Imaging of coronary atherosclerosis: intravascular ultrasound
17
REVIEW Imaging Imaging of coronary atherosclerosis: intravascular ultrasound Hector M. Garcia-Garcia 1 , Marco A. Costa 2 , and Patrick W. Serruys 1 * 1 Interventional Cardiology, Thoraxcenter, Erasmus MC, ’s-Gravendijkwal 230, 3015 CE Rotterdam, The Netherlands; and 2 Division of Cardiovascular Medicine, Harrington- McLaughlin Heart and Vascular Institute, University Hospitals, Case Western Reserve University, 11100 Euclid Ave. LKS 3001, Cleveland, OH 44106-5038, USA Received 4 March 2010; revised 1 July 2010; accepted 29 July 2010; online publish-ahead-of-print 7 September 2010 Atherosclerosis is the main cause of coronary heart disease, which is today the leading cause of death worldwide and will continue to be the first in the world in 2030. In the formation of atherosclerotic coronary lesions, a critical primary step is the accumulation and oxidation of low-density lipoprotein (LDL) particles. Oxidized-LDL favours leucocyte recruitment and their activation, as well as cell death. This leads to generation of complex atherosclerotic plaques. These plaques have a high content of necrotic core, a thin inflamed fibrous cap (intense accumulation of macrophages) and scarce presence of smooth muscle cells (i.e. thin-capped fibroatheroma). At early stages of the formation of the atheroma, the remodelling of the vessel wall usually prevents plaque from encroaching on the lumen, thereby masking the presence of atheroma on angiography. In contrast, greyscale intravascular ultrasound can fully assess the extension of the disease axially and longitudinally. This intravascular imaging technique has played a vital role in advancing our understanding of the pathophysiology of coronary artery disease, and in the development of novel cardiovascular drugs and device therapies. This intravascular imaging technology and its clinical and research applications are discussed in more detail below. ----------------------------------------------------------------------------------------------------------------------------------------------------------- Keywords Atherosclerosis † Imaging † Intravascular ultrasound Background Coronary angiography depicts arteries as a planar silhouette of the contrast-filled lumen. Importantly, angiography does not provide visualization of the vessel wall and is not suitable for assessment of atherosclerosis. Angiographic disease assessment is based on the comparison of the stenotic segment with the adjacent, ‘normal- appearing’ coronary, which is often an incorrect assumption due to the diffuse nature of atherosclerosis as shown by pathological and intravascular ultrasound (IVUS) studies 1,2 (Figure 1). Intravascular ultrasound Imaging formation The IVUS image is the result of reflected ultrasound waves that are converted to electrical signals and sent to an external processing system for amplification, filtering, and scan conversion. Greyscale IVUS imaging is formed by the envelope (amplitude) of the radio- frequency signal (Figure 2). More recently, autoregressive spectral analysis of IVUS backscat- tered data has been incorporated into conventional IVUS systems to facilitate image interpretation of different tissue components. The first commercially available IVUS backscattering image analysis, named virtual histology (TM) (IVUS-VH), was built on the electronic 20 MHz IVUS platform. In contrast iMAP is an imaging modality for atherosclerotic plaque tissue characterization based on pattern recognition 3 and integrated baskscattered (IB) IVUS values are calculated as the average power, measured in decibels, of the ultrasound signal backscattered using a fast Fourier transformation 4 (Figure 2). Lately, a rotational mechanical 45 MHz IVUS system has also integrated the classification tree for virtual histology tissue characterization (Figure 3). Another approach is to assess the deformability of coronary plaque using also the analysis of radiofrequency signals at different diastolic pressure levels using palpography. This allows the construction of a ‘strain’ image, in which harder (low strain) and softer (high strain) regions of the coronary arteries can be identified, with radial strain values ranging between 0 and 2% (Figure 2). High strain regions have been associated with a necrotic core rich and inflamed plaques. 5 * Corresponding author. Tel: +31 10 7035260, Fax: +31 10 4369154, Email: [email protected] Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2010. For permissions please email: [email protected]. doi:10.1093/eurheartj/ehq280 European Heart Journal (2010) 3, 2456–2469 Downloaded from https://academic.oup.com/eurheartj/article/31/20/2456/613364 by guest on 24 November 2021
Transcript of Imaging of coronary atherosclerosis: intravascular ultrasound

REVIEW
Imaging
Imaging of coronary atherosclerosis:intravascular ultrasoundHector M. Garcia-Garcia1, Marco A. Costa2, and Patrick W. Serruys1*
1Interventional Cardiology, Thoraxcenter, Erasmus MC, ’s-Gravendijkwal 230, 3015 CE Rotterdam, The Netherlands; and 2Division of Cardiovascular Medicine, Harrington-McLaughlin Heart and Vascular Institute, University Hospitals, Case Western Reserve University, 11100 Euclid Ave. LKS 3001, Cleveland, OH 44106-5038, USA
Received 4 March 2010; revised 1 July 2010; accepted 29 July 2010; online publish-ahead-of-print 7 September 2010
Atherosclerosis is the main cause of coronary heart disease, which is today the leading cause of death worldwide and will continue to be thefirst in the world in 2030. In the formation of atherosclerotic coronary lesions, a critical primary step is the accumulation and oxidation oflow-density lipoprotein (LDL) particles. Oxidized-LDL favours leucocyte recruitment and their activation, as well as cell death. This leads togeneration of complex atherosclerotic plaques. These plaques have a high content of necrotic core, a thin inflamed fibrous cap (intenseaccumulation of macrophages) and scarce presence of smooth muscle cells (i.e. thin-capped fibroatheroma). At early stages of the formationof the atheroma, the remodelling of the vessel wall usually prevents plaque from encroaching on the lumen, thereby masking the presence ofatheroma on angiography. In contrast, greyscale intravascular ultrasound can fully assess the extension of the disease axially and longitudinally.This intravascular imaging technique has played a vital role in advancing our understanding of the pathophysiology of coronary artery disease,and in the development of novel cardiovascular drugs and device therapies. This intravascular imaging technology and its clinical and researchapplications are discussed in more detail below.- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -Keywords Atherosclerosis † Imaging † Intravascular ultrasound
BackgroundCoronary angiography depicts arteries as a planar silhouette of thecontrast-filled lumen. Importantly, angiography does not providevisualization of the vessel wall and is not suitable for assessmentof atherosclerosis. Angiographic disease assessment is based onthe comparison of the stenotic segment with the adjacent, ‘normal-appearing’ coronary, which is often an incorrect assumption due tothe diffuse nature of atherosclerosis as shown by pathological andintravascular ultrasound (IVUS) studies1,2 (Figure 1).
Intravascular ultrasound
Imaging formationThe IVUS image is the result of reflected ultrasound waves that areconverted to electrical signals and sent to an external processingsystem for amplification, filtering, and scan conversion. GreyscaleIVUS imaging is formed by the envelope (amplitude) of the radio-frequency signal (Figure 2).
More recently, autoregressive spectral analysis of IVUS backscat-tered data has been incorporated into conventional IVUS systemsto facilitate image interpretation of different tissue components.The first commercially available IVUS backscattering image analysis,named virtual histology(TM) (IVUS-VH), was built on the electronic20 MHz IVUS platform. In contrast iMAP is an imaging modality foratherosclerotic plaque tissue characterization based on patternrecognition3 and integrated baskscattered (IB) IVUS values arecalculated as the average power, measured in decibels, of theultrasound signal backscattered using a fast Fourier transformation4
(Figure 2). Lately, a rotational mechanical 45 MHz IVUS system hasalso integrated the classification tree for virtual histology tissuecharacterization (Figure 3).
Another approach is to assess the deformability of coronary plaqueusing also the analysis of radiofrequency signals at different diastolicpressure levels using palpography. This allows the construction of a‘strain’ image, in which harder (low strain) and softer (high strain)regions of the coronary arteries can be identified, with radial strainvalues ranging between 0 and 2% (Figure 2). High strain regionshave been associated with a necrotic core rich and inflamed plaques.5
* Corresponding author. Tel: +31 10 7035260, Fax: +31 10 4369154, Email: [email protected]
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2010. For permissions please email: [email protected].
doi:10.1093/eurheartj/ehq280European Heart Journal (2010) 3, 2456–2469
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/20/2456/613364 by guest on 24 N
ovember 2021

Catheter designsThe IVUS equipment consists of a catheter incorporating a minia-turized transducer and a console to reconstruct and display theimage (Figure 4). Current catheters range from 2.6 to 3.2 Frenchin size and can be introduced through conventional 6-Frenchguide catheters. Rotational, mechanical IVUS probes rotate asingle piezoelectric transducer at 1800 r.p.m. and operate at fre-quencies between 30 and 45 MHz while electronic phased-arraysystems operate at a centre-frequency of �20 MHz. Higher ultra-sound frequencies are associated with better image resolution; butincreasing the frequency beyond 45 MHz has been limited becauseof decreased tissue penetration.6,7 Electronic systems have up to64 transducer elements in an annular array that are activatedsequentially to generate the cross-sectional image. In general, elec-tronic catheter designs are slightly easier to set up and use,whereas mechanical probes offer superior image quality. Electronic
IVUS catheters have the ability to display blood flow in colour tofacilitate distinction between lumen and wall boundaries.
Combined intravascular imagingcathetersAnother imaging modality able to characterize coronary athero-sclerosis (i.e. lipid core) invasively is NIR spectroscopy (NIRS).8
To this aim, the 3.2F FDA-approved near infrared spectroscopycatheter is used. This catheter is compatible with a conventional0.014′ guidewire, contains a rotating (240 Hz) NIRS light sourceat its tip, and is pulled back by a motor drive unit at 0.5 mm/s.9
A newer catheter has been introduced. The 3.2F rapid exchangeApollo catheter combines a 40 MHz real-time IVUS catheterwith a standard NIRS catheter (Figure 5). In the SPECTACL (SPEC-Troscopic Assessment of Coronary Lipid) trial, which was a paral-lel first-in-human multicentre study designed to demonstrate the
Figure 1 This figure illustrates the nature of heterogeneity of the atherosclerosis disease and the lack of correlation of intravascular ultra-sound findings (A–D) and angiography appearance (E). Patient presented with stable angina due to a significant lesion in the right coronaryartery which was stented (not shown). A greyscale IVUS pullback in the left anterior descending was performed in order to better characterizethe mild lesion present in its mid segment. (A) Shows a large eccentric plaque in the ostium of the left anterior descending that angiographicallyhas minimum lumen compromise. (B) Depicts a soft concentric plaque. (C) Shows a mixed plaque. (D) Depicts an eccentric, soft lesion.
