
IGNITE! Building Blocks of Quality Improvement part 2
29
A Virtual Ward • Common purpose • Common route/referral pathway • Communication ‘hard wired’ • Co-location • Cross cover of roles • Coordination of roles
-
Upload
innovation-agency -
Category
Healthcare
-
view
216 -
download
0
Transcript of IGNITE! Building Blocks of Quality Improvement part 2

A Virtual Ward
• Common purpose• Common route/referral pathway• Communication ‘hard wired’• Co-location• Cross cover of roles• Coordination of roles

QI
Leaders
Improvement Advisors
“Coaches”
All Staff
“Dosing Formula”
WTE dedicated Improvement
0.05% > 50% WTE
0.5% 10-50% WTE
5% 5-10% WTE
50% 1-5% WTE
Level Training
Strategic/ Expert
+1 year
Advanced Months -Year
Intermediate Weeks -Month
Basic Hours -Days
CAPACITY CAPABILITYIn
stitute
/ QIS
Fro
nt
line


“Stop THINKING outside the box, start GOING outside the box…”

Without this we won’t have the right values to continually improve
Learning System
Essentials
Person & Family
Centered Care
Learning System Essentials
Cultural & Infrastructure
Essentials

Without this we won’t have the right values to continually improve
Comprehensive ‘capture’ process: Issues, events & feedback
System diagnostics across the continuum
Model for Improvement active at the
frontline
Real time transparent
measurement & understanding of
variability
Learning System
Essentials
Person & Family
Centered Care
Learning System Essentials
Cultural & Infrastructure
Essentials

Organisation
Division
Ward
System diagnostics across the continuum

System diagnostics across the continuum
What is actually
going on in your
system?

System diagnostics across the continuum
Current“5 why’s”
Future

System diagnostics across the continuum
Aim
Measures
Change Concepts

System diagnostics across the continuum
From “Trial and error” to “Trial and learn”

System diagnostics across the continuum

System diagnostics across the continuum
Chile School Register
Ward Outcomes
Children receiving bedtime story

System diagnostics across the continuum
URGENT CARE TEAM DASHBOARD
15
20
25
30
35
Apr-
13
Jun-1
3A
ug-1
3O
ct-13
Dec-
13F
eb-1
4A
pr-
14
Jun-1
4A
ug-1
4O
ct-14
Dec-
14F
eb-1
5A
pr-
15
Jun-1
5A
ug-1
5O
ct-15
Dec-
15F
eb-1
6A
pr-
16
Jun-1
6A
ug-1
6Unplanned Admissions / 1000 population
(>64y) (O#1)
Num
ber/
month
Month
Num
ber/
month
25
27
29
31
33
35
37
39
41
43
45
Apr-
13
Jun-1
3A
ug-1
3O
ct-13
Dec-
13F
eb-1
4A
pr-
14
Jun-1
4A
ug-1
4O
ct-14
Dec-
14F
eb-1
5A
pr-
15
Jun-1
5A
ug-1
5O
ct-15
Dec-
15F
eb-1
6A
pr-
16
Jun-1
6A
ug-1
6
Type 1 A&E attendances / 1000 population (>64y) (O#2)
Month
0
20
40
60
80
100
120
140
Apr-
14
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
Oct-16
Dec-
16
NWAS cat green conveyances from care homes (O#3)
Conveyances p
er m
onth
Month
5
6
6
7
7
8
8
9
9
10
10
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
Patient & Family Experience Score (O#4)
Score
out of 10
Month
0
10
20
30
40
50
60
70
80
90
100
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
Mean response time (mins) (P#2)
Min
ute
s
Month
0
2
4
6
8
10
12
14
16
18
20
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
Number conversions to acute trust - % on graph (P#3)
Month
%
0
20
40
60
80
100
120
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
Average LOS under UCT team (P#4)
Month
Hours
0
20
40
60
80
100
120
140
160
180
200
Jul-14
Sep-1
4
Nov-
14
Jan-1
5
Mar-
15
May-
15
Jul-15
Sep-1
5
Nov-
15
Jan-1
6
Mar-
16
May-
16
Jul-16
CICT new referrals (B#1)
Num
ber/
month
Month
Num
ber/
month
0
10
20
30
40
50
60
70
80
90
100
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
CICT 95% Centile LOS (B#2)
Days
Month
0
5
10
15
20
25
30
35
40
45
50
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
Referral Source (P#6)
Month
Num
ber
per
0
20
40
60
80
100
120
140
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
New patients seen (activity) (P#1)
Month
New
patie
nts
seen
0
2
4
6
8
10
12
14
16
18
20
Jun-1
4
Aug-1
4
Oct-14
Dec-
14
Feb
-15
Apr-
15
Jun-1
5
Aug-1
5
Oct-15
Dec-
15
Feb
-16
Apr-
16
Jun-1
6
Aug-1
6
Potential & Actual Safety Events [DATIX] (P#5)
Month
Num
ber
per m
onth

