Identifying Optimal Diets for Glycemic Control during Pregnancy: A Network Meta-Analysis Vanessa Ha,...
23
Identifying Optimal Diets for Glycemic Control during Pregnancy: A Network Meta-Analysis Vanessa Ha, PhD Student Supervisors: Drs. Sonia Anand and Russell de Souza
-
Upload
baldwin-fletcher -
Category
Documents
-
view
212 -
download
0
Transcript of Identifying Optimal Diets for Glycemic Control during Pregnancy: A Network Meta-Analysis Vanessa Ha,...

Identifying Optimal Diets for Glycemic Control during Pregnancy:
A Network Meta-Analysis
Vanessa Ha, PhD Student
Supervisors: Drs. Sonia Anand and Russell de Souza

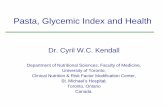
Complications of Gestational Diabetes Mellitus
High blood pressure&
pre-eclampsia
Type 2 diabetes
Mother
Child
Excessive Weight Gain
Pre-term Birth
HypoglycemiaType 2 diabetes
From: http://www.nlm.nih.gov & http://www.mayoclinic.org

Diet and Gestational Diabetes
Diet + Physical Activity
Thangaratinam et al. BMJ 2012;344:e2088
Energy Restrictive Diet (-30%)
Healthy & Energy Restrictive Diet
A Review of Food Intake

Dietary Guidelines
Energy intake for overweight or obese women may be restricted as long as the rate of weight gain is appropriate and provided ketosis is avoided [Grade D, Level 4].
It is generally recommended that total mixed carbohydrate comprise 40-45% of total energy or up to 50% of energy primarily from slowly released (low glycemic index) carbohydrate sources [Grade D, Level 4].
Accompanying a reduction in percentage of energy from carbohydrate, fat can comprise up to 40% of total energy intake during pregnancy [Grade D, Level 4]
For obese women (BMI 30 kg/m2), a 30 –33% calorie restriction (to 25 kcal/kg actual weight per day) has been shown to reduce hyperglycemia and plasma triglycerides with no increase in ketonuria (2). Restriction of carbohydrates to 35–40% of calories has been shown to decrease maternal glucose levels and improve maternal and fetal outcomes (3).
None for the Dietary Management of Glycemic Measures during Pregnancy

Dietary Guidelines
None for the Dietary Management of Glycemic Measures during Pregnancy
None for the Dietary Management of Glycemic Measures during Pregnancy
None for the Dietary Management of Glycemic Measures during Pregnancy
None for the Dietary Management of Glycemic Measures during Pregnancy

Objectives
To conduct a systematic review and network meta-analysis comparing the effects of various dietary patterns on glycaemic control (fasting blood glucose, fasting blood insulin, HbA1c, and HOMA-IR) in pregnant women.

CHOICE OF STUDY DESIGN:Traditional Pair-wise Meta-Analysis
vsNetwork Meta-Analysis

Pair-wise Meta-Analysis
Sievenpiper et al. Ann Int Med 2012; 156: 291.

Network Meta-Analysis
Extension of the pair-wise meta-analysis Multiple pair-wise comparisons are made by including both direct and
indirect evidence. To rank different treatment to assess which is the “best.”
Tianjing Li. Cochrane Comparing Multiple Interventions Methods GroupOxford Training event, March 2013.

Assumptions of Network Meta-Analysis
1. Homogeneity Measure of variance between studies Assumes that studies are “similar enough” to be pooled for analysis
2. Transitivity Assumes that one can make an indirect comparison between treatment
using a third treatment anchor Assumes that the distribution of effect modifiers between comparisons
are not systematically different
3. Consistency Degree of agreement between direct and indirect evidence If consistency holds, direct and indirect evidence can be pooled

STUDY METHODS

Literature Search
MEDLINE (up to July 6 2014)EMBASE (up to July 6 2014)
COCHRANE (up to July 8 2014)Manual search of references of included studies
Higgins JPT, Green S. Cochrane handbook for systematic reviews of interventions version 5.0.2 updated. The Cochrane Collaboration, 2009.
Reporting of results will follow the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. Hutton et al. Plos One 2014; 9 (3): e92508.
Protocol
Database

