Imaging of Bowel Obstruction
55
Imaging of Bowel Obstruction Rathachai Kaewlai, MD Ramathibodi Hospital, Mahidol University, Bangkok Emergency Radiology Minicourse 2015
-
Upload
rathachai-kaewlai -
Category
Health & Medicine
-
view
573 -
download
1
Transcript of Imaging of Bowel Obstruction

Imaging of Bowel Obstruction
Rathachai Kaewlai, MD Ramathibodi Hospital, Mahidol University, Bangkok
Emergency Radiology Minicourse 2015

What to Cover…
Imaging techniques
Gastric obstruction Small bowel obstruction Large bowel obstruction

Bowel Obstruction
Lack of transit of bowel contents
Small bowel obstruction: high or low Large bowel obstruction Simple (intact blood supply) vs. strangulated
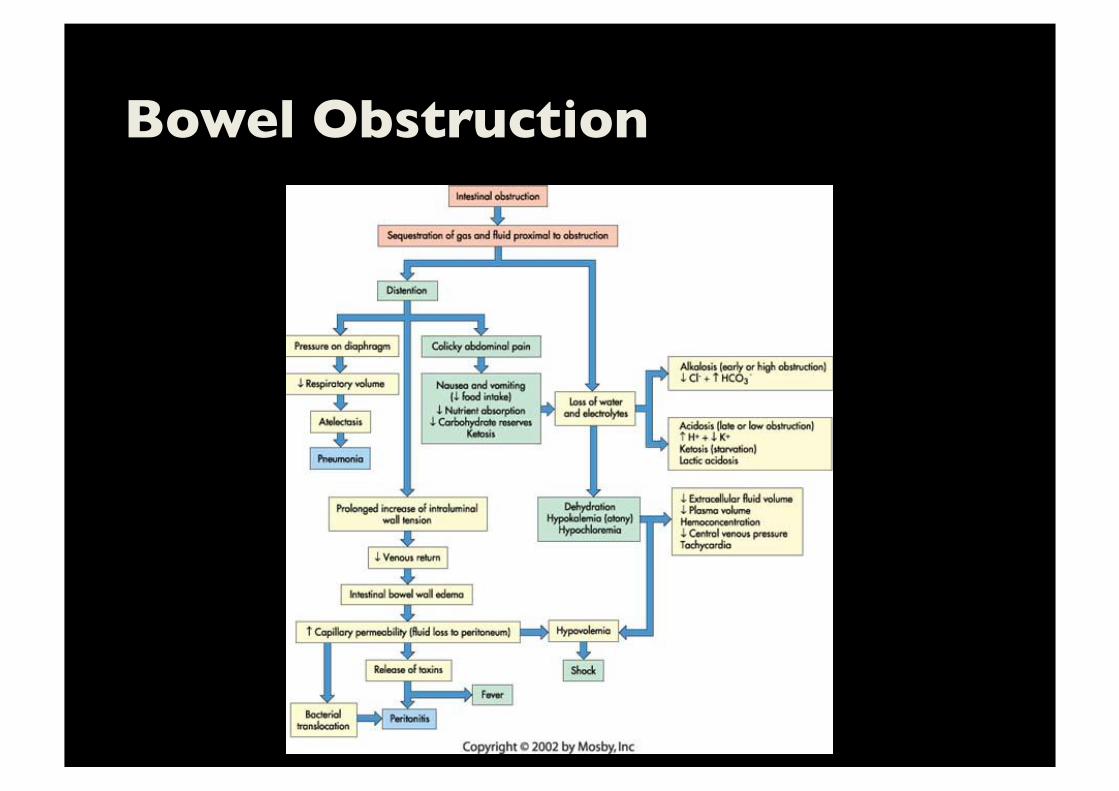
Bowel Obstruction

Clinical Presentation
Depend upon site of obstruction
High SBO – vomiting early, profuse, rapid dehydration Low SBO – pain with distension LBO – constipation Strangulation – shock, rigidity/rebound (localized/diffuse)
Treatment
Conservative
Surgery: Early – Strangulation
Closed loop obstruction Obstructed/strangulated hernia Delayed –
Adhesive obstruction without pain

Aims of Investigations
Is obstruction present?
Where is the location? What is the cause? Is emergent surgery needed?
Strangulation Closed loop Obstructed hernia
Radiography
CT

CT Techniques
Helical scan, thinnest collimation
Coronal reformats IV contrast, single venous phase No need for oral contrast. May be neutral
contrast No rectal contrast needed May be helpful if LBO, neutral contrast preferred

Gastric Outlet Obstruction (GOO):���Etiology Malignancy > benign (PUD)
Extrinsic: pancreatitis with pseudocyst, hematoma Intrinsic: malignancy, PUD with stricture
Intraluminal: bezoars, FB, GS Acute incarceration or strangulation:
obstructed paraesophageal hernia, gastric volvulus

