAIRMENT OF PHONETIC REAfJING IN DYSLEXIA 461
has been criticised by Vellutino (1979), who has suggested that poor readers maybe able to identify similar words presented as wholes, and yet be less aware of theirphonetic structure than normal readers.
The aim ofthe present study was to find out whether a defect in the processingof spoken sounds could be demonstrated in dyslexic subjects. It was decided to testthe general hypothesis that a disorder of spoken language underlies dyslexia, so thatno attempt was made to distinguish between auditory discrimination and thesegmentation or encoding of phonemes. The subjects were a carefully-definedgroup of adolescents and adults who had been diagnosed as suffering from a dyslexiclearning disorder in childhood. This approach provided an opportunity to ascertamwhether a linguistic deficit underlying the reading disorder persists into adulthood,even though the subject eventually attains an improved or even a normal level ofreading.
DIAGNOSTIC CRITERIA
For the purpose of this article, the term "dyslexia" will be used as descriptive ofadisorder of reading. [It should be distinguished from "deep dyslexia", applicableonly to a special type of acquired loss of reading in brain-injured patients (Marshalland Newcombe, 1980).] The term carries no special precision so that it is necessaryto specify the criteria for the inclusion of patients in the present study.
The essential criteria on initial clinical presentation ofthe child were as follows:(1) evidence of a learning disorder of reading with a reading attainment falling at
least 2 years below that expected by virtue of age and I.Q..;(2) a learning disorder of spelling so that the spelling age is even lower than the
reading age;(3) the absence of any evident basis for difficulties in learning, such as deafness,
blindness, cerebral injury, social deprivation, emotional disturbance, pooreducational opportunity or mental handicap.
An additional useful criterion provided on follow-up of the child is evidence thathe lags persistently behind in learning to read and spell.
Supportive criteria which are not always present are:(1) an additional developmental or learning disorder (e.g. retarded speech,
dyscalculia or right-left confusion);(2) a family history of learning disorders.
THF PATIENT SERIES
Sixteen dyslexic patients (15 male and 1 female) who had all been examined bythe author were included in the study. They fell into two groups (Table 1). Group Iconsisted of the first 10 patients who had been seen as children at ages rangingfrom 7.7 to 12.5 yr. Their progress had been monitored at regular intervals, andwith the sole exception of patient 10, their reading improved steadily. They werefinally reassessed after a follow-up which varied from 4.7 to 15.4 yr after the initialassessment, by which time their ages ranged from 14.1 to 23.2 yr. The remaining

462 G, RUSSELL
(yQZ<uO<oz
ua.
w'0<ozS<
oz
oXtJ
T)
ted
u
redi
a."auuu ^^
<
>M
nf
u
feera
. .
u bo" C-H-5cC0
ua
c
u
—
+- ^^
O "u
1 ^
Q "
(N CO CN CO
CO ^p o Tt-CO o c^ CO
CM
CO
CM
O
ID
CO
eo •X)
CM
CM
oCO
eo
Ol
(M
CO
•>*•
—
CM
en
en r -
CT) —
t^ in
t~' eoeo —
•n—
o
•.oCO
17
o•n
17
eoo
63
+ + + +
^ -p
t o
o3
uco
ra fljo C
ow c ^—'C O <U
0
S'TJ T) ^ .yC a; D i l _
^ c c J2 ^I; ra 'cB 3 >O « . ; O tin0 0 O

IMPAIRMENT OF PHONETIC READING IN DYSLEXIA 463
6 patients who formed Group II (patients 11-16) were first seen and included in thestudy when they were older, so that in their case there had been no opportunity ofmaking prior observations. The ages of patients 11-15 ranged from 14.0 to 21.3 yr.Patient 16 was much older (63.8 yr) and for this reason he will not be included in thecalculations of means, nor in the comparisons with control subjects.
Table 1 shows the relevant data on all 16 patients, including social class (accordingto the Registrar-General's Classification), and I.Q. Reading and spelling ages arealso shown. For Group I patients, two sets of data are presented: those obtainedon initial assessment and fmal retesting. All patients had a severe spelling disorderinitially found on clinical testing and confirmed by standard spelling tests on thefinal assessment. For Group II patients, the data obtained at the time ofthe presentstudy are shown. Seven patients (5, 6, 8, 9, 11, 13 and 14) had an earlier historyof speech disorder, most often described by the parents as a persistence of baby-talk, a lateness in speaking distinctly and a muddling of syllables. Four patients(6, 8, 10 and 16) had also experienced severe difficulties in learning arithmetic andin memorising multiplication tables. They were considered to be examples ofdevelopmental dyscalculia (Slade and Russell, 1971). A positive family history ofreading or spelling difficulties was elicited among the first-degree relatives of sevenpatients (1,2, 5, 6, 10, Hand 16).
