![THE REGISTRATION ACT, 1908 - U.Pcomtax.up.nic.in/Miscellaneous Act/the-registration-act-1908.pdf · THE REGISTRATION ACT, 1908 (16 OF 1908) [18th December, 1908] An Act to consolidate](https://static.fdocuments.in/doc/165x107/5acb37ad7f8b9aad468b4a7a/the-registration-act-1908-u-actthe-registration-act-1908pdfthe-registration.jpg)
europepmc.orgeuropepmc.org/articles/PMC2046476/pdf/procrsmed00832-0005.pdf · iBurgtcal %ectiol....
66
iBurgtcal %ectiol. October 13, 1908. Mr. J. WARRINGTON HAWARD, President of the Section, in the Chair. Traumatic Rupture of the Intestine, with a Case of Recovery after Operation and an Analysis of the 132 cases that have occurred in ten London hospitals during the last fifteen years (1893-1907). By JAMES BERRY, F.R.C.S., and PAUL L. GIuSEPPI, F.R.C.S. WILLIAM H., aged 26, was admitted to the Royal Free Hospital under the care of Mr. Berry on September 25, 1907, suffering from the effects of a kick on the abdomen. On September 25, 1907, at 5 p.m., the patient received a kick just above the pubis from a horse close to which he was standing. He was not knocked down. He immediately felt severe pain in the hypogastrium, and was brought to the hospital in a cab at 5.15 p.m. On examination, a slight bruise was found just above the pubis. There was tenderness over this area. The abdomen moved with respiration. The patient was not collapsed and did not seem very ill; the pain slowly increased in severity, as did also the hypogastric tenderness. The abdomuinal muscles were markedly contracted and hard. He vomited several times. The bladder had been emptied four hours previous to the accident. Urine was passed twice after adinission; on neither occasion did it contain any blood. He had had his last meal about 12 o'clock. A severe injury to the abdomen and probably ruptured intestine was diagnosed, and Mr. Berry summoned. Shortly before 9 p.m. the patient was first seen by Mr. Berry. There were then severe abdominal pain and marked tenderness over the hypogastrium. The muscles of the abdominal wall were very rigid, N-22
Transcript of europepmc.orgeuropepmc.org/articles/PMC2046476/pdf/procrsmed00832-0005.pdf · iBurgtcal %ectiol....

iBurgtcal %ectiol.October 13, 1908.
Mr. J. WARRINGTON HAWARD, President of the Section, in the Chair.
Traumatic Rupture of the Intestine, with a Case of Recoveryafter Operation and an Analysis of the 132 cases thathave occurred in ten London hospitals during the lastfifteen years (1893-1907).
By JAMES BERRY, F.R.C.S., and PAUL L. GIuSEPPI, F.R.C.S.
WILLIAM H., aged 26, was admitted to the Royal Free Hospitalunder the care of Mr. Berry on September 25, 1907, suffering fromthe effects of a kick on the abdomen. On September 25, 1907, at5 p.m., the patient received a kick just above the pubis from a horseclose to which he was standing. He was not knocked down. Heimmediately felt severe pain in the hypogastrium, and was broughtto the hospital in a cab at 5.15 p.m. On examination, a slight bruisewas found just above the pubis. There was tenderness over this area.The abdomen moved with respiration. The patient was not collapsedand did not seem very ill; the pain slowly increased in severity, asdid also the hypogastric tenderness. The abdomuinal muscles weremarkedly contracted and hard. He vomited several times. The bladderhad been emptied four hours previous to the accident. Urine waspassed twice after adinission; on neither occasion did it contain anyblood. He had had his last meal about 12 o'clock. A severe injuryto the abdomen and probably ruptured intestine was diagnosed, andMr. Berry summoned.
