
Il Management delle Sindromi Coronarie Acute oggi Il ... · with ticagrelor compared with...
34
Il Management delle Sindromi Coronarie Acute oggi Il paziente anziano e con IRC grave Filippo M. Sarullo U.O. di Riabilitazione Cardiovascolare Ospedale Buccheri La Ferla FBF Palermo
Transcript of Il Management delle Sindromi Coronarie Acute oggi Il ... · with ticagrelor compared with...
Il Management delle
Sindromi Coronarie Acute
oggi
Il paziente anziano e con
IRC grave
Filippo M. Sarullo
U.O. di Riabilitazione Cardiovascolare
Ospedale Buccheri La Ferla FBF
Palermo
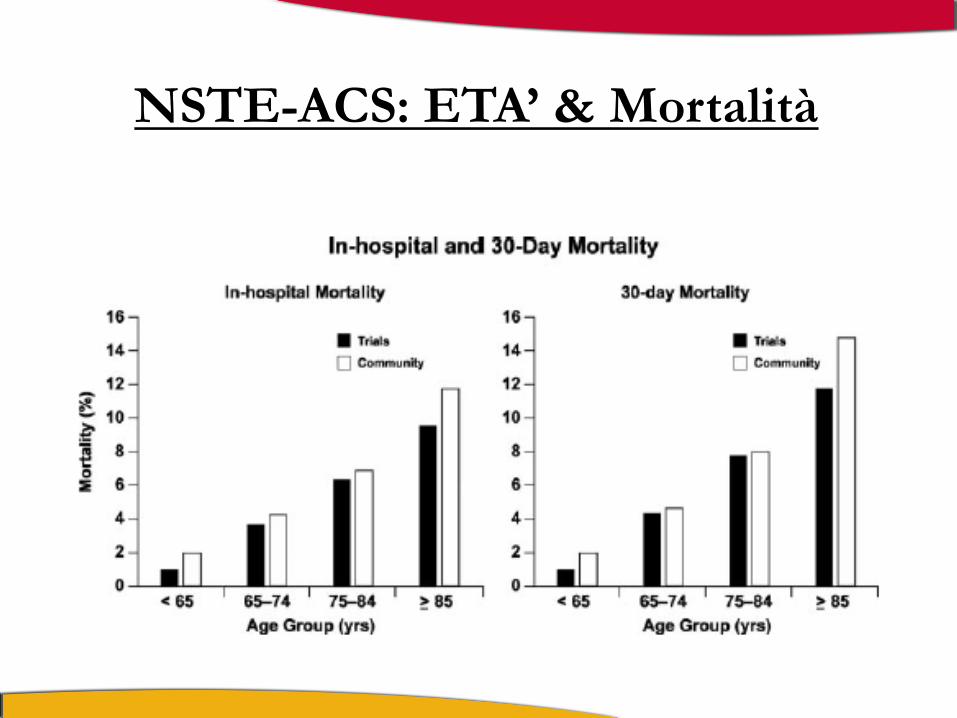
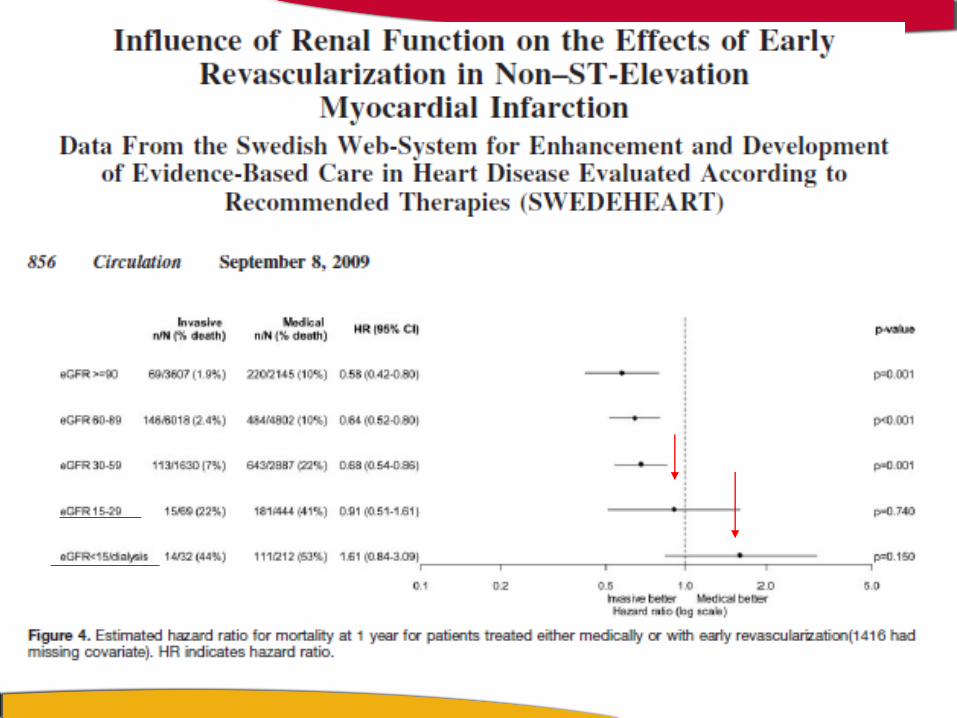
NSTE-ACS: ETA’ & Mortalità
VIGOUR trial and GRACE
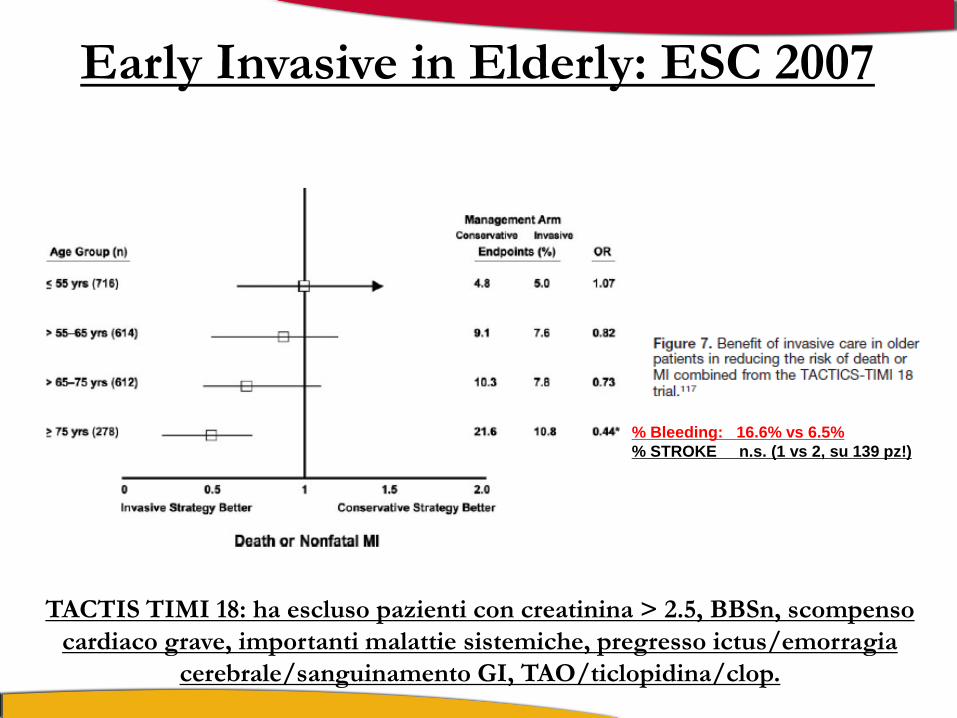
Early Invasive in Elderly: ESC 2007
TACTIS TIMI 18: ha escluso pazienti con creatinina > 2.5, BBSn, scompenso