The availability of the earlier estimates of reading age in the 10 patients of Group Iallowed a comparison to be made with the reading ages that would have beenpredicted in normal children. This can be done by applying the statistical techniqueof regression analysis, which predicts the reading age to be expected in a normalchild according to his actual age and level of intelligence (Yule, 1967; Fransella andGerver, 1965). The multiple regression equations calculated by Fransella andGerver were more readily applicable to the present study because they cover a widerage range of children. The predicted normal reading ages thus calculated are shown inTable 1. By subtracting from these values the reading ages actually achieved, adiscrepancy was obtained which gave a measure of the severity ol each child'sreading disability when originally assessed (Table 1). This discrepancy ranged from23 to 70 months ( = Index of Severity 1 in Table 1). The regression analysis couldonly be applied to patients in Group I owing to the unavailability of regressionequations in the older age group.
REPRESENTATIVE CASE SUMMARIESPatient 6
Thi.s boy's parents first sougbt help when he was aged 8 and making little progress with reading andspelling. His speech had previously been indi.stinct but improved by the time he started school at 5.Remedial teaching was provided from the age of 9. At school he tended to be disobedient and aggressivetowards other boys. He was slow in learning to tie his shoe laces and could not tell the time till he was101/2. At 12 !4 he read in a slow and halting manner. Reading errors included 'was' instead of 'as'and 'excellent' instead of 'exciting'. He spelt 'hows' for 'house' and 'hospel' for 'hospital'. He waspoor at simple arithmetic and had only learned the two-times multiplication table. He muddled thepoints of the compass. His father had been a poor speller. The estimates of this boy's I.Q., readingand spelling ages when he was 8 yr 11 months and 19 yr 5 months are shown in Table 1. He succeededin passing only two 'O ' level examinations at 15J4 . He returned to his studies later, however, and at 19passed six additional 'O ' grade examinations bul again failed in English language. When last seen hewas due to commence an engineering course at a technical college.

464 G RUSSELL
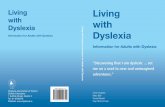
Patient 8
This boy's difficulties had been noted from the age of 3, when his speech had remained baby-likeand indistinct. He was given speech therapy and by the age of 6 he had improved considerably.Throughout his schooling he experienced considerable difficulties with reading, spellitig and arith-metic, in spite of assiduous efTorts on his part and that of his teachers, remedial teachers and mother.Figure 1 shows serial estitnates of reading age from 7K yr of age. His initial severe delay in readingpersisted until the age of 11; thereafter, he made more rapid progress, possibly as a result of theconsiderable remedial teaching provided. By the age of 17 he reached a reasonably normal readingage of over 15 yr. When last tesled he was able to read most words on the Schonell Graded WordReading Test, including phonetically ambiguous words such as 'sepulchre' and 'metamorphosis'.He achieved this by recogni.sing words with whose meanings he was already familiar. His arith-metical difficulties persisted, but he succeeded in passing 5 ' C level and one 'A' level examinations.He coped successfully with his work as a clerical officer and depended on a pocket calculator whencarrying out computations.
FIG. 1. Follow-up of dyslexic subject (patient
CONTROL SUBJECTS
The controls were 18 normal subjects (17 male and 1 female), most of whom werevolunteers from the sixth forms ofa private and a comprehensive school. Table 2shows close matching for age, I.Q. (progressive matrices) and social class. The shghtbias in age and I.Q. which might have favoured the normal control subjects towardsa better test performance would perhaps be counterbalanced by the social classdistribution which was slightly favourable to the dyslexic patients.
T.\BLE2. MATCHING OF DYSLEXIC PATIENTS AND NORMAL CONTROLS
Sex Age I.Q.M F (Mean ± SD) (Mean ± SD) I
Social classII III IV V
Dysiexics
Normals
14
17
1
I
17.4(± 2.68)
18.2(± 1.80)
114.2(± 12.95)
118.8(± 10.57)
3

IMPAIRMENT OF PHONETIC READING IN DYSLEXIA 465
METHODS
7>j( of phonetic reading and writingA dual test of phonetic reading and writing v/as devised in order to detect possible defects in the
proces.sing of spoken sounds in dyslexic patients. No attempt was made to distinguish betweenindividual processes such as auditory discrimination, segmentation into separate phonemes ur encodingbetween alphabetical symbols and spoken words. The phonetic test differs from standard reading andwriting tests in being independent of previous knowledge of the meaning of words and the vagaries ofnonphonetic spellings.
The dual phonetic test was therefore constructed from meaningless 'words' of graded complexity.These 'words' were to be read and written with the maximum degree of phonetic fidelity. The 'rules'of pronunciation were those of standard English but were more clearly defmed in order to overcomephonetic ambiguities and allow for past exposure to different teaching methods. In particular, thevowel sounds were clearly defined and used consistently throughout the test. The following 'rules' forthe pronunciation of vowels were accordingly laid down tor the test:
a as in cat, strt0 as in bow, polo1 as in pm, szt, lim/te as in mm, bHl, v,e\ec\.u as in put, bull, bush.