Radiography
Markedly dilated stomach, air or fluid filled
Filling defect (cancer)
Calcified gallstone (Bouveret syndrome)
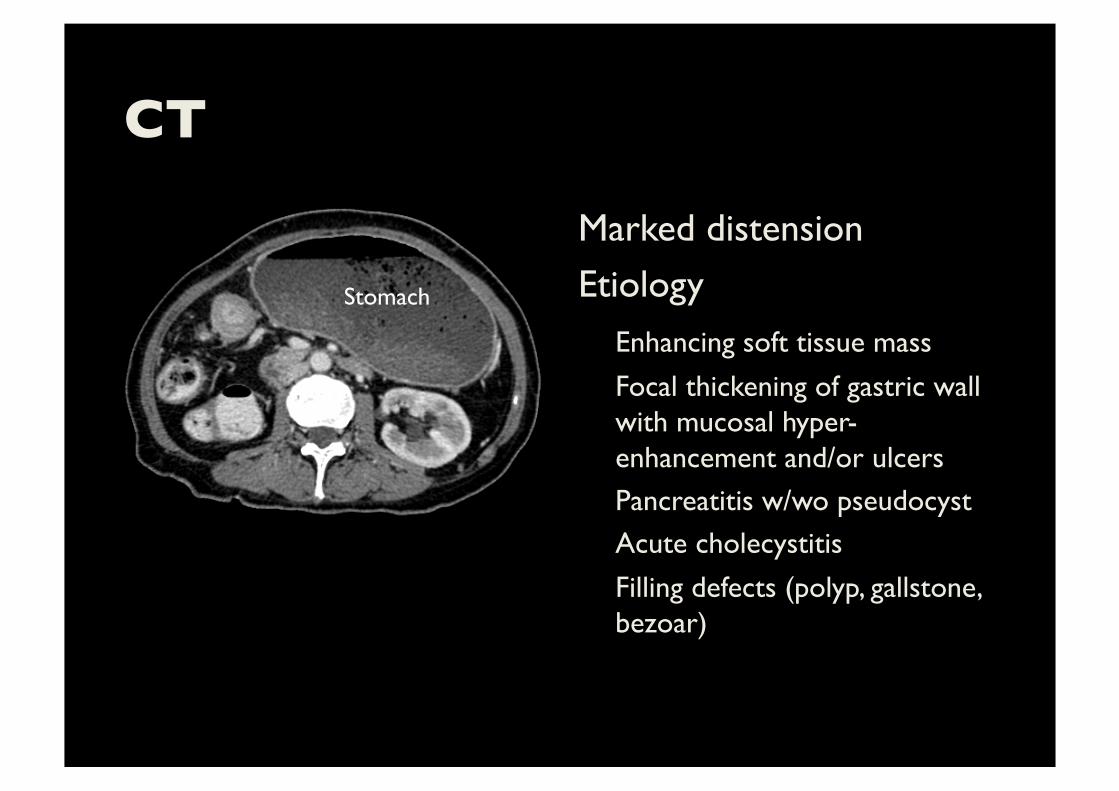
CT
Marked distension
Etiology Enhancing soft tissue mass
Focal thickening of gastric wall with mucosal hyper-enhancement and/or ulcers Pancreatitis w/wo pseudocyst Acute cholecystitis
Filling defects (polyp, gallstone, bezoar)
Stomach
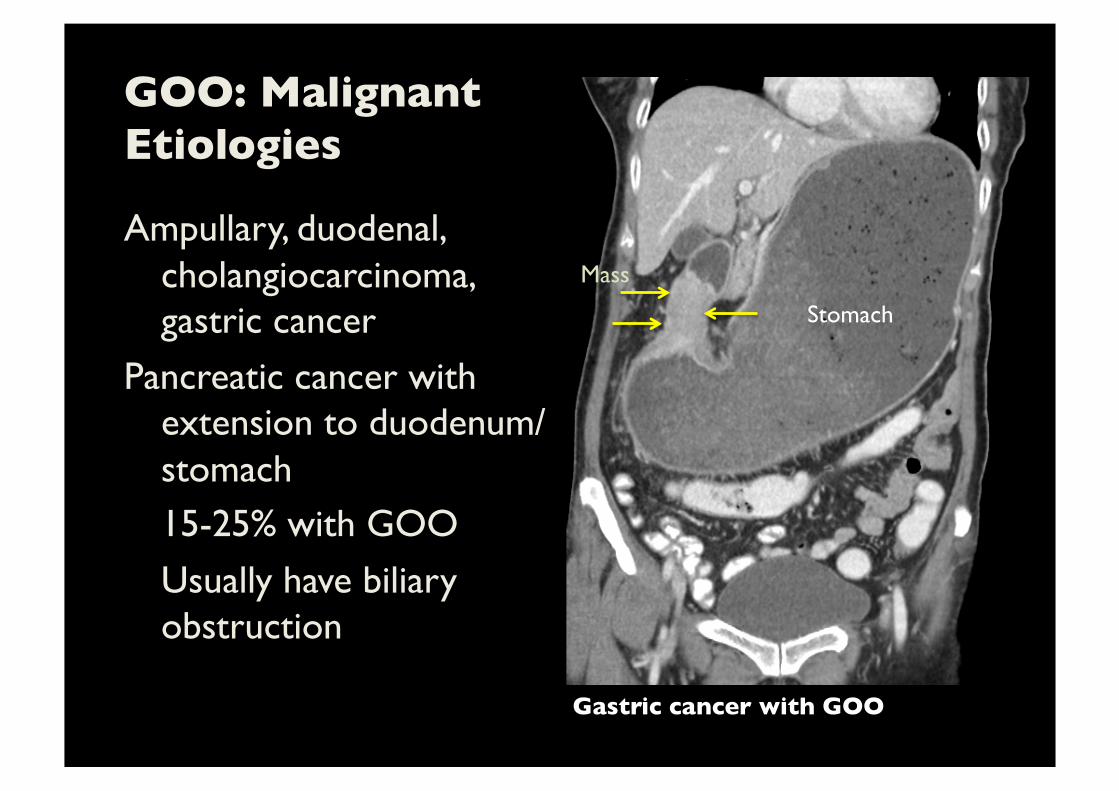
GOO: Malignant ���Etiologies
Ampullary, duodenal, cholangiocarcinoma, gastric cancer
Pancreatic cancer with extension to duodenum/stomach 15-25% with GOO
Usually have biliary obstruction
Stomach
Mass
Gastric cancer with GOO