cardiaco grave, importanti malattie sistemiche, pregresso ictus/emorragia
cerebrale/sanguinamento GI, TAO/ticlopidina/clop.
% Bleeding: 16.6% vs 6.5%
% STROKE n.s. (1 vs 2, su 139 pz!)
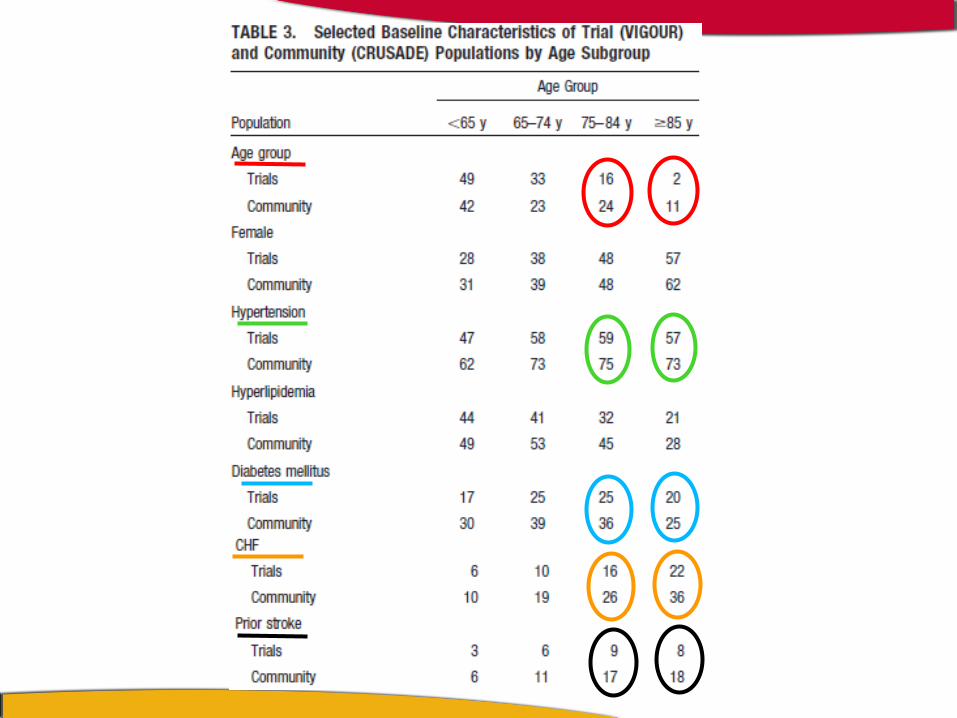
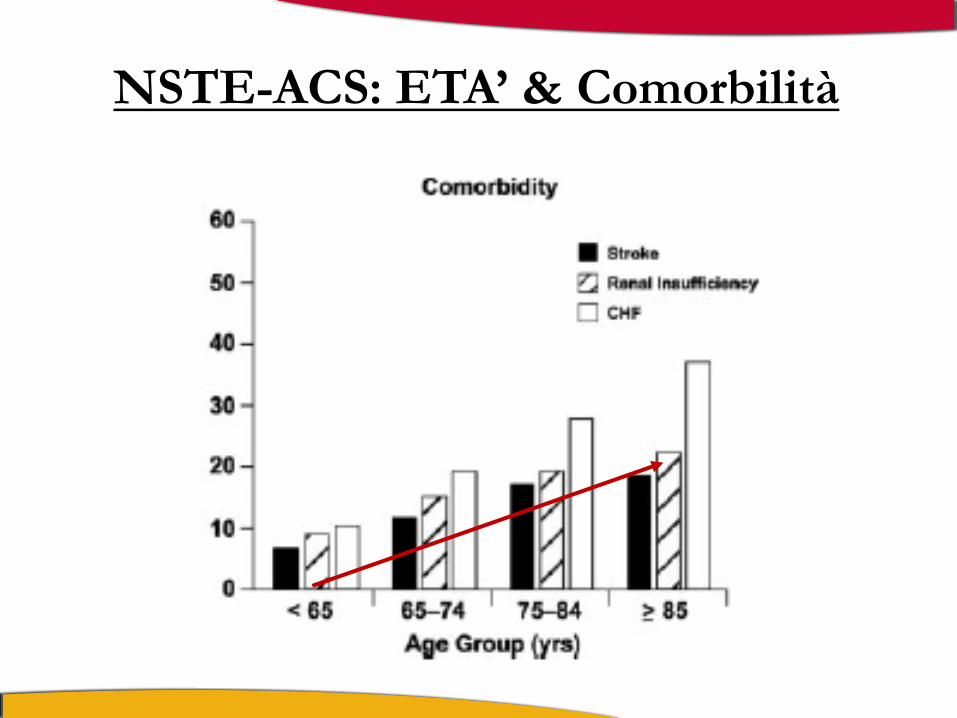
NSTE-ACS: ETA’ & Comorbilità
CRUSADE registry
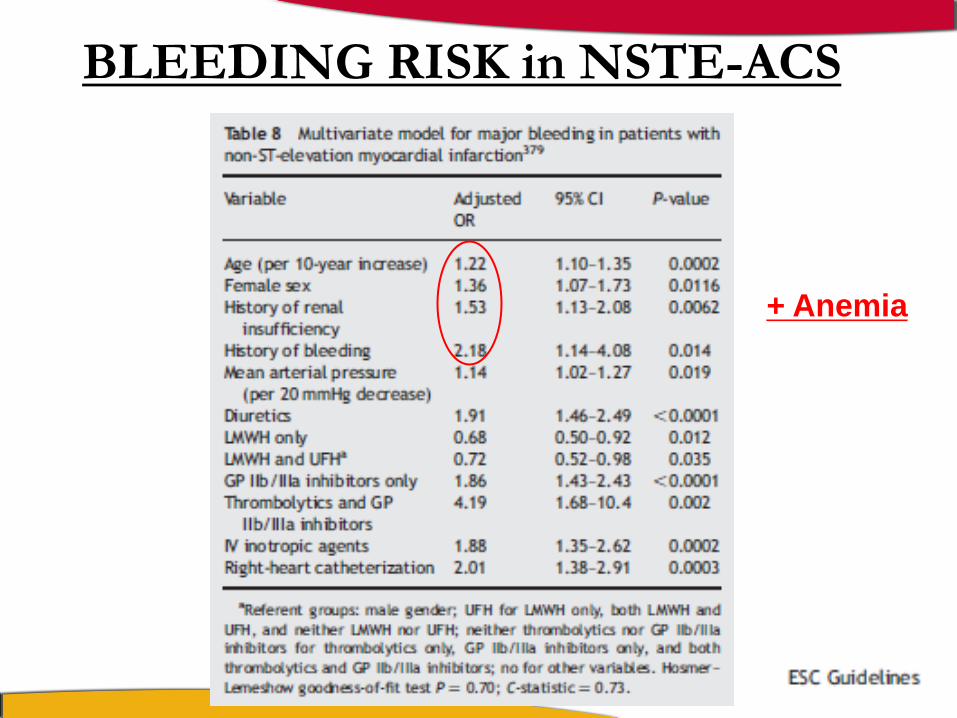
BLEEDING RISK in NSTE-ACS
+ Anemia


