
Impact Dosage Schedule on Efficacy ofGentamicin ...aac.asm.org/content/35/1/111.full.pdfANTIMICROB....
6
ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Jan. 1991, p. 111-116 0066-4804/91/010111-06$02.00/0 Copyright C 1991, American Society for Microbiology Impact of Dosage Schedule on the Efficacy of Gentamicin, Tobramycin, or Amikacin in an Experimental Model of Serratia marcescens Endocarditis: In Vitro-In Vivo Correlation GILLES POTEL,1* JOCELYNE CAILLON,1 BRUNO FANTIN,2 JOCELYNE RAZA,1 FLORENCE LE GALLOU,1 JEAN-YVES LEPAGE,' PHILIPPE LE CONTE,' DENIS BUGNON,1 DENIS BARON,' AND HENRI DRUGEON' Laboratoire d'Antibiologie, Faculte de Medecine, 1 rue Gaston Veil, 44000 Nantes,' and Institut National de la Sante et de la Recherche Medicale U.13, H6pital Claude Bernard, 75019 Paris,2 France Received 21 May 1990/Accepted 16 October 1990 Aminoglycosides are usually considered to be concentration-dependent antibiotics and to have similar pharmacodynamic and pharmacokinetic properties. To verify the equivalent activity of the aminoglycosides on a susceptible strain, we tested the killing rate of three aminoglycosides (gentamicin, tobramycin, and amikacin) on one strain of Serratia marcescens both in vitro and in vivo by using a rabbit model of left-ventricle endocarditis. Despite similar MICs, the time-kill curve of gentamicin was consistently better than those of amikacin and tobramycin, whatever the concentration of each antibiotic used (1, 2, 4, 8, 16, or 32 mg/liter), after a 5-h incubation. The in vivo bacterial reduction in the vegetations was measured 24 h after administration of an intravenous 48-mg/kg bolus of each antibiotic or at the end of a 24-h continuous intravenous infusion of the same dose. Gentamicin was significantly more effective when administered as a bolus than when administered as a continuous infusion (2.8 0.2 versus 6.4 1.5 log1o CFU/g of vegetation, respectively; P < 0.01), whereas amikacin was more effective as a continuous infusion than as a bolus injection (3.6 2.0 versus 7.5 + 1.3 loglo CFU/g of vegetation, respectively; P < 0.01). Tobramycin was not very effective, whatever the dosage tested (approximately 6.5 to 7 loglo CFU/g). These results suggest that concentration-dependent bactericidal activities, both in vitro and in vivo, may vary greatly among aminogly- cosides despite similar MICs. The bactericidal killing rates of aminoglycosides are usu- ally considered to be concentration dependent. This prop- erty is defined by an increased bactericidal effect with increasing concentration for any given period of exposure. Consistent data from different animal models (8, 13) suggest that in cases of pseudomonal experimental infections, single, large daily doses of aminoglycosides are at least as effective as conventional intermittent dosing regimens. Despite infre- quent in vivo comparative studies between aminoglycosides, Kapusnik et al. concluded that it is now possible to study the single-daily-dose regimen in humans and that any of the aminoglycosides may be used, because their pharmacoki- netic and pharmacodynamic properties are comparable (12). A clinical multiple-dose study (including bacteremia and pneumonia) of humans has shown that a high peak-concen- tration/MIC ratio was a factor of improved therapeutic outcome (16), suggesting that single daily dosing could further improve the prognosis of severely infected patients, allowing higher peak concentration of aminoglycosides. Fur- thermore, aminoglycosides are less toxic in single doses than in multiple doses (1, 21). Recent studies (4, 18) failed to show any evidence that aminoglycoside treatment once daily had greater ototoxicity or nephrotoxicity than the traditional three-times-daily regimen. Nevertheless, and before the routine clinical application of single daily doses, it should be pointed out that some bacterial species (like Serratia marcescens) have been ex- cluded from experimental studies despite a high mortality rate in clinical infections and a possible difference from other * Corresponding author. species in terms of optimal antimicrobial regimen. Juvin et al. (11) have shown for six clinical strains of S. marcescens that killing rates of aminoglycosides in vitro could be dif- ferent from one another for the same strain, even when their MICs were similar, suggesting a possible difference in terms of pharmacodynamic properties of aminoglycosides. Fur- thermore, gentamicin is intrinsically the most active amino- glycoside against Serratia strains which are susceptible to all aminoglycosides (11). The aim of this work was to verify the in vivo relevance of these findings on a rabbit model of S. marcescens endocardi- tis, comparing the in vivo dynamics of bacterial killing of a single equivalent dose of gentamicin, tobramycin, or amika- cin. To assess the in vivo impact of dosage schedule, we administered the same dosage of each drug as a pulse dosing or as a 24-h continuous intravenous (i.v.) infusion. MATERIALS AND METHODS Organism. The strain of S. marcescens used for inducing experimental endocarditis, strain HN229, was isolated from the urine of a hospital patient. This strain was found to be resistant to rabbit serum. Antibiotics. The three aminoglycosides tested were tobra- mycin (Eli-Lilly), gentamicin (Schering-Plough), and amika- cin (Bristol). In vitro studies. (i) Antibiotic susceptibility tests. The MIC of each antibiotic was determined by a Mueller-Hinton broth dilution technique with Ca2' and Mg2+ supplementation (24) in 200-pdl wells, with an inoculum of 105 CFU/ml in the mid-exponential phase of growth. The MIC was defined as the lowest concentration of the drug producing no visible 111 Vol. 35, No. 1 on June 24, 2018 by guest http://aac.asm.org/ Downloaded from
Transcript of Impact Dosage Schedule on Efficacy ofGentamicin ...aac.asm.org/content/35/1/111.full.pdfANTIMICROB....