GOO: Benign Etiologies
PUD (acute vs scarring/fibrosis)
Polyps, caustic ingestion, web, GS, pancreatic pseudocyst, bezoar

Gastritis vs. Neoplasm
Difficult differentiation on imaging. Endoscopy necessary to differentiate neoplasm
Gastritis Layered (halo) appearance Diffuse, segmental, or annular
Neoplasm Nodal disease
Metastasis Pseudothickening of antrum
Diagnostic Approach
Dilated stomach may contain up to 5L of fluid
Functional disturbance Postoperative, severe trauma, immobilization, inflammatory disease of abdomen, neurogenic, diabetes
Mechanical obstruction (stomach, duodenal, high SB)
Differentiate benign from malignant processes

Gastric Volvulus
Abnormal rotation around its axis
Surgical emergency if acute Organo-axial, mesenteroaxial, or both
Organoaxial Stomach rotates around axis connecting EGJ and pylorus
Mesenteroaxial Less common
Stomach rotates around axis bisecting both lesser and greater curvatures
Image: Differen-al diagnosis in conven-onal gastrointes-nal radiology. Burgener FA, Kormano M.

Gastric Volvulus
Diaphragmatic defect m.c. causative factor
Intrathoracic stomach Transverse lie with single air-fluid level = organoaxial Spherical lucency with beak in distal stomach + differential air fluid levels = mesenteroaxial
Case courtesy of Radiopaedia.org
Case courtesy of Dr Maxime St-Amant, Radiopaedia.org
Organoaxial volvulus
Mesenteroaxial volvulus
*
*
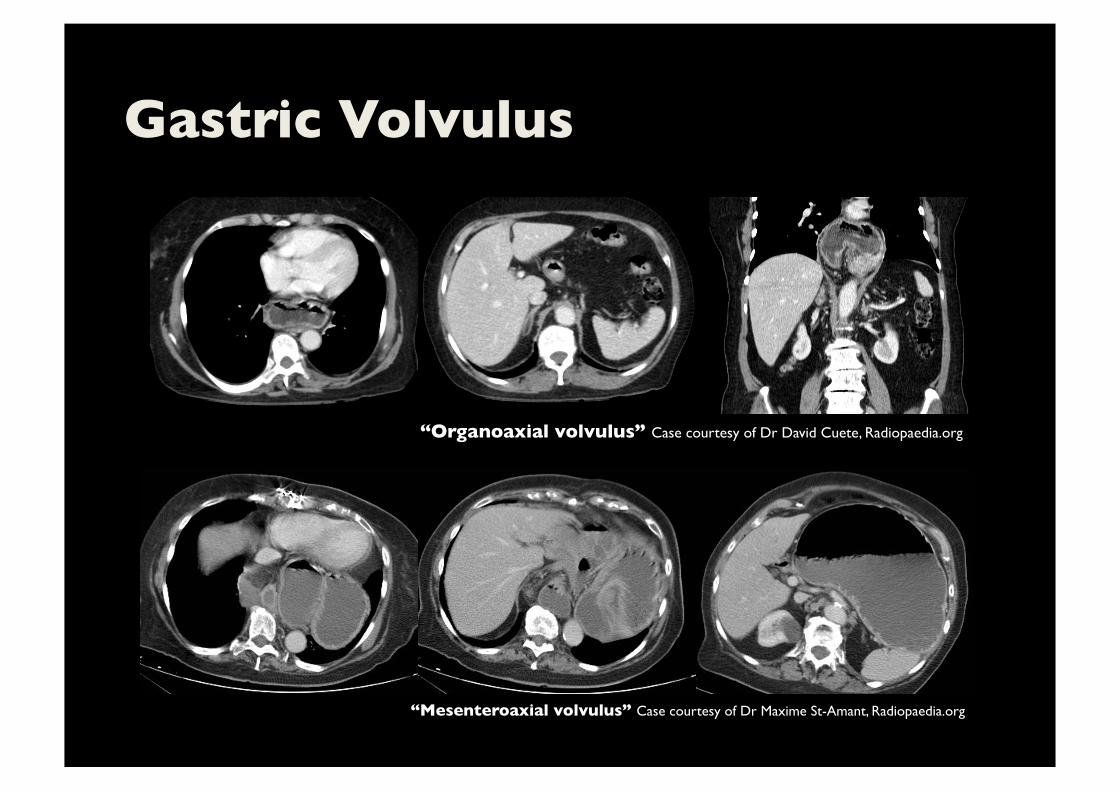
Gastric Volvulus
“Organoaxial volvulus” Case courtesy of Dr David Cuete, Radiopaedia.org
“Mesenteroaxial volvulus” Case courtesy of Dr Maxime St-Amant, Radiopaedia.org