Shortly before 9 p.m. the patient was first seen by Mr. Berry.There were then severe abdominal pain and marked tenderness overthe hypogastrium. The muscles of the abdominal wall were very rigid,
N-22

'2 Berry & Giuseppi: Traumatic Ruptutre of the Intestine
and there was somne dulness in the left lumbar region in front. Theliver dulness was normal. Per rectum, nothing abnormal could be felt.The pulse-rate had slowly risen from 76 to 96, temperature was 990 F.,respirations 26. It was decided to perform a laparotomy as soon aspossible. The operation commenced at 9.45 p.m. and lasted twenty-five minutes, chloroform and ether being administered; 'liv of liquorstrychninae were injected before the operation began. An incision6 in. long was made I in. to the left of the middle line, commencing1 in. above the umbilicus. On opening the peritoneal cavity no gas,but a thin, non-odorous, gruel-like material escaped; in it portions ofFrench beans were obvious. The visceral peritoneum had not lost itslustre, but was injected and slightly granular, and there were also someflakes of lymph adherent to the small intestines. A complete longi-tudinal rupture 12 in. long was quickly found on the side oppositeto the mesenteric attachment. The mucous membrane was slightlyeverted. The affected coil was brought out, an intestinal clamlp applied,and the contents squeezed out. The opening was closed with a doublerow of continuous fine silk sutures. The first row passed through all thecoats; the second row was of Lembert sutures. The opening wasclosed in the direction of the long axis of the bowel. The lumen of thegut was reduced thus to about one-half its normal size. The rupturewas situated in the ileunm, judging from the size of the gut; no otherrupture could be found. Saline solution at 105° F. was poured into theperitoneal cavity and then expelled by compressing the abdolliinal wall.This was repeated several times; the time thus spent did not exceedfour minutes. A rubber tube, 8 in. long and 11 in. in diameter, wasinserted into Douglas's pouch. The abdominal wall was united in twolayers with catgut and silkworm-gut sutures. The patient was thenturned on to his face for half a minute, with the shoulders raised, soas to empty the abdomen comnpletely.
The patient, on returning to bed, was sat up at an angle of 450.The after-treatment consisted in the subcutaneous administration of utvof liquor strychninae everv hour and rectal infusiQns of saline (2 pints)every two hours.
September 26: Temperature 1000 F., respirations 26, pulse 102;complexion sallow. The patient had had but little pain. He was nowsat up erect in bed. At 10 a.m. the tube was removed and replaced byone i in. in diameter. There was some difficulty in removing the tube,as a coil of small intestine had slipped into one of the holes in thetube. Some discharge was sucked out of the pelvis. The patient had

Surgical Section3continued to vomit. Five minims of liquor strychninae were now givenevery two hours, and saline 1 pint per rectum every two hours.September 27: Patient less sallow. The wound was dressed in themorning, and a large piece of membranous lymph was removed. Therewas hardly any discharge from the tube. There was some little dis-tension of the abdomen, and the patient continued to vomit; the vomithad an intestinal odour. In the afternoon the tube was removed andthe wound lightly packed with gauze. Leucocyte count, 15,200 per cubicmillimetre; liquor strychninal, wlv, every two hours. Five grains ofcalomrel were given with a good result, and a turpentine enema. Sep-tember 28: The patient was much better and able to read and enjoy themorning paper. The vomiting ceased at 4 a.m.; the distension. wasless. Five minirms of liquor strychninme every six hours; 4 oz. ofpeptonized milk every two hours. September 29: Milk 6 oz. by themouth every four hours was given to the patient, who up to this timehad had nothing but water by the mouth.
Since admission the patient had absorbed 26 pints of water perrectunm and had had 173 miniins of liquor strychninae subcutaneously;of these, 95 were given in the first twenty-four hours; he never hadmuscular twitching at any time. On the mnorning after the operationthe temperature rose to 100'2° F. ; after this it never reached 1000 F.,and after the third day it remained perfectly normal. The highestpulse-rate recorded was 102 on the morning after the operation; afterthis it was generally between 80 and 90.
October 1 : The wound looked healthy, the stitches were removedexcept those just above the sinus. For the last three days the bowelshad been opened without any purgative. October 2: The remnainingstitches were taken out. October 3: The edges of the wound gaped for11 in. October 8: The sinus extended backwards for 2 in. October 15:Sinus measured 1I in. October 22: The sinus has completely healed.
November 4: The granulating wound was stitched up. November12: The wound measured 13 in. wide. The stitches that were put indid not hold. November 14: The patient left for a convalescent homefifty days after the operation.