ANTIMICROBIAL AGENTS AND CHEMOTHERAPY, Jan. 1991, p. 111-1160066-4804/91/010111-06$02.00/0Copyright C 1991, American Society for Microbiology
Impact of Dosage Schedule on the Efficacy of Gentamicin,Tobramycin, or Amikacin in an Experimental Model of Serratia
marcescens Endocarditis: In Vitro-In Vivo CorrelationGILLES POTEL,1* JOCELYNE CAILLON,1 BRUNO FANTIN,2 JOCELYNE RAZA,1 FLORENCE LE GALLOU,1JEAN-YVES LEPAGE,' PHILIPPE LE CONTE,' DENIS BUGNON,1 DENIS BARON,' AND HENRI DRUGEON'
Laboratoire d'Antibiologie, Faculte de Medecine, 1 rue Gaston Veil, 44000 Nantes,' and Institut National de laSante et de la Recherche Medicale U.13, H6pital Claude Bernard, 75019 Paris,2 France
Received 21 May 1990/Accepted 16 October 1990
Aminoglycosides are usually considered to be concentration-dependent antibiotics and to have similarpharmacodynamic and pharmacokinetic properties. To verify the equivalent activity of the aminoglycosides ona susceptible strain, we tested the killing rate of three aminoglycosides (gentamicin, tobramycin, and amikacin)on one strain of Serratia marcescens both in vitro and in vivo by using a rabbit model of left-ventricleendocarditis. Despite similar MICs, the time-kill curve of gentamicin was consistently better than those ofamikacin and tobramycin, whatever the concentration of each antibiotic used (1, 2, 4, 8, 16, or 32 mg/liter),after a 5-h incubation. The in vivo bacterial reduction in the vegetations was measured 24 h afteradministration of an intravenous 48-mg/kg bolus of each antibiotic or at the end of a 24-h continuousintravenous infusion of the same dose. Gentamicin was significantly more effective when administered as abolus than when administered as a continuous infusion (2.8 0.2 versus 6.4 1.5 log1o CFU/g of vegetation,respectively; P < 0.01), whereas amikacin was more effective as a continuous infusion than as a bolus injection(3.6 2.0 versus 7.5 + 1.3 loglo CFU/g of vegetation, respectively; P < 0.01). Tobramycin was not veryeffective, whatever the dosage tested (approximately 6.5 to 7 loglo CFU/g). These results suggest thatconcentration-dependent bactericidal activities, both in vitro and in vivo, may vary greatly among aminogly-cosides despite similar MICs.
The bactericidal killing rates of aminoglycosides are usu-ally considered to be concentration dependent. This prop-erty is defined by an increased bactericidal effect withincreasing concentration for any given period of exposure.Consistent data from different animal models (8, 13) suggestthat in cases of pseudomonal experimental infections, single,large daily doses of aminoglycosides are at least as effectiveas conventional intermittent dosing regimens. Despite infre-quent in vivo comparative studies between aminoglycosides,Kapusnik et al. concluded that it is now possible to study thesingle-daily-dose regimen in humans and that any of theaminoglycosides may be used, because their pharmacoki-netic and pharmacodynamic properties are comparable (12).A clinical multiple-dose study (including bacteremia andpneumonia) of humans has shown that a high peak-concen-tration/MIC ratio was a factor of improved therapeuticoutcome (16), suggesting that single daily dosing couldfurther improve the prognosis of severely infected patients,allowing higher peak concentration of aminoglycosides. Fur-thermore, aminoglycosides are less toxic in single doses thanin multiple doses (1, 21). Recent studies (4, 18) failed to showany evidence that aminoglycoside treatment once daily hadgreater ototoxicity or nephrotoxicity than the traditionalthree-times-daily regimen.