Superior Mesenteric ���Artery Syndrome
Dilatation of 1st and 2nd part of duodenum with abrupt narrowing at 3rd portion
Relieved by changing position
Aorta-SMA distance <8-10 mm
Aortomesenteric angle <22 degrees
(compression of LRV – renal vein thrombosis, pneumatosis, PVG, AAA)
Narrow aortomesenteric angle and compression at 3rd portion of duodenum

Small Bowel Obstruction (SBO)
Dilated small bowel proximal to the site of obstruction with distal decompression
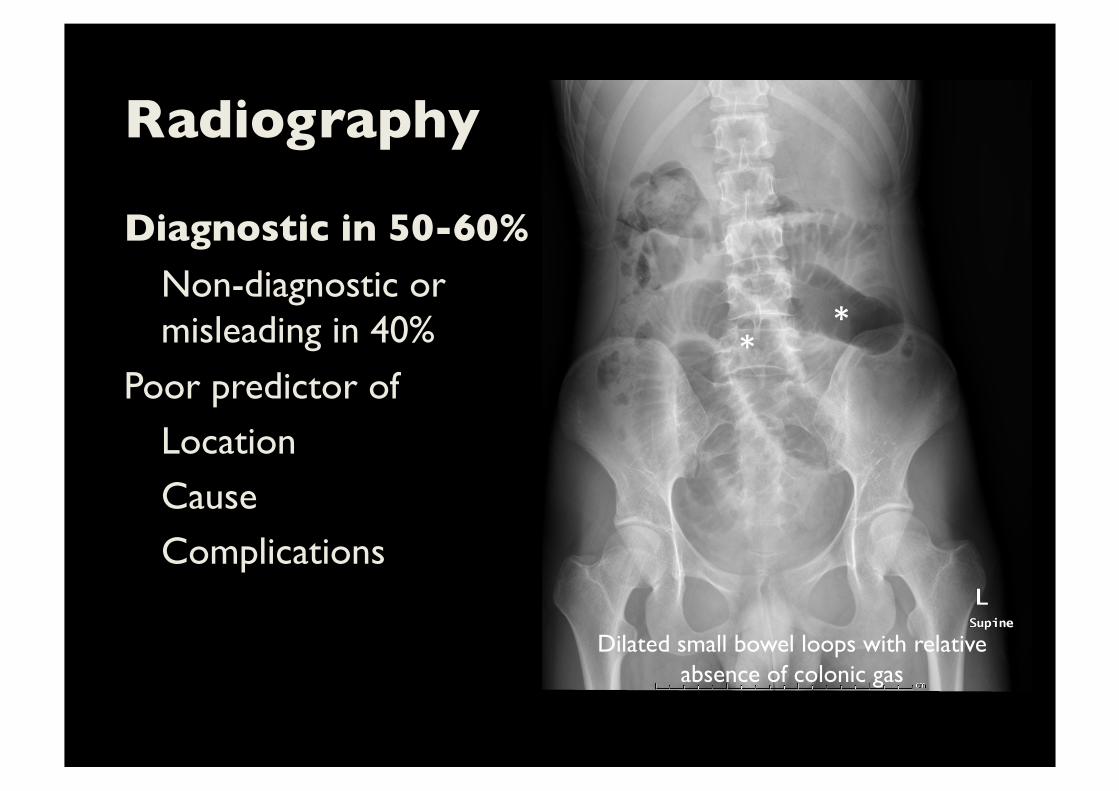
Radiography
Diagnostic in 50-60% Non-diagnostic or misleading in 40%
Poor predictor of Location Cause Complications
* *
Dilated small bowel loops with relative absence of colonic gas