Imaging of coronary atherosclerosis 2457D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

applicability of the lipid core plaques detection algorithm in 106living patients, it has been confirmed that the intravascular NIRSsystem safely obtained spectral data in patients that were similarto those from autopsy specimens.10 Currently, an observationalstudy of cholesterol in coronary arteries (COLOR registry,NCT00831116) is aimed enrolling at �1000 patients in 14centres in the USA. In Europe, this imaging modality is beingused in the IBIS 3 trial which is a study that will be able toassess the effects of rosuvastatin on the content of necrotic core(IVUS-VH) and lipid-containing regions (NIR spectroscopy) at 52weeks.
Characterization ofatherosclerosis
Atheroma: pathological insightsA detailed description of atherosclerosis development and compo-sition is beyond the scope of this review. Nevertheless, we high-light here some important concepts that will support the use oftissue characterization imaging modalities for plaque typification.
In brief, an atheroma is formed by an intricate sequence ofevents, not necessarily in a linear chronologic order, that involves
Figure 2 Intravascular ultrasound signal is obtained from the vessel wall (A). Greyscale intravascular ultrasound imaging is formed by theenvelope (amplitude) (B) of the radiofrequency signal (C). By greyscale, atherosclerotic plaque can be classified into four categories: soft, fibro-tic, calcified, and mixed plaques. (D) Shows a cross-sectional view of a greyscale image. The blue lines limit the actual atheroma. The frequencyand power of the signal commonly differ between tissues, regardless of similarities in the amplitude. From the backscatter radiofrequency datadifferent types of information can be retrieved: virtual histology (E), palpography (F), integrated backscattered (IB) intravascular ultrasound (G),and iMAP (H ). Virtual histology is able to detect four tissue types: necrotic core, fibrous, fibrofatty, and dense calcium. Plaque deformability atpalpography is reported in strain values, which are subsequently categorized into four grades according to the ROtterdam Classification (ROC).The tissues characterized by integrated backscattered (IB) intravascular ultrasound are lipidic, fibrous, and calcified; and iMAP detects fibrotic,lipidic, necrotic, and calcified.
H.M. Garcia-Garcia et al.2458D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

extracellular lipid accumulation, endothelial dysfunction, leucocyterecruitment, intracellular lipid accumulation (foam cells), smoothmuscle cell migration and proliferation, expansion of extracellularmatrix, neoangiogenesis, tissue necrosis, and mineralization atlater stages. The ultimate characteristic of an atheroscleroticplaque at any given time depends on the relative contribution ofeach of these features.11 Thus, in histological cross-sections, thepathologic intimal thickening is rich in proteoglycans and lipidpools, but no trace of necrotic core is seen. The earliest lesionwith a necrotic core is the fibroatheroma (FA), and this is the pre-cursor lesion that may give rise to symptomatic heart disease.Thin-capped fibroatheroma (TCFA) is a lesion characterized by alarge necrotic core containing numerous cholesterol clefts. Theoverlying fibrous cap is thin and rich in inflammatory cells, macro-phages, and T lymphocytes with a few smooth muscle cells.
Atheroma: linking pathology conceptsand intracoronary imagingFigure 6 outlines the virtual histology plaque and lesion types thatare proposed based on the previous paragraph which describespathologic data.12
On the basis of tissue echogenicity (i.e. their appearance), notnecessarily histological composition, atheromas have been classi-fied in four categories by greyscale IVUS: (i) soft plaque (lesionechogenicity less than the surrounding adventitia), (ii) fibrousplaque [intermediate echogenicity between soft (echolucent)atheromas and highly echogenic calcified plaques], (iii) calcifiedplaque (echogenicity higher than the adventitia with acoustic sha-dowing), and (iv) mixed plaques (no single acoustical subtype rep-resents .80% of the plaque)13 (Figure 1).
Description of the validation against pathology of the IVUS grey-scale and the IVUS-based imaging modalities for plaque character-ization is beyond the scope of this review. All available validationreports are to be found in the list of references.3 –5,14–23
Detection of calcificationThe presence, depth and circumferential distribution of calcifica-tion are important factors not only for selecting the type of inter-ventional device and estimating the risk of vessel dissection and
perforation during PCI,24 but also in designing and conductingstudies on progression/regression of coronary atheroma. Plaqueswith moderate to severe calcification showed no change or pro-gression of atheroma size.25 Thus, careful selection of coronarysegments to evaluate the effect of drugs on coronary atherosclero-sis should be considered.
On IVUS, calcium appears as bright echoes that obstruct thepenetration of ultrasound (acoustic shadowing) (Figure 1C). There-fore, IVUS detects only the leading edge of calcium and cannotdetermine its thickness. Using greyscale IVUS, a three-dimensionaland quantitative analysis of atherosclerotic plaque composition byautomated differential echogenicity has been developed to facili-tate automatic detection of calcified areas.16
Virtual histology, in comparison with histology, has a predictiveaccuracy of 96.7% for detection of dense calcium.26
Coronary remodellingCoronary remodelling refers to a continuous process involvingchanges in vessel size measured by the external elastic membrane(EEM) cross-sectional area (also called vessel cross-sectionalarea—CSA). ‘Positive remodelling’ occurs when there is anoutward increase in EEM. ‘Negative remodelling’ occurs whenthe EEM decreases in size (shrinkage of the vessel).13 The magni-tude and direction of remodelling can be expressed by the follow-ing index: EEM CSA at the plaque site divided by EEM CSA at thereference ‘non-diseased’ vessel. Positive remodelling will demon-strate an index .1.0, while negative remodelling has an index,1.0. Direct evidence of remodelling can only be demonstratedin serial studies showing changes in the EEM CSA over time,since remodelling may also be encountered at the ‘normal-appearing’ reference coronary segment.27
Pathological studies have also suggested a relationship betweenpositive vessel remodelling and plaque vulnerability. Vessel withpositive remodelling showed increased inflammatory marker con-centrations, larger lipid cores, paucity of smooth muscle cells,and medial thinning.28 –30 Several IVUS studies have linked positivevessel remodelling with culprit31 and ruptured coronaryplaques.32,33 Positive remodelling has been observed more oftenin patients with acute coronary syndromes than in those with
Figure 3 (A) Shows a greyscale image. (B) Depicts a VH image created using the Revolution 45-MHz IVUS catheter, which is currently underdevelopment by Volcano. This plaque is classified as a fibroatheroma as it has a visible fibrous cap covering a more than 10% confluent necroticcore. (C) Shows the corresponding histological section.
Imaging of coronary atherosclerosis 2459D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

stable coronary artery disease (CAD),34,35 and has been identifiedas an independent predictor of major adverse cardiac events inpatients with unstable angina.36 Plaques exhibiting positive remo-delling also had more often thrombus and signs of rupture.37
The pattern of remodelling has also been correlated with plaquecomposition; soft plaques are associated with positive remodellingwhile fibrocalcific plaques more often have negative or constrictiveremodelling.38 Similar findings have been observed in studies
Figure 4 Intravascular ultrasound systems. The console of the Boston Scientific is iLabw ultrasound imaging system (A) and the iCrossTM isthe coronary imaging catheter (B). The Console of the Volcano’s s5TM ultrasound imaging system and the Eagle EyeTM platinum coronaryimaging catheter are shown in (C and D). (E and F) The console of the Terumo Corporation Visiwave and the IVUS catheter ViewIT are shown.
H.M. Garcia-Garcia et al.2460D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

utilizing virtual histology; positive remodelling was directly corre-lated with the presence and the size of the necrotic core, andinversely associated with fibrotic tissue39 (Figure 7).
Vulnerable plaque and thrombiAcute coronary syndromes are often the first manifestation of cor-onary atherosclerosis, making the identification of plaques at highrisk of complication an important component of strategies toreduce casualties. Approximately 60% of clinically evident plaqueruptures originate within an inflamed TCFA.40,41
The definition of a VH-TCFA is a lesion fulfilling the followingcriteria in at least 3 frames: (i) plaque burden ≥ 40%; (ii) confluentnecrotic core ≥ 10% in direct contact with the lumen (i.e. novisible overlying tissue).42 Using this definition of VH-TCFA, inpatients with ACS who underwent IVUS of all three epicardial cor-onaries, on average, there were 2 VH-TCFA per patient with halfof them showing outward remodelling.42
Hong et al. reported the frequency and distribution of TCFAidentified by virtual histology intravascular ultrasound in acute cor-onary syndrome (ACS ¼ 105 patients) and stable angina pectoris(SAP ¼ 107 patients) in a 3-vessel IVUS-VH study.43 There were
Figure 5 Left anterior oblique view of the right coronary artery where the angiographic appearance of the Apollo catheter can be seen (A).The proximal near infrared spectroscopy (NIRS) optical core and distal ultrasound transducer (IVUS) are both clearly visible (B). A picture ofthe Apollo catheter tip indicating the relative positions to each other of the NIRS light source and IVUS probe (C). The combined intravascularultrasound images and chemical information from a pullback through the right coronary artery obtained using the Apollo catheter. The chemo-gram obtained from the Apollo catheter pullback, with the stented area as indicated (D). The chemogram is a map of the measured probabilityof the lipid core plaque (LCP) from each scanned arterial segment; the yellow regions represent those with the highest probability for thepresence of the LCP, while red regions represent those with the lowest. The chemogram displays the pullback position against the circumfer-ential position of the measurement in degrees. The § represents a region of the coronary artery where insufficient NIRS signals were obtainedto generate a chemogram. In this image the proximal end of the stent is located in an area with a high probability of the LCP (yellow). The blockchemogram provides a summary of the raw data from the chemogram and displays the probability that an LCP is present for all measurementsin a 2 mm block of coronary artery. The order of probability for the presence of the LCP from highest to lowest is yellow, light brown, brown,and red (E). The longitudinal IVUS pullback, with NIRS overlay (F). The lilac and blue lines mark the anatomical position on the IVUS, and thecorresponding position on the chemogram during pullback, enabling simultaneous assessment of plaque structure and composition. (G) Shows across-sectional intravascular ultrasound image with the chemogram obtained from (D), demonstrating well opposed clearly identifiable stentstruts (ss), highlighting the ability of the Apollo catheter to be used as a standalone IVUS catheter if required. The corresponding longitudinalIVUS image and chemogram is indicated by the lilac line on (D), (E), and (F). The chemogram indicates that there is a low probability of lipidpresent in the stented plaque. (H) A cross-sectional IVUS image distal to the stent demonstrates the presence of echolucent plaque between 1and 7 o’clock. The chemogram displays a high probability of lipid in this plaque. The corresponding longitudinal IVUS image, and chemogram areindicated by the blue lines on (D), (E), and (F).
Imaging of coronary atherosclerosis 2461D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

2.5+ 1.5 in ACS and 1.7+1.1 in SAP VH-TCFAs per patient, P ,
0.001. Presentation of ACS was the only independent predictorfor multiple VH-TCFA (P ¼ 0.011). Eighty-three per cent ofVH-TCFAs were located within 40 mm of the coronary.