La Finestra Terapeutica dell’Anziano
FT: intervallo di sicurezza tra la dose efficace minima di un farmaco e la
sua concentrazione tossica minima.
Anziani
Prasugrel: analisi dei sottogruppi per età del TRITON-TIMI38, ha evidenziato nei pz > 75aa un incremento delle emorragie con perdita del beneficio clinico
Ticagrelor: Studio Elderly (2012)
Husted S, et al. Circ Cardiovasc Qual Outcomes 2012;5:680–688.

PLATO elderly patient subgroup analysis:
demographics, treatment and procedures
• Of the 18,622 patients in the PLATO study for whom age data was available,
2878 (15.5%) were elderly [Husted 2011:B]
- Elderly patients were defined as being aged ≥75 years old
• Several notable differences were observed in the elderly subgroup compared
with the younger patient subgroup[Husted 2011:C]
- Greater proportion of women
- Lower body weight
- Increased prevalence of CV risk factors and renal disease
- More likely to have a history of prior ischaemic CV events or CV disease
- Reduced glomerular filtration rate
- Elderly patients were less likely to present with STEMI[Husted 2011:C]
• Initial treatment plans for elderly patients were less likely to involve an invasive
strategy[Husted 2011:C,D]
ACS, acute coronary syndromes; CV, cardiovascular; STEMI, ST-segment elevation myocardial infarction. Husted S, et al. J Am Coll Cardiol 2011;57:E1099.