Radiography
Dilated small bowel >3 cm
Paucity of colonic gas Air fluid levels Multiple
Differential Longer than 2.5 cm
String of beads sign
Multiple air fluid levels in dilated small bowel loops

CT
Quick and accurate
No need for luminal contrast
Bowel wall assessment Extraluminal abnormalities
* *
* *
Diffuse, fluid-filled, dilated loops of small bowel
Free fluid

CT: Indications
Non-diagnostic radiography but clinical suspicion
Virgin abdomen History of abdominal malignancy Suspected complications
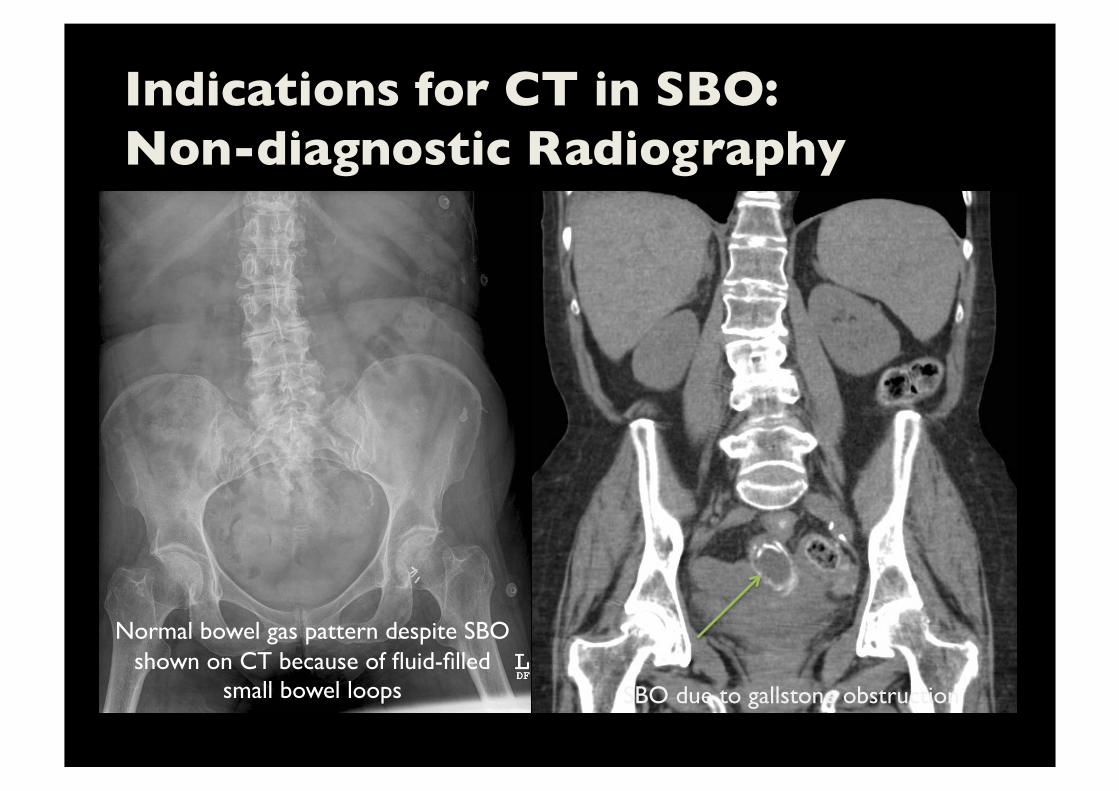
Indications for CT in SBO:���Non-diagnostic Radiography
SBO due to gallstone obstruction
Normal bowel gas pattern despite SBO shown on CT because of fluid-filled
small bowel loops

Indications for CT in SBO:���Virgin Abdomen Known diseases
Metastasis (54%) Crohn disease (46%)
No known diseases
Adhesions (75%) Metastasis (10%) Rare: sclerosing encapsulating peritonitis, Meckel diverticulum, gallstone ileus
Beardsley C, et al. Am J Surg 2014

Indications for CT in SBO:���History of Abdominal Malignancy Spread/extent of tumor around bowel
Pre-operative planning for bypass/debulking procedures

Transition Point
Dilated loops change in caliber to decompressed loops
Trace rectum ! colon ! small bowel Small bowel feces Scroll images on workstation
(difficult on hardcopy films) Multiplanar reformats

