Identify stages of patient assessment
34
Patient Assessment Ms. Manasa trinath Lecturer, KKU, SA
-
Upload
manasa-trinath -
Category
Health & Medicine
-
view
36 -
download
1
Transcript of Identify stages of patient assessment
Patient Assessment
Ms. Manasa trinathLecturer, KKU, SA

Stages you take from the moment you arrive at the scene of an incident to when you safely get your patient to the appropriate receiving hospital
• Survey of the Scene/Approach• Gloves on• Danger• Scene History (What has happened, get info
visually and Verbally)• Patient level of consciousness on the AVPU
scale
Primary Survey• Airway - Clear. Aspirate if necessary• C-Spine - Consider spinal immobilization if an
injury is suspected• Breathing - Head tilt, chin lift, Jaw thrust. Look,
Listen and Feel. Consider adjuncts to maintain airway. Oropharyngeal or Nasopharyngeal. If no respiratory effort use a Bag and Mask with 100% O2 if available.
• Circulation - Feel for a carotid pulse. If no pulse consider Precordial thump. Recheck pulse if absent commence chest compressions. Control any Major Bleeding
Secondary Survey
• History taking - Asking questions about signs and symptoms i.e.. When did they start etc. Previous Medical History
• Conduct a Top to Toe examination• Record pulse and respiratory rates

Patient Management/Transport
• T.L.C• Appropriate Care for Patient's Particular
Complaint• Smooth journey to hospital
Continually Reassess Patient
• Carry on monitoring for any changes in condition
• Carry out thorough observations e.g. BP, ECG, SPO2 etc
Pre-Alert Call to Receiving Hospital
• A - Age• S - Sex• H - History of event• I - Injuries sustained• C - Condition of patient. GCS, Revised Trauma
Score, BP etc• E - Estimated Time of Arrival at Hospital
Patient History
• Obtaining an accurate account is a critical first step in determining the history of a patient's chief complaint. History taking is an 'art' in itself and will take a little while to get to grips with, on top of thinking what could be wrong and what treatment you should give. This is the time when your crewmate will be able to help you out when your thoughts go blank. More often than not asking just one question will put you back on track.
Some points to taking a patient history:• Introduce yourself to the patient. Add a smile as this will help put
them at ease• If possible bring yourself to their level and not talk down to them• Ask them their name. Older people often like to be addressed by
their surname, but ask which name they'd like to be known as. • Try not to be too informal by using names like sweetheart, darling,
love.• Ask open ended questions to start with. Something like "What's been
happening today" or "What made you call for an ambulance"• Try and get the patient to be specific as to why the ambulance has
been called, this may require you to push for the chief complaint as patients can wander off track and drift back 10 years to when they had flu if you not careful.
• A patient may have a number of complaints that they may want to talk about. You can only deal with one at a time so each condition will have to be explored individually

Continue..… • Follow up questions such as those below will be the next step in gaining a
successful history. As an example I will use the types of questions asked of a patient with a complaint of pain.
– Duration - How long ago did pain start? What were you doing at time when pain started? Have you experienced this before?
– Severity - Can you describe this pain? Get them to score the pain from 1 to 10, Is the pain sharp or pressure like.
– Provocation - Does anything in particular bring on pain?
– Radiation - What is the main location of pain and does it radiate to other parts e.g. Into back, jaw, down arms and legs
– Associated problems - Does the patient have any other signs and symptoms they think are related to the current complaint?
– Reason to call ambulance - If this is an on going problem ask why they felt a visit from an ambulance was necessary today? Try to word this so it doesn't sound as though the patient is wasting your time.
Points 1 to 5 can be condensed into a simple phrase to make remembering the types of questions easier.
• P - Provocation (What were you doing at time of pain)
• Q - Quality (What the pain feels like)• R - Radiation (Is the pain felt anywhere else)• S - Severity (Score pain from 1 to 10)• T - Time (How long has pain been present)• A - Associated signs and symptoms

Neurological Assessment
• The Glasgow Coma Scale is a simple but effective way of assessing a patients neurological condition. It categorizes the patients responses to certain stimuli and gives that response a score.
• It is divided into 3 main categories of response.

