Images in Ultrasound and CT imaging assessment of renal ...
3
Images in . . . Ultrasound and CT imaging assessment of renal angiomyolipoma Alexandros Kotis, 1 Filippos Lisgos, 2 Stylianos Karatapanis 2 1 CT and MRI Department, General Hospital of Rhodes, Rhodes, Greece 2 Department of 1st Internal Medicine, General Hospital of Rhodes, Rhodes, Greece Correspondence to Alexandros Kotis, [email protected] Summary The authors report a case of a 41-year-old woman who was admitted to the emergency department of our hospital because of acute right flank pain. Laboratory investigations and cultures were negative. A transabdominal ultrasonography revealed a large mass of the upper pole of the right kidney as an incidental finding. CASE PRESENTATION A 41-year-old woman was admitted to the emergency department of our hospital because of acute right flank pain. Laboratory investigations and cultures were negative. A transabdominal colour doppler ultrasonography scan using head transducer 1.75–4 MHz (Siemens/Acuson; Aspen, Mountain view, California, USA) revealed a large (5×4 cm), highly hyperechoic well-demarcated exophytic mass with shadowing, of the upper pole of the right kidney as an inci- dental finding (figure 1). Subsequently abdominal CT spiral scan (10/10 mm sections GE SX Prospeed before and after contrast injection) showed a mass with mixed hyper- dense and fatty tissue elements (figures 2,3). Renal excre- tion and filling of the urinary bladder were both satisfactory. There was no evidence of lymph node enlarge- ment or other space occupying lesion in the abdomen. All the diagnostic imaging findings were consistent with the diagnosis of angiomyolipoma. A follow-up was recommended. Figure 1 Large uniformly hyperechoic mass of the upper pole of the right kidney with sharp borders where echogenicity of the mass is at least equal to that of renal sinus fat. A picture of the classic ultrasonography appearance of acute myeloid leukaemia. 1 of 3 BMJ Case Reports 2010; doi:10.1136/bcr.01.2010.2624 on 17 February 2022 by guest. Protected by copyright. http://casereports.bmj.com/ BMJ Case Reports: first published as 10.1136/bcr.01.2010.2624 on 29 November 2010. Downloaded from
Transcript of Images in Ultrasound and CT imaging assessment of renal ...
Images in . . .
Ultrasound and CT imaging assessment of renalangiomyolipoma