Nevertheless, and before the routine clinical application ofsingle daily doses, it should be pointed out that somebacterial species (like Serratia marcescens) have been ex-cluded from experimental studies despite a high mortalityrate in clinical infections and a possible difference from other
* Corresponding author.
species in terms of optimal antimicrobial regimen. Juvin etal. (11) have shown for six clinical strains of S. marcescensthat killing rates of aminoglycosides in vitro could be dif-ferent from one another for the same strain, even when theirMICs were similar, suggesting a possible difference in termsof pharmacodynamic properties of aminoglycosides. Fur-thermore, gentamicin is intrinsically the most active amino-glycoside against Serratia strains which are susceptible to allaminoglycosides (11).The aim of this work was to verify the in vivo relevance of
these findings on a rabbit model of S. marcescens endocardi-tis, comparing the in vivo dynamics of bacterial killing of asingle equivalent dose of gentamicin, tobramycin, or amika-cin. To assess the in vivo impact of dosage schedule, weadministered the same dosage of each drug as a pulse dosingor as a 24-h continuous intravenous (i.v.) infusion.
MATERIALS AND METHODS
Organism. The strain of S. marcescens used for inducingexperimental endocarditis, strain HN229, was isolated fromthe urine of a hospital patient. This strain was found to beresistant to rabbit serum.
Antibiotics. The three aminoglycosides tested were tobra-mycin (Eli-Lilly), gentamicin (Schering-Plough), and amika-cin (Bristol).
In vitro studies. (i) Antibiotic susceptibility tests. The MICof each antibiotic was determined by a Mueller-Hinton brothdilution technique with Ca2' and Mg2+ supplementation (24)in 200-pdl wells, with an inoculum of 105 CFU/ml in themid-exponential phase of growth. The MIC was defined asthe lowest concentration of the drug producing no visible
111
Vol. 35, No. 1
on June 24, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIMICROB. AGENTS CHEMOTHER.
growth after an incubation of 18 h. After 24 h, a subculturewas made on Mueller-Hinton agar (Difco Laboratories,Detroit, Mich.) The MBC corresponded to the lowest con-
centration of the drug permitting 0.1% of the bacteria to
survive and was obtained by replicating 1 ml, using a Steersapparatus, onto agar plates with polyanethole sulfonic acidsodium salt (SPS; Sigma).
(ii) Killing curves. Time-kill curves were drawn for eachantibiotic at 11 concentrations in Mueller-Hinton broth: 0,0.06, 0.12, 0.25, 0.5, 1, 2, 4, 8, 16, and 32 mg/liter. For eachconcentration the antibiotics were incubated in a microtube(1-ml tubes, Macrowell; Skatron, Lier, Norway) with an
inoculum of 107 S. marcescens cells per ml in the stationaryphase of growth. Surviving bacteria were counted in eachtube after 1.5, 3, 5, and 24 h of incubation by a semiauto-matic dilution micromethod involving an automatic 96-welldispenser (Skatron) and a Steers replicator distributing 2 ±
0.5 IlI of each dilution onto agar plates. A 3% solution of SPSwas added, avoiding a carryover phenomenon. After a 24-hincubation, the first dilution with 5 to 30 colonies was readand the colony count was then multiplied by the dilutionfactor. The standard error of this count was 0.2 log1oCFU/ml. The sensitivity limit of detection is equal to 2.4log1o CFU/ml. This method was detailed in a previous work(5).
Experimental endocarditis. In vivo studies were carriedout on New Zealand White female rabbits (age range, 12 to15 weeks; weight range, 2.5 to 3.5 kg). The animals were
kept in individual cages and allowed free access to food andwater throughout the experiment. Left-ventricular en-
docarditis was induced as described previously (19). At 24 hafter introduction of a polyethylene catheter through theaortic valve, each rabbit received 1 ml of a suspensioncontaining i07 organisms per ml, injected through the mar-
ginal ear vein.(i) Experimental design. At 48 h after inoculation, the
animals were randomly assigned to one of the six followingtherapeutic regimens: 48 mg of gentamicin, tobramycin, or
amikacin per kg administered as an i.v. bolus or as a 24-h i.v.continuous infusion. For the infusion, a catheter (22-gauge)was inserted into a marginal ear vein and connected to an
electric syringe pump. The antibiotic was diluted iti sterilesaline, and the infusion output chosen was equal to 2 ml/h.The animals were kept for 24 h in rabbit-restraining cages.
Nine untreated rabbits made up the control group. Aspreviously shown, the dose chosen (48 mg/kg) allowed fortrough concentrations in vegetations averaging 2 ,ug/g ofvegetation 24 h after an i.v. bolus (20), assuming that no
bacterial regrowth could occur during the experiment; thispermitted valuable comparisons between drugs. Moreover,three infected animals were assigned to each therapeuticregimen to determine the pharmacokinetics of each drug. Acatheter was inserted into the left femoral artery to takeserum samnples 5, 15, and 30 min and 1, 2, 4, 6, and 24 h afterthe bolus or 0.25, 0.5, 1, 2, 3, 6, and 24 h after the beginningof the infusion.