December 11 : The wound had now comlpletely healed. The scarseemed strong. A belt was ordered.'
Leucocyte counts from September 27 till October 17 varied between10,000 and 17,000.
' The patient was shown at the meeting on October 13. He was in excellent health andsaid that his bowels acted regularly and normally.
3

4 Berry & Giuseppi: Traumatic Rupture of the Intestine
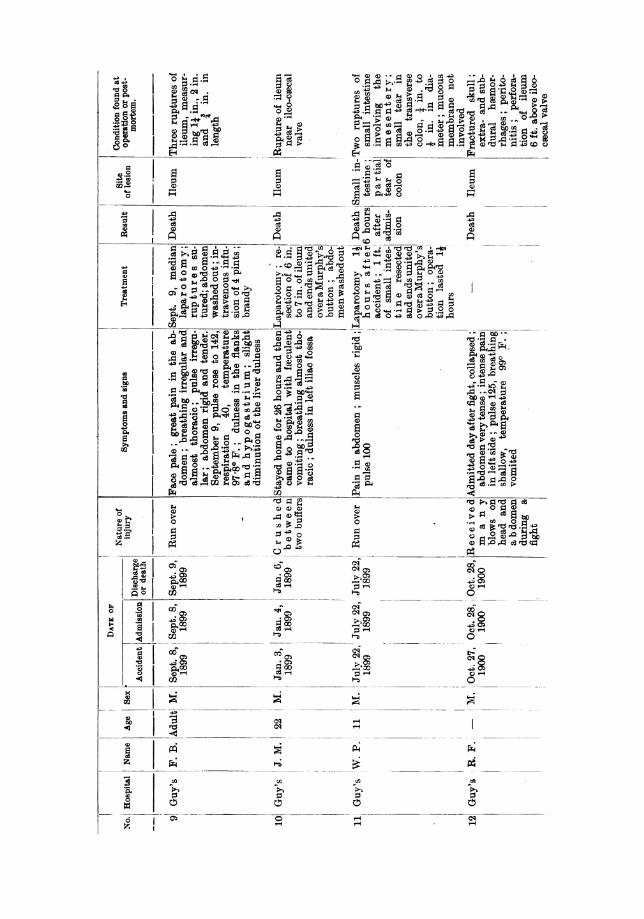
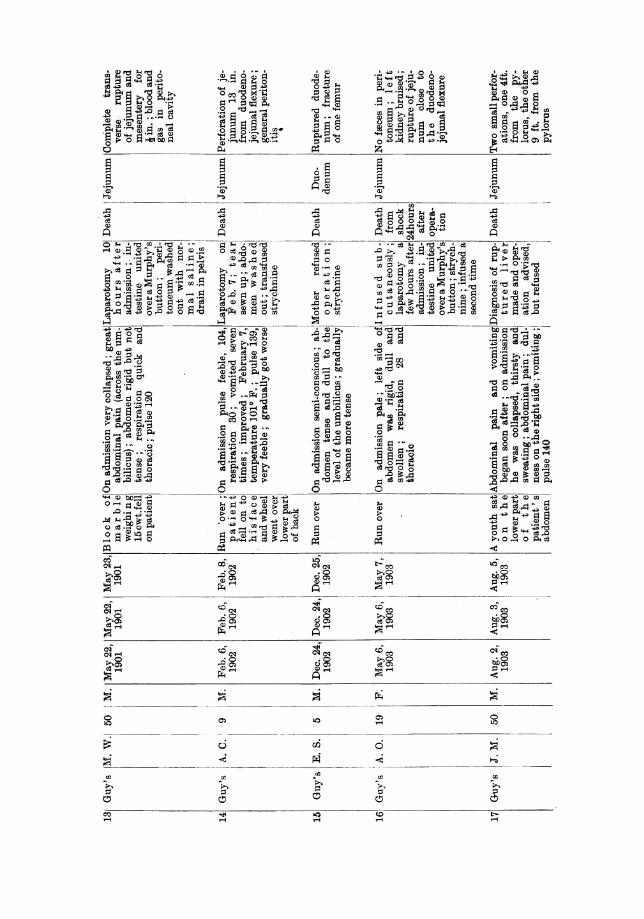
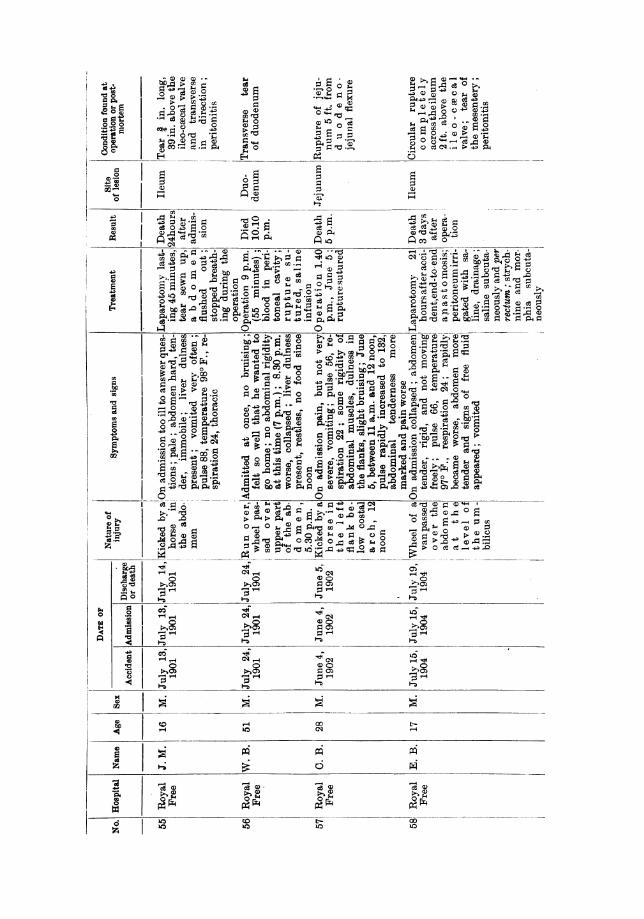
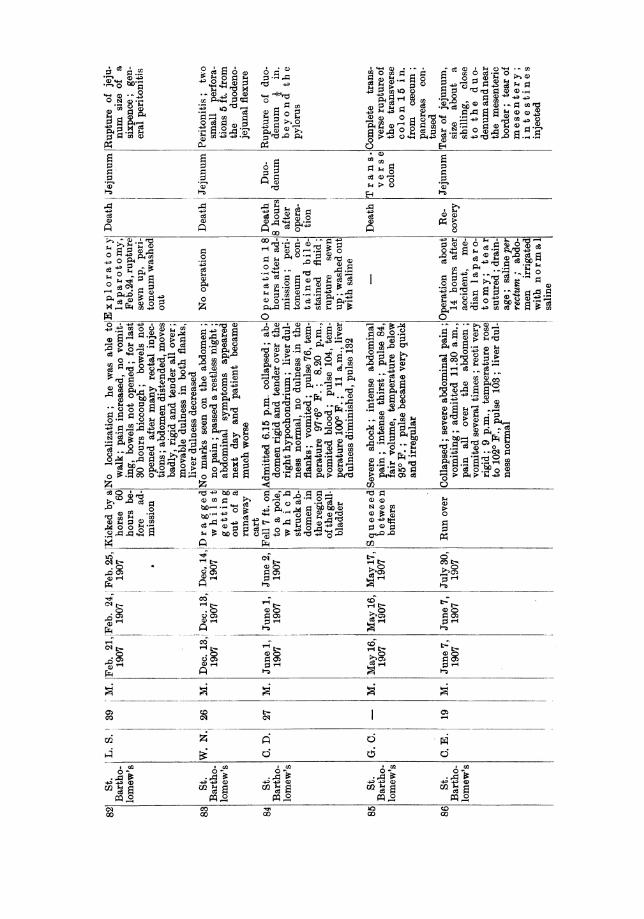
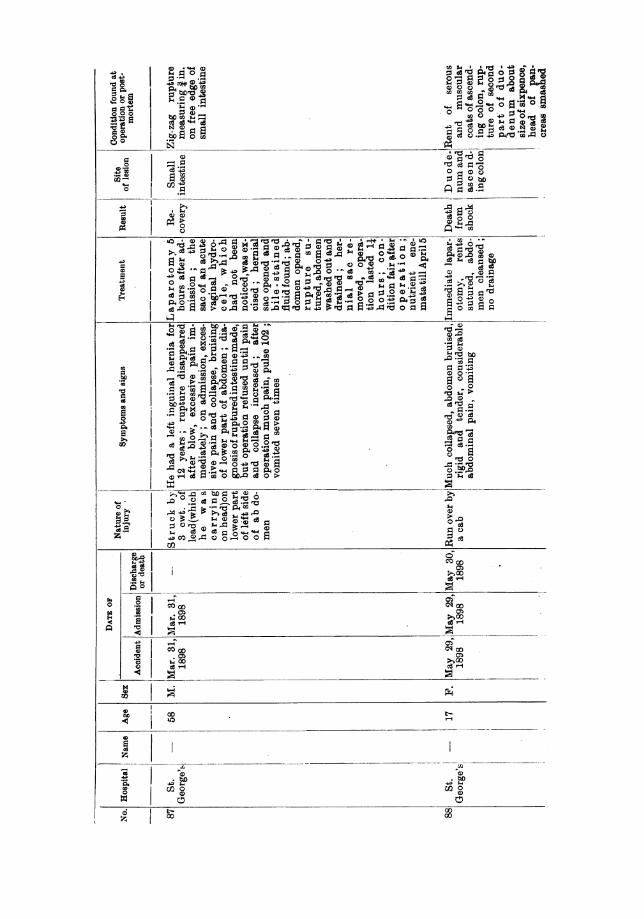
This case has led us to an investigation into the subject of rupture ofthe intestine, in the hope that we might be able to throw more lightupon the difficult problems of the early diagnosis of such injuries alnd thebest methods of dealing with them. For this purpose we have collectednotes of all the cases of ruptured intestine, without external wound, thathave occurred in the last fifteen years (1893 to 1907 inclusive) in ten ofthe principal general hospitals in London (see Appendix, Table I).These hospitals are Charing Cross, Guv's, London, Royal Free, St.Bartholomew's, St. George's, St. Thomas's, University