The potential value of these VH IVUS-derived plaque types inthe prediction of adverse coronary events was evaluated in aninternational multicentre prospective study, the Providing RegionalObservations to Study Predictors of Events in the Coronary Treestudy (PROSPECT study), which has been completed but not yetpublished.
Although plaque characteristics (i.e. tissue characterization) donot yet influence current therapeutic guidelines, the availableclinical imaging modalities, IVUS and IVUS-based tissue character-ization techniques such as virtual histology, integrated basckscat-tered IVUS, and iMAP, have the ability to identify some of thepathological atheroma features described above and could helpus to advance further our understanding on atherosclerosisFigure 2.
Plaque ruptures occur at sites of significant plaque accumulation,but are often not highly stenotic by coronary angiography due topositive vascular remodelling.32,33,44 The transition to plaquerupture has been characterized by the presence of active
inflammation (monocyte/ macrophage infiltration), thinning of thefibrous cap (,65 mm), development of a large lipid necroticcore, endothelial denudation with superficial platelet aggregationand intraplaque haemorrhage.45
Ruptured plaques may have a variable appearance in IVUS; theAmerican College of Cardiology clinical expert consensus docu-ment recommended use of the following definitions: (i) Plaqueulceration: A recess in the plaque beginning at the luminal-intimalborder, typically without enlargement of the EEM compared withthe reference segment. (ii) Plaque rupture: plaque ulcerationwith a tear detected in a fibrous cap. Contrast injections may beused to prove and define the communication point.46
The tear of the rupture (identified in �60%) occurs more oftenat the shoulder of the plaque than in the centre.32,47,48 IVUS fea-tures of ruptured plaques are as follows: large in volume, eccentric,have mixed or soft composition and irregular surface, and areassociated with positive vessel remodelling.32,33,49,50 Rupturedplaques have less calcium, especially superficial calcium, but alarger number of small (,908 arc) calcium deposits, particularlydeep calcium deposits.51
Several IVUS studies have reported the frequency and distri-bution of ruptured plaques in the coronary arteries (Table 1).
Figure 6 Virtual histology plaque types. FF, fibrofatty; FT, fibrous tissue; NC, necrotic core and DC, dense calcium.
H.M. Garcia-Garcia et al.2462D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

Intravascular ultrasound has also been used to assess thenatural evolution of ruptured plaques. Up to 50% of the rupturedplaques detected in a first ACS event heal with medical therapy,without significant change in plaque size.52 Another studyrevealed complete healing of plaque rupture in 29% of thepatients treated with statins and incomplete healing in untreatedpatients.53
Thrombus represents the ultimate pathological feature leadingto ACS. Thrombus is usually recognized as an echolucent intra-luminal mass, often with a layered or pedunculated appearanceby IVUS.13 Fresh or acute thrombus may appear as an echodenseintraluminal tissue, which does not follow the circular appearanceof the vessel wall, while an older, more organized thrombus has adarker ultrasound appearance. However, none of these IVUS fea-tures are a hallmark for thrombus, and one should consider slowflow (fresh thrombus), air, stagnant contrast or black hole, anecholucent neointimal tissue observed after drug eluting stentand radiation therapy, as differential diagnoses.13 In addition,IVUS resolution is limited to precisely characterize thrombus. Ina study in patients with acute myocardial infarction (AMI), intra-coronary thrombus was observed in all cases by optical coher-ence tomography (OCT) and angioscopy but was identified inonly 33% by IVUS.54
Clinical applications: diagnostic
Determination of severity and extentof atherosclerosisDetermination of severity and extent of atherosclerosis remainsone of the main diagnostic clinical applications of intravascularimaging, as angiography and non-invasive methods lack spatial ortemporal resolution for accurate coronary disease assessment.
Assessment of atheroma burdenQuantification of atheroma or plaque area in cross-sectional IVUSimages is performed by subtracting the lumen area from the EEMarea. Hence, an IVUS-defined atheroma area is a combination ofplaque plus media area. The atheroma area can be calculated ineach frame (cross-sectional image), and total atheroma volume(TAV) can be calculated based on the pullback speed duringimaging acquisition. Atheroma volume can be reported as theper cent of the volume of the EEM occupied by atheroma,namely per cent atheroma volume (PAV). Parameters commonlyused to report the extent of the coronary atherosclerosis areshown in Figure 8.
Figure 7 Relationship between vessel wall remodelling and plaque composition. At the top, six consecutive greyscale frames are shown. (A)The size of the plaque is smaller when compared with the cross-section shown in (B). (B) The vessel wall is also clearly larger resulting in aremodelling index of 1.1. Thus, the vessel needs to grow to accommodate the plaque without affecting lumen size (Glagov phenomenon).The atheroma in (B) is also necrotic core rich. This suggests that positive remodelled plaques are commonly necrotic core rich. VCSA,vessel cross-sectional area.
Imaging of coronary atherosclerosis 2463D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 1 Frequency and distribution of ruptured plaque in ultrasound transducer studies
Author Year IVUS/Otherimaging modalities
Clinicalpresentation
n Frequency/distribution
Rioufol et al.75 2002 IVUS ACS 24 2 RP per patient and 12.5% of these patients had RP in the three major coronary arteries. Only37.5% of the RP were located on the culprit lesion, and 79% of the patients had also an RPsomewhere other than on the culprit lesion
Maehara et al.32 2002 IVUS SA/ACS 254 Multiple ruptures were observed in 39 of 254 patients (15%), 36 in the same artery
Hong et al.76 2004 IVUS SA/AMI 235 (122 AMI and 113 SA) RP of infarct-related or target lesions occurred in 66% of AMI patients and in 27% of SA patients.Non-infarct-related or non-target artery RP occurred in 17% of AMI patients and 5% of SApatients. Multiple RP were observed in 20% AMI and 6% of SA patients
Tanaka et al.77 2005 IVUS AMI 45 RP was observed in 47% of patients at the culprit site and 17 additional RP were found at remotesites in 24% of patients
Hong et al.78 2005 IVUS SA/ACS 392 (231 ACS and 161 SA) 3-vessel IVUS imaging showed that RP occurred mainly in proximal segments of the LAD (83%of LAD RP), the proximal and distal segments of the RCA (48 and 32% of RCA RP,respectively), and the entire LCX
Tyczynski et al.79 2005 IVUS SA/ACS 16 (2 AMI, 13 UA and 1 SA) RP in the left main coronary artery (LMCA) were located in the distal portion and/or bifurcationof the LMCA (i.e. opposite to the flow divider) often did not compromise the lumen, and hadan angiographic complex appearance
Pregowski et al.80 2005 IVUS SA/ACS 791 RP in saphenous vein grafts (SVGs) have a prevalence of 9.7%. These RP were found to beassociated with complex angiographic characteristics and positive remodelling
Pregowski et al.81 2006 IVUS SA 104 patients with RP in the LAD; the majority were located within the proximal 30 mm of the artery
Rodriguez-Granilloet al.82
2006 IVUS VH SA/ACS 40 RP located in the left anterior descending were clustered in the proximal part of the vessel,whereas ruptures located in the right coronary artery were more distally located
Hong et al.43 2008 IVUS VH SA/ACS 212 (105 ACS and 107 SA) There were 76 RP (55 in ACS and 21 in SAP). 12 patients with ACS and 1 with SAP hadmultiple RP
Hong et al.83 2010 IVUS AMI 310 (125 STEMI and 185NSTEMI patients)
Culprit lesion PR, lipid-pool-like images, and thrombus were observed more frequently inpatients with STEMI than in those with NSTEMI (46 vs. 29%, 39 vs. 25%, and 34 vs. 21%,respectively)
IVUS, intravascular ultrasound; RP, ruptured plaque; ACS, acute coronary syndrome; SA, stable angina; AMI, acute myocardial infarction. H.M
.Garcia-G
arciaet
al.2464
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/20/2456/613364 by guest on 24 N
ovember 2021

Research applicationsIntravascular imaging has played an important role in the under-standing of atherosclerosis disease in humans and translation ofnovel therapies to the clinical arena.
Cardiac allograft diseaseMost clinical adverse events in transplant patients occur after1 year. Cumulative incidence of cardiac events per patient yearwas 0.9% within the first year, increasing to 1.9% by 5 years.Cardiac events accounted for 3.8% of the deaths by the end ofthe first year, rising to 18% of total mortality by 7 years afterheart transplantation. After the first year of transplantation, 36%(20/55) of the patients died because of sequelae of CAD.55
Death is usually silent because heart is denervated. Therefore,there is a need for screening in order to detect coronary athero-sclerosis early. The presence of obstructive coronary disease inangiography is a predictor of any cardiac event [odds ratio (OR)3.44, P , 0.05], as well as a predictor of cardiac death (OR 4.6,P , 0.05). However, a pathological study reported 10 patientswho died or underwent retransplantation within 2 months of cor-onary angiography. One quarter of the patients had intermediatelesions or atheromatous plaques. Fresh or organizing thrombuswas most often associated with discrete lesions and accountedfor all complete occlusions. Authors concluded that transplantCAD has a heterogeneous histologic and angiographic appearance,with angiographic underestimation of disease in some patients.Accordingly, many active transplant centres incorporated IVUSimaging into their post-transplant surveillance, but there is no con-sensus on how frequent IVUS should be performed. The predictivevalue of IVUS has been explored in a study that included 143patients who underwent 3-vessel IVUS investigation at 1 and 12months after transplantation. The change in intimal thickness wascalculated (≥0.5 mm was defined as rapidly progressive vasculopa-thy). At 1 year, rapid progression was demonstrated in 37% of thepatients and in 47% of them a new lesion was found. At 5.9 years,
patients with rapid progression died more than their counterparts(26 vs. 11%, P ¼ 0.03). The combined endpoint of death and MIwas also more frequently seen in patients with rapid progression(51 vs. 16%, P , 0.0001).56
Intravascular ultrasound has been also used to assess noveltherapies in heart transplantation recipients. Eisen et al. random-ized 634 patients to receive 1.5 mg of everolimus per day (209patients), 3.0 mg of everolimus per day (211 patients), or 1.0–3.0 mg of azathioprine per kilogram of body weight per day (214patients), in combination with cyclosporine, corticosteroids, andstatins. The primary efficacy endpoint was a composite of death,graft loss or retransplantation, loss to follow-up, biopsy-provedacute rejection of grade 3A, or rejection with haemodynamic com-promise. At 1 year, IVUS showed that the average increase inmaximal intimal thickness was significantly smaller in the two ever-olimus groups than in the azathioprine group.57
Drug effects on atherosclerosisThe initial observations about a positive continuous relationshipbetween coronary heart disease risk and blood cholesterol levelsled to the conduction of a number of IVUS-based studies to evalu-ate the effect of different lipid lowering drugs on atheroma size.The efficacy of lowering low-density lipoprotein cholesterol(LDL-C) with inhibitors of hydroxymethylglutaryl-coenzyme Areductase (statins) is unequivocal; however, the change in ather-oma size by statins is not constant across all IVUS studies(Table 2). There are many potential explanations for these discre-pancies in IVUS studies such as drug properties, dose, and durationof treatment. In early studies like the GAIN study,58 atheromavolume was not reduced by atorvastatin despite the reduction inLDL-C (86 vs. 140 mg/dL) at 12 months. In contrast, the REVER-SAL study59 showed that LDL-C levels were further lowered byatorvastatin vs. pravastatin (110 vs. 79 mg/dL) which was associ-ated with an increase of 2.7% of the atheroma volume inpravastatin-treated patients and in a 0.4% reduction in the
Figure 8 Parameters commonly used to report the extent of the coronary atherosclerosis are the total atheroma volume (TAV) and the percent atheroma volume (PAV). EEM, external elastic membrane; CSA, cross-sectional area.