Search Term
Search Concept 1: Expectant Mothers
Search Concept 2: Diet/Nutrient Intake
Search Concept 3: Gestational Diabetes
MeSH Terms
- Pregnant Women- Prenatal Care- Maternal-Fetal Exchange
- Diet (exp)- Diet Therapy (exp)- Food - Food Habits- Food Quality- Nutritional Status
- Diabetes, Gestational (exp)- Blood Glucose- Hyperglycemia (exp)- Glucose Tolerance Test- Insulin Resistance (exp)- Hemoglobin A, Glycosylated - Fructosamine
Joint MeSH Terms
- Maternal Nutritional Physiological Phenomena (exp)
Text Words
- Pregnan*- Prenatal- Maternal- Expectant mother*
- Diet OR Diets OR Dietary- Food*- Nutrition*- Nutrient*
- Gestational diabetes- Blood glucose- Blood sugar- Glycaemic- Glycemic- Glycaemia- Glycemia- Hyperglycaemia*- Hyperglycemia*- Insulin- Glucose tolerance test- OGTT- Homostatic model assessment- HOMA-IR- Glycosylated haemoglobin*- Glycosylated hemoglobin*- Glycated haemoglobin*- Glycated hemoglobin*- HbA1c- Fructosamine- Impaired fasting glucose- Impaired glucose tolerance- Glucose intolerance- Hyperinsulin*- Dysglycaemia- Dysglycemia
• Eg. Medline

Entry Criteria
Inclusion Criteria Exclusion Criteria
Pregnant Women with or without GDM Randomized Trials Dietary Interventions Dietary Comparator or Standard of Care Outcomes of interest: FBG, FBI, HbA1c,
HOMA-IR Follow-up duration ≥1 month
Non-pregnant participants Non-Randomized Trials Observational Studies Non-Human Studies Nutrient Supplemental Studies No Adequate Comparator No report on outcomes of
interest Acute studies <1 month
No language restriction will be placed.

Data Extraction
• 2 independent reviewers (VH, TBD)
• Variables of Interest: Study design (parallel or
crossover) Blinding (yes or no) Sample size (n) Sample characteristics (age,
gender, BMI, pre-existing conditions)
Dietary Pattern Comparator Follow-up Duration Macronutrient profile of the
background diet Mean±SD end values P-values for differences
between start and end values, and between treatments

Study Quality Assessment-Cochrane’s Risk of Bias Tool
Low Risk of Bias High Risk of Bias Unclear Risk of Bias
Random Sequence Generation
Allocation Concealment
Blinding of Participants and Personnel
Incomplete Outcome Data
Selective Reporting
Other Sources of Bias
Modified from: Higgins & Green. Cochrane handbook for systematic reviews of interventions version 5.0.2 updated. The Cochrane Collaboration, 2009.
To assess if there are biases that would lead to under- or over estimation of the true intervention effect

Statistical Analysis
Pooled Primary Outcomes
Bayesian Fixed or Random Effects Model (Mean Difference with 95% Credible Intervals):
1. Fasting Blood Glucose2. Fasting Blood Insulin3. HbA1c4. Homeostatic Assessment Model- Insulin Resistance (HOMA-IR)
Heterogeneity
Significance by Cochran’s Q-statistics with quantification by I2
a priori Subgroups
1. Ethnicity (European, Asian, African, or Others)2. Stage of Pregnancy (First, Second, or Third Trimester)3. Gestational Diabetes Status (yes or no)4. Pre-Pregnancy Body Weight
Heterogeneity

Statistical Analysis
Consistency
Assessed using node-splitting method
Ranking
Markov Chain Monte Carlo Methods to generate probabilities of a given treatment as being the best
Publication Bias
1. Visual inspection of funnel plots2. Egger’s and Begg’s tests
3. Trim-and-Fill Method

GRADE Assessment
To assess the overall network meta-analysis confidence via:1. Grading each pairwise network estimate2. Grading the ranking
GRADE:1. Study limitations2. Indirectness3. Inconsistency4. Imprecision5. Publication Bias

PRELIMINARY RESULTS

Consort Statement
4566 articles identified. 1240 MEDLINE (up to July 6 2014). 2650 EMBASE (up to July 6 2014). 676 Cochrane Library (up to July 8 2014).
Articles excluded based on title and/or abstract.
Articles that will be reviewed in full.
Articles that will be included in the network meta-analysis.

Next Steps
Time Task
September 2014 Database Search
December 2014 Literature Search
February 2014 Data Extraction and Entry
April 2014 Data Imputations
July 2014 Manuscript Draft
October 2014 Submit for Publication

Thank you!