Comprehensive ‘capture’ process: Issues, events & feedback
System diagnostics across the continuum
Model for Improvement active at the
frontline
Real time transparent
measurement & understanding of
variability
Learning System Actions
DEMOSTRATE
DELIVER
DO
DEVELOP
DIAGNOSE
DISCOVER

Cycle time
Comprehensive ‘capture’ process: Issues, events & feedback
System diagnostics across the continuum
Model for Improvement active at the
frontline
Real time transparent
measurement & understanding of
variability
Learning System Effectiveness
Proximity to the frontline
Alignment to strategic objectives

Without this we won’t have the right values to continually improve
Family as a unit of care
Partnership in personalizedcare
From “what’s the matter?” to “what matters to me”
System co-designRepresentationCollective Voice
Valued workforce & psychological safety
Compassionate leadership with relentless focus
who connect with the ‘front
line’
Functional ‘Team’ ethos incl. clinical &
informatics integration
Increasing staff capacity
& capability in QI & innovation
Comprehensive ‘capture’ process: Issues, events & feedback
System diagnostics across the continuum
Model for Improvement active at the
frontline
Real time transparent
measurement & understanding of
variability
Cultural & Infrastructure
Essentials
Learning System
Essentials
Person & Family
Centered Care
© Dr Peter Chamberlain

Without this we won’t have the right values to continually improve
Family as a unit of care
Partnership in personalizedcare
From “what’s the matter?” to “what matters to me”
System co-designRepresentationCollective Voice
Valued workforce & psychological safety
Compassionate leadership with relentless focus
who connect with the ‘front
line’
Functional ‘Team’ ethos incl. clinical &
informatics integration
Increasing staff capacity
& capability in QI & innovation
Comprehensive ‘capture’ process: Issues, events & feedback
System diagnostics across the continuum
Model for Improvement active at the
frontline
Real time transparent
measurement & understanding of
variability
Cultural & Infrastructure
Essentials
Learning System
Essentials
Person & Family
Centered Care
© Dr Peter Chamberlain
Deming’s “System of Profound Knowledge”
S
K P
V

Without this we won’t have the right values to continually improve
Family as a unit of care
Partnership in personalizedcare
From “what’s the matter?” to “what matters to me”
System co-designRepresentationCollective Voice
Valued workforce & psychological safety
Compassionate leadership with relentless focus
who connect with the ‘front
line’
Functional ‘Team’ ethos incl. clinical &
informatics integration
Increasing staff capacity
& capability in QI & innovation
Cultural & Infrastructure
Essentials
Learning System
Essentials
Person & Family
Centered Care
© Dr Peter Chamberlain
Without this we won’t have the mechanisms to sustain continuous improvement

Without this we won’t have the right values to continually improve
Family as a unit of care
Partnership in personalizedcare
From “what’s the matter?” to “what matters to me”
System co-designRepresentationCollective Voice
Cultural & Infrastructure
Essentials
Learning System
Essentials
Person & Family
Centered Care
© Dr Peter Chamberlain
Without this we won’t have the mechanisms to sustain continuous improvement
Without this we won’t have the foundationsto support continuous improvement

Cultural & Infrastructure
Essentials
Learning System
Essentials
Person & Family
Centered Care
© Dr Peter Chamberlain
Without this we won’t have the mechanisms to sustain continuous improvement
Without this we won’t have the foundationsto support continuous improvement
Without this we won’t have the principlesto direct continuous improvement

“Going under the bonnet”
Where do we go from here?

