Immuno flow cytometry
8
Immunoflow cytometry and cell block immunohistochemistry in the FNA diagnosis of lymphoma: a review of 73 consecutive cases Frederick Mayall, Michael Dray, Dianne Stanley, Barbara Harrison, Robin Allen Abstract Aims—To review the results of 73 consecu- tive fine needle aspirations (FNAs) that were collected by a pathologist and ana- lysed by immunoflow cytometry. Material for a cell block was also collected from some of these lesions. Methods—The setting was a large general hospital in rural New Zealand. The FNAs were performed by a pathologist, or a radiologist for image guided localisations. Material for immunoflow cytometry was collected into RPMI and, when required, material for a cell block was collected into formalin. Results—Of the 73 samples collected by FNA nine were inadequate. Light chain restriction could be demonstrated in most FNA samples from B cell lymphomas (28 of 30 adequate samples). The exceptions were two cases of T cell rich B cell lymphoma. Artefactual light chain re- striction was seen occasionally in T cell lymphomas, presumably as a result of autoantibodies binding to the cell sur- faces. It was possible to subtype most (18 of 30 adequate samples) B cell lymphomas as chronic lymphocytic leukaemia (CLL), follicle centre cell lymphoma (FCCL), or mantle cell lymphoma. The CD4 to CD8 ratio was not usually restricted in T cell lymphomas and coexpression of CD4 and CD8 was not usually found. Loss of pan-T cell antigens was seen in some T cell lym- phomas. Four of the six T cell lymphomas and three of the four non-lymphoid malig- nancies were diagnosed with the aid of cell block immunohistochemistry. Only one of the four cases of Hodgkin’s lymphoma showed Reed-Sternberg cells in the FNA smears. Conclusions—It is not always possible to characterise lymphomas as fully with FNA and immunoflow cytometry as is possible with biopsy histology and a full battery of modern investigations. Nevertheless, in the setting of a large rural general hospital immunoflow cytometry on FNA samples is a highly eVective method of diagnosing and typing B cell lymphomas. Immunoflow cytometry is of little use for T cell lymphomas or Hodg- kin’s lymphomas. We advocate the use of cell block immunohistochemistry in pref- erence to immunoflow cytometry for cases in which the cytological appearance of the specimen is overtly malignant but the diVerential diagnosis includes non- lymphoid malignancy. (J Clin Pathol 2000;53:451–457) Keywords: lymphoma; flow cytometry; cell blocks; immunolabelling; fine needle aspiration In the past, the cytological diagnosis of lymphomas from fine needle aspiration (FNA) samples has been particularly diYcult. Usually, one obtains a sample that is either obviously malignant but equivocally lymphoid or, con- versely, a sample that is obviously lymphoid but equivocally malignant. However, recently FNA diagnosis of lymphoid lesions has been made easier by the arrival of immunoflow cytometry in most large pathology laboratories. Immuno- flow cytometry has been used mainly for the analysis of haematological diseases, but in- creasingly it is being used by cytologists. Early studies of FNAs and immunoflow cytometry used a limited range of antibodies and were not able to perform dual staining. Recently, there have been substantial advances in the sophisti- cation of the methods and equipment used for flow cytometry. It is accepted that FNA cytol- ogy with immunolabelled flow cytometry can, in some circumstances, serve as a replacement for open biopsy and conventional histology and immunohistochemistry. 12 However, FNA with immunoflow cytometry is not always success- ful. Scanty cellularity in the sample can prevent a satisfactory analysis, and even with an adequate sample the results might be mislead- ing. In particular, non-lymphoid malignancies can be hard to distinguish from lymphoid lesions if the sample also contains reactive lym- phoid cells; B cell lymphomas sometimes do not exhibit light chain restriction; and T cell lymphomas can have a large population of reactive B cells. The aim of our study was to review the results of 73 consecutive FNAs that were collected by a pathologist and analysed by immunoflow cytometry. Material for a cell block was also collected from some of these lesions. The setting was a large general hospital in rural New Zealand. The FNAs were performed over a two year period. In this time, approximately 800 FNAs of non-breast lesions were performed together with approximately 1400 breast FNAs. Methods The FNAs were performed by one of two mobile pathologists with an interest in FNA cytology, except for image guided FNAs, in J Clin Pathol 2000;53:451–457 451 Department of Pathology, Waikato Hospital, Private Bag 3200, Hamilton, New Zealand F Mayall M Dray D Stanley B Harrison R Allen Correspondence to: Dr Mayall email: [email protected] Accepted for publication 4 November 1999 group.bmj.com on May 24, 2012 - Published by jcp.bmj.com Downloaded from