Each vowel was thus restricted to one sound so as to avoid the common ambiguities of English. Thesound of the vowel 'u' was the only slightly unusual one but was chosen to avoid the diphthong sound'iou'. Consonant sound.s produced fewer problems and were confined to those corresponding to theletters B, D, F, G, K, L, M, N, P, R, S, T and V. Y was also omitted. The test itself consisted of 60meaningless words in six sets often. Each set is typified by the following 'words': KAM, AKO, KALOB,NALOPUT, ALOBI, ANEKOBI. Thus there was a progression from one to four syllables. Eachletter was used a balanced number of times (30 times for each vowel, 13 or 14 for each consonant).
The writing part ofthe phonetic test was administered first; the 60 'words' were each slowly read outtwice, and the subject was asked to write them on cards according to the above phonetic rules. Thereading part of the test was administered second: the subject was asked to read the same sets of meanmg-less words using the same rules of pronunciation. This order was chosen so as to give the subjects themaximum possible amount of practice before trying the reading test, which was considered the moreimportant ofthe two.
The phonetic test was administered to all dyslexic patients and control subjects in a standardisedmanner, using an audio-tape listened to through earphones. The tape consisted of ihree parts —instructions, a period of practice and the writing test itself. The instructions explained the phoneticrules, which were aiso written on a card which the subject couid refer to during the test. A generousperiod of reading practice was given with a different set of 20 meaningless words {e.g. KAP, AKO),until the subject showed that he understood the phonetic rules and read these simpler 'words' correctly.The writing tests proper consisted of 60 trial 'words'. Each 'word' was sounded twice, allowing sufficienttime for the subject to write it down. The reading test followed the writing test and the subject's per-formance was audio-taped. Each subject's reading tape was scored independently by two raters, aswere the cards on which the subjects had written the meaningless words. For scoring purposes, it wasagreed beforehand that C and K were equivalent. Similarly, a spelling of OU or OO for 'U' wasaccepted. On the other hand, the addition of unsounded vowels was scored as wrong. The phoneticreading and writing tests were scored according to the correct number of words read or writtenrespectively out ofa possible 60. Inter-raier reliability was found to be very high: for the reading test,r = 0.98 (d.f. = 32); for the writing test, ^ = 1.0 (d.f. = 34).
AudiometryAudiometry was performed on as many dyslexic patients as possible (l-IO). It was important to rule
out possible defects of hearing because congenital deafness usually prevents the attainment of morethan a basic level of reading (Conrad, 1977), and impaired hearing would interfere with thephonetic test itself.

466 G. RUSSELL
Standard reading and writing tests
The Schonell Graded Word Reading Test was selected because its results could more readily becompared with previous testing at an earlier age. In order to assess reading age, the revised normspublished by Schonell and Goodacre (1974) were used for children aged up to 12 yr; for older childrenthe corrected standards published by the Ministry of Education (HMSO, pamphlet No. 18) wereemployed. The Schonell Graded Word Spelling Test was used to assess spelling age (Schonell andSchonell, 1960).
Intelligence testingI.Q. results were available on all the dyslexic patient.s in Group I from tests performed when they
first presented at a young age, using the Wechsler Intelligence Scale for Children in its full or shortenedform. They were all retested on follow-up for inclusion in the present study, as were the Group IIdyslexic patients and the normai control subjects, using Raven's Progressive Matrices.
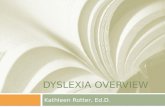
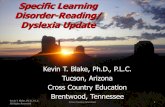
Test of visual discriminationThe 15 dyslexic patients and 18 normal contnjl subjects were given the test of visual discrimination
devised by Slade (personal communication) (patient 16 was excluded because of his age). This test isbased on the old observation that dyslexic children tend to confuse letters that are mirror images of eachother. It consists of 8 lines containing the letters b and d randomly arranged: the first two lines consistof single letters, the next two of paired letters, the next two of 3-letter sets and the last two of 4-lettersets. Figure 2 shows half the combinations of letters. The subject was asked to underline the ]etter(s)in each line as indicated by the underlined key on the left of each line. The test was scored by countingthe number of errors tor each subject.
Visual Discrimination Test
d b d b b d d b d
db db bd bd bd db bd db bd
dbd dbb bbd bdb dbd ddb dbd bdd bdb
dbbd dbdb dbbd bddb dbdb bdbd dbbd dbdb bbdd
FK;. 2. (This figure shows half the test letters presented during each test.)