(ii) Evaluation of therapy. The effect of each treatment wasevaluated 24 h after the i.v. bolus of each antibiotic or at theend of the 24-h i.v. infusion. The animals were sacrificedwith an i.v. bolus of thiopental. The heart was removed, andvegetations were excised and rapidly rinsed in sterile saline.Some of the vegetations were weighed and homogenized in aThomas Teflon pestle tissue homogenizer with 0.5 ml ofsterile saline. Serial dilutions of 50-pd aliquots were spreadby using a Spiral System (Interscience) and quantitativelycultured on Trypcase-soy agar plates for 24 h at 370C.
Bacterial titers were expressed as log1o CFU/g of vegetation.We were able to detect quantities as small as 20 CFU/ml.Owing to this sensitivity limit, vegetations found to be sterilewere considered to contain 20 CFU/ml of homogenate, andthe value integrated for the calculation of the mean bacterialtiter took into account the weight of vegetations. Part of eachvegetation was frozen prior to antibiotic assays.
(iii) Antibiotic assays. Concentrations of each antibiotic inserum were determined by using a microbiological assaywith Bacillus subtilis ATCC 6633. The range of measurableconcentrations with this strain was 0.06 to 1 ,ug/ml for allthree antibiotics. After being weighed and homogenized with0.3 ml of 0.1 M phosphate buffer, the vegetations werecentrifuged and the supernatant fluid was sampled for micro-biologal assay. The same strain of B. subtilis was used.
(iv) Statistical evaluation. A Kruskall-Wallis test and then aMann-Whitney test were performed to compare the bacterialtiters measured in treated animals versus controls. A Fisherexact test was used to compare the number of sterilevegetations (no growth of the undiluted tissue homogenate)in each group versus the controls.
RESULTS
In vitro studies. (i) Antibiotic susceptibiity tests. The MICs(and the MBCs) for the S. marcescens strain studied were0.5 -jg of gentamicin per ml and 1 jig of tobramycin andamikacin per ml.
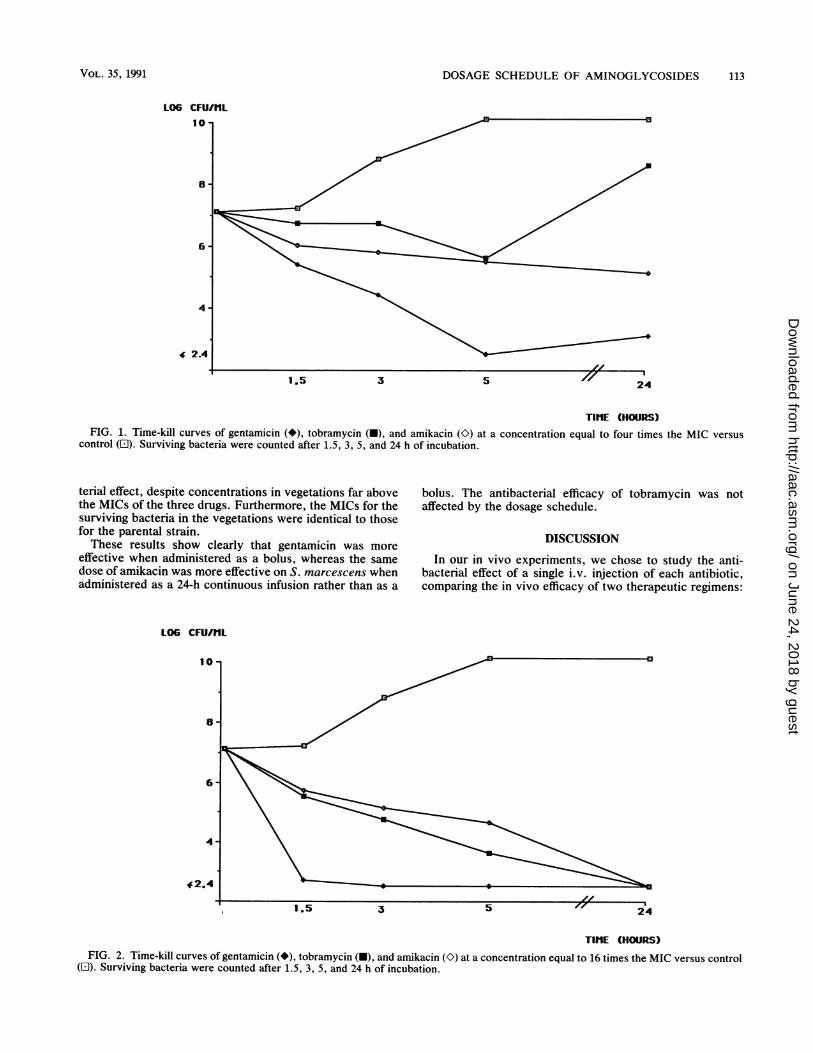
(ii) Killing curves. At concentrations of twice the MIC, thethree aminoglycosides exhibited a slight bactericidal activitybetween 0 and 5 h, but regrowth was noted between 5 and 24h only for tobramycin and amikacin; this regrowth reachedthe same level as the control (10 log CFU/ml). The time-killcurves of the three aminoglycosides at 4 times the MIC arerepresented in Fig. 1. Gentamicin exhibited the best killing,apparently sterilizing the culture after a 5-h incubationperiod. At a concentration 16 times the MIC (Fig. 2),gentamicin sterilized the culture after a 3-h incubation pe-riod, without regrowth at 24 h. Amikacin and tobramycinexhibited a concentration-dependent killing between 4 and16 times the MIC, although their effect was less dramaticthan that of gentamicin. The MICs for surviving bacteriaafter a 24-h exposure were unchanged compared with thosefor the parental strain.