-
Upload
syed-hassan-raza-naqvi -
Category
Documents
-
view
32 -
download
0
description
Immuno flow cytometry and cell block immunohistrochemistry in the FNA Diagnosis
Transcript of Immuno flow cytometry

Immunoflow cytometry and cell blockimmunohistochemistry in the FNA diagnosis oflymphoma: a review of 73 consecutive cases
Frederick Mayall, Michael Dray, Dianne Stanley, Barbara Harrison, Robin Allen
AbstractAims—To review the results of 73 consecu-tive fine needle aspirations (FNAs) thatwere collected by a pathologist and ana-lysed by immunoflow cytometry. Materialfor a cell block was also collected fromsome of these lesions.Methods—The setting was a large generalhospital in rural New Zealand. The FNAswere performed by a pathologist, or aradiologist for image guided localisations.Material for immunoflow cytometry wascollected into RPMI and, when required,material for a cell block was collected intoformalin.Results—Of the 73 samples collected byFNA nine were inadequate. Light chainrestriction could be demonstrated in mostFNA samples from B cell lymphomas (28of 30 adequate samples). The exceptionswere two cases of T cell rich B celllymphoma. Artefactual light chain re-striction was seen occasionally in T celllymphomas, presumably as a result ofautoantibodies binding to the cell sur-faces. It was possible to subtype most (18of 30 adequate samples) B cell lymphomasas chronic lymphocytic leukaemia (CLL),follicle centre cell lymphoma (FCCL), ormantle cell lymphoma. The CD4 to CD8ratio was not usually restricted in T celllymphomas and coexpression of CD4 andCD8 was not usually found. Loss of pan-Tcell antigens was seen in some T cell lym-phomas. Four of the six T cell lymphomasand three of the four non-lymphoid malig-nancies were diagnosed with the aid of cellblock immunohistochemistry. Only one ofthe four cases of Hodgkin’s lymphomashowed Reed-Sternberg cells in the FNAsmears.Conclusions—It is not always possible tocharacterise lymphomas as fully withFNA and immunoflow cytometry as ispossible with biopsy histology and a fullbattery of modern investigations.Nevertheless, in the setting of a large ruralgeneral hospital immunoflow cytometryon FNA samples is a highly eVectivemethod of diagnosing and typing B celllymphomas. Immunoflow cytometry is oflittle use for T cell lymphomas or Hodg-kin’s lymphomas. We advocate the use ofcell block immunohistochemistry in pref-erence to immunoflow cytometry forcases in which the cytological appearanceof the specimen is overtly malignant but
the diVerential diagnosis includes non-lymphoid malignancy.(J Clin Pathol 2000;53:451–457)
Keywords: lymphoma; flow cytometry; cell blocks;immunolabelling; fine needle aspiration
In the past, the cytological diagnosis oflymphomas from fine needle aspiration (FNA)samples has been particularly diYcult. Usually,one obtains a sample that is either obviouslymalignant but equivocally lymphoid or, con-versely, a sample that is obviously lymphoid butequivocally malignant. However, recently FNAdiagnosis of lymphoid lesions has been madeeasier by the arrival of immunoflow cytometryin most large pathology laboratories. Immuno-flow cytometry has been used mainly for theanalysis of haematological diseases, but in-creasingly it is being used by cytologists. Earlystudies of FNAs and immunoflow cytometryused a limited range of antibodies and were notable to perform dual staining. Recently, therehave been substantial advances in the sophisti-cation of the methods and equipment used forflow cytometry. It is accepted that FNA cytol-ogy with immunolabelled flow cytometry can,in some circumstances, serve as a replacementfor open biopsy and conventional histology andimmunohistochemistry.1 2 However, FNA withimmunoflow cytometry is not always success-ful. Scanty cellularity in the sample can preventa satisfactory analysis, and even with anadequate sample the results might be mislead-ing. In particular, non-lymphoid malignanciescan be hard to distinguish from lymphoidlesions if the sample also contains reactive lym-phoid cells; B cell lymphomas sometimes donot exhibit light chain restriction; and T celllymphomas can have a large population ofreactive B cells.
The aim of our study was to review theresults of 73 consecutive FNAs that werecollected by a pathologist and analysed byimmunoflow cytometry. Material for a cellblock was also collected from some of theselesions. The setting was a large general hospitalin rural New Zealand. The FNAs wereperformed over a two year period. In this time,approximately 800 FNAs of non-breast lesionswere performed together with approximately1400 breast FNAs.