RESULTSPhonetic reading
Table 3 shows the results obtained in the dyslexic patients and the normal subjects.The Schonell test of reading is scored out of 100 and the results were used to derivethe reading ages shown in Table 1 (on final testing). The phonetic test of reading isscored out of 60. Although the test of phonetic reading differed from standard testsof reading in not being tied to the meaning of words or to the caprices of Englishorthography, the two types of test would have components in common, namely theapplication of linguistic processes to reading. A positive correlation between thescores obtained using both tests in each subject would therefore be expected to theextent that they share these linguistic processes. A positive and significant correlationwas indeed found between the scores obtained with the phonetic and the Schonellreading tests, both in the dyslexic patients (r = +0.66; d.f. = 14;/*< 0.01) and inthe normal subjects (r = +0.77; d.f. = 16;/ '< 0.001).

IMPAIRMENT OF PHONETIC READING IN DYSLEXIA 467
BO
o
-c r*
if
D -5
a.so

468 G. RUSSELL
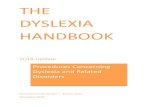
Validity and diagnostic value of the phonetic reading test. The validity of the phoneticreading test can be assessed from its ability to distinguish between dyslexic patientsand normal controls. Would the phonetic test be as useful or even more useful inseparating these two groups than the standard Schonell reading test? Both readingtests were capable of distinguishing between the dysiexics and the controls, as isshown in Fig. 3. The differences between mean scores obtained by dysiexics andnormals were examined by Mests, firstly on the Schonell reading test and secondlyon the phonetic reading test. The differences turned out to be highly significant(Schonell:/ = 4.42; d.f. = 31; / '< 0.001; phonetic: / = 6.01; d.f. - 31;/*< 0.001).In order to compare the diagnostic value ofthe two reading tests, a linear discriminantfunction analysis was carried out. Relying only on the Schonell reading test, 84.8%of total subjects (dysiexics and controls) would be correctly assigned to their respectivediagnostic categories. Relying only on the phonetic reading tests, 87.9% of totalsubjects would be correetly assigned. The difference in the relative diagnosticvalue of the two tests is due to only one subjeet. In faet, the phonetic test failed todetect 3 dyslexic patients and wrongly assigned one control subject. The Sehonelltest failed to detect 2 dyslexic patients and wrongly assigned three control subjects.The errors obtained with the Schonell test would therefore be more serious clinically.The results of this analysis indicate an advantage for the phonetic reading test, butthe small size ofthe groups makes it necessary to interpret this finding with caution.
READING TESTS% score1O0 u
0 0 0 0 0 Cf 00
I
controls1
*
1j
dysiexics2
o o
0 O
0oo o
o
o ooo
controls3
•
t
• • • aI
d v s l e x i c s4
% score100
SCHONELL. PHONETIC
FIG. 3. Pcrceniage scores on reading tests (Schonell and phonetic) in controls (! and 3) and dysiexics(2 and 4).

IMPAIRMENT OF PHONETIC READING IN DYSLEXIA 469
Impairment of phonetic reading: an enduring measure of severity of dyslexia. It is apparentthat when dyslexic patients grow up, most of them can achieve a level of readingwhich is normal or close to normal when measured on standard tests such as theSchonell. The question arises whether this represents a gradual neuro-linguisticmaturation or is the result of persistent effort on the part of the patient and histeachers. It was shown in Fig. 3 that the phonetic reading test in the dyslexic patientsresults in a wider separation of scores than the Schonell reading test. It would beuseful to examine whether the scores on the phonetic reading test grade thedyslexics according to the severity of the neuro-linguistic defect underlying thedisorder. This was examined by comparing these scores with the index of severity ofthe dyslexic disorder when the patients first presented, shown in Table 1 and explainedin The Patient Series. A correlation was therefore sought between the index ofseverity and the score on the phonetic reading test: it was found to be statisticallysignificant (r = 0.75, d.f. = 8; P< 0.01). In contrast, a lower and non-significantcorrelation coefficient was obtained when a similar comparison was made betweenthe severity of the dyslexia assessed in childhood and the score on the Schonellreading test obtained at follow-up (r = 0.51;d.f. = 8; / '> 0.05).
Inevitably, these comparisons could only be made on the ten dyslexic patientswho had been Ibllowed up from childhood to adolescence or adulthood. In order toincrease the size of the sample, another comparison was made including the sixdyslexic patients in Group II who were only identified and tested when they wereolder. As a multiple regression analysis cannot be applied to them, a difierentmethod must be chosen to assess the severity of their dyslexia. This was takensimply as the discrepancy between their age (or a ceiling of 19 if over that age)and their reading age. A correlation was again sought between this composite indexof severity of dyslexia and the score on the phonetic reading test. Again, it wasfound to be statistically significant (r = 0.64; d.f. - 14;/*< 0.005).