QI Building blocks Framework
1 2 3 4 5Is coded data collected and collated automatically in real time ie. within one time unit of specified analysis (shorter time unit the better, maximum time unit 1 month)
Does data on projects/ work streams consistently cover a family of meaningful measures including outcome, process and balancing measures?
Is there a suite of system measures actively in place aligned to strategic objectives? Are these measures reported on time on a monthly basis?Is there evidence of the identification of improvement gaps and QI projects as a result?
Are projects and system measures data consistently presented in time series and routinely analysed using ratified statistical process control?
Are data summaries of live and current improvement work are made available throughout the organisation within publically facing areas either physically or electronically?
0-3 0-3 0-3 0-3 0-3

/60
/60
/60
-----180
0 Organisation has not started/ no progress1 Organisation has started / early progress2 Organisation has embedded / steady progress3 Organisation has fully met criteria across whole organisation
QI Building blocks Framework

Aims of QI Building Blocks Framework
DIALOGIC (jigsaw)
Help individuals and teams understand & assimilate key factors required for continuous quality improvement
DIAGNOSTIC (180 point framework)
Provide pragmatic guidance for organisations in operationalising their
quality strategy and achieving high performing organisational status

Inputs ActivitiesOutputs –
Knowledge & Strategy
Outputs –Operational Effectiveness
Outcomes — ImpactShort Term Medium Term Long Term
(1years) (2+years) (3+years)
• QIBBF dialogic & diagnostic
• AQuA commitment to QIBB concept
• Resources to support QIBB program
• Networking, coordination & promotion
• Academicexpertise
• Senior leadership involvement in learning and deployment
• Organizational & respect & interest to learn and apply
• Interest with people of influence
• Accessible and effective communication mechanisms
• Engagement with stakeholderorganisations online and workshops
• Testing & adaptation
• Supported learning platform including active peer involvement
• Accessible framework, guide and expert support
• Connection of framework to OD strategies
• Promotion of QIBB at different levels on different programs
• Formative evaluation
• Academicratification
• New knowledge applied to current thinking
• Individuals understanding key linkages between philosophy, foundations & mechanisms
• Reframing of organisational quality narrative & values
• Re-alignment of organisational development plans and priorities
• Prioritisation of staff skills and areas of focus
• Leader and staff training at respective levels
• Healthy and key Vision & Values embedded in ‘functional ‘DNA’’
• Redefined and new transformationprograms
• Changes to organisational procedures
• Capacity & capability embedded systematically
• Staff enthusiasm and motivation
• Revised measurement, quality and performance systems
• Improved intra and inter organisational relationships
• Assimilation of core QI methods, innovation, integration & leadership
• Alignment of organisational goals and frontline improvement
• Continuous improvement of systems and processes
• Improvement in staff satisfaction,joy at work & psychological safety
• Internal culture thriving and healthy
• Shift from organisational to system focus
• Evidence of change from patient feedback
• Partnership between public, patient and organisation
• Improvedefficiency of use of resource
• Improvement in mortality & safety metrics
• Reduced waiting times for services
• Equitable service
• Development of innovative treatment, pathways and services
• Demonstrable continuous improvement in care outcomes
• Improved staff retention & skill
• Improved financial balance
• Adoption of newest advances
• Improvement in patient reported experience measures
ORGANISATIONAL
Excellence in quality
High performing organisation recognition
Clear upward trajectory in resilience, responsiveness & reputation
Assumptions
Value of quality improvement methodology
Executive support & organisational commitment
Senior leadership capacity to implement
Resources for deployment
Mechanisms for improvement & deployment
External Factors
Activity vs quality agenda / contractual basis
Financial austerity
Political re-organisation
Change in senior leadership
Competing organisational priorities
QUALITY IMPROVEMENT BUILDING BLOCKS FRAMEWORK LOGIC MODEL v01