Imaging of coronary atherosclerosis 2465D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Table 2 Intravascular ultrasound progression/regression studies
Study Design Year Treatment n FU Primary endpoint Results (mean+++++SD)
Statin trials
GAIN58 RCT 2001 Atorvastatin 48 12 months Plaque volume 2.5+24.9 mm3
Control 51 11.8+31 mm3
ESTABLISH84 RCT 2004 Atorvastatin 24 6 months % Change in plaque volume 13.1+12.8%Control 24 8.7+14.9%
REVERSAL59 RCT 2004 Atorvastatin 253 18 months % Change in plaque volume 4.1+29.6%Pravastatin 249 5.4+20.1%
Jensen et al.85 Non-RCT 2004 Simvastatin 40 12 months % Change in plaque volume 6.30%
Petronio et al.86 RCT 2005 Simvastatin 36 12 months Plaque volume 22.5+3.0 mm3/mmControl 35 1.0+3.0 mm3/mm
Nishioka et al.87 Non-RCT 2004 Pravastatin, atorvastatin, simvastatin, andfluvastatin
22 6 months Plaque Volume 30.9+15.6 mm3
Control 26 35.5+12.7 mm3
Tani et al.88 RCT 2005 Pravastatin 52 6 months % Change in plaque volume 214.4+23%Control 23 1.1+4.6%
ASTEROID89 Non-RCT 2006 Rosuvastatin 349 24 months Change in PAV 20.98+3.15%
Takashima et al.90 Non-RCT 2007 Pitavastatin 41 6 months % Change in plaque volume 210.6+9.4%Control 41 8.1+14.0%
COSMOS91 Non-RCT 2009 Rosuvastatin 126 18 months Change in PAV 25.1+14.1%
JAPAN-ACS92 RCT 2009 Atorvastatin 127 8–12months
% Change in plaque volume 218.1+14.2%
Pitavastatin 125 216.9+13.9%
Hirayama Non-RCT 2009 Atorvastatin 28 28 weeks % Change in plaque volume 29.4+10.3%80 weeks 218.9+14.1%
ACAT (acyl-coenzyme A:cholesterol acyltransferase) inhibitor trials
A-PLUS93 RCT 2004 Avasimibe 50 mg 108 24 months Change in PAV 0.7+0.4%Avasimibe 250 mg 98 0.8+0.4%Avasimibe 750 mg 117 1.0+0.3%Placebo 109 0.4+0.4%
ACTIVATE64 RCT 2006 pactimibe 206 18 months Change in PAV 0.69+0.25%Placebo 202 20.59+0.25%
Increasing high-density lipoprotein therapies
ApoA-I Milano94 RCT 2003 ApoA-I Milano 15 mg/kg 21 5 weeks Change in PAV 21.29+3.5%ApoA-I Milano 45 mg/kg 15 20.73+2.8%
Placebo 11 0.14+3.09%
ERASE62 RCT 2007 CSL-111 (reconstituted HDL infusion) 89 4 weeks % change in plaque volume 23.41 (IQR, 26.55 to 2.25)Placebo 47 21.62 (IQR, 25.95 to 1.94)
CART-295 RCT 2008 Succinobucol (AGI-1067) 183 12 months Absolute change in plaque volume 23.4+14.5 mm3
Placebo 49 20.6+13.4 mm3
Other therapies
H.M
.Garcia-G
arciaet
al.2466
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/20/2456/613364 by guest on 24 N
ovember 2021
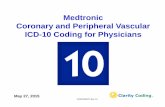
CAMELOT65 RCT 2004 Amlodipine 91 24 months Change in PAV 0.5+3.9%Enalapril 88 0.8+3.7%Placebo 95 1.3+4.4%
Waseda Non-RCT 2006 Losartan 41 7 months Change in plaque area 29.9+3.1 mm2
Non-ARB 23 7 months 29.1+2.7 mm2
ILLUSTRATE63 RCT 2007 Torcetrapib + atorvastatin 464 24 months Change in PAV 0.12+2.99%Atorvastatin 446 0.19+2.83%
PERSPECTIVE66 RCT 2007 Perindopril 75 36 months Change in plaque area 20.2+1.6 mm2
Placebo 69 20.1+1.2 mm2
PERISCOPE68 RCT 2008 Pioglitazone 179 18 months Change in PAV 20.16% (95% CI 20.57 to 0.25%)Glimepiride 181 0.73% (95% CI 0.33–1.12%)
STRADIVARIUS96 RCT 2008 Rimonabant 335 18 months Change in PAV 0.25% (95% CI 20.04 to 0.54%)Placebo 341 0.51% (95% CI 0.22–0.80%)
ENCORE II97 RCT 2009 Nifedipine 97 18–24months
% change in plaque volume 5.0 (95% CI 21.3, 11.2)
Placebo 96 3.2 (95% CI 21.9, 8.3)
APPROACH67 RCT 2010 rosiglitazone 233 18 months Change in PAV 20.21 (95% CI 20.86, 0.44)Glipizide 229 0.43 (95% CI 20.22, 1.08)
IVUS-based tissue characterization studies
Yokoyama et al.98 RCT 2005 Atorvastatin 25 6 months Overall plaque size and tissuecharacterization by IB IVUS
Atorvastatin reduced plaque size and changedplaque composition
Control 25
Kawasaki et al.99 RCT 2005 Pravastatin 17 6 months Overall tissue characterization by IB IVUS Statins reduced lipid without changes in plaque sizeAtorvastatin 18Diet 17
IBIS 271 RCT 2008 Darapladib 175 12 months Necrotic core volume by IVUS VH Darapladid reduced significantly necrotic corePlacebo 155
Nasu et al.69 Non-RCT 2009 Fluvastatin 40 12 months Overall tissue characterization by IVUS VH Fluvastatin reduced plaque volume and fibrofattyControl 40
Hong et al.70 RCT 2009 Simvastatin 50 12 months Overall tissue characterization by IVUS VH Both reduced necrotic core and increased infibrofatty volume
Rosuvastatin 50
Toi et al.100 RCT 2009 Atorvastatin 80 2–3 weeks Overall tissue characterization by IVUS VH Pitavastatin reduced plaque volume and fibrofattyPivastatin 80
Miyagi et al.101 Non-RCT 2009 Statin (pravastatin, pitavastatin,atorvastatin, fluvastatin, simvastatin)
44 6 months Overall tissue characterization by IB IVUS Statins reduced lipid and increased fibrous
Non-statin 56
IVUS, intravascular ultrasound; IB, integrated backscatter; VH, virtual histology; FU, follow-up; SD, standard deviation; CI, confidence interval; RCT, randomized controlled trial; IB, integrated backscattered.
Imaging
ofcoronary
atherosclerosis2467
Dow
nloaded from https://academ
ic.oup.com/eurheartj/article/31/20/2456/613364 by guest on 24 N
ovember 2021

atheroma volume in atorvastatin-treated patients. The clinical sig-nificance and the accuracy of IVUS for such measurements arestill debatable, but these results were statistically significant. ThePROVE-IT study,60 showed that the lower the LDL-C andC-reactive protein values, the greater the reduction in clinicalevents and atheroma progression.
The first study showing regression of plaque size was theASTEROID trial.61 At 24 months treatment with rosuvastatin40 mg daily resulted in lowering of LDL-C to 60.8 mg/dL andelevation of high-density lipoprotein cholesterol (HDL-C) by14.7%. These lipid effects were associated with statistically signifi-cant, albeit small reductions in PAV (0.79%) and the TAV (6.8%).
Intravascular ultrasound studies have also demonstrated coronaryplaque modification in HDL-treated patients. The infusion of syn-thetic HDL-C particles containing the variant apolipoprotein,apoA-I Milano, complexed with phospholipids (ETC-216) reducedthe PAV by 21.06% (3.17% P ¼ 0.02 compared with the baseline)in the combined ETC-216 group at 5 weeks. On the contrary, inthe placebo group, the PAV increased by 0.14% (3.09%; P ¼ 0.97compared with the baseline). In the ERASE study,62 60 patientswere randomly assigned to receive 4 weekly infusions of placebo(saline), 111 to receive 40 mg/kg of reconstituted HDL (CSL-111),and 12 to receive 80 mg/kg of CSL-111. The latter was discontinueddue to liver function test abnormalities. Within the treated group,the percentage change in the atheroma volume was 23.4% withCSL-111 (P , 0.001 vs. baseline), while for the placebo group itwas 21.6% (P ¼ 0.48 between groups). It is still unclear what thefuture holds for these therapeutical agents.
Patients with human deficiency of cholesterylester transferprotein (CETP) have elevated circulating levels of HDL-C. Thishas led to investigation on CETP inhibition as a novel and poten-tially effective approach to elevate HDL-C. In the ILLUSTRATEtrial, the PAV (the primary efficacy measure) increase was similarlylow in patients receiving atorvastatin monotherapy vs. in thosereceiving the combined torcetrapib–atorvastatin therapy after 24months (0.19 vs. 0.12%, respectively).63
The enzyme acyl-coenzyme A:cholesterol acyltransferase(ACAT) esterifies cholesterol in a variety of cells and tissues. Inhi-bition of ACAT1, by blocking the esterification of cholesterol,could prevent the transformation of macrophages into foam cellsand slow the progression of atherosclerosis, while inhibition ofACAT2 would be expected to decrease serum lipid levels. In theACTIVATE study, the change in the PAV was similar in the pacti-mibe (100 mg daily) and placebo groups (0.69 and 0.59%, respect-ively; P ¼ 0.77).64
Systolic blood pressure has been shown to be an independentpredictor of plaque progression by IVUS.65 A randomized studyof patients with CAD and a diastolic blood pressure,100 mmHg treated with placebo or antihypertensive therapyusing either amlodipine 10 mg daily or enalapril 20 mg dailyshowed that patients treated with amlodipine had a reduction inplaque size and also a reduction in cardiovascular events whencompared with placebo at 24 months.65 The PERSPECTIVEstudy,66 a substudy of the EUROPA trial, evaluated the effect ofperindopril on coronary plaque progression in 244 patients.There were no differences in changes in IVUS plaque measure-ments detected between the perindopril and placebo groups.
