Igo Goldberg M.D, Hand Surgeon Tel-Aviv, Israel Clinical Examination of the Wrist.
48
Igo Goldberg M.D, Hand Surgeon Tel-Aviv, Israel Clinical Examination of the Wrist
-
Upload
ryan-tremelling -
Category
Documents
-
view
228 -
download
4
Transcript of Igo Goldberg M.D, Hand Surgeon Tel-Aviv, Israel Clinical Examination of the Wrist.

Igo Goldberg M.D, Hand Surgeon
Tel-Aviv, Israel
Clinical Examination of the Wrist

MOST COMMON CAUSES OF WRIST PAIN - 1
Traumatic
Disorders
Fracture and Malunion
Radius-ulna
Scaphoid
Other carpal bones
Nonunion
Scaphoid
Capitate
Hamate
Chondritis/Osteochondritis/
Posttraumatic arthritis
SNAC
SLAC
Piso-triquetral arthrosis
Hamate-triquetral arthrosis
Hyperextension radioscaphoid impingement
(Gymnast’s wrist)
Ulno-carpal impingement
Ligamentous Injuries and Instability
Perilunate (scapholunate,lunotriquetral)
Midcarpal (intrinsic,extrinsic)
Radiocarpal (ventral or dorsal subluxation,ulnar translocation)
Dorsal wrist syndrome
Distal radioulnar joint (luxation,subluxation,TFCC injury)
Carpo-metacarpal j (1st CMC;2nd-3rd CMC;carpal boss;4th-5th CMC)
Extensor Carpi Ulnaris Tendon Subluxation
Degenerative
Inflammatory
Disease
Connective Tissue Diseases
Rheumatoid arthritis
Systematic lupus erythematosus
Metabolic diseases
Gout /pseudogout
Hyperparathyroidism
Chondrocalcinosis
Tendonitis
Tenosynovitis
Repetitive Strain Injury
Chondritis/
Primary Arthrosis

MOST COMMON CAUSES OF WRIST PAIN - 2
Infective
Disorders
Common Bacterial/Atypical AgentSpecific Granulomatous Disease
Neoplastic
Disorders
Ganglia
(extraosseous/
Intraosseous/occult)
Tendon Cysts
Bone Tumors
Enchondroma,
Osteoid osteoma,
Chondromatosis,etc.
Soft Tissue Tumors
Pigmented villonodular synovitis,
Giant cell tumor,etc
Malignant
Tumors
Congenital and Developmental Disorders
Simple Osseous CystMadelung’s deformityMuscular Anomalies
Extensor brevis manus
Carpal Coalition
Scapholunate
Scaphotrapezial
Lunotriquetral
Neurological Disorders
Traumatic
Palmar branch median n. (from section)
Sens.branch radial n. (from injection)
Dorsal sens.branch ulnar n. (direct contusion)
Distal post.interosseous n. (recurrent ganglion)
Compressive
Carpal tunnel syndrome (CTS)
Wartenberg’s syndrome
Guyon’s syndrome
T.O.S
Radicular compression
Vascular Disorders
Aneurysm/thrombosis of the ulnar artery
Avascular necrosis of the lunate (Kienbock’s disease) ; of the scaphoid (Preiser’s disease) ;
Of the capitate; of the triquetrum

What constitutes the first part of every thorough physical examination?
A thorough history

STEPS IN TAKING A PATIENT HISTORY

CLINICAL EXAMINATION
• ROM active, passive• Grip - Jamar dynamometer (flat curve, rapid exchange grip strength,
coefficient of variation) • Pinch - Pinchmeter • Circumference measurements• (Volumetric measurements)• Palpation• Provocative tests• Anaesthetic examination• DASH Questionnaire• Mayo evaluation score

RANGE OF MOTION (ROM)
“The wrist is a key joint of the hand” – Starling Bunnel
Wrist movement occurs around three principal functional axes: yet all of them are complex and are not restricted to a fixed geometric axis.
• Flexion-Extension : transverse axis, sagital plane
• Radial-Ulnar deviation: sagital axis, coronal (frontal) plane
• Pronation-Supination : longitudinal axis, horizontal plane
What is their relative contribution to the upper extremity (UE) function?