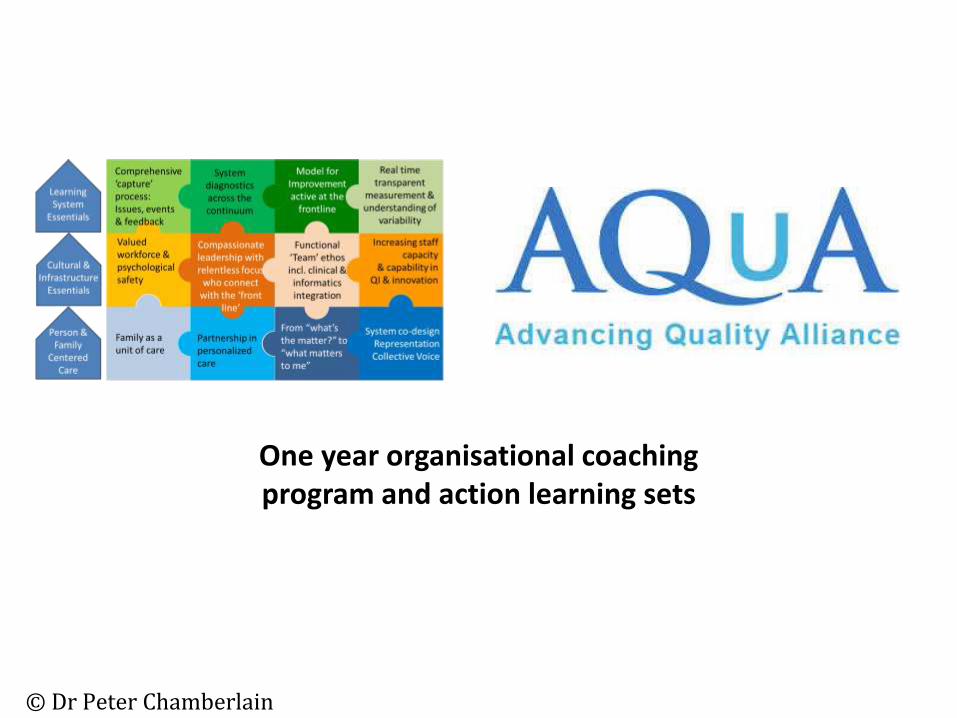
Without this we won’t have the right values to continually improve
Family as a unit of care
Partnership in personalizedcare
From “what’s the matter?” to “what matters to me”
System co-designRepresentationCollective Voice
Valued workforce & psychological safety
Compassionate leadership with relentless focus
who connect with the ‘front
line’
Functional ‘Team’ ethos incl. clinical &
informatics integration
Increasing staff capacity
& capability in QI & innovation
Comprehensive ‘capture’ process: Issues, events & feedback
System diagnostics across the continuum
Model for Improvement active at the
frontline
Real time transparent
measurement & understanding of
variability
Cultural & Infrastructure
Essentials
Learning System
Essentials
Person & Family
Centered Care
© Dr Peter Chamberlain

Without this we won’t have the right values to continually improve
Family as a unit of care
Partnership in personalizedcare
From “what’s the matter?” to “what matters to me”
System co-designRepresentationCollective Voice
Valued workforce & psychological safety
Compassionate leadership with relentless focus
who connect with the ‘front
line’
Functional ‘Team’ ethos incl. clinical &
informatics integration
Increasing staff capacity
& capability in QI & innovation
Comprehensive ‘capture’ process: Issues, events & feedback
System diagnostics across the continuum
Model for Improvement active at the
frontline
Real time transparent
measurement & understanding of
variability
Cultural & Infrastructure
Essentials
Learning System
Essentials
Person & Family
Centered Care
© Dr Peter Chamberlain
/
© Dr Peter Chamberlain
One year organisational coaching program and action learning sets


