Thiazolidinediones increase insulin sensitivity in peripheraltissues, thereby lowering glucose, and also lower blood pressureand inflammatory markers, and improve lipid profile, endothelialfunction, and carotid IMT. Thiazolidinediones (i.e. rosiglitazoneand pioglitazone) may therefore reduce progression of coronaryatherosclerosis compared with other antidiabetic drugs. Twostudies have addressed this question. The APPROACH (Rosiglita-zone study)67 and the PERISCOPE (Pioglitazone study) trials.68 Achange in PAV in the APPROACH study was not different inpatients allocated to glipizide or rosiglitazone [20.64%, 95% con-fidence interval (CI) 21.46, 0.17; P ¼ 0.12], while in the PERI-SCOPE study pioglitazone vs. glimepiride was associated withfavourable effects on the change of PAV (–0.16+0.21 vs.0.73+ 0.20%, P ¼ 0.002). Rosiglitazone significantly reduced thenormalized TAV by 5.1 mm3 (95% CI 210.0, 20.3; P ¼ 0.04)when compared with glipizide, whereas pioglitazone just failed toachieve a statistically significant change in the TAV (–5.5+1.6vs. –1.5+1.5 mm3, P ¼ 0.06) when compared with glimepiride.Pioglitazone resulted in comparable plaque size reduction (i.e.TAV) as rosiglitazone, but this reduction was associated with analmost double reduction in vessel size. The formula of change inthe PAV has as a numerator change in atheroma volume and asdenominator change in vessel volume; this may mask the specificdirectional changes in its numerator and denominator when usedas primary endpoint to compare two pharmacological agents.
There are several recent reports showing serial changes ofplaque composition in patients treated with various statin treat-ments. In one of them, patients with stable angina pectoris (n ¼80) treated with fluvastatin for 1 year had significant regressionof the plaque volume, and changes in the atherosclerotic plaquecomposition with a significant reduction of the fibrofatty volume(P , 0.0001). This change in the fibrofatty volume had a significantcorrelation with change in the LDL-cholesterol level (r ¼ 0.703,P , 0.0001) and change in the hsCRP level (r ¼ 0.357, P ¼0.006).69 Of note, the necrotic core did not change significantly.In a second study, Hong et al. randomized 100 patients withstable angina and ACS to either rosuvastatin 10 mg or simvastatin20 mg for 1 year. The overall necrotic core volume significantlydecreased (P ¼ 0.010) and the fibrofatty plaque volume increased(P ¼ 0.006) after statin treatments. Particularly, there was a signifi-cant decrease in the necrotic core volume (P ¼ 0.015) in therosuvastatin-treated subgroup. By multiple stepwise logisticregression analysis, they showed that the only independentclinical predictor of decrease in the necrotic core volume wasthe baseline HDL-cholesterol level (P ¼ 0.040, OR: 1.044, 95%CI 1.002–1.089).70
The IBIS 2 study compared the effects of 12 months of treat-ment with darapladib (oral Lp-PLA2 inhibitor, 160 mg daily) orplacebo in 330 patients.71 This study failed to demonstrate thetreatment effect of darapladib on the two co-primary endpoints(i.e. density of high strain values by palpography and change inhsCRP). Other endpoints included changes in the necrotic coresize (IVUS-VH) and atheroma size (IVUS-greyscale). Backgroundtherapy was comparable between groups, with no difference inthe LDL-cholesterol at 12 months. In the placebo-treated group,however, the necrotic core volume increased significantly,whereas darapladib halted this increase, resulting in a significant
H.M. Garcia-Garcia et al.2468D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

treatment difference of 25.2 mm3 (P ¼ 0.012). These intraplaquecompositional changes occurred without a significant treatmentdifference in the TAV.
Nevertheless, there is no a single report describing a clear directassociation between reduction in the plaque size and/or the plaquecomposition with reduction in clinical events. This is in part due tothe fact that clinical outcome studies are expensive since they haveto include a large population (that should be imaged at least at twodifferent time points) that has to be followed up for a long periodof time to collect the number of events (which are becomingscarce due to improvement in the standard of care) needed toassess the treatment effect.
Future directionsIn the future, integration of multiple image technologies in a singlecatheter is likely to provide a more comprehensive assessment ofthe coronary vasculature.
IVUS-VH has a limited axial resolution (100–200 mm) notallowing a precise measurement of the fibrous thin cap; on thecontrary OCT is a high-resolution imaging technique (10–20 mm) that can be used in the assessment of microstructure,but only using OCT in plaque-type characterization can be asource of misclassification. The OCT signal has in fact a low pen-etration, limited to 1–2 mm, and could not detect lipid pools orcalcium behind thick fibrous caps, thus producing inaccuratedetection of signal-poor areas.72 The combined use of IVUS-VHanalysis and OCT seems to improve the accuracy for TCFAdetection.73,74
Intravascular ultrasound guidance during the treatment ofchronic total occlusions, in which the most exacting parts of theprocedure are to enter into the proximal part of the occlusionand to keep the guidewire within the limits of the vessel toavoid coronary perforations, with a forward-looking intravascularultrasound (FL-IVUS) holds promise because it is able to visualizethe vessel, plaque morphology, and true and false lumens in frontof the imaging catheter. The Preview catheter is currently under-going preclinical and early clinical evaluation. It is a single-use,over-the-wire imaging catheter, and the distal imaging tip isshown in Figure 9.
Conflict of interest: M.A.C. is a consulting speaker (,10 000USD threshold) and received research grants (through theUniversity and/or core lab) from Boston Scientific and Lightlab,and is a consulting speaker for the drug companies: Sanofi andEli Lilly (,10 000 USD per year).
References1. Roberts WC, Jones AA. Quantitation of coronary arterial narrowing at necropsy
in sudden coronary death: analysis of 31 patients and comparison with 25control subjects. Am J Cardiol 1979;44:39–45.
2. Escaned J, Baptista J, Di Mario C, Haase J, Ozaki Y, Linker DT, de Feyter PJ,Roelandt JR, Serruys PW. Significance of automated stenosis detection duringquantitative angiography. Insights gained from intracoronary ultrasoundimaging. Circulation 1996;94:966–972.
3. Sathyanarayana S, Carlier S, Li W, Thomas L. Characterisation of atheroscleroticplaque by spectral similarity of radiofrequency intravascular ultrasound signals.EuroIntervention 2009;5:133–139.
4. Kawasaki M, Bouma BE, Bressner J, Houser SL, Nadkarni SK, MacNeill BD,Jang IK, Fujiwara H, Tearney GJ. Diagnostic accuracy of optical coherence tom-ography and integrated backscatter intravascular ultrasound images for tissuecharacterization of human coronary plaques. J Am Coll Cardiol 2006;48:81–88.
Figure 9 Forward-looking intravascular ultrasound (Volcano Corporation) is a 45 MHz transducer oriented at a 458 angle at the tip of thecatheter, which rotates providing a forward-looking cone of visualization (A). A 0.014-inch chronic total occlusion dedicated guidewire can beadvanced through the catheter. Thus, a true lumen position can be maintained under forward-looking intravascular ultrasound guidance whiletreating chronic total occlusion via antegrade. An forward-looking intravascular ultrasound view of the proximal end of the chronic total occlu-sion phantom model (B), and directed in real time to maintain a true lumen position.
Imaging of coronary atherosclerosis 2469D
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

5. Schaar JA, De Korte CL, Mastik F, Strijder C, Pasterkamp G, Boersma E,Serruys PW, Van Der Steen AF. Characterizing vulnerable plaque featureswith intravascular elastography. Circulation 2003;108:2636–2641.
6. Lockwood GR, Ryan LK, Hunt JW, Foster FS. Measurement of the ultrasonicproperties of vascular tissues and blood from 35–65 MHz. Ultrasound MedBiol 1991;17:653–666.
7. Bridal SL, Fornes P, Bruneval P, Berger G. Parametric (integrated backscatterattenuation) images constructed using backscattered radio frequency signals(25–56 MHz) from human aortae in vitro. Ultrasound Med Biol 1997;23:215–229.
8. Gardner CM, Tan H, Hull EL, Lisauskas JB, Sum ST, Meese TM, Jiang C,Madden SP, Caplan JD, Burke AP, Virmani R, Goldstein J, Muller JE. Detectionof lipid core coronary plaques in autopsy specimens with a novel catheterbased near-infrared spectroscopy system. Am Coll Cardiol Img 2008;1:638–648.
9. Gardner CM, Tan H, Hull EL, Lisauskas JB, Sum ST, Meese TM, Jiang C,Madden SP, Caplan JD, Burke AP, Virmani R, Goldstein J, Muller JE. Detectionof lipid core coronary plaques in autopsy specimens with a novel catheter-basednear-infrared spectroscopy system. JACC Cardiovasc Imaging 2008;1:638–648.
10. Waxman S, Dixon SR, L’Allier P, Moses JW, Petersen JL, Cutlip D, Tardif JC,Nesto RW, Muller JE, Hendricks MJ, Sum ST, Gardner CM, Goldstein JA,Stone GW, Krucoff MW. In vivo validation of a catheter-based near-infraredspectroscopy system for detection of lipid core coronary plaques: initialresults of the SPECTACL study. JACC Cardiovasc Imaging 2009;2:858–868.
11. Virmani R, Kolodgie FD, Burke AP, Farb A, Schwartz SM. Lessons from suddencoronary death: a comprehensive morphological classification scheme for ather-osclerotic lesions. Arterioscler Thromb Vasc Biol 2000;20:1262–1275.
12. Garcı́a-Garcı́a HMMG, Lerman A, Vince DG, Margolis MP, van Es GA,Morel MA, Nair A, Virmani R, Burke AP, Stone GW, Serruys PW. Tissue charac-terisation using intravascular radiofrequency data analysis: recommendations foracquisition, analysis, interpretation and reporting. Eurointervention 2009;5:177.
13. Mintz GS, Nissen SE, Anderson WD, Bailey SR, Erbel R, Fitzgerald PJ, Pinto FJ,Rosenfield K, Siegel RJ, Tuzcu EM, Yock PG. American College of CardiologyClinical Expert Consensus Document on Standards for Acquisition, Measure-ment and Reporting of Intravascular Ultrasound Studies (IVUS). A report ofthe American College of Cardiology Task Force on Clinical Expert ConsensusDocuments. J Am Coll Cardiol 2001;37:1478–1492.