1. Best Motor Response
6 Obeys Commands5 Localises pain.4 Withdrawal to pain3 Flexion2 Extension1 No response to pain.

2.Best Verbal Response
5 Oriented4 Confused conversation3 Inappropriate words2 Incomprehensible sounds1 No verbal response
3.Eye Opening
4 Spontaneous.3 Open to speech2 Open to pain.1 No eye opening
A GCS of 8 or less indicates severe injury, one of 9-12 moderate injury, and a GCS score of 13-15 is obtained when the injury is minor.

Pulse
• Definition of a Pulse: The throbbing of a person's arteries as an effect of their heart beat, which can be felt at the wrist and other places
• Pulses are manually palpated with two fingers, generally the pointer and middle finger. The thumb must not be used because it has its own pulse that will be felt instead of the patient's pulse. The two fingers must be placed near to an artery in order to feel the blood pulsating through the circulatory system.
Major Pulse Points
• Radial pulse - located on the thumb side of the wrist
• Carotid pulse - located in the neck• Brachial pulse - located in between the bicep
and tricep; frequently used in place of carotid pulse in infants, who have no neck
• Femoral pulse - located in the thigh• Dorsalis pedis pulse - located on top of the
foot

• Taking a pulse is a good indicator as to whether a PT's heart rate is fast (Tachycardia), Slow (Bradycardia), whether the PT has a Regular or Irregular beat and if the pulse is Strong or Weak. A pulse is also felt for in the case of a fracture to see whether or not blood is flowing to the distal point of a limb past the site of injury. The palpability of a pulse is dictated by the patient's blood pressure .

Other types of assessment that are carried out while performing your secondary survey
• Auscultation - The technical term for listening to the internal sounds of the body, usually using a stethoscope. Auscultation is normally performed for the purposes of examining the cardiovascular system and respiratory systems (heart and lung sounds), as well as the gastrointestinal system (bowel sounds).

Approximate Auscultation Sites
Auscultate from side to side and top to bottomAvoid the area over the scapulaeNote any differences in sounds from each sideList findings on Patient Report Form

• Palpation - a method of examination in which you feel the size, shape or firmness of body parts.
• Palpation is used particularly for thoracic and abdominal examinations, but also for examination and palpation of pulses.
Percussion
• - is a method used to find out about the changes in the thorax or abdomen. It is done with the middle finger of one hand tapping on the middle finger of the other hand, which is positioned with the whole palm on the body. Depending on what is happening in the structure below, this will create a different type of sound. e.g. If a patient has a pneumothorax, when you tap on the affected side it will sound like you are tapping on a drum compared to the non affected side.

Pulse and Respiratory Rates (These figures vary depending on the literature you read)
• Respirations• Descriptors: Normal, Shallow, Laboured, Noisy,
Kussmaul• Adult (normal) 12 to 20 breaths per minute• Children - age 1 to 8 years 15 to 30• Infants - age 1 to 12 months 25 to 50• Neonates - age 1 to 28 days 40 to 60
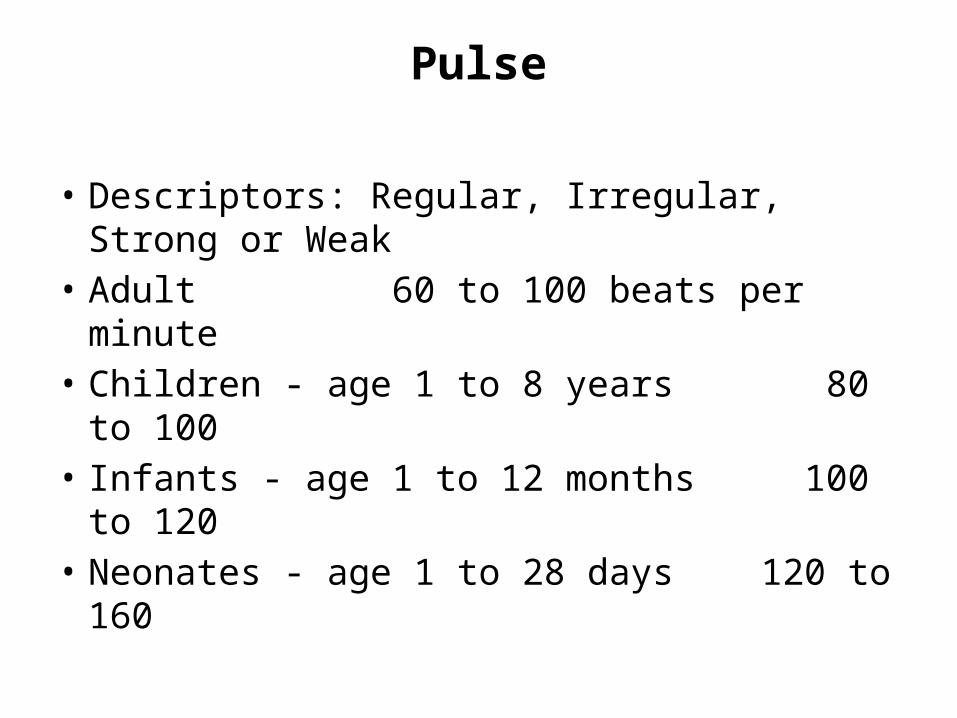
Pulse
• Descriptors: Regular, Irregular, Strong or Weak• Adult 60 to 100 beats per minute• Children - age 1 to 8 years 80 to 100• Infants - age 1 to 12 months 100 to 120• Neonates - age 1 to 28 days 120 to 160