PLATO elderly subgroup: 2878 pts (15.5%) Caratteristiche demografiche e cliniche
Husted S et al . JACC 2011; 57: E 1099
> 75 aa < 75 aa p
§
§

25 35 45 55 65 75 85 95
PLATO elderly patient subgroup analysis: Primary composite endpoint according to age
Husted S, et al. J Am Coll Cardiol 2011;57:E1099; Wallentin L, et al. N Engl J Med 2009;361:1045–1057
Age (years)
CV
death
, M
I o
r str
oke (
%)
35
30
25
20
15
10
5
0
Ticagrelor Clopidogrel
Primary endpoint benefit with ticagrelor was consistent with the overall PLATO trial results
[Husted 2011:H; Wallentin 2009:H]
No interaction between age and treatment was observed [Husted 2011:I]
p for interaction = 0.2163
CV, cardiovascular; MI, myocardial infarction.

PLATO elderly patient subgroup analysis:
Association of age with bleeding
Events, n
Age <75
years old, %
(n=15,744)
Age ≥75
years old, %
(n=2878)
HR (95% CI)
Safety endpoints
Major bleeding
Fatal bleeding
Life-threatening/fatal bleed
Non-CABG-related major bleeding
CABG-related major bleeding
1886
43
968
665
1272
11.0
0.2
5.6
3.5
7.8
13.8
0.8
7.1
7.7
6.7
Age ≥75 years better Age ≥75 years worse
CABG, coronary artery bypass graft; CI, confidence interval; HR, hazard ratio.
0.5 1.0 2.0 7.0 1.5 3.0
Elderly patients have a greater risk of non-CABG-related major bleeding and fatal bleeding compared with younger patients[Husted 2011:I]
Husted S, et al. J Am Coll Cardiol 2011;57:E1099

PLATO elderly patient subgroup analysis: Major bleeding according to age
Ticagrelor Clopidogrel
Majo
r b
lee
din
g (
%)
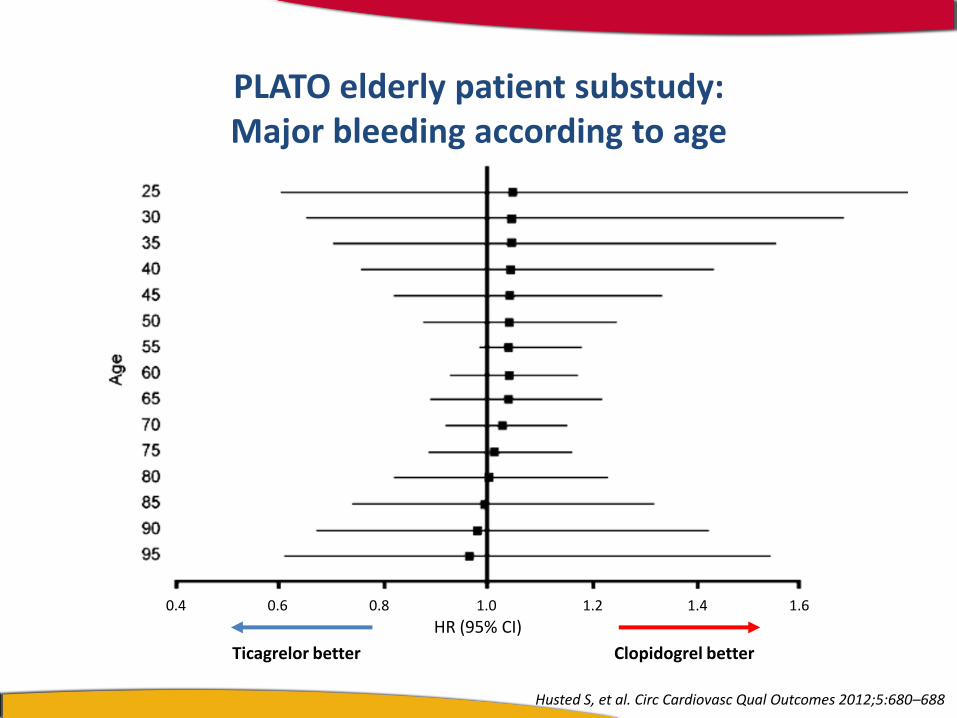
Major bleeding occurred with similar frequency in the ticagrelor and clopidogrel groups as observed in the overall PLATO population [Wallentin 2009:I; Husted 2011:L]
No interaction between age and treatment was observed [Husted 2011:L]
25
20
15
10
5
0
25 35 45 55 65 75 85 95
p for interaction = 0.9971
Age (years)
Husted S, et al. J Am Coll Cardiol 2011;57:E1099