14. Di Mario C, The SH, Madretsma S, van Suylen RJ, Wilson RA, Bom N,Serruys PW, Gussenhoven EJ, Roelandt JR. Detection and characterization ofvascular lesions by intravascular ultrasound: an in vitro study correlated with his-tology. J Am Soc Echocardiogr 1992;5:135–146.
15. Prati F, Arbustini E, Labellarte A, Dal Bello B, Sommariva L, Mallus MT, Pagano A,Boccanelli A. Correlation between high frequency intravascular ultrasound andhistomorphology in human coronary arteries. Heart 2001;85:567–570.
16. Bruining N, Verheye S, Knaapen M, Somers P, Roelandt JR, Regar E, Heller I, deWinter S, Ligthart J, Van Langenhove G, de Feijter PJ, Serruys PW, Hamers R.Three-dimensional and quantitative analysis of atherosclerotic plaque compo-sition by automated differential echogenicity. Catheter Cardiovasc Interv 2007;70:968–978.
17. Nair A, Kuban BD, Tuzcu EM, Schoenhagen P, Nissen SE, Vince DG. Coronaryplaque classification with intravascular ultrasound radiofrequency data analysis.Circulation 2002;106:2200–2206.
18. Nair A, Margolis MP, Kuban BD, Vince DG. Automated coronary plaque charac-terisation with intravascular ultrasound backscatter: ex vivo validation. EuroInter-vention 2007;3:113–120.
19. Nasu K, Tsuchikane E, Katoh O, Vince DG, Virmani R, Surmely J-Fi, Murata A,Takeda Y, Ito T, Ehara M, Matsubara T, Terashima M, Suzuki T. Accuracy of invivo coronary plaque morphology assessment: a validation study of in vivovirtual histology compared with in vitro histopathology. J Am Coll Cardiol 2006;47:2405–2412.
20. Nasu K, Tsuchikane E, Katoh O, Vince DG, Margolis PM, Virmani R, Surmely JF,Ehara M, Kinoshita Y, Fujita H, Kimura M, Asakura K, Asakura Y, Matsubara T,Terashima M, Suzuki T. Impact of intramural thrombus in coronary arteries onthe accuracy of tissue characterization by in vivo intravascular ultrasound radio-frequency data analysis. Am J Cardiol 2008;101:1079–1083.
21. Granada JF, Wallace-Bradley D, Win HK, Alviar CL, Builes A, Lev EI, Barrios R,Schulz DG, Raizner AE, Kaluza GL. In vivo plaque characterization using intravas-cular ultrasound-virtual histology in a porcine model of complex coronarylesions. Arterioscler Thromb Vasc Biol 2007;27:387–393.
22. Van Herck J, De Meyer G, Ennekens G, Van Herck P, Herman A, Vrints C. Vali-dation of in vivo plaque characterisation by virtual histology in a rabbit model ofatherosclerosis. EuroIntervention 2009;5:149–156.
23. Thim T, Hagensen MK, Wallace-Bradley D, Granada JF, Kaluza GL, Drouet L,Paaske WP, Botker HE, Falk E. Unreliable assessment of necrotic core byVHTM IVUS in porcine coronary artery disease. Circ Cardiovasc Imaging 2010;3:384–391.
24. Silber S, Albertsson P, Aviles FF, Camici PG, Colombo A, Hamm C, Jorgensen E,Marco J, Nordrehaug JE, Ruzyllo W, Urban P, Stone GW, Wijns W. Guidelinesfor percutaneous coronary interventions. The task force for percutaneous cor-onary interventions of the European society of cardiology. Eur Heart J 2005;26:804–847.
25. Bruining N, de Winter S, Roelandt JR, Rodriguez-Granillo GA, Heller I, vanDomburg RT, Hamers R, de Feijter PJ. Coronary calcium significantly affectsquantitative analysis of coronary ultrasound: importance for atherosclerosisprogression/regression studies. Coron Artery Dis 2009;20:409–414.
26. Nair AMP, Kuban BD, Vince DG. Automated coronary plaque characterizationwith intravascular ultrasound backscatter: ex vivo validation. Eurointervention2007;3:113–130.
27. Nissen SE, Gurley JC, Grines CL, Booth DC, McClure R, Berk M, Fischer C,DeMaria AN. Intravascular ultrasound assessment of lumen size and wall mor-phology in normal subjects and patients with coronary artery disease. Circulation1991;84:1087–1099.
28. Pasterkamp G, Schoneveld AH, van der Wal AC, Haudenschild CC, Clarijs RJ,Becker AE, Hillen B, Borst C. Relation of arterial geometry to luminal narrowingand histologic markers for plaque vulnerability: the remodeling paradox. J AmColl Cardiol 1998;32:655–662.
29. Varnava AM, Mills PG, Davies MJ. Relationship between coronary artery remo-deling and plaque vulnerability. Circulation 2002;105:939–943.
30. Burke AP, Kolodgie FD, Farb A, Weber D, Virmani R. Morphological predictorsof arterial remodeling in coronary atherosclerosis. Circulation 2002;105:297–303.
31. Kotani J, Mintz GS, Castagna MT, Pinnow E, Berzingi CO, Bui AB, Pichard AD,Satler LF, Suddath WO, Waksman R, Laird JR Jr, Kent KM, Weissman NJ. Intra-vascular ultrasound analysis of infarct-related and non-infarct-related arteries inpatients who presented with an acute myocardial infarction. Circulation 2003;107:2889–2893.
32. Maehara A, Mintz GS, Bui AB, Walter OR, Castagna MT, Canos D, Pichard AD,Satler LF, Waksman R, Suddath WO, Laird JR Jr, Kent KM, Weissman NJ. Mor-phologic and angiographic features of coronary plaque rupture detected byintravascular ultrasound. J Am Coll Cardiol 2002;40:904–910.
33. von Birgelen C, Klinkhart W, Mintz GS, Papatheodorou A, Herrmann J,Baumgart D, Haude M, Wieneke H, Ge J, Erbel R. Plaque distribution and vas-cular remodeling of ruptured and nonruptured coronary plaques in the samevessel: an intravascular ultrasound study in vivo. J Am Coll Cardiol 2001;37:1864–1870.
34. Jeremias A, Spies C, Herity NA, Pomerantsev E, Yock PG, Fitzgerald PJ,Yeung AC. Coronary artery compliance and adaptive vessel remodelling inpatients with stable and unstable coronary artery disease. Heart 2000;84:314–319.
35. Nakamura M, Nishikawa H, Mukai S, Setsuda M, Nakajima K, Tamada H,Suzuki H, Ohnishi T, Kakuta Y, Nakano T, Yeung AC. Impact of coronaryartery remodeling on clinical presentation of coronary artery disease: an intra-vascular ultrasound study. J Am Coll Cardiol 2001;37:63–69.
36. Gyongyosi M, Yang P, Hassan A, Domanovits H, Laggner A, Weidinger F,Glogar D. Intravascular ultrasound predictors of major adverse cardiac eventsin patients with unstable angina. Clin Cardiol 2000;23:507–515.
37. Gyongyosi M, Yang P, Hassan A, Weidinger F, Domanovits H, Laggner A,Glogar D. Arterial remodelling of native human coronary arteries in patientswith unstable angina pectoris: a prospective intravascular ultrasound study.Heart 1999;82:68–74.
38. Tauth J, Pinnow E, Sullebarger JT, Basta L, Gursoy S, Lindsay J Jr, Matar F. Pre-dictors of coronary arterial remodeling patterns in patients with myocardialischemia. Am J Cardiol 1997;80:1352–1355.
39. Rodriguez-Granillo GA, Serruys PW, Garcia-Garcia HM, Aoki J, Valgimigli M, vanMieghem CA, McFadden E, de Jaegere PP, de Feyter P. Coronary artery remo-delling is related to plaque composition. Heart 2006;92:388–391.
40. Virmani R, Burke AP, Farb A, Kolodgie FD. Pathology of the vulnerable plaque.J Am Coll Cardiol 2006;47(Suppl. 8):C13–C18.
41. Schaar JA, Muller JE, Falk E, Virmani R, Fuster V, Serruys PW, Colombo A,Stefanadis C, Ward Casscells S, Moreno PR, Maseri A, van der Steen AF. Termi-nology for high-risk and vulnerable coronary artery plaques. Report of a meetingon the vulnerable plaque, June 17 and 18, 2003, Santorini, Greece. Eur Heart J2004;25:1077–1082.
42. Garcia-Garcia HM, Goedhart D, Schuurbiers JC, Kukreja N, Tanimoto S,Daemen J, Morel MA, Bressers M, van Es GA, Wentzel J, Gijsen F, van derSteen AF, Serruys PW. Virtual histology and remodeling index allow in vivoidentification of allegedly high risk coronary plaques in patients with acute cor-onary syndromes: a three vessel intravascular ultrasound radiofrequency dataanalysis. Eurointervention 2006;2:338–344.
43. Hong MK, Mintz GS, Lee CW, Lee JW, Park JH, Park DW, Lee SW, Kim YH,Cheong SS, Kim JJ, Park SW, Park SJ. A three-vessel virtual histology intravascular
H.M. Garcia-Garcia et al.2469aD
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

ultrasound analysis of frequency and distribution of thin-cap fibroatheromas inpatients with acute coronary syndrome or stable angina pectoris. Am J Cardiol2008;101:568–572.
44. Fujii K, Mintz GS, Carlier SG, Costa JR Jr, Kimura M, Sano K, Tanaka K, Costa RA,Lui J, Stone GW, Moses JW, Leon MB. Intravascular ultrasound profile analysis ofruptured coronary plaques. Am J Cardiol 2006;98:429–435.
45. Kolodgie FD, Gold HK, Burke AP, Fowler DR, Kruth HS, Weber DK, Farb A,Guerrero LJ, Hayase M, Kutys R, Narula J, Finn AV, Virmani R. Intraplaquehemorrhage and progression of coronary atheroma. N Engl J Med 2003;349:2316–2325.
46. Mintz GS, Nissen SE, Anderson WD, Bailey SR, Erbel R, Fitzgerald PJ, Pinto FJ,Rosenfield K, Siegel RJ, Tuzcu EM, Yock PG, O’Rourke RA, Abrams J,Bates ER, Brodie BR, Douglas PS, Gregoratos G, Hlatky MA, Hochman JS,Kaul S, Tracy CM, Waters DD, Winters WL. American College of CardiologyClinical Expert Consensus Document on Standards For Acquisition, Measure-ment and Reporting of Intravascular Ultrasound Studies (IVUS): a report ofthe American College of Cardiology Task Force on Clinical Expert ConsensusDocuments developed in collaboration with the European Society of Cardiologyendorsed by the society of cardiac angiography and interventions. J Am CollCardiol 2001;37:1478–1492.