In vivo studies. (i) Concentrations in serum. The drug levelsobtained in serum after a 48-mg/kg i.v. bolus of gentamicin,tobramycin, and amikacin were quite similar each time, witha peak level (5 min after the injection) around 300 ,ug/ml anda trough level (24 h after the injection) around 1 ,ug/ml. Themean half-life at 1B phase for the three aminoglycosides,calculated between 30 min and 6 h, was 54 min (r = 0.97; P< 0.001). The steady state of the 24-h i.v. infusion wasreached between 3 and 6 h. The mean level in serum wasslightly lower for gentamicin (7.9 + 2.1 ,ug/ml) than fortobramycin (9.2 + 1.9 ,ug/ml) or amikacin (8.0 ± 1.9 ,ug/ml),but this difference was not significant.
(ii) Experimental endocarditis. The in vivo effect of a48-mg/kg dose of each antibiotic administered as a bolus isshown in Table 1. Gentamicin was the most effective antibi-otic and had a significant antibacterial effect on vegetations,whereas amikacin and tobramycin did not. The mean troughconcentration in vegetations was similar in each group(around 2 ,ug/g of vegetation). When the same dose wasadministered as a continuous 24-h i.v. infusion (Table 2),amikacin proved the most effective, more so than gentamicin(P < 0.05), whereas tobramycin had no significant antibac-
112 POTEL ET AL.
on June 24, 2018 by guesthttp://aac.asm
.org/D
ownloaded from
DOSAGE SCHEDULE OF AMINOGLYCOSIDES 113
L06 CFU/fIL
4
24
TIME (HOURS)FIG. 1. Time-kill curves of gentamicin (*), tobramycin (O), and amikacin (K) at a concentration equal to four times the MIC versus
control (El). Surviving bacteria were counted after 1.5, 3, 5, and 24 h of incubation.
terial effect, despite concentrations in vegetations far abovethe MICs of the three drugs. Furthermore, the MICs for thesurviving bacteria in the vegetations were identical to thosefor the parental strain.These results show clearly that gentamicin was more
effective when administered as a bolus, whereas the samedose of amikacin was more effective on S. marcescens whenadministered as a 24-h continuous infusion rather than as a
bolus. The antibacterial efficacy of tobramycin was notaffected by the dosage schedule.
DISCUSSION
In our in vivo experiments, we chose to study the anti-bacterial effect of a single i.v. injection of each antibiotic,comparing the in vivo efficacy of two therapeutic regimens:
LOG CFU/IL
10
6
3
TIME (HOURS)FIG. 2. Time-kill curves of gentamicin (*), tobramycin (U), and amikacin (O) at a concentration equal to 16 times the MIC versus control
(El). Surviving bacteria were counted after 1.5, 3, 5, and 24 h of incubation.
VOL. 35, 1991
on June 24, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

ANTIMICROB. AGENTS CHEMOTHER.
TABLE 1. In vivo mean antibacterial effect of gentamicin, amikacin, or tobramycin in vegetations 24 h after an i.v. 48-mg/kg doseadministered as a bolus
Treatment group No. of rabbits Mean vegetation titer ± SD No. of sterile Trough concn in vegetationssacrificed (log CFU/g of vegetation) vegetations/total no." (gLg/g of vegetation) (mean ± SD)
Control 11 7.8 ± 0.4 0/11Gentamicin 9 2.8 ± 0.2b 6/9c 2.2 ± 1.2Amikacin 10 7.5 ± 1.3 0/10 1.9 ± 1.8Tobramycin 7 6.8 ± 1.9 0/7 2.3 ± 1.5
a Number of culture-negative vegetations/total number of animals sacrificed.b P < 0.01 versus control (Mann-Whitney U test).c P = 0.004 versus control (Fisher's exact test).