College, King'sCollege, and Middlesex. To the various Surgical Registrars and otherauthorities of these hospitals we desire to express our grateful acknow-ledgment for the help afforded to us in obtaining access to these records.Many of the cases have been published already, in hospital reports orelsewhere, but most of them are to be found only in manuscript in thehospital records.
The list of 132 cases embraces, so far as we are aware, all the casesof ruptured intestine that have occurred at these hospitals within theperiod mentioned. Among the many excellent papers that have beenwritten on the subject of ruptured intestine we should like to referespeciallv to that of Hertle, who has given a detailed list of 145 cases,compiled partly from the records of the Graz (Austria) clinic, partlyfroiii other German and Austrian clinics, and partly from the literature(mainly recent).
Curtis's list of 116 cases was published in 1887, and is compiledwholly fronm published cases, mainly American and English. Few, ifany, of Hertle's cases are to be found in Curtis's list, and none of oursOCCUrS in either of the two other lists. These three long lists of cases donot overlap to any appreciable extent, and may be used for purposes ofcomparison. Ouir own list of cases is, so far as we know, the only largecollection of cases drawn exclusively from hospital records, and hastherefore in sonme respects more value than lists compiled solely ormainly from published surgical literature, in which successful or remark-able cases are apt to attain undue prominence. Of Mr. Makins's well-known list of 21 cases occurring at St. Thomas's Hospital during theyears' 1889 to 1898, no fewer than 14 are necessarily also included inour own list.
It so happens that, of the whole number of 132 cases in ourlist, 10 have been under the care of one of us at the Royal FreeHospital. Of the 27 cases that occurred at St. Bartholomew's Hospital,7 of the earlier ones came under the observation of one of us when

Surgical Section 5
Surgical Registrar at that hospital in the years 1893 to 1897 inclusive,and the post-mortemn examinations on most of these were made by him.Upon the clinical and pathological knowledge thus obtained, and uponthe examination of the hospital and other records above mentioned, theconclusions in our paper are based.