Alexandros Kotis,1 Filippos Lisgos,2 Stylianos Karatapanis2
1 CT and MRI Department, General Hospital of Rhodes, Rhodes, Greece2 Department of 1st Internal Medicine, General Hospital of Rhodes, Rhodes, Greece
Correspondence to Alexandros Kotis, [email protected]
SummaryThe authors report a case of a 41-year-old woman who was admitted to the emergency department of our hospital because of acute right flankpain. Laboratory investigations and cultures were negative. A transabdominal ultrasonography revealed a large mass of the upper pole of theright kidney as an incidental finding.
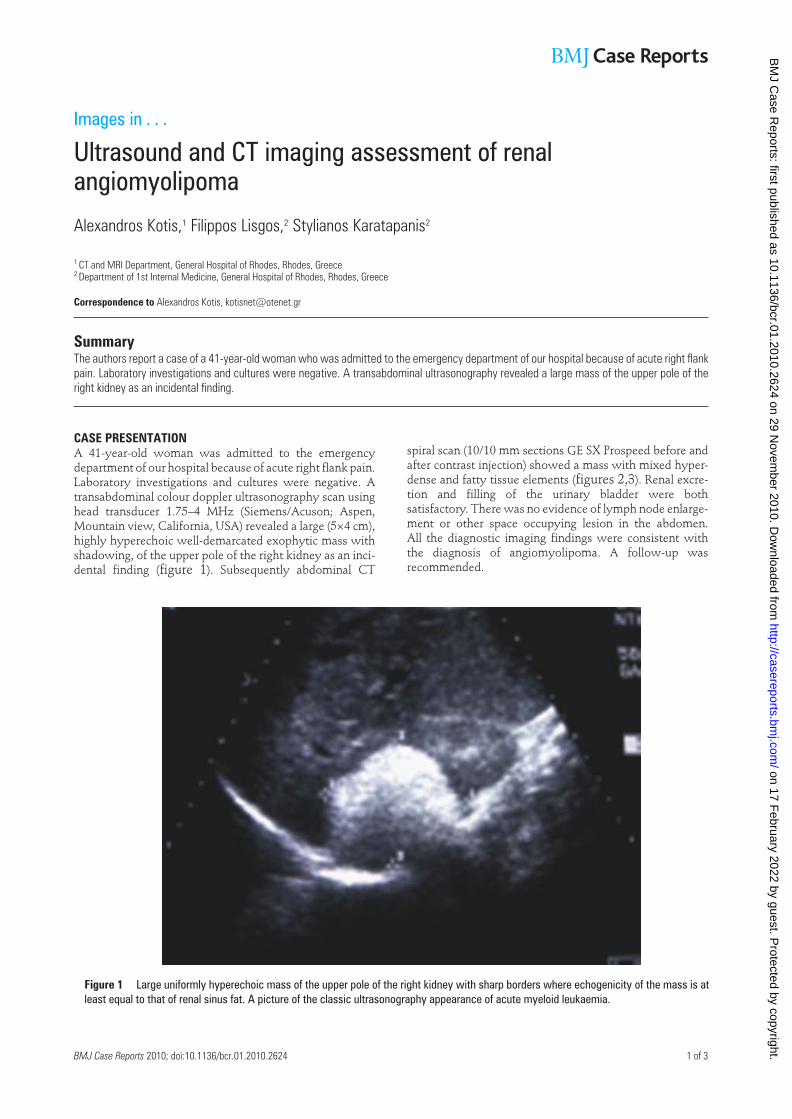
CASE PRESENTATIONA 41-year-old woman was admitted to the emergencydepartment of our hospital because of acute right flank pain.Laboratory investigations and cultures were negative. Atransabdominal colour doppler ultrasonography scan usinghead transducer 1.75–4 MHz (Siemens/Acuson; Aspen,Mountain view, California, USA) revealed a large (5×4 cm),highly hyperechoic well-demarcated exophytic mass withshadowing, of the upper pole of the right kidney as an inci-dental finding (figure 1). Subsequently abdominal CT
spiral scan (10/10 mm sections GE SX Prospeed before andafter contrast injection) showed a mass with mixed hyper-dense and fatty tissue elements (figures 2,3). Renal excre-tion and filling of the urinary bladder were bothsatisfactory. There was no evidence of lymph node enlarge-ment or other space occupying lesion in the abdomen.All the diagnostic imaging findings were consistent withthe diagnosis of angiomyolipoma. A follow-up wasrecommended.
Figure 1 Large uniformly hyperechoic mass of the upper pole of the right kidney with sharp borders where echogenicity of the mass is atleast equal to that of renal sinus fat. A picture of the classic ultrasonography appearance of acute myeloid leukaemia.
1 of 3BMJ Case Reports 2010; doi:10.1136/bcr.01.2010.2624
on 17 February 2022 by guest. P
rotected by copyright.http://casereports.bm
j.com/
BM
J Case R
eports: first published as 10.1136/bcr.01.2010.2624 on 29 Novem
ber 2010. Dow
nloaded from

Figure 2 CT shows well-demarcated mass of the upper pole of the right kidney with mixed soft tissue and fatty tissue elements.
Figure 3 CT picture of angiomyolipoma. Enhancement of smooth muscle and vascular portions of the tumour after administration ofcontrast.