MethodsThe FNAs were performed by one of twomobile pathologists with an interest in FNAcytology, except for image guided FNAs, in
J Clin Pathol 2000;53:451–457 451
Department ofPathology, WaikatoHospital, Private Bag3200, Hamilton, NewZealandF MayallM DrayD StanleyB HarrisonR Allen
Correspondence to:Dr Mayallemail: [email protected]
Accepted for publication4 November 1999
group.bmj.com on May 24, 2012 - Published by jcp.bmj.comDownloaded from

which case one of these pathologists preparedthe slides after the radiologist had aspirated thelesion. The FNAs performed by the patholo-gists were done with a needle only technique,using a 23 or 25 gauge 1.25 inch (3 cm) needle.The slides were air dried, often aided by a smallhair dryer, and DiV-Quik® stained (DadeBehring Diagnostics, Newmarket, Auckland,New Zealand). The slides were then examinedwith a portable Olympus CHK microscopeand a hand written report was issued within afew minutes. If this examination of thespecimen suggested that the lesion might belymphoid and lymphoma seemed possible,then a second FNA was performed, still using aneedle only technique, to collect a second sam-ple. This sample was collected quickly and theneedle was washed through with 3 ml ofheparin RPMI (12.8 mg of heparin ammo-nium in 45 ml of RPMI) within a few secondsof being collected. The reason for the urgencywas that a clotted sample reduces the yield ofcells for flow cytometry. Early in our experi-ence with collecting specimens for flow cyto-metry we washed needles through with sterileheparin saline before the FNA was performed,but we found that this was not necessary. Theslides were taken back to the laboratory to bemounted and examined again. The specimenin RPMI was taken to the haematology labora-tory, transferred to a 5 ml tube and centrifugedfor two minutes at approximately 400 ×g. Thesupernatant was discarded and the cells wereresuspended in 2 ml of ammonium chloridelysis solution. The cells were gently vortexed,incubated at room temperature for 10 minutes,and then centrifuged again for two minutes.The leucocytes were then resuspended in 2 mlof phosphate buVered saline (PBS). If debriswas present, it was removed with a nylon Swissscreen filter. An approximate cell count wasperformed and a panel of directly conjugatedmonoclonal antibodies was selected (table 1)(Immunotech Inc, Westbrook, Maine, USA).The cells and the antibodies were incubated for20 minutes in the dark at room temperature.These were then washed once in PBS, spundown, and then washed again. They were thenanalysed with the flow cytometer. Material forê and ë light chain analysis was treated diVer-ently. The centrifuged sample in RPMI wasincubated with prewarmed PBS for 20–30minutes at 37°C, to remove the cytophilicimmunoglobulin, and then centrifuged. Thesupernatant was discarded and if red bloodcells were present they were lysed with ammo-
nium chloride as above. Cells were thenincubated with antibodies (against CD19/êlight chain or CD19/ë light chain) as above.
The “first run” panel of antibodies evolvedas our experience developed and with theacquisition of a new immunoflow cytometerapproximately half way through our study. Atthe start of the study, a Coulter PROFILE IIwas used but later the laboratory obtained aCoulter EPICS® XL (Beckman Coulter Inc,Fullerton, California, USA). In some cases weperformed a “second run” with a more special-ised panel to investigate a specific diagnosis.The panel of antibodies used was sometimesrestricted by the scarcity of cells. In these cases,antibodies against CD19/ê light chain andCD19/ë light chain were given priority.
In our laboratory we have adopted lightchain ratio limits from previous studies.2–4 A êto ë ratio of greater than 3 or a ë to ê ratio ofgreater than 2 was accepted as evidence ofmonoclonality.
For some cases, cell blocks for immunohisto-chemistry were collected as describedpreviously.5 These were usually taken after theinitial FNA showed overtly malignant cytologybut it was not certain that the lesion waslymphoid in nature.
ResultsTable 2 shows our results—the cases are set inchronological order within each diagnostic cat-egory. It can be seen that the range of cellmarkers expanded during the course of ourstudy. The panel of markers was sometimestailored a little in view of the initial diagnosis,so as to focus on a particular issue and to avoidwasting cells.
DiscussionNine of the 73 samples (12%) had inadequatecells for analysis. Four of these were frombenign lymph nodes. It was felt that adequatesamples were easier to obtain from malignantlesions simply because of their larger size.Young et al found that five of 107 (4.7%) oftheir specimens were inadequate in a similarstudy.2 A highly cellular lymphoma aspiratemight exhibit uniform negativity on immuno-flow cytometry if the cells are necrotic, as incase 3.
Twenty eight cases exhibited light chainrestriction (defined above), allowing an un-equivocal diagnosis of B cell lymphoma to bemade on the FNA sample alone. On review ofthe notes at the end of our study, we could findno evidence that any of these diagnoses wereincorrect. Case 48 had been thought to be sus-picious of lymphoma with a ê to ë ratio of 1.95.However, a review of the notes about a yearafter the FNA was performed revealed no clearevidence that the patient had developedlymphoma. In particular, there was no evi-dence of lymphoma on a computed tomogra-phy scan. Case 73 also had a marginal lightchain ratio but did not have clinically evidentlymphoma eight months later.
Five of the 33 B cell lymphomas did notexhibit light chain restriction. For three casethis was because of inadequate cellularity. The
Table 1 Antibodies and their fluorochrome labels
Antibody Fluorochrome
CD2 FITCCD3 FITCCD4/CD8 FITC/PECD5 PECD10 FITCCD19 FITCCD20 FITCCD23 FITCFMC7 FITCSm IgM FITCCD19/ê chain PE/FITCCD19/ë chain PE/FITC
FITC, fluorescein isothiocyanate; PE, phycoerythrin.