bolus or continuous infusion. S. marcescens endocarditis,although uncommon in humans, provided a useful experi-mental model of acute gram-negative bacterial infection andwas also used to assess the relationship between the bacte-rial titer and the antibiotic level in infected sites (6). More-over, a single i.v. injection allowed us to study the in vivointrinsic activity of each drug more accurately, avoidingcomplex interactions of dosing intervals or postantibioticeffects.Our in vitro results showed clearly that, despite similar
MICs and MBCs, the killing rate of gentamicin was mark-edly higher than those of tobramycin and amikacin, what-ever the concentration used. In vivo, gentamicin exhibitedthe best antibacterial effect when administered as a bolus,whereas amikacin proved most effective when administeredas a continuous infusion, more so than gentamicin andtobramycin.The differences observed in vivo cannot apparently be
explained by pharmacokinetic parameters. The dose chosen(48 mg/kg) proved capable of achieving similar mean troughconcentrations for each drug 24 h after a bolus (2.2, 1.9, and2.3 ,ug/g of vegetation for gentamicin, amikacin, and tobra-mycin, respectively). Furthermore, the half-lives in serum
were very similar from one drug to another. Nevertheless,despite similar pharmacokinetics in serum, it is not clear thatthe areas under the concentration-time curves are similar inthe vegetations themselves. Therefore, Carbon et al. (2)showed that of the aminoglycosides injected in 1.5-mg/kgdoses, gentamicin induced higher interstitial levels than didtobramycin. In this work, we did not determine the earlyconcentrations of aminoglycosides after administration ofthe bolus in the vegetations themselves, and a possibledifference (in terms of local concentrations between drugs)cannot be excluded. Finally, it must be stressed that thetobramycin bolus has a mediocre in vivo antibacterial effect,whereas its distribution is rapid and homogeneous, as has
been recently shown in quantitative autohistoradiography(3).The differences observed may be due to the antibiotic
itself: the activity of gentamicin in vitro (in time-kill curve
terms) is significantly more concentration dependent thanthat of amikacin or tobramycin, which may explain thebetter in vivo activity of a gentamicin bolus. It has beenshown in vitro that the antibacterial effect of aminoglyco-sides on gram-negative bacteria necessitates an active up-
take, which consumes energy (9, 23). In recent research, ithas been shown with Escherichia coli and Salmonella typhithat the level of this uptake is genetically determined (15).The hypothesis can thus be put forward that this level ofuptake may be different from one aminoglycoside to anotherand that, for the same bacterium, the higher the uptake, themore efficient a high concentration (gentamicin) would be.On the contrary, a lower level for tobramycin and amikacinwould be responsible for the poor result observed in vivowith the bolus. In continuous administration, only amikacinenables five of eight animals to clear the bacteria, confirmingits time-dependent activity on S. marcescens. As the steadystate is similar for the three antibiotics tested, it is hard tounderstand why tobramycin does not cause the same resultsas amikacin with this regimen, since their in vitro behavior issimilar. It is possible that local physicochemical conditions(pH, anaerobiosis) are less favorable to its activity on S.
marcescens, although this fact, to our knowledge, has never
been demonstrated. Therefore, the active concentrations invivo are probably higher than the MICs in vitro and may bedifferent from one drug to another. Finally, it is possible thatour strain of S. marcescens produces a 6'-aminoglycosideacetyltransferase (AAC 6') enzyme, which preferentiallyinactivates tobramycin and amikacin (10, 17, 22), even
though the MICs for surviving bacteria (both in vitro and invivo) were apparently identical to those for the parental
TABLE 2. In vivo mean antibacterial effect of gentamicin, amikacin, or tobramycin in vegetations after an i.v. 24-h continuous infusionof a 48-mg/kg dose
No. of rabbits Mean vegetation titer ± SD No. of sterile Concn in vegetation at steady stateTreatment group sacrificed (log CFU/g of vegetation) vegetations/total no." (p.g/g of vegetation) (mean ± SD)
Control 11 7.8 ± 0.4 0/11Gentamicin 7 6.4 1.5b 0/7 10.5 ± 2.5Amikacin 8 3.6 ± 2.0C 5/8d 8.2 ± 3.7Tobramycin 7 6.5 ± 2.2 0/7 11.3 ± 3.6
a Number of culture-negative vegetations/total number of animals sacrificed.b p < 0.05 versus control (Mann-Whitney U test).C P < 0.01 versus control (Mann-Whitney U test).d p = 0.004 versus control (Fisher's exact test).
114 POTEL ET AL.
on June 24, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

DOSAGE SCHEDULE OF AMINOGLYCOSIDES 115
strains. New in vitro experiments are now in progress in anattempt to elucidate this important point.