WRIST MOTION IMPAIRMENT - 1
The wrist functional unit represents 60% of the upper extremity (UE) function.
Flexion-Extension unit: 70% of wrist function:70%x60%=42% of UE function.
Radial-Ulnar deviation unit: 30% of wrist function: 30%x60%=18% of UE function
ההטיות חשיבות גדולה יותר מאשר לשמירה על טווח כיפוף-ישור לשמירה על טווחלצדדים
Normal ROM 60-60 F-E
Functional ROM: 10-10 F-E
Normal ROM 20-30 R-U
Functional ROM: 0-10 R-U
Wrist fusion:
10 extension
10 ulnar deviation

WRIST MOTION IMPAIRMENT - 2
Pronation-Supination
Impairments of pronation-supination are ascribed to the elbow because the major muscles for this function are inserted about the elbow. This applies even if the loss of rotation results primarily from the wrist involvement in the presence of an intact elbow
The relative value of this motion unit
is 28% of the UE function Normal ROM : 80-80 P-S
Functional position: 20 P

WRIST MOTION IMPAIRMENT - 3
The relative contribution of various motion units to the upper extremity (UE) function:
• F-E 42%• P-S 28%• R-U 18%

How much wrist motion is required for most activities of daily living (ADL) ?
PALMER (1985)Ruy (1991)
Flexion50400
Extension300400
Radial deviation100100
Ulnar deviation150300

האם טווח התנועה בשורש היד חשוב בכל מחיר ?
תקנות המל"ל )(ב')[10(41]תקנה נכות20%"קשיון נוח" שורש יד -
)(ז')[10(41]תקנה נכות10% - קשיון ברוטציה של האמה במנח נוח )[2+3+4(44]תקנה נכות31%"קשיון נוח" של כל האצבעות (במצטבר)-
מסקנה:
תפקודן התקין של האצבעות חשוב יותר מתפקודו של שורש היד !!!!!!!
מה הם שני התפקידים העיקריים של היד ?
אחיזה (על כל צורותיה)1.
מגע2.

טופל עקב שבר ברדיוס רחיקני ע"י קיבוע חיצוני וגבס.40גבר בשנות ה-
תמונות רנטגן וטווחי תנועה בשורש יד "יפים...."
פרונציה סופינציה
כיפוף יישור

...............ויד פגועה קשה
................................?.

TOPOGRAPHIC ANATOMY OF THE WRIST
Radial border 1st comp
Ulnar
border FCR
Ulnar border FCU
radialcentralulnar
middle axis 4th finger
VOLAR

TOPOGRAPHIC ANATOMY OF THE WRIST
Dorsal
ulnarcentralradialRadial border
1st comp
Radial border
2nd comp
Ulnar border 4th comp
Ulnar border FCU

COMMON CAUSES OF WRIST PAIN ACCORDING TO TOPOGRAPHIC AREAS - 1

COMMON CAUSES OF WRIST PAIN ACCORDING TO TOPOGRAPHIC AREAS - 2
Volar areasDorsal areas
Radial Central Ulnar Radial Central Ulnar
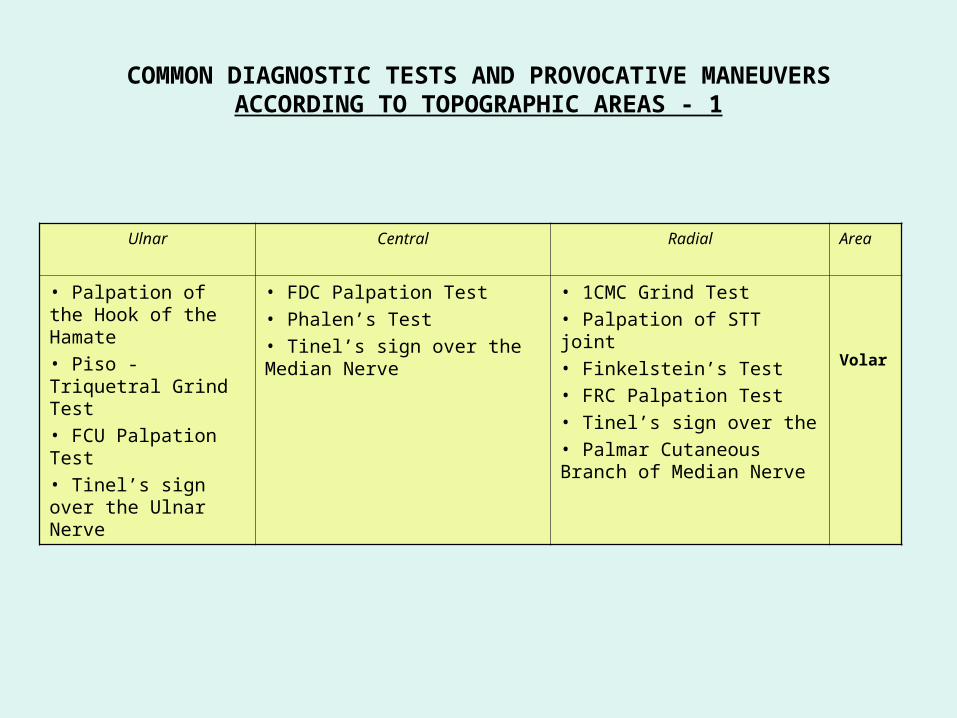
COMMON DIAGNOSTIC TESTS AND PROVOCATIVE MANEUVERS ACCORDING TO TOPOGRAPHIC AREAS - 1
AreaRadialCentralUlnar
Volar
• 1CMC Grind Test• Palpation of STT joint• Finkelstein’s Test• FRC Palpation Test• Tinel’s sign over the• Palmar Cutaneous Branch of Median Nerve
• FDC Palpation Test• Phalen’s Test• Tinel’s sign over the Median Nerve
• Palpation of the Hook of the Hamate• Piso -Triquetral Grind Test• FCU Palpation Test• Tinel’s sign over the Ulnar Nerve