These findings confirmed the value ofthe phonetic reading test in measuring thedegree of severity of the neuro-linguistic defect underlying the reading disorder andits superiority over the Schonell reading test.
Relevance of a history of delayed speech development. There was no discernable associationbetween low scores on the phonetic reading test and a previous history of delayedspeech in early childhood.
Phonetic writingTable 3 again shows the results obtained in the dyslexic patients and the normal
subjects. The Schonell writing test is scored out of 100 and the results were usedto derive the spelling ages (Table 1, on final testing). The phonetic writing test isscored out of 60. A correlation was sought, as with the reading tests, between thescores on the Schonell and phonetic writing tests administered to each subject. Itwas thought that a positive correlation would indicate the degree to which the twotests shared the assessment of common linguistic processes. The correlationcoefficient found in the dyslexic patients was low and not significant (r = 0.33;d.f. = 13; P > 0.05); it was rather higher and just significant in the normal subjects(r = 0.53; d.f. = 16; PK 0.05). This result suggests that the Schonell and phoneticwriting tests are examining mainly different linguistic processes.

470 G. RUSSELL
Validity and diagnostic value of the phonetic writing test. The capacity of the phoneticwriting test to distinguish between dyslexic patients and normal subjects wasexamined and compared with that of the standard Schonell spelling test. Withboth tests, a significant difference was found between the mean scores obtained bydyslexics and controls (Schonell:^ = 8.49; d.f. = 31; P < 0.001; phonetic; / = 5.47;d.f. = 31, P< 0.001). Figure 4 shows, however, a clear separation of scores betweendyslexics and controls on the Schonell spelling test, but some overlap on the phoneticwriting test. In order to examine the diagnostic value of the two writing tests, alinear discriminant function analysis was carried out. The Schonell writing test wascapable of correctly assigning 97.0% of total subjects (dyslexics and controls) to theirrespective categories. On the other hand, the phonetic writing test assigned only78.8% of total subjects. The Schonell writing test failed to detect only one dyslexicsubject and could therefore be said to have high diagnostic value.
% scoretoo
WHITING TESTS
controls dyslexics
% score100
• •oo oo oo
a o
controls dyslexics
SCHONELL PHONETIC
FIG. 4. Percentage scores on writing (spelling) tests (Schonell and phonetic) in controls (I and 3) anddyslexics (2 and 4).
Comparison of performance on writing tests and severity of dyslexia. The potential value ofthe phonetic writing test in grading dyslexic patients according to the initial severityof their neuro-linguistic defect was examined in the same way as with the phoneticreading test. A correlation was sought between the index of severity (Table 1) and thescores obtained on each writing test in turn. This time the correlation between thephonetic writing test and the index of severity was found to be low and only just

IMPAIRMENT OF PHONETIC READING IN DYSLEXIA 471
significant (r = 0.55; d.f. = Q, P < 0.05). In view ofthe small size ofthe group,this result must be interpreted with caution. Moreover, when a correlation wassought between the scores on the Schonell spelling test and the index of severity,a very low coefficient was obtained which was not significant (r = 0.16; d.f. = 8;P > 0.05). These findings suggest that the phonetic writing test may be of somelimited value in measuring the neuro-linguistic detect in older dyslexics, but it is ofless value than the phonet'ic reading test. Considering the results ofthe reading andwriting tests together, it can be concluded that an impairment in the phonologicalaspects of reading and writing (especially the former) is an enduring measure oftheseverity of the dyslexia. This continues to be true even in adolescent and adultsubjects in whom the standard test of reading (Schonell) has lost its usefulness inmeasuring the severity of the dyslexia in its earlier stages. The standard (Schonell)spelling test retains its diagnostic value but is not a good indicator of the severityofthe reading disorder.
AudiometryThe ten dyslexic patients in Group I who had their hearing tested by audiometry
included six dyslexic patients with markedly impaired performance on the phoneticreading and writing tests (patients 3, 5, 7, 8, 9 and-10). In only one of these(patient 9) was there an abnormal result, with an apparent bilateral reduction ofauditory acuity throughout the range of frequencies. He had been examined at theRoyal National Throat, Nose and Ear Hospital at the age of six and it was concludedthat his hearing was normal. Subsequent examinations led to variable results. Theexpert opinion (provided by Dr. J. A. M. Martin) was that there was no significanthearing loss and that the variable results might be psychogenic or possibly secondaryto a 'language disorder'. Thus, in none of these dyslexic patients was thereevidence of reduced hearing to account for the impaired reading and writing tests.
Visual discriminationThe average number of errors committed by 15 dyslexic patients was 1.9 and by
17 normal controls, 2.1. The proportion of subjects who made at least one error wasalso compared: for the dyslexic patients it was 10/15 and for the normal controlsit was 12/17. Whichever way the performance of the two groups is compared,there is no significant difference between the dyslexics and the control subjects.