Experimental research comparing the dose-efficacy orconcentration-efficacy relation of several aminoglycosideson the same type of bacterium are rare. Recently, Legett etal. (14) studied the effect of different doses and the interval ofadministration of netilmicin and gentamicin on a murinemodel of Klebsiella pneumoniae thigh infection or pneumo-nia. The authors found no difference in activity between thetwo antibiotics, but there were no data available in thisresearch concerning the in vitro time-kill curves. On theother hand, much experimental research has shown theconcentration-dependent activity of aminoglycosides (8, 12,14), but none of this research has been carried out for S.marcescens infections. Moore et al. (16) do not identify theresults obtained on S. marcescens in terms of the aminogly-coside used. Interestingly, Garraffo et al. studied the serumantibacterial activity of an i.v. infusion of amikacin on thesame strain of S. marcescens in healthy volunteers. Serumkilling curves showed a time-dependent activity against thisstrain, but a concentration-dependent activity against Esch-erichia coli and Enterobacter cloacae (7).
Finally, our results show that the in vivo activities of threeaminoglycosides against S. marcescens can be different,despite similar MICs. Their pharmacodynamics (in time-killcurve terms) are different, both in vitro and in vivo. More-over, the in vivo effect of a bolus can indeed be predicted bythe in vitro time-kill curves, which demonstrate the superioractivity of gentamicin. Despite an initial dose with concen-trations close to those observed in humans, amikacin is lessefficient as a bolus than in continuous administration. Thus,concentration-dependent killing can differ markedly amongaminoglycosides, and concentration-dependent killing maybe relatively less important than time-dependent killing. Therelative contributions of time- and concentration-dependentkilling to overall in vivo antibacterial effect are difficult topredict from in vitro studies. Our results do not agree withthose of Kapusnik et al. (12), and optimum dosing regimensdetermined with one aminoglycoside and species should notbe generalized to others. Other in vitro studies are nownecessary to explain the mechanism(s) which would enablethese differences to be elucidated.
In short, the type of antibacterial activity (time or concen-tration dependent) of aminoglycosides depends both on themolecule chosen and on the bacterium under treatment. Theweak activity of amikacin in bolus form on S. marcescens(compared with that of gentamicin) could explain in part theabsence of agreement in the literature concerning the opti-mum therapeutic dosage regimen of aminoglycosides (13).
ACKNOWLEDGMENTS
This work was supported in part by grants from Facultd deMddecine de Nantes.We thank M. 0. Hervy for her helpful secretarial assistance.
REFERENCES1. Bennett, W. M., C. E. Plamp, D. N. Gilbert, R. A. Parker, and
G. A. Porter. 1979. The influence of dosage regimen on exper-imental gentamicin nephrotoxicity: dissociation of peak serumlevels from renal failure. J. Infect. Dis. 140:576-580.
2. Carbon, C., A. Contrepois, and S. Lamotte-Barrillon. 1978.Comparative distribution of gentamicin, tobramycin, sisomicin,netilmicin, and amikacin in interstitial fluid in rabbits. Antimi-crob. Agents Chemother. 13:368-372.
3. Cremieux, A. C., B. Maziere, J. M. Vallois, M. Ottaviani, A.Azancot, H. Raffoul, A. Bouvet, J. J. Pocidalo, and C. Carbon.1989. Evaluation of antibiotic diffusion into cardiac vegetations
by quantitative autoradiography. J. Infect. Dis. 159:938-944.
4. de Vries, P. J., R. P. Verkooyen, P. Lequit, and H. A. Verbrugh.1990. Prospective randomized of once-daily versus thrice-dailynetilmicin regimens in patients with intraabdominal infections.Eur. J. Clin. Microbiol. Infect. Dis. 9:161-168.
5. Drugeon, H. B., J. Caillon, M. E. Juvin, and J. L. Pirault. 1987.Dynamics of ceftazidime-pefloxacin interaction shown by a newkilling curve-chequer board method. J. Antimicrob. Chemother.19:197-203.
6. Fantin, B., B. Pangon, G. Potel, J. M. Vallois, F. Caron, A.Bure, and C. Carbon. 1989. Ceftriaxone-netilmicin combinationin single-daily-dose treatment of experimental Escherichia coliendocarditis. Antimicrob. Agents Chemother. 33:767-770.
7. Garraffo, R., H. B. Drugeon, P. Dellamonica, E. Bernard, and P.Lapalus. 1990. Determination of optimal dosage regimen foramikacin in healthy volunteers by study of pharmacokineticsand bactericidal activity. Antimicrob. Agents Chemother. 34:614-621.
8. Gerber, A. U., W. A. Craig, H. P. Brugger, C. Feller, A. P.Vastola, and J. Brandel. 1983. Impact of dosing intervals onactivity of gentamicin and ticarcillin against Pseudomonasaeruginosa in granulocytopenic mice. J. Infect. Dis. 147:910-917.