452 Mayall, Dray, Stanley, et al
group.bmj.com on May 24, 2012 - Published by jcp.bmj.comDownloaded from

Tabl
e2
Imm
unofl
owcy
tom
etry
resu
ltsfr
om73
susp
ecte
dly
mph
omas
toge
ther
with
cell
bloc
kan
dbi
opsy
hist
olog
y
Cas
eS
iteM
etho
dIn
itial
diag
nosi
s
Perc
enta
geof
cells
posi
tive
(num
bers
indi
cate
CD
num
bers
)
Fin
aldi
agno
sis
23
45
810
1920
23Ig
MF
MC
719
/ê19
/ë5/
194/
8
Bce
llly
mph
oma
1A
bd
omin
alm
ass
IS
usp
.of
lym
ph
oma
21
13
9897
7585
98<
1D
iVu
sela
rge
Bce
llly
mph
oma
2B
ase
ofn
eck
MB
enig
n/ly
mp
hom
a4
445
28
CL
L3
Ln
eck
MN
ecro
tic
lym
phom
aIn
adeq
uat
e(n
ecro
tic
asa
resu
ltof
chem
othe
rapy
)F
CC
L(f
rom
pre
viou
shi
stor
y)4
Ste
rnal
mas
sI
Mye
lom
aIn
adeq
uat
eM
yelo
ma
(on
cell
bloc
kh
isto
logy
)5
Rgr
oin
nod
eM
Su
sp.o
fC
LL
1213
174
575
CL
L6
Lp
oste
rior
nec
kM
Su
sp.o
fC
LL
9990
488
88C
LL
7R
pos
tn
eck
MS
usp
.of
FC
CL
915
81P
rob
able
FC
CL
8R
par
aver
tebr
alI
Su
sp.o
fC
LL
62
53
283
82<
1C
LL
9L
nec
kM
Pro
babl
eca
rcin
oma
9841
9048
117
12T
cell
rich
Bce
llly
mph
oma
(on
bio
psy
his
tolo
gy)
10R
nec
kM
“Hig
hgr
ade”
lym
phom
aIn
adeq
uat
eD
iVu
sela
rge
Bce
llly
mph
oma
(on
bio
psy
his
tolo
gy)
11R
nec
kM
Nec
roti
cly
mp
hom
a6
48
491
4288
5086
8F
CC
L12
Rin
guin
alM
Lym
ph
oma
1616
8184
844
8167
741
FC
CL
13L
ingu
inal
MS
usp
.of
lym
ph
oma
93
13
9299
3434
1792
<1
<1
DiV
use
larg
eB
cell
lym
phom
a14
Rax
illar
yn
ode
ML
ymp
hom
a20
2119
213
7878
8016
6978
771
2F
CC
L15
Bas
eof
nec
kM
Lym
ph
oma
1918
1228
5<
181
<1
489
293
81D
iVu
sela
rge
Bce
llly
mph
oma
16L
nec
kM
Lym
phoi
dce
lls54
7013
2731
397
22<
1B
cell
lym
phom
a,ex
act
type
un
cert
ain
17A
bd
omin
alm
ass
ML
ymp
hom
a24
1327
868
5879
31
56<
1F
CC
L18
Rn
eck
MS
usp
.of
lym
ph
oma
5834
143
3943
139
3B
cell
lym
ph
oma,
exac
tty
pe
un
cert
ain
19L
nec
kM
Su
sp.o
fly
mp
hom
a21
1599
5<
180
5579
588
1969
79<
1C
LL
20R
bre
ast
ML
ymp
hom
a2
55
100
61
9999
1499
992
9799
Man
tle
cell
lym
ph
oma
21L
sup
racl
avic
ula
rM
Pos
sib
lely
mp
hom
a10
133
7085
873
8353
801
65
FC
CL
22L
nec
kM
Pos
sib
leC
LL
4133
9910
<1
6142
3637
13
4557
<1
CL
L23
Lsu
pra
clav
icu
lar
MP
revi
ous
CL
L13
989
32
9979
8484
2881
188
<1
CL
L24
Lp
arot
idM
Lym
ph
oma
42
100
11
9799
1298
595
97<
1M
antl
ece
llly
mp
hom
a25
Rn
eck
ML
ymp
hom
a29
1524
1156
6461
1273
7755
52
1F
CC
L26
Rn
eck
ML
ymp
hom
a18
9396
1290
16F
CC
L27
Rn
eck
ML
ymp
hom
a13
207
2079
8711
804
66<
1<
1B
cell
lym
ph
oma,
exac
tty
pe
un
cert
ain
28L
nec
kM
Lym
ph
oma
1813
208
7825
814
7873
726
<1
<1
FC
CL
29A
bd
omin
alm
ass
IL
ymp
hom
a17
1316
274
8283
8184
8282
11
1F
CC
L30
Rsu
bm
and
ibu
lar
ML
ymp
hom
a41
4329
8824
3356
1433
1410
136
38F
CC
L(f
rom
pre
viou
sh
isto
ry)
31R
ingu
inal
MIn
farc
ted
tiss
ue
6639
6025
131
264
2027
164
34
Bce
llly
mph
oma,
exac
tty
peu
nce
rtai
n32
Rn
eck
MS
can
tyce
lls1
9090
26B
cell
lym
phom
a,ex
act
type
un
cert
ain
33R
nec
kM
Lym
phom
a87
96
6T
cell
rich
Bce
llly
mph
oma
(on
bio
psy
his
tolo
gy)
Tce
llly
mph
oma
34L
nec
kM
Mal
ign
ant
6817
5160
40<
17
37P
erip
hera
lTce
llly
mph
oma
(on
cell
bloc
kh
isto
logy
)35
Ln
eck
MM
alig
nan
t70
<1
1610
13P
erip
hera
lTce
llly
mph
oma
(on
cell
bloc
kh
isto
logy
)36
Rca
lfM
Lym
phom
a98
596
9511
115
11
<1
<1
Per
iphe
ralT
cell
lym
phom
a(o
nce
llbl
ock
his
tolo
gy)
37R
back
MM
alig
nan
t22
21
15
1722
531
1<
1<
1P
erip
hera
lTce
llly
mph
oma
(on
bio
psy
his
tolo
gy)
38P
erih
epat
icm
ass
IL
ymph
oma/
ca.