47. Jensen LO, Mintz GS, Carlier SG, Fujii K, Moussa I, Dangas G, Mehran R,Stone GW, Leon MB, Moses JW. Intravascular ultrasound assessment offibrous cap remnants after coronary plaque rupture. Am Heart J 2006;152:327–332.
48. Ge J, Chirillo F, Schwedtmann J, Gorge G, Haude M, Baumgart D, Shah V, vonBirgelen C, Sack S, Boudoulas H, Erbel R. Screening of ruptured plaques inpatients with coronary artery disease by intravascular ultrasound. Heart 1999;81:621–627.
49. von Birgelen C, Klinkhart W, Mintz GS, Wieneke H, Baumgart D, Haude M,Bartel T, Sack S, Ge J, Erbel R. Size of emptied plaque cavity following spon-taneous rupture is related to coronary dimensions not to the degree oflumen narrowing. A study with intravascular ultrasound in vivo. Heart 2000;84:483–488.
50. Fujii K, Kobayashi Y, Mintz GS, Takebayashi H, Dangas G, Moussa I, Mehran R,Lansky AJ, Kreps E, Collins M, Colombo A, Stone GW, Leon MB, Moses JW.Intravascular ultrasound assessment of ulcerated ruptured plaques: a compari-son of culprit and nonculprit lesions of patients with acute coronary syndromesand lesions in patients without acute coronary syndromes. Circulation 2003;108:2473–2478.
51. Fujii K, Carlier SG, Mintz GS, Takebayashi H, Yasuda T, Costa RA, Moussa I,Dangas G, Mehran R, Lansky AJ, Kreps EM, Collins M, Stone GW, Moses JW,Leon MB. Intravascular ultrasound study of patterns of calcium in ruptured cor-onary plaques. Am J Cardiol 2005;96:352–357.
52. Rioufol G, Gilard M, Finet G, Ginon I, Boschat J, Andre-Fouet X. Evolution ofspontaneous atherosclerotic plaque rupture with medical therapy: long-termfollow-up with intravascular ultrasound. Circulation 2004;110:2875–2880.
53. Hong MK, Mintz GS, Lee CW, Suh IW, Hwang ES, Jeong YH, Park DW, Kim YH,Han KH, Cheong SS, Kim JJ, Park SW, Park SJ. Serial intravascular ultrasound evi-dence of both plaque stabilization and lesion progression in patients with rup-tured coronary plaques: effects of statin therapy on ruptured coronaryplaque. Atherosclerosis 2007;191:107–114.
54. Kubo T, Imanishi T, Takarada S, Kuroi A, Ueno S, Yamano T, Tanimoto T,Matsuo Y, Masho T, Kitabata H, Tsuda K, Tomobuchi Y, Akasaka T. Assessmentof culprit lesion morphology in acute myocardial infarction: ability of opticalcoherence tomography compared with intravascular ultrasound and coronaryangioscopy. J Am Coll Cardiol 2007;50:933–939.
55. Uretsky BF, Kormos RL, Zerbe TR, Lee A, Tokarczyk TR, Murali S, Reddy PS,Denys BG, Griffith BP, Hardesty RL et al. Cardiac events after heart transplan-tation: incidence and predictive value of coronary arteriography. J Heart LungTransplant 1992;11:S45–S51.
56. Tuzcu EM, Kapadia SR, Sachar R, Ziada KM, Crowe TD, Feng J, Magyar WA,Hobbs RE, Starling RC, Young JB, McCarthy P, Nissen SE. Intravascular ultra-sound evidence of angiographically silent progression in coronary atherosclero-sis predicts long-term morbidity and mortality after cardiac transplantation. J AmColl Cardiol 2005;45:1538–1542.
57. Eisen HJ, Tuzcu EM, Dorent R, Kobashigawa J, Mancini D, Valantine-vonKaeppler HA, Starling RC, Sorensen K, Hummel M, Lind JM,Abeywickrama KH, Bernhardt P. Everolimus for the prevention of allograft rejec-tion and vasculopathy in cardiac-transplant recipients. N Engl J Med 2003;349:847–858.
58. Schartl M, Bocksch W, Koschyk DH, Voelker W, Karsch KR, Kreuzer J,Hausmann D, Beckmann S, Gross M. Use of intravascular ultrasound tocompare effects of different strategies of lipid-lowering therapy on plaquevolume and composition in patients with coronary artery disease. Circulation2001;104:387–392.
59. Nissen SE, Tuzcu EM, Schoenhagen P, Brown BG, Ganz P, Vogel RA, Crowe T,Howard G, Cooper CJ, Brodie B, Grines CL, DeMaria AN. Effect of intensivecompared with moderate lipid-lowering therapy on progression of coronaryatherosclerosis: a randomized controlled trial. J Am Med Assoc 2004;291:1071–1080.
60. Cannon CP, Braunwald E, McCabe CH, Rader DJ, Rouleau JL, Belder R, Joyal SV,Hill KA, Pfeffer MA, Skene AM. Intensive versus moderate lipid lowering withstatins after acute coronary syndromes. N Engl J Med 2004;350:1495–1504.
61. Nissen SE, Nicholls SJ, Sipahi I, Libby P, Raichlen JS, Ballantyne CM, Davignon J,Erbel R, Fruchart JC, Tardif JC, Schoenhagen P, Crowe T, Cain V, Wolski K,Goormastic M, Tuzcu EM. Effect of very high-intensity statin therapy onregression of coronary atherosclerosis: the ASTEROID trial. J Am Med Assoc2006;295:1556–1565.
62. Tardif JC, Gregoire J, L’Allier PL, Ibrahim R, Lesperance J, Heinonen TM, Kouz S,Berry C, Basser R, Lavoie MA, Guertin MC, Rodes-Cabau J. Effects of reconsti-tuted high-density lipoprotein infusions on coronary atherosclerosis: a random-ized controlled trial. J Am Med Assoc 2007;297:1675–1682.
63. Nissen SE, Tardif JC, Nicholls SJ, Revkin JH, Shear CL, Duggan WT, Ruzyllo W,Bachinsky WB, Lasala GP, Tuzcu EM. Effect of torcetrapib on the progression ofcoronary atherosclerosis. N Engl J Med 2007;356:1304–1316.
64. Nissen SE, Tuzcu EM, Brewer HB, Sipahi I, Nicholls SJ, Ganz P, Schoenhagen P,Waters DD, Pepine CJ, Crowe TD, Davidson MH, Deanfield JE, Wisniewski LM,Hanyok JJ, Kassalow LM. Effect of ACAT inhibition on the progression of coron-ary atherosclerosis. N Engl J Med 2006;354:1253–1263.
65. Nissen SE, Tuzcu EM, Libby P, Thompson PD, Ghali M, Garza D, Berman L,Shi H, Buebendorf E, Topol EJ. Effect of antihypertensive agents on cardiovascu-lar events in patients with coronary disease and normal blood pressure: theCAMELOT study: a randomized controlled trial. J Am Med Assoc 2004;292:2217–2225.
66. Rodriguez-Granillo GA, Vos J, Bruining N, Garcia-Garcia HM, de Winter S,Ligthart JM, Deckers JW, Bertrand M, Simoons ML, Ferrari R, Fox KM,Remme W, De Feyter PJ. Long-term effect of perindopril on coronary athero-sclerosis progression (from the perindopril’s prospective effect on coronaryatherosclerosis by angiography and intravascular ultrasound evaluation [PER-SPECTIVE] study). Am J Cardiol 2007;100:159–163.
67. Gerstein HC, Ratner RE, Cannon CP, Serruys PW, Garcia-Garcia HM,van Es GA, Kolatkar NS, Kravitz BG, Miller DM, Huang C, Fitzgerald PJ,Nesto RW. Effect of rosiglitazone on progression of coronary atherosclerosisin patients with type 2 diabetes mellitus and coronary artery disease: the assess-ment on the prevention of progression by rosiglitazone on atherosclerosis indiabetes patients with cardiovascular history trial. Circulation 2010;121:1176–1187.
68. Nissen SE, Nicholls SJ, Wolski K, Nesto R, Kupfer S, Perez A, Jure H, DeLarochelliere R, Staniloae CS, Mavromatis K, Saw J, Hu B, Lincoff AM,Tuzcu EM. Comparison of pioglitazone vs glimepiride on progression of coron-ary atherosclerosis in patients with type 2 diabetes: the PERISCOPE randomizedcontrolled trial. J Am Med Assoc 2008;299:1561–1573.
69. Nasu K, Tsuchikane E, Katoh O, Tanaka N, Kimura M, Ehara M, Kinoshita Y,Matsubara T, Matsuo H, Asakura K, Asakura Y, Terashima M, Takayama T,Honye J, Hirayama A, Saito S, Suzuki T. Effect of fluvastatin on progression ofcoronary atherosclerotic plaque evaluated by virtual histology intravascularultrasound. JACC Cardiovasc Interv 2009;2:689–696.
70. Hong MK, Park DW, Lee CW, Lee SW, Kim YH, Kang DH, Song JK, Kim JJ,Park SW, Park SJ. Effects of statin treatments on coronary plaques assessedby volumetric virtual histology intravascular ultrasound analysis. JACC CardiovascInterv 2009;2:679–688.
71. Serruys PW, Garcia-Garcia HM, Buszman P, Erne P, Verheye S, Aschermann M,Duckers H, Bleie O, Dudek D, Botker HE, von Birgelen C, D’Amico D,Hutchinson T, Zambanini A, Mastik F, van Es GA, van der Steen AF,Vince DG, Ganz P, Hamm CW, Wijns W, Zalewski A. Effects of the directlipoprotein-associated phospholipase A(2) inhibitor darapladib on human coron-ary atherosclerotic plaque. Circulation 2008;118:1172–1182.
72. Manfrini O, Mont E, Leone O, Arbustini E, Eusebi V, Virmani R, Bugiardini R.Sources of error and interpretation of plaque morphology by optical coherencetomography. Am J Cardiol 2006;98:156–159.
73. Sawada T, Shite J, Garcia-Garcia HM, Shinke T, Watanabe S, Otake H,Matsumoto D, Tanino Y, Ogasawara D, Kawamori H, Kato H, Miyoshi N,Yokoyama M, Serruys PW, Hirata K. Feasibility of combined use of intravascularultrasound radiofrequency data analysis and optical coherence tomography fordetecting thin-cap fibroatheroma. Eur Heart J 2008;29:1136–1146.
74. Gonzalo N, Garcia-Garcia HM, Regar E, Barlis P, Wentzel J, Onuma Y, Ligthart J,Serruys PW. In vivo assessment of high-risk coronary plaques at bifurcationswith combined intravascular ultrasound and optical coherence tomography.JACC Cardiovasc Imaging 2009;2:473–482.