COMMON DIAGNOSTIC TESTS AND PROVOCATIVE MANEUVERS ACCORDING TO TOPOGRAPHIC AREAS - 2
AreaRadialCentralUlnar
Dorsal
• 1 CMC Grind Test• 2-3 CMC Shear test• Palpation of Anatomic snuffbox/
Articular-Nonarticular test• Intersection Syndrome•Tinel’s sign over the sensory branch of Radial Nerve (Wartenberg’s Neuralgia)
• Finger Extension Test (FET)• Scaphoid shift (Watson’s) test• SL Shear Test• “Catch-up clunk” (Lichtman’s Test)• EPL Test• EIP Test• Radio-Carpal Subluxation Test• Palpation of Extensor Digitorum Brevis Manus
• LT Shear Test• Derby’s Method for LT dissociation• Ballottement Test• Triquetral Impingement Ligament Tear (TILT) test• Ulnar Snuff Box Compression test• Piano Key Test• Press Test• Ulno-Carpal impaction test• Ulnar styloid impaction test• EDM test• ECU Palpation Test• ECU Subluxation Provoc Test• Tinel’s sign over the Dorsal Branch of Ulnar Nerve

PROVOCATIVE TESTS
בדיקת הצד הרדיאלי של שורש הידא-
בדיקת הצד האולנרי של שורש הידב-
בדיקת המפרקים הרדיוקרפלים ג-ומידקרפלים
בדיקת המפרקים הקרפומטקרפליםד-
סיבות חוץ פרקיות לכאבים בשורש הידה-

א.בדיקת הצד הרדיאלי של שורש היד
1. Dorsal wrist (DWS) test
2. Finger extension (FET) test
3. Articular/nonarticular (ANA) test
4. Scaphotrapeziotrapezoid (STT) test
5. Scaphoid shift maneuver (SSM)
6. Ballotment test (shear) test for SL