Blood Pressure
• Blood pressure is the name given to the force that the beating heart causes in the arteries, veins, and blood vessels which carry blood around the body. When the heart contracts, forcing blood through the arteries and other blood vessels, your blood pressure goes up, and falls when the heart relaxes. High blood pressure can cause heart problems and strokes.

• When blood pressure is measured, the result is given as two figures, one higher than the other, for example 120/80. This is because tests measure the pressure in vessels when the heart is contracting (the higher figure also called systolic blood pressure), and then when it is relaxing (the lower figure also called diastolic blood pressure).

How to measure blood pressure
• Blood pressure is measured using a cuff which is placed around the upper arm and inflated until tight. It then deflates and a blood pressure reading is taken.
• The target for adults is for blood pressure to be below 140/90, or below 130/80 in people with diabetes. It is advised that if blood pressure is above this range, action should be taken to bring it down.
Why high blood pressure is a concern
• If blood pressure is high it causes a strain on blood vessels and the heart. High blood pressure can also cause kidney problems, and heart failure, when the heart is unable to pump blood around the body properly.
• The higher the blood pressure is, the greater the risk of stroke, heart problems and kidney failure.

Causes of high blood pressure• People with a family history of high blood
pressure, stroke, or heart disease are more likely to have high blood pressure. Diabetes and kidney disease also increase the risk.
• Blood pressure can be raised by diet and lifestyle. Being overweight increases blood pressure, as does eating a fatty diet and drinking too much alcohol. Smokers, people who consume too much salt, and those who do not take regular vigorous exercise are also more likely to have high blood pressure.

How to take a manual Blood Pressure
• Tools required: sphygmomanometer and a stethoscope
The following steps may be helpful to take a blood pressure.• Sit up or lie down with the arm stretched out. The arm should
be level with the heart.• Put the cuff about 1 inch (2.5 cm) above the elbow (over the
brachial artery). Wrap the cuff snugly around the arm. The blood pressure reading may not be correct if the cuff is too loose.
• Put the stethoscope earpieces in your ears.• Using your middle and index fingers, gently feel for the brachial
pulse. You will feel the pulse beating when you find it.• Put the diaphragm of the stethoscope over the brachial artery
pulse. Listen for the heartbeat.
Continue..• Tighten the screw on the bulb and quickly squeeze and pump the
bulb. This will cause the cuff to tighten.• Keep squeezing the bulb until the scale on the gauge reads about
160. Or, until the gauge reads at least 10 points higher than when you last hear the heartbeat.
• Slowly loosen the screw to let air escape from the cuff. Carefully look at the gauge and listen to the sounds. Remember the number on the gauge where you first heard the thumping sound.
• Continue to listen and read the gauge at the point where the sound stops.
• The number of the first sound is the systolic (top number) pressure.
• The second number is the diastolic (bottom number) pressure.

Estimating Blood Pressure
• The advanced trauma life support course teaches that a patients systolic blood pressure can be "estimated" if you haven't got a sphygmomanometer to hand. This is achieved by feeling for a pulse, i.e.
• If a Radial pulse is present then the PT's systolic BP is > 80mmHg
• If a Brachial pulse is present then the PT's systolic BP is 70-80mmHg
• If a Carotid pulse is present then the PT's systolic BP is 60-70mmHg

Thanks