Imaging of coronary atherosclerosis 2469bD
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021

75. Rioufol G, Finet G, Ginon I, Andre-Fouet X, Rossi R, Vialle E, Desjoyaux E,Convert G, Huret JF, Tabib A. Multiple atherosclerotic plaque rupture inacute coronary syndrome: a three-vessel intravascular ultrasound study. Circula-tion 2002;106:804–808. doi:10.1161/01.CIR.0000025609.13806.31
76. Hong MK, Mintz GS, Lee CW, Kim YH, Lee SW, Song JM, Han KH, Kang DH,Song JK, Kim JJ, Park SW, Park SJ. Comparison of coronary plaque rupturebetween stable angina and acute myocardial infarction: a three-vessel intravascu-lar ultrasound study in 235 patients. Circulation 2004;110:928–933.
77. Tanaka A, Shimada K, Sano T, Namba M, Sakamoto T, Nishida Y,Kawarabayashi T, Fukuda D, Yoshikawa J. Multiple plaque rupture and C-reactiveprotein in acute myocardial infarction. J Am Coll Cardiol 2005;45:1594–1599.
78. Hong MK, Mintz GS, Lee CW, Lee BK, Yang TH, Kim YH, Song JM, Han KH,Kang DH, Cheong SS, Song JK, Kim JJ, Park SW, Park SJ. The site of plaquerupture in native coronary arteries: a three-vessel intravascular ultrasound analy-sis. J Am Coll Cardiol 2005;46:261–265.
79. Tyczynski P, Pregowski J, Mintz GS, Witkowski A, Kim SW, Waksman R, Satler L,Pichard A, Kalinczuk L, Maehara A, Weissman NJ. Intravascular ultrasoundassessment of ruptured atherosclerotic plaques in left main coronary arteries.Am J Cardiol 2005;96:794–798.
80. Pregowski J, Tyczynski P, Mintz GS, Kim SW, Witkowski A, Waksman R,Pichard A, Satler L, Kent K, Kruk M, Bieganski S, Ohlmann P, Weissman NJ. Inci-dence and clinical correlates of ruptured plaques in saphenous vein grafts: anintravascular ultrasound study. J Am Coll Cardiol 2005;45:1974–1979.
81. Pregowski J, Tyczynski P, Mintz GS, Kim SW, Witkowski A, Satler L, Kruk M,Waksman R, Maehara A, Weissman NJ. Intravascular ultrasound assessment ofthe spatial distribution of ruptured coronary plaques in the left anterior des-cending coronary artery. Am Heart J 2006;151:898–901.
82. Rodriguez-Granillo GA, Garcia-Garcia HM, Valgimigli M, Vaina S, vanMieghem C, van Geuns RJ, van der Ent M, Regar E, de Jaegere P, van derGiessen W, de Feyter P, Serruys PW. Global characterization of coronaryplaque rupture phenotype using three-vessel intravascular ultrasound radiofre-quency data analysis. Eur Heart J 2006;27:1921–1927.
83. Hong YJ, Jeong MH, Choi YH, Ma EH, Ko JS, Lee MG, Park KH, Sim DS,Yoon NS, Youn HJ, Kim KH, Park HW, Kim JH, Ahn Y, Cho JG, Park JC,Kang JC. Differences in intravascular ultrasound findings in culprit lesions ininfarct-related arteries between ST segment elevation myocardial infarctionand non-ST segment elevation myocardial infarction. J Cardiol 2010;56:15–22.
84. Okazaki S, Yokoyama T, Miyauchi K, Shimada K, Kurata T, Sato H, Daida H. Earlystatin treatment in patients with acute coronary syndrome: demonstration of thebeneficial effect on atherosclerotic lesions by serial volumetric intravascularultrasound analysis during half a year after coronary event: the ESTABLISHStudy. Circulation 2004;110:1061–1068.
85. Jensen LO, Thayssen P, Pedersen KE, Stender S, Haghfelt T. Regression of cor-onary atherosclerosis by simvastatin: a serial intravascular ultrasound study. Cir-culation 2004;110:265–270.
86. Petronio AS, Amoroso G, Limbruno U, Papini B, De Carlo M, Micheli A,Ciabatti N, Mariani M. Simvastatin does not inhibit intimal hyperplasia and rest-enosis but promotes plaque regression in normocholesterolemic patientsundergoing coronary stenting: a randomized study with intravascular ultrasound.Am Heart J 2005;149:520–526.
87. Nishioka H, Shimada K, Kataoka T, Hirose M, Asawa K, Hasegawa T,Yamashita H, Ehara S, Kamimori K, Sakamoto T, Kobayashi Y, Yoshimura T,Yoshiyama M, Takeuchi K, Yoshikawa J. Impact of HMG-CoA reductase inhibi-tors for non-treated coronary segments. Osaka City Med J 2004;50:61–68.
88. Tani S, Watanabe I, Anazawa T, Kawamata H, Tachibana E, Furukawa K, Sato Y,Nagao K, Kanmatsuse K, Kushiro T. Effect of pravastatin on malondialdehyde-modified low-density lipoprotein levels and coronary plaque regression asdetermined by three-dimensional intravascular ultrasound. Am J Cardiol 2005;96:1089–1094.
89. Nissen SE, Nicholls SJ, Sipahi I, Libby P, Raichlen JS, Ballantyne CM, Davignon J,Erbel R, Fruchart JC, Tardif J-C, Schoenhagen P, Crowe T, Cain V, Wolski K,Goormastic M, Tuzcu EM, for the ASTEROID Investigators. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTER-OID trial. J Am Med Assoc 2006;295:1556–1565.
90. Takashima H, Ozaki Y, Yasukawa T, Waseda K, Asai K, Wakita Y, Kuroda Y,Kosaka T, Kuhara Y, Ito T. Impact of lipid-lowering therapy with pitavastatin, anew HMG-CoA reductase inhibitor, on regression of coronary atheroscleroticplaque. Circ J 2007;71:1678–1684.
91. Takayama T, Hiro T, Yamagishi M, Daida H, Hirayama A, Saito S, Yamaguchi T,Matsuzaki M. Effect of rosuvastatin on coronary atheroma in stable coronaryartery disease: multicenter coronary atherosclerosis study measuring effects ofrosuvastatin using intravascular ultrasound in Japanese subjects (COSMOS).Circ J 2009;73:2110–2117.
92. Hiro T, Kimura T, Morimoto T, Miyauchi K, Nakagawa Y, Yamagishi M, Ozaki Y,Kimura K, Saito S, Yamaguchi T, Daida H, Matsuzaki M. Effect of intensive statintherapy on regression of coronary atherosclerosis in patients with acute coron-ary syndrome: a multicenter randomized trial evaluated by volumetric intravas-cular ultrasound using pitavastatin versus atorvastatin (JAPAN-ACS [Japanassessment of pitavastatin and atorvastatin in acute coronary syndrome]study). J Am Coll Cardiol 2009;54:293–302.
93. Tardif JC, Gregoire J, L’Allier PL, Anderson TJ, Bertrand O, Reeves F, Title LM,Alfonso F, Schampaert E, Hassan A, McLain R, Pressler ML, Ibrahim R,Lesperance J, Blue J, Heinonen T, Rodes-Cabau J. Effects of the acyl coenzymeA:cholesterol acyltransferase inhibitor avasimibe on human atheroscleroticlesions. Circulation 2004;110:3372–3377.
94. Nissen SE, Tsunoda T, Tuzcu EM, Schoenhagen P, Cooper CJ, Yasin M,Eaton GM, Lauer MA, Sheldon WS, Grines CL, Halpern S, Crowe T,Blankenship JC, Kerensky R. Effect of recombinant ApoA-I Milano on coronaryatherosclerosis in patients with acute coronary syndromes: a randomized con-trolled trial. J Am Med Assoc 2003;290:2292–2300.
95. Tardif JC, Gregoire J, L’Allier PL, Ibrahim R, Anderson TJ, Reeves F, Title LM,Schampaert E, LeMay M, Lesperance J, Scott R, Guertin MC, Brennan ML,Hazen SL, Bertrand OF. Effects of the antioxidant succinobucol (AGI-1067)on human atherosclerosis in a randomized clinical trial. Atherosclerosis 2008;197:480–486.
96. Nissen SE, Nicholls SJ, Wolski K, Rodes-Cabau J, Cannon CP, Deanfield JE,Despres JP, Kastelein JJ, Steinhubl SR, Kapadia S, Yasin M, Ruzyllo W,Gaudin C, Job B, Hu B, Bhatt DL, Lincoff AM, Tuzcu EM. Effect of rimonabanton progression of atherosclerosis in patients with abdominal obesity and coron-ary artery disease: the STRADIVARIUS randomized controlled trial. J Am MedAssoc 2008;299:1547–1560.
97. Luscher TF, Pieper M, Tendera M, Vrolix M, Rutsch W, van den Branden F, Gil R,Bischoff KO, Haude M, Fischer D, Meinertz T, Munzel T. A randomized placebo-controlled study on the effect of nifedipine on coronary endothelial function andplaque formation in patients with coronary artery disease: the ENCORE II study.Eur Heart J 2009;30:1590–1597.
98. Yokoyama M, Komiyama N, Courtney BK, Nakayama T, Namikawa S,Kuriyama N, Koizumi T, Nameki M, Fitzgerald PJ, Komuro I. Plasma low-densitylipoprotein reduction and structural effects on coronary atherosclerotic plaquesby atorvastatin as clinically assessed with intravascular ultrasound radio-frequency signal analysis: a randomized prospective study. Am Heart J 2005;150:287.
99. Kawasaki M, Sano K, Okubo M, Yokoyama H, Ito Y, Murata I, Tsuchiya K,Minatoguchi S, Zhou X, Fujita H, Fujiwara H. Volumetric quantitative analysisof tissue characteristics of coronary plaques after statin therapy using three-dimensional integrated backscatter intravascular ultrasound. J Am Coll Cardiol2005;45:1946–1953.
100. Toi T, Taguchi I, Yoneda S, Kageyama M, Kikuchi A, Tokura M, Kanaya T, Abe S,Matsuda R, Kaneko N. Early effect of lipid-lowering therapy with pitavastatin onregression of coronary atherosclerotic plaque. Comparison with atorvastatin.Circ J 2009;73:1466–1472.
101. Miyagi M, Ishii H, Murakami R, Isobe S, Hayashi M, Amano T, Arai K, Ohashi T,Uetani T, Matsubara T, Murohara T. Impact of long-term statin treatment oncoronary plaque composition at angiographically severe lesions: a nonrando-mized study of the history of long-term statin treatment before coronary angio-plasty. Clin Ther 2009;31:64–73.
H.M. Garcia-Garcia et al.2469cD
ownloaded from
https://academic.oup.com
/eurheartj/article/31/20/2456/613364 by guest on 24 Novem
ber 2021