1.Dorsal wrist (DWS) test
:S-Lלבדיקת פרק • This joint is not painful
to palpation.
If painful, suspect: S-L dissociation Kienbock’s disease Dorsal wrist syndrome
(S-L joint overloading with wrist pain secondary to S-L ligament synovitis and/or tear preceding evidence of rotary subluxation of the scaphoid)
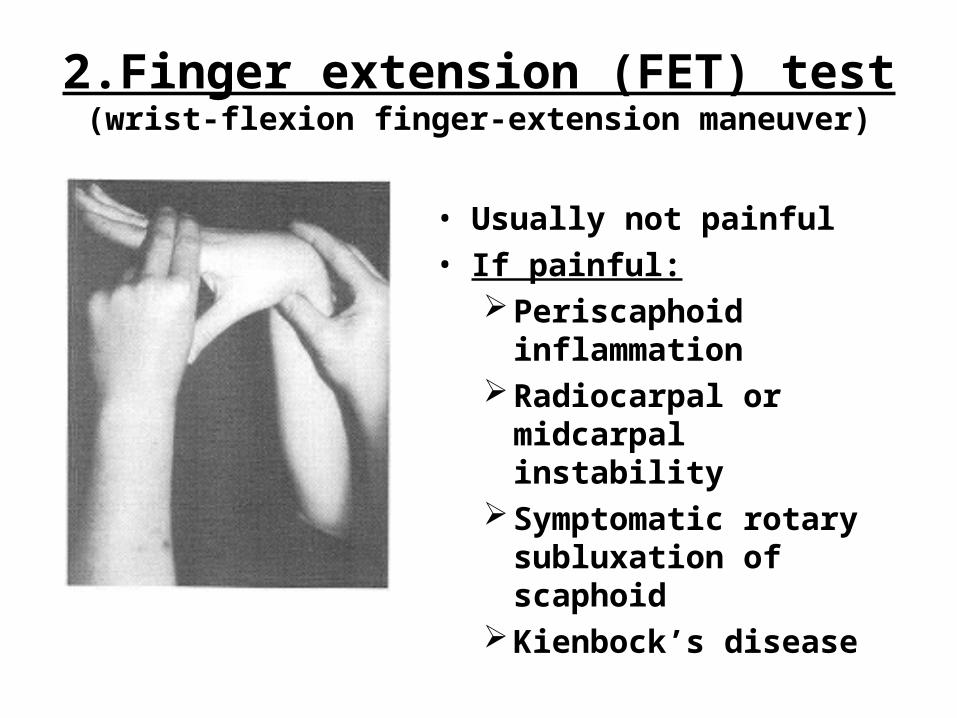
2.Finger extension (FET) test(wrist-flexion finger-extension maneuver)
• Usually not painful• If painful:
Periscaphoid inflammation
Radiocarpal or midcarpal instability
Symptomatic rotary subluxation of scaphoid
Kienbock’s disease

3.Articular/nonarticular (ANA) test.
• Always compare to the other side
• If severe pain:Periscaphoid
synovitisScaphoid instabilitySLAC changes

4.Scaphotrapeziotrapezoid (STT) test
• Palpation of this joint is not painful
• If painful, suspect:Triscaphe synovitisTriscaphe OA

5.Scaphoid shift maneuver (SSM)(Watson test, scaphoid shear test)
• If painful: rotary subluxation, periscaphoid arthritis

6 .S- L shear test
Pressure on the scaphoid tubercle Pressure on dorsal aspect of the lunate
Simultaneous pressure in opposite directions

7.Scapholunate ballottement test

ב.בדיקת הצד האולנרי של שורש היד
Areas involved:
1. DRUJ
2. TFCC
3. Ulnar carpus

1.DRUJ
Decreased and/or painful pronosupination:Degenerative diseaseSubluxation
“Piano key” sign: exaggeration of normal ulna head prominance.
Dorsal subluxationArticular effusion

Ulnar impingement or impaction syndrome
Decreased and/or painful pronosupination while ulnar head is pressed volarward and the pisiformis pressed dorsally

2.TFCC
Suspected when: Loss of forearm prosupination and wrist motion Tenderness over TFCC dorsally Palpable and/or audible click with forearm rotation
or radioulnar deviation (Ulnar carpal abutment test)
Necessitates: Three compartment arthrography

3.ULNAR CARPUS
LT compression test: direct pressure along ulnoradial axis by palpating within the ulnar snuffbox. (Linscheid’s test)
If painful:LT instabilitySynovitisDegenerative diseasePartial synchondrosis

LT instability: Reagan’s test(L-T ballottement, shuck, shear)
Pressure on the lunate
Pressure on the triquetrum

LT instability: Masquelet’s test

LT instability: Masquelet’s test
Pressure on pisiformis Pressure on dorsal aspect of the lunate
Simultaneous pressure in opposite directions

TH instability test
1. Grasping of the triquetrum2. Stabilization of capitate and carpus with other
hand3. Volar and dorsal stressing of the triquetrum

TILT: Triquetral Impingement Ligament Tear syndrome
Triad of:Localized triquetral pain History of hyperflexion injuryNormal radiographs
Mechanism: cuff of fibrous tissue that has become detached from the ulnar sling mechanism and chronically impinges on the triquetrum, resulting in synovitis, bony eburnation and pain.