• In elderly ACS patients, the benefits of ticagrelor over clopidogrel
were consistent with the overall PLATO study[Husted 2011:M]
• The efficacy of ticagrelor compared with clopidogrel was independent
of age[Husted 2011:M]
- Primary composite endpoint of CV death, MI or stroke was lower
with ticagrelor compared with clopidogrel, irrespective of age
- All-cause mortality, CV death, MI and definite stent thrombosis
were reduced by ticagrelor compared with clopidogrel,
irrespective of age
• Major bleeding was similar in ticagrelor- and clopidogrel-treated
patients regardless of age[Husted 2011:M]
ACS, acute coronary syndromes; CV, cardiovascular; MI, myocardial infarction; Husted S, et al. J Am Coll Cardiol 2011;57:E1099.
Summary of the PLATO elderly patient subgroup analysis
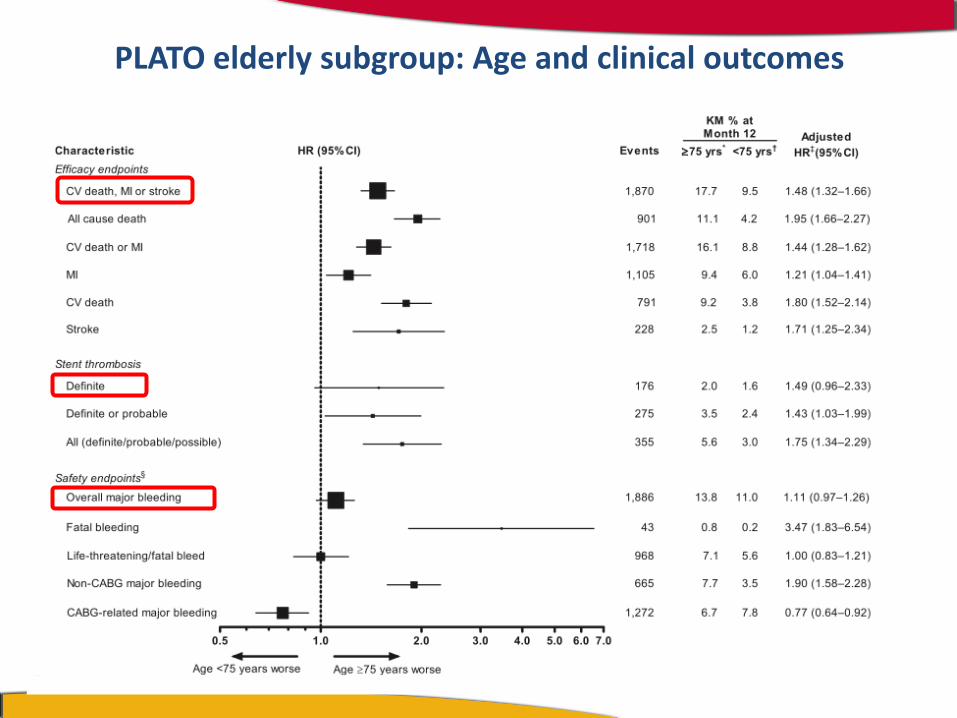
PLATO elderly subgroup: Age and clinical outcomes
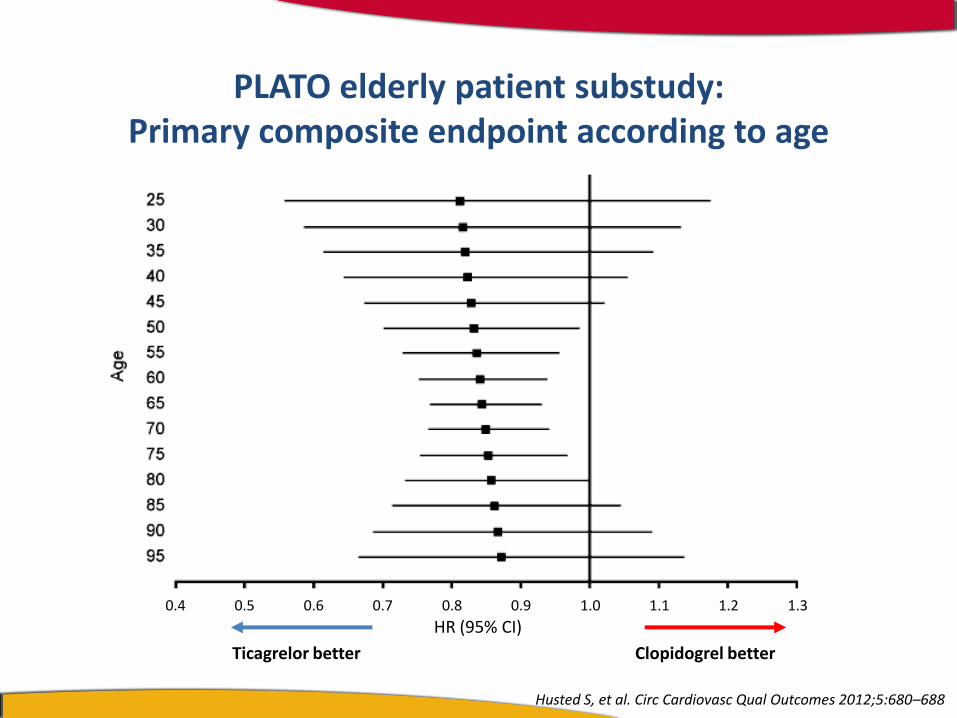
Ticagrelor better Clopidogrel better
Husted S, et al. Circ Cardiovasc Qual Outcomes 2012;5:680–688
PLATO elderly patient substudy: Primary composite endpoint according to age
1.3 1.2 1.0 1.1 0.8 0.6 0.4
HR (95% CI) 0.5 0.7 0.9
1.6 1.4 1.2 1.0 0.8 0.6 0.4
Ticagrelor better Clopidogrel better
Husted S, et al. Circ Cardiovasc Qual Outcomes 2012;5:680–688
HR (95% CI)
PLATO elderly patient substudy: Major bleeding according to age
Anziani
Ticagrelor, in base allo studio Elderly
ottiene, anche nei pazienti oltre i 75aa, un vantaggio rispetto al clopidogrel in termini di - end-point combinato - mortalità totale senza incremento dei sanguinamenti maggiori