Transition Point
Adhesions inferred when no cause identified
Abrupt tapering Beak
External hernias
Tumors, esp. metastasis to bowel/peritoneum Inflammation/infection, gallstones CT accuracy 63-95% for identifying transition point

Transition Point Tells Etiology of Obstruction
Cecal cancer Femoral hernia
Transition point
Transition point

Small Bowel Feces Sign
Gas bubbles and particulate matter within dilated SB
Usually just proximal to transition point
Secondary to prolonged stasis Transition point

Small Bowel Feces Sign
Suggestive of preserved SB function
Negative predictor of failure of conservative Rx
Unlikely to be ischemic Longer segment, less chance
of getting surgery
SB feces

Etiology of SBO
Adhesions 50-75%
Hernias 8-15% Malignancies 10-15% Others: Crohn, intussusception, volvulus, trauma,
iatrogenic conditions

Adhesions
Most common sites = omentum to incision site
Most problematic adhesions = involving small bowel Appendectomy, colorectal surgery and gynecology Most common to produce adhesive obstruction
Anytime from operation 20% <1m 20% >10y
Dayton MT et al. 2012 Curr Probl Surg

External Hernia
2nd most common cause of SBO
Inguinal > femoral
Umbilical = m/c congenital hernia
Incisional and parastomal = m/c iatrogenic hernia
Others: spigelian, lumbar, Richter, Littre Umbilical hernia,
obstructed & strangulated
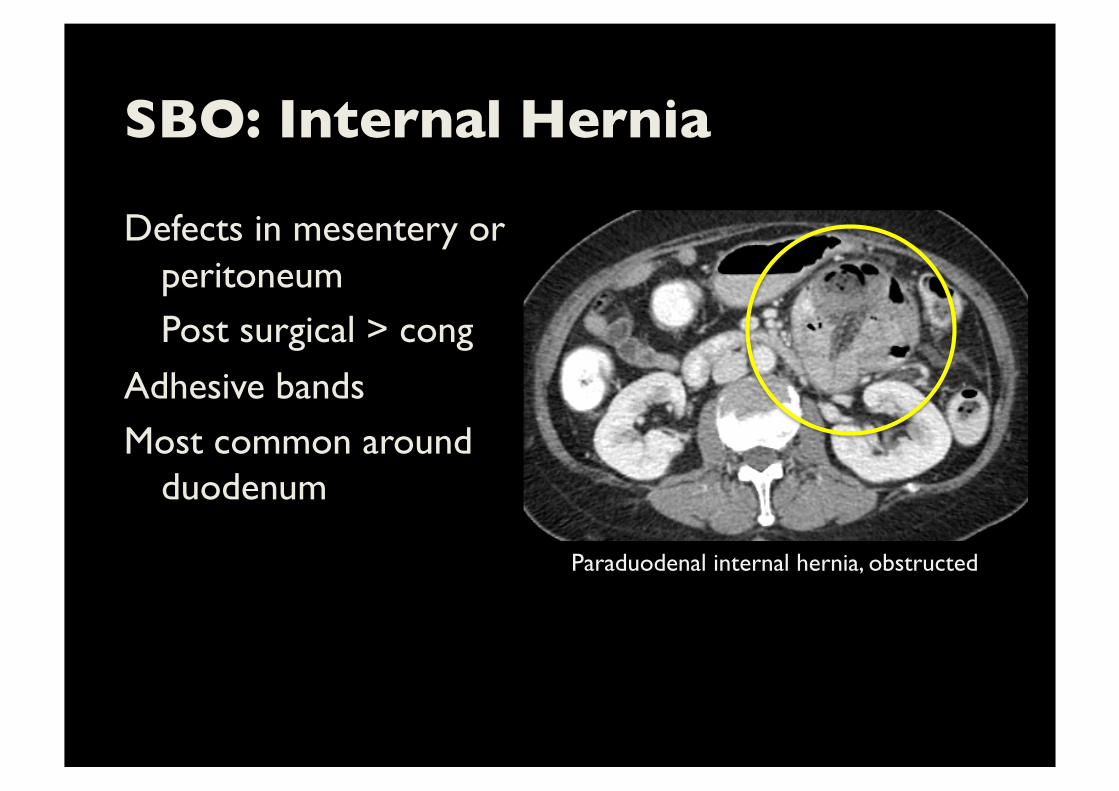
SBO: Internal Hernia
Defects in mesentery or peritoneum Post surgical > cong
Adhesive bands Most common around
duodenum
Paraduodenal internal hernia, obstructed