DISCUSSION
The present study was conducted on a series of patients suffering from dyslexiawho met defmed criteria ofthe disorder. The dyslexic patients who first presentedin childhood were followed up for an average period of over 7 yr, when it was foundthat six out of ten of them had attained a fair degree of reading proficiency. Theirreading attainment at follow-up was indeed so good that it was difficult to confirmthe previous diagnosis with the Schonell reading test. It was then that the phoneticreading test, specially devised for this study, proved its usefulness. This test aimedat assessing particularly the perception and/or processing of spoken sounds, andreduced to a minimum any dependence on the meaning of words or the perception

472 G. RUSSELL
of visual patterns. Even at the end of follow-up, performance on the phoneticreading test continued to mirror the severity of the dyslexic disorder as initiallyascertained in childhood. When it came to examining the relative diagnostic meritsofthe writing tests the position was reversed; the Schonell spelling test had greatervalue than the phonetic writing test in discriminating between dyslexics and normalreaders. The impairment ofthe phonetic processes which has been demonstratedin the dyslexic patients could not be ascribed simply to a peripheral defect of hearing.Neither could a simple relationship be established between a delay in speech develop-ment and the severity of the child's dyslexic disorder. A test of visual perceptionfailed to separate the dyslexic patients from the normal subjects.
The fmdings ofthe present study confirm recent researches into the perceptual,cognitive and linguistic functions of poor readers and dyslexic patients. Vellutinoet al. (1972) tested the performance of poor readers in copying and reading frommemory non-verbal and verbal stimuli presented by brief tachistoscopic exposure.They found that the performance of poor readers was similar to that of normalreaders with the non-verbal stimuli, but inferior with verbal stimuli. Vellutino (1979)also showed that poor readers have no basic difficulties in the visual discriminationof confusing configurations of letters (b/d) and words (was/saw). He concluded thatreading disability is not caused by any deficiency in visual perception or visualmemory, but represents an impairment of some aspect of verbal processing,Bradley and Bryant (1978) also provided experimental evidence for the broadhypothesis that difficulty in organising spoken sounds contributes to reading back-wardness. The test consisted of sets of four spoken monosyllabic words, only threeof which had a sound in common, and the odd word out had to be identified. Thechildren who made most errors were backward readers and spellers.
Other workers have sought to identify more specific mechanisms in the process ofreading disability. For example, Liberman et al. (1974) supposed that an impairedacquisition of explicit phoneme segmentation might be an important factor. Moraiset al. (1979) studied the ability of illiterate adults to change the beginning of wordsby addition or deletion of phonemes. They found it much impaired in comparisonwith aduhs who had received some instruction in reading, and concluded that thisability would become manifest while learning to read. They stressed the reciprocalrelationship between the cognitive capacity for the awareness ofthe phonetic structureof speech and the specific training provided by reading itself. Most relevant to thepresent study are the results reported in dyslexic children by Snowling (1980). Shetested their ability to establish the sameness or difference of two very similar non-words (e.g. 'sond' and 'snod'). Their performance was impaired when the firstnon-word was presented visually and the second auditorily, when compared withnormal children matched for reading age. The defect is termed one of 'grapheme-phoneme' conversion. The dyslexic subjects, unlike normal readers, showed noimprovement in grapheme-phoneme conversion with increasing age. This lastobservation is also consistent with the finding in the present study of an impair-ment of phonetic reading which persisted into adolescence or adulthood and stillreflected the original severity of the reading disorder.
Severely faulty spelling is a constant clinical sign in dyslexic patients. It is likelyto remain demonstrable using standard spelling tests, even in older patients whose

IMPAIRMENTOFPHONETICRKADING IN DYSLEXIA 473
reading has improved so much that standard reading tests fail to show a conclusivedisability. This observation is relevant to the subclassification of dyslexic patientsby Boder (1971), who divided them into three groups according to their patterns ofspelling—dysphonetic, dyseidetic and mixed. The dysphonetic dyslexic can onlyspell the few words of his sight vocabulary that he can visualise. The dyseideticdyslexic does not spell so bizarrely and his misspellings tend to be phonetic. Thissubclassification of dyslexia is similar to that of Johnson and Myklebust (1967).Frith (1978, 1980) has clarified the nature of spelling disorders. She recogniseschildren who read well but spell badly: their spellings tend to be phoneticallyaccurate. Other children read poorly as well as being bad spellers (dyslexics ormild dyslexics), and much of their spelling is non-phonetic. Frith suggests there aretwo major types of deficit: the first arises from relating the sound of words to theirwritten representation and the second from relating their meaning to their writtenform. In her view, however, a satisfactory theory of spelling difficulties is not yetavailable. The findings of the present study suggest that impaired writing in dyslexicsis less clearly indicative of def'ective phonological processes and does not reflect theinitial severity ofthe dyslexic disorder. Defective spelling in dyslexia may be due to acombination of two kinds of deficit—in the processing of phonetic units and inlinking the written word to its meaning. It would seem hazardous to base asubclassification of dyslexia on patterns of spelling errors.