8062
7810
<1
712
55
<1
<1
Per
iphe
ralT
cell
lym
phom
a(o
nb
iops
yh
isto
logy
)39
Lin
guin
alM
Lym
phom
a/ca
.70
4226
330
305
5P
erip
hera
lTce
llly
mph
oma
(on
cell
bloc
kh
isto
logy
)H
odgk
in’s
lym
phom
a40
Lsu
prac
lavi
cula
rM
Inad
equ
ate
cells
Inad
equ
ate
Hod
gkin
’sly
mp
hom
a(o
nb
iop
syh
isto
logy
)41
Med
iast
inu
mI
Rea
ctiv
e90
7787
202
119
239
96
53
<1
Hod
gkin
’sly
mph
oma
(on
bio
psy
his
tolo
gy)
42L
nec
kM
Rea
ctiv
e69
3115
20H
odgk
in’s
lym
phom
a(o
nb
iops
yh
isto
logy
)43
Ln
eck
MH
odgk
in’s
lym
ph
oma
Inad
equ
ate
Hod
gkin
’sly
mp
hom
aN
on-l
ymph
oid
tum
ours
44M
edia
stin
um
IT
hym
oma/
lym
ph
oma
1953
9499
905
23
3T
hym
oma
(on
cell
blo
ckan
db
iop
syh
isto
logy
)45
Par
aver
tebr
alm
ass
IC
arci
nom
a/ly
mp
hom
a67
4320
2418
11A
den
ocar
cin
oma
(on
bio
psy
his
tolo
gy)
46R
brea
stM
Car
cin
oma/
lym
phom
aN
oly
mph
oid
cells
Bre
ast
carc
inom
a(o
nce
llbl
ock
his
tolo
gy)
47R
supr
acla
vicu
lar
MC
arci
nom
a/ly
mph
oma
No
lym
phoi
dce
llsS
mal
lcel
lcar
cin
oma
(on
cell
bloc
kh
isto
logy
)B
enig
n48
Lpa
roti
dm
ass
MS
iala
den
itis
6034
5713
146
4750
4121
<1
<1
Su
sp.B
cell
lym
phom
a(b
ut
no
over
tly
mph
oma
aye
arla
ter)
49R
nec
kM
Ben
ign
Inad
equ
ate
Ben
ign
Flow cytometry and immunohistochemistry in lymphoma diagnosis 453
group.bmj.com on May 24, 2012 - Published by jcp.bmj.comDownloaded from

other two (cases 9 and 33) were particularlyconfusing because the cytology showed amalignant tumour with highly atypical cellsmixed with benign looking lymphoid cells. Theflow cytometry showed no evidence of lightchain restriction. Biopsies were taken and theflow cytometry results from these were similarto those from the FNA. However, paraYn waxembedded sections and immunohistochemis-try showed that the large highly atypical cellswere CD45 and CD20 positive and negativefor cytokeratin, S100, and CD3. Thus, a diag-nosis of T cell rich B cell lymphoma was made.We assumed that the neoplastic B cells werenot expressing light chains strongly or were“swamped” by a population of reactive B cells.
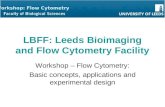
Except for cases 9 and 33, the lowest lightchain ratio of any B cell lymphoma was a ë to êratio of 3.1 (case 16). Case 37 was remarkablein that it showed artefactual light chain restric-tion in a T cell lymphoma (fig 1). We assumethat this was as a result of specific binding of êto the surface of the tumour cells, perhaps as anautoimmune response to the tumour cells. Thelymphoma occurred in a patient with AIDS.On biopsy, the tumours cells were stronglypositive for CD3 but negative for CD20.Fortunately, this artefact did not confuse thediagnosis, because coexpression of light chainwith CD19 was not found.
For 18 cases it was possible to make a diag-nosis of B cell lymphoma and also subtype thelymphoma as either CLL (chronic lymphocyticleukaemia/small lymphocytic lymphoma),FCCL (follicle centre cell lymphoma), or man-tle cell lymphoma. Most of the other cases thatexhibited light chain restriction were called “Bcell lymphoma, exact type uncertain” or“diVuse large B cell lymphoma” if they werecomposed of overtly malignant large cells.Uncertainty as to the exact type of B celllymphoma was not considered suYcient reasonto perform a biopsy. This was usually becausethe patient had other medical problems thatwere a more immediate risk to the patient’shealth or because exact typing would not altertreatment.