ג.בדיקת המפרקים הרדיוקרפלים ומידקרפלים
Radiocarpal anteroposterior drawer test

The “pivot shift” of the mid-carpal joint
עם אמה בסופינציה מלאה90מרפק מכופף ל- 1.
אחיזה יציבה של האמה2.
הטיה רדיאלית מקסימלית של שורש היד3.
סופינציה נוספת לכף היד ללא תנועה בשורש היד4.
העברת היד מהטיה רדיאלית לאולנרית5.

The “pivot shift” of the mid-carpal joint
הסבר
במנח שתואר לעיל ראש הקפיטטום "ננעל" בלונטום והמטום "ננעל" בטריקווטרום.
העצמות הנ"ל אינן יכולות לנוע יותר וולרית משום שהן נעצרות ע"י קפסולה
.LTקידמית ורצועה
במידה וקיים קרע ברצועות הנ"ל (או רפיון מולד) הקפיטטום "יוצא" מתוך
הלונטום ובזמן העברת היד מהטיה רדיאלית להטיה אולנרית, השורה הרחיקנית
"קופצת" בחזרה למקומה מלווה בנקישה מכאיבה.

ג.בדיקת המפרקים הרדיוקרפלים ומידקרפלים
Midcarpal anteroposterior drawer test
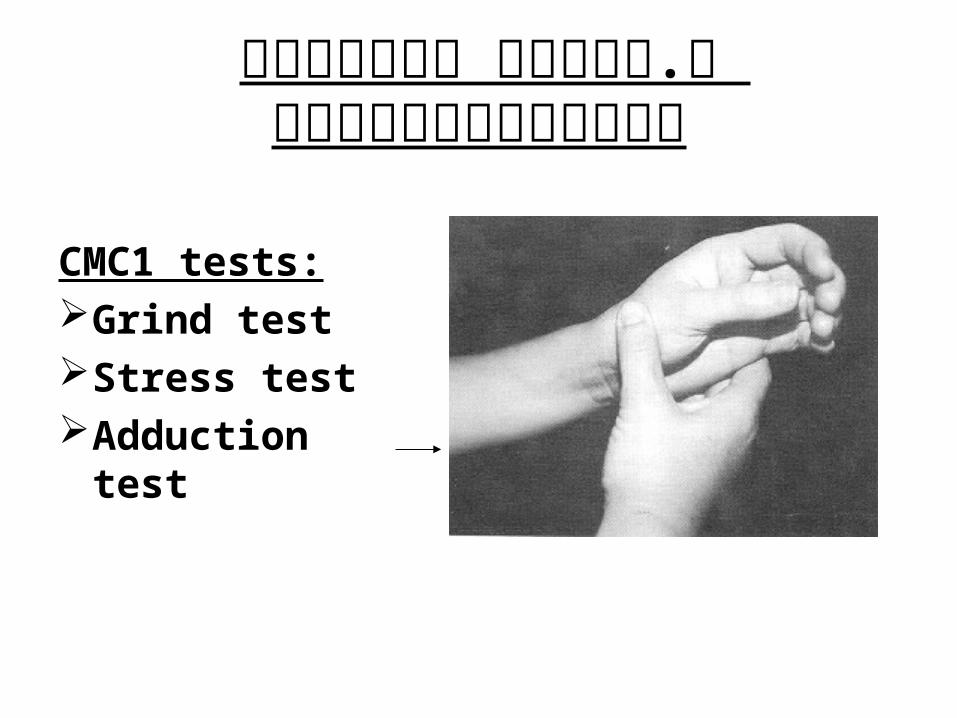
ד.בדיקת המפרקים הקרפומטקרפלים
CMC1 tests:Grind testStress testAdduction test

Carpal boss

ה.סיבות חוץ פרקיות לכאבים בשורש היד
• Finkelstein’s test• “Wet leather” sign• ECU problems: synovitis, subluxation,
stenosis, partial rupture• Pisiformis problems: fractures, OA• Hook of hamate• FCR tendinitis• intersection syndrome• Substitution maneuvers

COMMON DIAGNOSTIC TESTS AND PROVOCATIVE MANEUVERS
List of publications and suggested readings
www.goldberg-hand.co.il
for download in:

Thank you!