17.3%
22.0%
Renal function and outcomes in PLATO:
Primary composite endpoint
James S, et al. Circulation 2010;122:1056–1067; Wallentin L, et al. N Engl J Med 2009;361:1045–1057
Days after randomisation
Normal renal function Ticagrelor Clopidogrel HR (95% CI) = 0.90(0.79–1.02)
7.9% 8.9%
0 60 120 180 240 300 360
25
20
15
10
5
0
CV
de
ath
, MI
or
stro
ke (
%)
CKD Ticagrelor Clopidogrel HR (95% CI) = 0.77(0.65–0.90)
p for interaction = 0.13
L’efficacia del ticagrelor sull’EP primario è confermata nei pz con IRC
Non vi sono interazioni tra funzione renale e terapia (p=0.13)

James S, et al. Circulation 2010;122:1056–1067
End-point primario di efficacia in funzione della
funzionalità renale (CrCl)
Ticagrelor better
Clopidogrel better
Risk of CV death, stroke or MI HR (95% CI)
30
40
50
60
70
80
90
100
CrCl (mL/min)
0.5 0.6 0.7 0.8 0.9 1.0 1.1 1.2 0.4
Incr
easi
ng
ren
al im
pai
rmen
t
Non vi sono interazioni tra funzione renale e terapia (p=0.13)

p for interaction = 0.92
Sanguinamenti e funzionalità renale nel Plato
15.1% 14.3%
Non-CABG TIMI bleeding’ et al. James S et al - Circulation 2010;122:1056–1067
Days after randomisation
0 60 120 180 240 300 360
Maj
or
ble
ed
ing
(%)
25
20
15
10
5
0
CKD Ticagrelor Clopidogrel HR (95% CI) = 1.07 (0.88–1.30)
Normal renal function Ticagrelor Clopidogrel HR (95% CI) = 1.08 (0.96–1.22)
9.8%
10.6%
La frequenza di sanguinamenti è simile nei 2 gruppi ticagrelor e clopidogrel

• Il ticagrelor è un antiaggregante più efficace rispetto al clopidogrel nelle SCA
• indipendentemente dalla funzionalità renale
• con un beneficio maggiore nei pz con funzionalità renale compromessa
• senza necessità di ridurre il dosaggio per prevenire sanguinamenti maggiori.
• Non sono però disponibili informazioni riguardo ai pazienti in trattamento dialitico.
Ticagrelor ed insufficienza renale nelle SCA


CONCLUSIONI Nel paziente anziano con SCA, la insufficienza renale è sempre
importante, anche se lieve: calcolare il GFR!
In assenza pazienti anziani, con grave insufficienza renale e SCA, la
gestione clinica è individualizzata (rischio/beneficio). Questi pazienti
non rappresentano una importante percentuale degli anziani ricoverati
per SCA, ed hanno una mortalità estremamente elevata, a prescindere
dal tipo di trattamento.
Prima di un trattamento invasivo, oltre alle comorbilità, si deve
sempre tenere conto delle condizioni geriatriche (autonomia, qualità
di vita, decadimento cognitivo), della volontà e della spettanza di vita
del paziente.

34


