Four of the six T cell lymphomas were diag-nosed with a combination of cytology, flowcytometry, and cell block immunohistochemis-try, but for two it was not possible to collect acell block. Both of these then had biopsies. Theparticipation of the pathologist in the collec-tion of the specimen and the immediate assess-ment of the cytology meant that the need forcell block histology had been anticipated. Theratio of CD4 to CD8 (or CD8 to CD4) wasexamined but this was not usually useful in therecognition of T cell lymphoma. The benignlesions in cases 59 and 65 had CD4 to CD8ratios of 4.15 and 4.29, respectively. Only twoof the six T cell lymphomas had CD4 to CD8(or CD8 to CD4) ratios greater than these. Jef-fers et al describe one case of T cell lymphomain their series of 46 FNA sampled lesions.6 Thislymphoma showed subset restriction, withmore than 90% of T cells expressing CD8.Coexpression of CD4 and CD8 was examinedfor four of the six T cell lymphomas but wasonly found in case 34. Loss of pan-T cell anti-Ta
ble
2Im
mun
oflow
cyto
met
ryre
sults
from
73su
spec
ted
lym
phom
asto
geth
erw
ithce
llbl
ock
and
biop
syhi
stol
ogy
Cas
eS
iteM
etho
dIn
itial
diag
nosi
s
Perc
enta
geof
cells
posi
tive
(num
bers
indi
cate
CD
num
bers
)
Fin
aldi
agno
sis
23
45
810
1920
23Ig
MF
MC
719
/ê19
/ë5/
194/
8
50R
nec
kM
Ben
ign
4938
5767
184
1914
259
1616
3G
ran
ulo
mat
ous
infl
amm
atio
n51
Lax
illa
MB
enig
nIn
adeq
uat
eB
enig
n52
Lpa
roti
dM
Pro
babl
yb
enig
n30
3146
2317
Tox
opla
smos
is(c
linic
ally
)53
Ln
eck
MB
enig
n38
3823
142
4256
4033
25B
enig
n54
Rn
eck
MB
enig
nIn
adeq
uat
eB
enig
n55
Rin
frac
lavi
cula
rM
Ben
ign
Inad
equ
ate
Ben
ign
56R
nec
kM
Ben
ign
2318
6<
176
1322
Ben
ign
57R
nec
kM
Ben
ign
5870
5551
1437
233
2714
Ben
ign
58L
nec
kM
Ben
ign
8625
1811
Ben
ign
59R
nec
kM
Ben
ign
6154
1315
4019
19<
1B
enig
n60
Rn
eck
MB
enig
n89
6188
251
1214
86
54
<1
Ben
ign
61P
erip
orta
lnod
eI
Ben
ign
9063
262
1212
410
23
11
Ben
ign
62L
nec
kM
Ben
ign
<1
2315
1110
Ben
ign
63R
sup
racl
avic
ula
rM
Ben
ign
4831
4415
<1
5458
2145
2919
1<
1B
enig
n64
Ln
eck
MB
enig
n84
5881
20<
119
197
1116
102
2B
enig
n65
Rn
eck
MB
enig
n44
3039
7<
160
6036
4025
1<
1B
enig
n66
Ln
eck
MB
enig
n58
3653
151
4445
1121
3420
91
<1
Ben
ign
67S
aliv
ary
glan
dM
Ben
ign
2010
186
7781
7578
45<
1<
1B
enig
n68
Rin
guin
alM
Ben
ign
7052
6816
<1
3217
2813
2813
12<
1<
1B
enig
n69
Lax
illa
MB
enig
n76
6282
296
2234
1541
3838
<1
<1
Ben
ign
70L
par
otid
MB
enig
n71
5375
16<
121
911
1011
2212
62
Ben
ign
71R
nec
kM
Ben
ign
5354
5050
12<
141
411
2923
2022
<5
<1
Ben
ign
72M
edia
stin
alm
ass
IB
enig
n60
3666
203
3641
3034
228
910
<1
Ben
ign
ency
sted
sero
us
flu
id73
Ln
eck
MP
ossi
ble
lym
ph
oma
21<
188
4723
Su
sp.B
cell
lym
ph
oma
(bu
tn
oov
ert
lym
ph
oma
1.5
year
sla
ter)
Ca.
,car
cin
oma;
CL
L,c
hron
icly
mph
ocyt
icle
uka
emia
;FC
CL
,fol
licle
cen
tre
cell
lym
phom
a;F
NA
,fin
en
eed
leas
pira
tion
;I,i
mag
egu
ided
FN
A;L
,lef
t;M
,man
ual
lygu
ided
FN
A;R
,rig
ht;s
usp
.,su
spic
iou
s.
454 Mayall, Dray, Stanley, et al
group.bmj.com on May 24, 2012 - Published by jcp.bmj.comDownloaded from

gens was seen in cases 34 and 37. Zardawi et alhave stated that the loss of one or more pan-Tcell antigen allows a firm diagnosis of T celllymphoma to be made (in the correct clinicalcontext).4 It should be remembered thatimmature thymic T cells exhibit loss of pan-Tcell antigens, as in case 44.
The cytological diagnosis of Hodgkin’slymphoma depends on the presence of typical
Reed-Sternberg cells. Flow cytometry does notcontribute except to exclude a monoclonal Bcell population. There were no definite Reed-Sternberg cells in the FNA samples of three ofour four cases. Because a diagnosis oflymphoma was suspected clinically, the nodeswere biopsied. One case did show abundantReed-Sternberg cells in the FNA sample and adiagnosis was made cytologically. The node
Figure 1 A scatter plot showing ê light chain restriction in a T cell lymphoma from a patient with AIDS (case 37). Therewas no coexpression of CD19 and ê, exemplifying the importance of dual staining in assessing light chain restriction.