The changing views on the nature of dyslexia will have repercussions on theapproach to remedial teaching. On the one hand, it has been suggested that thesegmenting and blending of phonemic units is such a difficult step in learning toread that it should be taken last. Rozin and Gleitman (1977), for example, advisethat the historical development of writing from visual symbols to syllabaries shouldbe recapitulated in the classroom before tackling finally the alphabet. This view issimilar to an earlier one of Rozin f/a/. (1971) that the syllable, which is more readilypronounced than the phoneme, is the more suitable introduction to reading.
A different approach is that of Liberman ^/a/. (1974), who consider it possible anddesirable to teach dyslexics the explicit segmentation into phonemes. Williams(1980) has gone further in developing an instructional programme for learning-disabled children which provides explicit training in phoneme analysis and blending,letter-sound correspondences and decoding. Her approach was partly based on thework of Elkonin (1963, 1973), previously discussed. She describes her method as adecoding programme rather than a complete reading programme. Nevertheless, shewas able to show that following this method of instruction, children were able totransfer their decoding skills to the reading of new words, whether these were realwords or nonsense material. She concluded that phonemic decoding instruction,contained within a comprehensive reading programme, is likely to benefit learning-disabled children.
SUMMARY
A previous analysis of the historical development of writing towards progressivephonetisation gave rise to the hypothesis that disorders of reading arise from adefective processing of spoken sounds. Sixteen adolescent and adult dyslexic patients

474 G. RUSSELL
were studied, 10 of whom had been followed up from childhood. A newly devisedtest of phonetic reading proved superior to the Schonell reading test in distinguishingdyslexics from normals, and mirrored the original severity ofthe disorder. A phoneticwriting test was less useful. The findings support the view that dyslexia is due to adefect of verbal processing which may persist beyond childhood.
Acknowledgements—I wish to thank Mrs. Maud Heath, former Secretary of the London DyslexiaAssociation, Mr. G. C. Giles, Headmaster, Highgate School, and Mr. A. Sparks, Acting Headmaster,Peckham Manor Boys' School, who enabled me to approach suitable and cooperative subjects. Mr.Brian Everitt gave invaluable advice on the statistical analyses.
REFERENCES
BELMONT, L . and BIRCH, H . G . (1965) Lateral dominance, lateral awareness, and reading disability.ChildDev. 36,57-71.
BODF.R, E. (1971) Developmental dyslexia: prevailing diagnostic concepts and a new diagnosticapproach. In Progress in Learning Disabilities (Edited by MYKLEBUST, H. R.), pp. 293-321.Grune Stratton, New York.
BRADLEY, L . and BRYA.NT, P. E. (1978) Difficulties in auditory organisation as a possible cause ofreading backwardness. Nature, Lond. 271, 746-747.
CONRAD, R. (1977) The reading ability of deaf school-leavers. B r . / educ. Psychol. 47, 138-148.CRITCHLEY, M . (1970) TheDyslexic Child. William Heinemann Medical Books, London.ELKONIN, D . B. (1963) The psychology of mastering the elements of reading. In Educational Psychology
in the USSR (Edited by SiMON, B. and SIMON, J.), pp. 165-179. Routledge and Kegan Paul,London.
ELKONIN, D . B. (1973) Comparative reading—USSR. In Comparative Reading. Cross-National Studies ofBehavior and Processes in Reading and Writing (Edited by DOWNING, J.) , pp. 551-579. Macmillan,Nevkf York.
FRANSELI.A, F . and GERVER, D . (1965) Research notes: multiple regression equations for predictingreading age from chronological age and WISC verbal IQ. Br. J. educ. Psychol. 35, 86-89.
FRITH, U. (1978) Annotation: spelling difficulties./ Child Psychot. Psychiat. 19,279-285.FRITH, U . (1980) Unexpected spelling problems. In Cognitive Processes in Spelling (Edited by FRITH, U . ) ,
pp. 495-516. Academic Press, London.GALABURDA, A . M . and KEMPER, T . L . (1979) Cytoarchitectonic abnormalities in developmental
dyslexia: a case study. Ann. Neurol. 6, 94-100.HIER, D. B., LEMAY, M . , ROSENBERGF.R, P. B. and PERU), V. P. (1978) Developmental dyslexia.