Obstructing Tumors
Adenocarcinoma
Irregular, nodular mass Carcinoid rarely obstructive GIST
Lymphoma rarely obstructive Peritoneal carcinomatosis Ovary, colon, stomach, pancreas, breast, endometrium Small bowel adenocarcinoma, obstructed
Diagnologic.com
Others
Intussusception
Inflammatory bowel TB very common inflammatory cause of SBO, ileocecal, local nodes with hypodense center
Acute Crohn Chronic Crohn Pancreatitis, diverticulitis and appendicitis
Radiation enteropathy Stone and bezoar
Is Emergent Surgery Needed?
YES IF:
Strangulation = SBO + Ischemia Closed loop obstruction
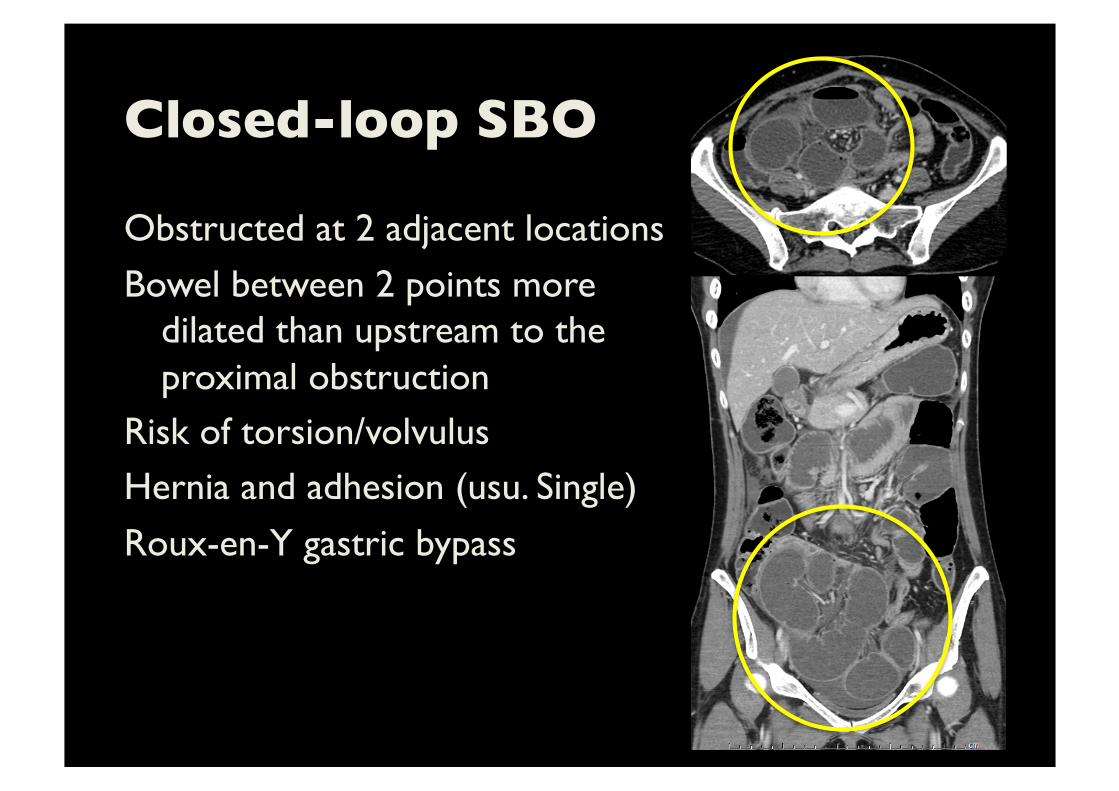
Closed-loop SBO
Obstructed at 2 adjacent locations
Bowel between 2 points more dilated than upstream to the proximal obstruction
Risk of torsion/volvulus Hernia and adhesion (usu. Single)
Roux-en-Y gastric bypass

Closed-loop SBO
U-, C- or coffee bean
Radial orientation of dilated loops
Beak Balloons on a string Whirl sign Sensitivity 60%
PPV 80%

Ischemia Complicating SBO
Two mechanisms
Inc. pressure in bowel wall Direct occlusion of mesenteric vessels 2/2 torsion, hernia or tight adhesion
Mortality 25% (only 2% for non-strangulated SBO)
Need high suspicion

Ischemia Complicating SBO
Enhancement – hyper ! hypo ! absent Reduced bowel wall enhancement 11x probability of strangulation
Wall thickening – nonspecific Wall thinning can be 2/2
transmural infarction Pneumatosis and
portomesenteric gas
Millet I, et al. Eur Radiol 2014