9. Hancock, R. E. W., and A. Bell. 1988. Antibiotic uptake intoGram-negative bacteria. Eur. J. Clin. Microbiol. Infect. Dis.7:713-720.
10. John, J. F., W. F. McNeill, K. E. Price, and P. A. Kresel. 1982.Evidence for chromosomal site specifying amikacin resistancein multiresistant Serratia marcescens. Antimicrob. Agents Che-mother. 21:587-591.
11. Juvin, M. E., H. B. Drugeon, J. Caillon, and J. L. Pirault. 1987.Comparaison de l'activitd bactdricide de trois aminosides: gen-tamicine, tobramycine, amikacine. Pathol. Biol. 35:461-465.
12. Kapusnik, J. E., C. J. Hachbarth, H. F. Chambers, T. Carpen-ter, and M. A. Sande. 1988. Single, large, daily dosing versusintermittent dosing of tobramycin for treating experimentalpseudomonas pneumonia. J. Infect. Dis. 158:7-12.
13. Le Bel, M., and M. Spino. 1988. Pulse dosing versus continuousinfusion of antibiotics. Pharmacokinetic-pharmacodynamic con-siderations. Clin. Pharmacokinet. 14:71-95.
14. Legett, J. E., B. Fantin, S. Ebert, K. Totsuka, B. Vogelman, W.Calame, H. Mattie, and W. A. Craig. 1989. Comparative antibi-otic dose-effect relations at several dosing intervals in murinepneumonitis and thigh-infection models. J. Infect. Dis. 159:281-292.
15. Merlin, T. L., G. E. Davis, W. L. Anderson, R. K. Moyzis, andJ. K. Griffith. 1989. Aminoglycoside uptake increased by tetgene expression. Antimicrob. Agents Chemother. 33:1549-1552.
16. Moore, R. D., P. S. Lietman, and C. R. Smith. 1987. Clinicalresponse to aminoglycoside therapy: importance of the ratio ofpeak concentration to minimal inhibitory concentration. J. In-fect. Dis. 155:93-99.
17. Morohoshi, T., M. Toriya, S. Yokoiyama, K. Fujimoto, K.Hayano, S. Goto, and A. Tsuji. 1984. The acetylation of 6'-aminogroup of amikacin by a new enzyme prepared from Serratia sp.J. Antibiot. 37:1687-1691.
18. Nordstrom L., H. Ringberg, S. Cronberg, 0. Tjernstrom, and M.Walder. 1990. Does administration of an aminoglycoside in asingle daily dose affect its efficacy and toxicity? J. Antimicrob.Chemother. 25:159-173.
19. Perlman, B. B., and L. R. Freedman. 1971. Experimentalendocarditis. II. Staphylococcal infection of the aortic valvefollowing placement of a polyethylene catheter in the left side ofthe heart. Yale J. Biol. Med. 44:206-213.
20. Potel, G., B. Pangon, B. Fantin, J. M. Vallois, F. Faurisson, andC. Carbon. 1986. Program Abstr. 26th Intersci. Conf. Antimi-crob. Agents Chemother., abstr. 575.
21. Powell, S. H., W. B. Thompson, M. A. Luthe, R. C. Stern, D. A.Grossniklaus, D. D. Bloxham, D. L. Groden, M. R. Jacobs, A. 0.Discenna, H. A. Cash, and J. D. Klinger. 1983. Once daily vscontinuous aminoglycoside dosing: efficacy and toxicity in ani-
VOL. 35, 1991
on June 24, 2018 by guesthttp://aac.asm
.org/D
ownloaded from

116 POTEL ET AL. ANTIMICROB. AGENTS CHEMOTHER.
mal and clinical studies of gentamicin, netilmicin and tobramy-cin. J. Infect. Dis. 147:918-932.
22. Sanders, C. C., and C. Watanakunakorn. 1986. Emergence ofresistance to f-lactams, aminoglycosides and quinolones duringcombination therapy for infection due to Serratia marcescens.
J. Infect. Dis. 153:617-619.23. Taber, H. W., J. P. Mueller, P. F. Miller, and A. S. Arrow. 1987.
Bacterial uptake of aminoglycoside antibiotics. Microbiol. Rev.51:439-457.
24. Washington, J. A., II, and V. L. Sutter. 1980. Dilution suscep-tibility test: agar and macro-broth dilution procedures, p. 453-458. In E. H. Lennette, A. Balows, W. J. Hausler, Jr., and J. P.Truant (ed.), Manual of clinical microbiology, 3rd ed. AmericanSociety for Microbiology, Washington, D.C.
on June 24, 2018 by guesthttp://aac.asm
.org/D
ownloaded from


