Archs Neurol. 35,90-92.HlNSHELWOOD,J. (1895) Word-blindness and visual memory. Lancetii, 1564-1570.HINSHELWOOD, J. (1917) Congenital Word-blindness. H. K. Lewis &Co., London.JOHNSON, D.J . and MYKLEBUST, H . R . (1967) Disorders of reading. In Learning Disabilities: Educational
Principles and Practices, pp. 147-192. Grune Stratton, New York.KAVANAGH, J . F . (1968) Communicating by Language: The Reading Process. National Institute of Child
Health and Human Development, Bethesda, MD.Lancrt (1966) Annotations: Congenital word blindness, i i ,p . 36.LIBERMAN, I. Y., SHANKWEILER, D . , FISCHER, F . W . and CARTER, B. (1974) Explicit syllable and
phoneme segmentation in the young child./ exp. ChildPsychol. 18,201-212.MARSHALL, J. G. and NEWCOMBE, F . (1980) The conceptual status of deep dyslexia: an historical
perspective. In Deep Dyslexia (Edited by COLTHEART, M., PATTERSON, K. and MARSHALL, J. C ) ,pp. 1-21. Routledge and Kegan Paul, London.
MATTINGLY. I. C. (1968) In Communicaling hy Language: The Reading Process (Edited by KAVANAGH, J. F.).National Institute of Child Health and Human Development, Bethesda, MD.

IMPAIRMENT OF PHONETIC READING IN DYSLEXIA 475
MATTINGLY, I. G. (1972) In Language by Ear and by Eye: The Relationship between Speech and Reading(Editedby KAVANAGH, J. F. and MATTINGLY, I. G.), pp. 133-147. MIT Press, Cambridge, MA.
MORAIS, J., CARY, L . , ALEGRIA, J. and BERTELSON, P. (1979) Does awareness of speech as asequence of phones arise spontaneously? Cognition 7, 323-331.
ORTON, S . T . (1937) Reading, Writing and Speech Problems in Children. Chapman &Hall, London.P R I N G L E M 0 R G A N , W . (1896) Congenital word blindness. .Br. med.J. 2, 1378-1379.ROZIN, P., PORITSKY, S. E. and SOTSKY, R . (1971) American children with reading problems can
easily learn to read English represented by Chinese characters. Scierue, N.Y. 171, 1264-1267.ROZlN, P. and GLEITMAN, L. R. (1977) The structure and acquisition of Reading II. The reading
process and the acquisition ofthe alphabetic principle. In Towards a Psychology of Reading {Edited byREBER, A. S. and SCARBOROUGH, D . L ) , pp. 55-141. Lawrence Erlbaum Associates, HillsdaJe, NJ.
RUSSELL, G . F . M . (1982) Writing and dyslexia—an historical analysis. / Child Psychot. Psychiat. 23,383-400.
SCHONELL, F . J. and GOODACRE, E . (1974) The Psychology and Teaching of Reading. Oliver and Boyd,Edinburgh, 5th Edition.
SCHONELL, F. J. and SCHONELL, F . E . (1960) Diagnostic and Attainment Testing Including a Manual of Tests,Their Nature, Use, Recording and Interpretation, 4th edition. Oliver and Boyd, Edinburgh.
SHANKWEILER, D . and LIBERMAN, I. Y. (1976) Exploring the relations between reading and speech.In The Neuropsychology of Learning Disorders—Theoretical Approaches (Edited by KNIGHTS, R. M. andBAKKER, D . J ) , pp. 297-313. University Park Press, Baltimore, MD.
SLADE, P . D . and RusSELL, G. F. M. (1971) Developmental dyscalculia: a brief report on four cases.Psychol. Med. 1,292-298.
SNOWLING, M . J. (1980) The development of grapheme-phoneme correspondence in normal anddyslexic readers./ exp. ChildPsychol. 29, 294-305.
SPARROW, S. S. and SATZ, P. (1970) Dyslexia, laterality and neuropsychological developmenl. InSpecific Reading Disability. Advances in Theory and Method (Edited by BAKKER. D. J. and SATZ, P.),pp. 41-60. Rotterdam University Press, Rotterdam.
THOMSON, M . E. (1976) A comparison of laterality effects in dyslexics and controls using verbaldichotic listening tasks. Neuropsychologia 14, 243-246.
VELLUTINO, F . R . (\97 9) L>yslexia, Theory and Research. MIT Press, Cambridge, MA.VELLUTINO, F . R . , STEGER.J . A. and KANDEL, G . (1972) Reading disability: an investigation of the
perceptual deficit hypothesis. Cortex S, 106-118.WEPMAN, J. M. (1961) The interrelationship of hearing, speech and reading. The Reading Teacher 14,
245-247.WILLIAMS, J. P. (1980) Teaching decoding with an emphasis on phoneme analysis and phoneme
blending./ educ. Psychol. 72, 1-15.YULE, W . (1967) Predicting reading ages on Neale's analysis of reading ability. Br. J. educ. Psychol. 37,
252-255.