Mimics of SBO on AXR
Ileus
Mesenteric ischemia Obstruction of cecum/
ascending colon (cecum filled with mass or fluid)
SMA occlusion
Large Bowel Obstruction (LBO):���Etiology More in elderly
Malignancy 60% Volvulus 15% Diverticulitis 10%
Others: incarcerated hernia, fecal impaction, adhesion
15-20% of colorectal malignancy present with LBO
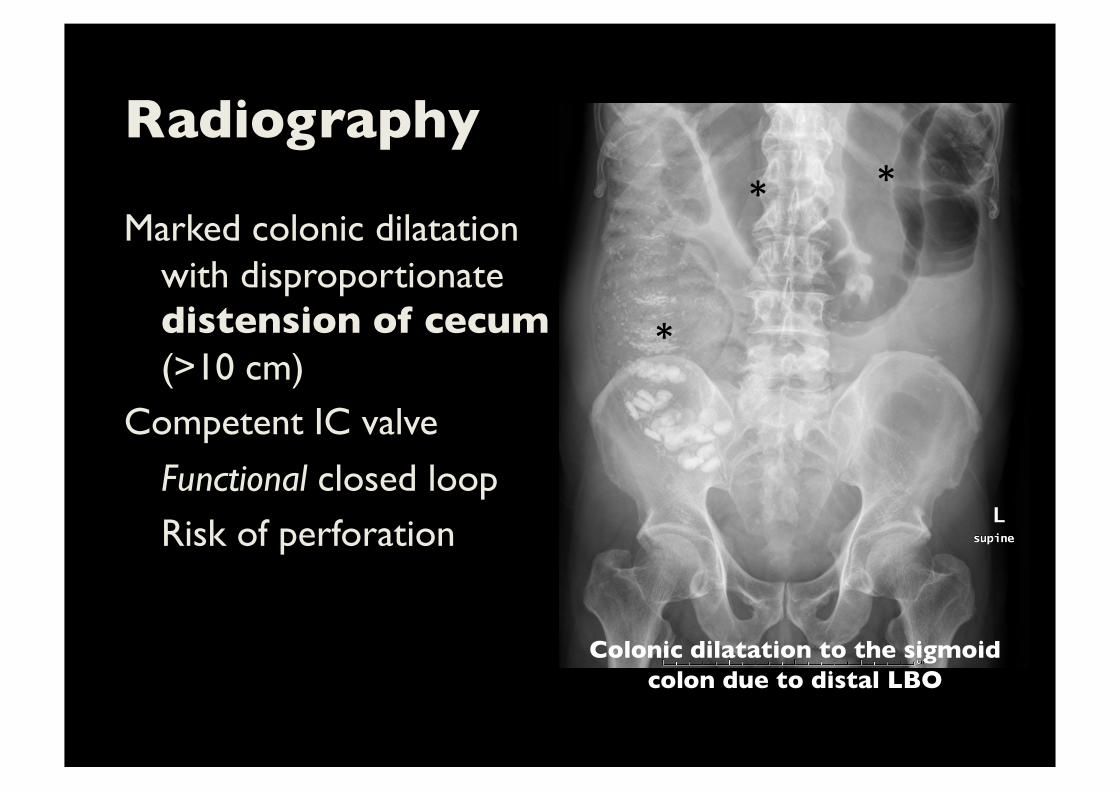
Radiography
Marked colonic dilatation with disproportionate distension of cecum (>10 cm)
Competent IC valve
Functional closed loop Risk of perforation
* *
*
Colonic dilatation to the sigmoid colon due to distal LBO

Radiography
Incompetent IC valve
Dilated SB and colon Cecum dilated v. non-dilated
Difficult Dx on AXR Poor sensitivity, specificity and interobserver agreement
* *
Colonic and small bowel dilatation to the splenic flexure colon due to
distal LBO
*

Colon Cancer
CT sensitivity and specificity 90%
Imaging of choice = CT 60% of LBO Mostly adenocarcinoma
Mass, involvement of adjacent structures, lymphadenopathy, intraperitoneal metastasis
Cancer of the splenic flexure colon

Extrinsic Neoplasm
Direct invasion
Intraperitoneal seeding Hematogenous metastasis Lymphatic extension

Sigmoid Volvulus
Twist around sigmoid mesocolon
Massive distension Lack of haustration Coffee bean shaped
classic- Rt dome Central stripe

Sigmoid Volvulus
Diagrams from surgeonsblog.blogspot.com and pmj.bmj.com
Beak sign

Cecal Volvulus
Dilated cecum
Dilated cecum
Beak sign
Volvulus: CT?
Classic picture
Colon dilatation alone LBO Toxic megacolon
Pseudo-obstruction Colon + SB dilatation LBO
Ileus
CT
Rx
CT

Mimics of LBO
Toxic megacolon
Clinical toxicity Colonic pseudo-obstruction CT often needed to exclude a mass
Diffuse colonic dilatation. CT confirmed no evidence of obstruction

Summary
Investigative questions:
Obstruction present? Where? Cause? Surgery? Radiography still has a limited role in bowel obstruction CT is the mainstay imaging:
Quick and safe No luminal contrast Confirm obstruction, site, etiology, surgical need
Extraluminal abnormalities