% Count Mn X Mn Y PkPosX PkPosY PkCnt FPCVX FPCVY
B1 BB2 BB3 BB4 B
1.51.1
94.82.6
11787
7437203
0.5285.27
0.4041.51
1.142.08
0.3670.478
0.5765.36
0.1021.27
1.021.10
0.1020.619
63
789
58.5294.4467.3622.37
22.3485.6362.0756.50
Stats: Normalised, Listgating: DisabledRegion ID % Count Mn X Mn Y PkPosX PkPosY PkCnt FPCVX FPCVY
B1 B
Hist
2
Stats: Normalised, Listgating: DisabledRegion IDHist
2
B2 BB3 BB4 B
0.01.0
13.285.8
262
8405474
0.1587.04
0.3661.49
11.02.78
0.3810.497
0.1022.43
0.5761.10
10.21.58
0.6190.619
13
1325
43.51105.7947.8251.37
7.2066.6560.5260.29
Scale
Lambda–FITC
14731 C
D19
–PE
(128
× 1
28)
10001 2
4
B
100
10
1
0.10.1 1 100 100010
Scale
Kappa–FITC
12631 C
D19
–PE
(128
× 1
28)
10001 2
B3 4
100
10
1
0.10.1 1 100 100010
Flow cytometry and immunohistochemistry in lymphoma diagnosis 455
group.bmj.com on May 24, 2012 - Published by jcp.bmj.comDownloaded from

was excised before treatment and the diagnosiswas confirmed. We would not advocate thediagnosis of Hodgkin’s lymphoma being madeon FNA alone except in exceptional circum-stances. Young et al studied the cytology andflow cytometry of 107 aspirates of suspectedlymphoid lesions.2 Three of these were Hodg-kin’s lymphoma but none showed Reed-Sternberg cells in the FNA samples. Flowcytometry showed a polyclonal population.
There were four cases that had a finaldiagnosis of a non-lymphoid neoplasm. Theinitial diVerential diagnosis favoured a non-lymphoid tumour in each case but lymphomawas also thought to be possible. In one of thesepatients, a core biopsy was performed by aradiologist once the cytology had been exam-ined. Cell blocks were taken for the others.
There were 28 cases that seemed to bebenign on cytology and flow cytometry.However, two of these were clinically suspi-cious and had biopsies that showed them to beHodgkin’s lymphoma. None of the otherpatients had a biopsy and none had evidence oflymphoma when the notes were reviewed at theend of our study.
Before the widespread availability ofimmunoflow cytometry, immunofluorescentcytochemistry on cytospin preparations wasused in some large laboratories for the charac-terisation of lymphomas from FNA samples.This has the advantage that it can beperformed with fewer cells and it is not diYcultto appreciate the relation between the size ofthe cells and their antigen expression. The lat-ter makes it easier to diagnose some conditionssuch as T cell rich B cell lymphomas.Immunocytochemistry has some major disad-vantages. The technique is highly labour inten-sive and requires specially trained technicalstaV. Dual expression of markers is less easy todemonstrate. A result would usually takeconsiderably longer than the four hour turnaround time that we have for immunoflowcytometry. The number of cells that can becounted and the number of markers that can beused are restricted by the time it takes toperform manual counting. A higher light chainratio (about 6 : 1) is required to provemonoclonality,7 although in practice this rarelyalters the detection of monoclonality in asample.8 For these reasons, immunoflow cyto-metry is probably the preferred method exceptin a few specialist centres.
Young et al graded the follicle centre celllymphomas in their study2 according to theproportion of “transformed cells” in the smear.Their method was validated in a previousstudy.9 We did not attempt to do this because itwould rarely change the way in which thepatient was treated.
Eight of the 47 malignant lesions were diag-nosed using cell blocks. These comprised onecase of myeloma, four of the six T cell lympho-mas, and three of the four non-lymphoidmalignancies. This demonstrates the role ofcell block immunohistochemistry in the diag-nosis of suspected lymphoid neoplasms. Al-though immunoflow cytometry is highly eVec-tive in the diagnosis of B cell lymphomas,
particularly CLL, FCCL, and mantle celllymphoma, cell block immunohistochemistryis probably more useful for “high gradelymphomas”, especially peripheral T cell lym-phomas, and also for non-lymphoid neo-plasms. If a sample from a suspected lymphoidlesion is overtly malignant on cytological crite-ria then more information is likely to beobtained from a cell block, but if the sample isequivocally benign/malignant then immuno-flow cytometry is probably more useful.Ideally, tissue should be obtained for immuno-flow cytometry and a cell block, although inpractice this is often not possible.