2 of 4 BMJ Case Reports 2010; doi:10.1136/bcr.01.2010.2624
on 17 February 2022 by guest. P
rotected by copyright.http://casereports.bm
j.com/
BM
J Case R
eports: first published as 10.1136/bcr.01.2010.2624 on 29 Novem
ber 2010. Dow
nloaded from

DISCUSSIONAngiomyolipoma is a benign renal neoplasm composed offat, vascular and smooth muscle elements. It has a preva-lence of about 0.3–3%. Two types are described: isolatedangiomyolipoma and angiomyolipoma associated withtuberous sclerosis. Isolated angiomyolipoma occurssporadically, is often solitary and accounts for 80% of allangiomyolipomas.1 Shadowing on sonography is seen in33% of acute myeloid leukaemias.2 3 In the general popula-tion in both sexes angiomyolipoma are most common inthe age group 40–45 years. The mean age at presentation inpatients with isolated angiomyolipoma is 43 years. Thisneoplasm is about four times more common in women thanin men and interestingly 80% of cases involve the right kid-ney. Angiomyolipomas have thicker arteries than normalbut abnormally weak vessel walls which predispose toaneurysm formation.4 Angiomyolipoma that is associatedwith tuberous sclerosis accounts for 20% of angiomyolipo-mas. The lesions are typically larger than isolated angi-omyolipomas, and they are often bilateral and multiple.Angiomyolipomas occur in 80% of patients with tuberoussclerosis.1 The male-to-female distribution of angiomyoli-poma in patients with tuberous sclerosis is almost equal.Angiomyolipomas occur in young women with lymphan-giomyomatosis without other stigmata of tuberous sclero-sis. Although angiomyolipomas are considered benign, rarecases that are possibly related to multicentric disease havebeen reported regarding extension into the renal vein, theinferior vena cava, or both; deposits in the regional lymphnodes have also been reported. The risk is probably verylow in tumours that are <3 cm in diameter. Apart from thisgroup with tuberous sclerosis, follow-up may be reason-ably restricted to patients with sporadic tumours >4 cm in
diameter, in whom the prevalence rate of haemorrhagiccomplications is higher. Thin section multidetector CT isthe preferred method to demonstrate fat in problem cases(table 1).5
Table 1 Examination methods of angiomyolipomaPlain abdominal radiography Ultrasonography
CT scanning Intravenous urography
Renal arterial embolisation Isotope renography and dimercapto-succinic acid
Angiography
Percutaneous renal biopsy DMSA scanning
MRI Renal arterial embolisation
DMSA, dimercaptosuccinic acid.
Competing interests None.
Patient consent Obtained.
REFERENCES1. Rakowski SK, Winterkorn EB, Paul E, et al. Renal manifestations of tuberous
sclerosis complex: incidence, prognosis, and predictive factors. Kidney Int2006;70:1777–82.
2. Rumack CM, Wilson SR, Charboneau JW. The urinary tract. In: Wilson SR, ed.Diagnostic Ultrasound. Third edition. St. Louis: Elsevier Mosby 2005:321–93.
3. Siegel CL, Middleton WD, Teefey SA, et al. Angiomyolipoma and renal cellcarcinoma: US differentiation. Radiology 1996;198:789–93.
4. Webb WR, Brant WE, Major NM. Kidneys and ureters. In: Webb WR, Brant WE,Major NM, eds. Fundamentals of Body CT. Third edition. Philadelphia, PA: Saun-ders 2005:273–302.
5. Brant WE. Adrenal glands and kidneys. In: Brant WE, Helms CA, eds.Fundamentals of Diagnostic Radiology. Third edition. Baltimore: Lippincott Will-iams & Wilkins 2007:867–86.
This pdf has been created automatically from the final edited text and images.
Copyright 2010 BMJ Publishing Group. All rights reserved. For permission to reuse any of this content visithttp://group.bmj.com/group/rights-licensing/permissions.BMJ Case Report Fellows may re-use this article for personal use and teaching without any further permission.
Please cite this article as follows (you will need to access the article online to obtain the date of publication).
Kotis A, Lisgos F, Karatapanis S Ultrasound and CT imaging assessment of renal angiomyolipoma. BMJ Case Reports 2010;10.1136/bcr.01.2010.2624, date ofpublication
Become a Fellow of BMJ Case Reports today and you can:▲
Submit as many cases as you like▲
Enjoy fast sympathetic peer review and rapid publication of accepted articles▲
Access all the published articles▲
Re-use any of the published material for personal use and teaching without further permission
For information on Institutional Fellowships contact [email protected]
Visit casereports.bmj.com for more articles like this and to become a Fellow
3 of 3BMJ Case Reports 2010; doi:10.1136/bcr.01.2010.2624
on 17 February 2022 by guest. P
rotected by copyright.http://casereports.bm
j.com/
BM
J Case R
eports: first published as 10.1136/bcr.01.2010.2624 on 29 Novem
ber 2010. Dow
nloaded from