Optimum diagnostic information might bebest obtained by biopsying every suspiciouslymph node and performing a battery of sophis-ticated investigations including oncogene ex-pression, cell kinetic studies, and detailedmolecular analysis. A biopsy might be particu-larly important if spare material is needed forresearch. However, only a few centres have thebudget, facilities, or expertise to do all of this. Wewould always advocate that an FNA diagnosedlymphoma in an otherwise fit young patientshould be followed by a biopsy. Most lympho-mas occur in elderly patients and are notcurable. In these patients, treatment and survivalare often influenced more by coexistent pathol-ogy, so that detailed analysis of the lymphomamight supply the clinician with a level of detailthat is superfluous. Despite the pitfalls that wereapparent in our study, FNA with immunoflowcytometry is a powerful technique for thediagnosis and typing of B cell lymphomas. Closecommunication between the oncologist andpathologist is needed to ensure that FNAsampling is performed on appropriate cases andthat the result and issues of uncertainty are con-veyed. In the setting of a large general hospital inrural New Zealand, the speed with which FNAcytology and immunoflow cytometry could beperformed (about four hours) was important. Itallowed patients who had travelled a longdistance to be given their result quickly, andallowed other investigations to be undertakenthe same day in preparation for treatment.
ConclusionsOur study shows that it is almost always possi-ble to obtain an adequate sample for immuno-flow cytometry from a fine needle aspirate.Light chain restriction could be demonstratedin almost all FNA samples from B cell lympho-mas. One notable exception was T cell rich Bcell lymphoma. Artefactual light chain restric-tion could occasionally be seen in T celllymphomas, presumably because of autoanti-bodies binding to the cell surfaces. It was pos-sible to subtype most B cell lymphomas asCLL, FCCL, or mantle cell lymphoma.Immunoflow cytometry is not particularlyhelpful in the diagnosis of T cell lymphoma orHodgkin’s lymphoma. The CD4 to CD8 ratiowas not usually restricted in T cell lymphomasand neither was coexpression of CD4 and CD8usually found. Loss of pan-T cell antigens wasseen in some T cell lymphomas. Four of the sixT cell lymphomas and three of the fournon-lymphoid malignancies were diagnosed
456 Mayall, Dray, Stanley, et al
group.bmj.com on May 24, 2012 - Published by jcp.bmj.comDownloaded from

with the aid of cell block immunohistochemis-try. We advocate the use of cell block immuno-histochemistry in preference to immunoflowcytometry for cases in which the cytologicalappearance of the specimen is overtly malig-nant but the diVerential diagnosis includesnon-lymphoid malignancy.
1 Skoog L, Tani E. The role of fine-needle aspiration cytologyin the diagnosis of non-Hodgkin’s lymphoma. Diagn Oncol1991;1:12–18.
2 Young NA, Al-Saleem TI, Ehya H, et al. Utilization of fine-needle aspiration cytology and flow cytometry in the diag-nosis and subclassification of primary and recurrentlymphoma. Cancer 1998;84:252–61.
3 Zander DS, Iturraspe JA, Everett ET, et al. Flow cytometry:in vitro assessment of its potential application for the diag-nosis and classification of lymphoid processes in cytologicalpreparations from fine-needle aspirates. Am J Clin Pathol1994;101:577–86.
4 Zardawi IM, Jain S, Bennett G. Flow-cytometric algorithmon fine-needle aspirates for the clinical workup of patientswith lymphadenopathy. Diagn Cytopathol 1998;19:274–8.
5 Mayall F, Chang B, Darlington A. A review of 50 consecu-tive cytology cell block preparations in a large general hos-pital. J Clin Pathol 1997;50:985–90.
6 JeVers MD, Milton J, Herriot R, et al. Fine needle aspirationcytology in the investigation of non-Hodgkins lymphoma. JClin Pathol 1998;51:189–96.
7 Sneige N, Dekmezian RH, Katz RL, et al. Morphologic andimmunocytochemical evaluation of 220 fine needle aspi-rates of malignant lymphoma and lymphoid hyperplasia.Acta Cytol 1990;34:311–22.
8 Robins DB, Katz RL, Swan F, et al. Immunotyping oflymphoma by fine needle aspiration: a comparative study ofcytospin preparations and flow cytometry. Am J Clin Pathol1994;101:569–76.
9 Young NA, Al-Saleem TI, Al-Saleem Z, et al. The value oftransformed lymphocyte count in subclassification of non-Hodgkin’s lymphoma by fine needle aspiration. Am J ClinPathol 1997;108:143–51.
Flow cytometry and immunohistochemistry in lymphoma diagnosis 457
group.bmj.com on May 24, 2012 - Published by jcp.bmj.comDownloaded from

doi: 10.1136/jcp.53.6.451 2000 53: 451-457J Clin Pathol
Frederick Mayall, Michael Dray, Dianne Stanley, et al. casesof lymphoma: a review of 73 consecutiveimmunohistochemistry in the FNA diagnosis Immunoflow cytometry and cell block
http://jcp.bmj.com/content/53/6/451.full.htmlUpdated information and services can be found at:
These include:
References
http://jcp.bmj.com/content/53/6/451.full.html#related-urlsArticle cited in:
http://jcp.bmj.com/content/53/6/451.full.html#ref-list-1This article cites 8 articles, 2 of which can be accessed free at:
serviceEmail alerting
box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in the
CollectionsTopic
(651 articles)Clinical diagnostic tests � (1296 articles)Immunology (including allergy) �
Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on May 24, 2012 - Published by jcp.bmj.comDownloaded from