ETIOLOGY AND PATHOLOGY.
Tables III, IV, and V show the relative frequency of the injury inthe two sexes and at various ages. As might be expected, it occursmost commonly in boys and young men, whose occupations render themmore liable to accidents from violence. Rupture of the intestine inwomen and children is caused most often by being run over or by falls.Of the 14 children under 10 years of age, in 10 the injury was due tobeing run over, in 2 to falls, in 1 to a kick, and in 1 to a blow. Of the10 women 7 were run over, in 1 case a wall fell on the patient, and in2 the injury was due to a fall.
Berry and Giuseppi(ten London hospitals,1893 to 1907 inclusive)
Male 122Female ... 10
TABLE III-SEX.
Petry(Prague clinicand literatuire)
217 ...
15 ...
Hertle(Graz clinic
and literature)124
4
Makins(St. Thomas's Hospital,1889 to 1898 incluisive)
... 210
TABLE IV-AGE (STATED IN 125 CASES).
Berry and Giuseppi.
Total Under 5 to 10 10 to 20 to 3cases 5 20 30
10 - 3
23 - 5 7 4
32 -- 1 8 10(2) (1)
32 1 2 6 4(1)
25 2 3 5 4(1) (2) (1)
4 1 23 2 1
32__ 3 (1) (1)
132 3 11 32 28
30 to 40 to 50 to 00 to40 50 60 70
3 2 - 1(1)
1 1 3 1
4 4 3 --
Over Not Situation of rupture70 stated
1 Large intestine
_ 1 Duodenum ...- Duodeno-jejunal
flexure ...
2 Jejunum l Small
intestine
_ - " Small intes-tine" ..
-- Large and small intestine_ - Partial rupture
Figures in brackets mean recoveries.
I

6 Berry & Giuseppi: Traumatic Rupture of the Intestine
TABLE V-HERTLE'S COLLECTED CASES.
Age Men Women0 to 10 years ... 511 , 20 ,, ... 14 ...
21 , 30 ,, ... 33 ...31 ,40 ,, ... 35 ... -
41 ,,50 ,, ... 27 ... 151 ,60,, ... 17 .. 261 ,,70 ,,..3 ... 1Not stated ..7 ...
141 4
Hernia to a small extent predisposes to rupture of the intestine, asshown in Case 87, in which a mass of lead fell upon an inguinal herniaand caused rupture of the intestine.
When we come to consider the causation of the injury, it will beseen at once that the various forms of injury may be classed under veryfew headings, namely: run over, squeeze or crush, blow, kick, and fall.These five headings include almost all the cases in our series and in thatof Hertle.
TABLE VI-CAUSES OF TRAUMATIC RUPTURE OF THE INTESTINE.
Berry and Giuseppi Hertle(hospital records) (literature)
Run over ... ... 51 ... 10Squeeze or crush ... 24 ... 11Blow.. ... ... 23 ... 47Kick ... ... ... 16 ... 40Fall .. ... ... 11 ... 20Reduction of hernia ... 1Trodden on ... ... ... 4Uncertain ... ... 6 ..
Severe exertion ... . . . 6
132 138
As might he expected, our statistics, drawn from the hospital recordsof a crowded metropolis, show a relatively large number of run-overcases-no fewer than 51 out of 132. Hertle's figures, drawn mainly fromliterature, are 10 run-over cases out of 138; and Curtis's, taken alsofrom literature, are 13 out of 116 cases. On the other hand, in only16 of our cases was the injury due to a kick, while Hertle's and Curtis'sfigures are respectively 40 and 28. The discrepancy in these figures isprobably due to the fact that ruptures due to kicks are less likely to becomplicated by other severe injuries, are therefore more likely to bethe subjects of operative interference, and consequently find their waymore readily into surgical literature.
Of the 24 cases in our list in which the rupture of the intestine wascomplicated by other injuries, in no case was the injury stated to have
Surgical Section
been due to a kick. Of the 24, no fewer than 19 were due to being runover or crushed, or to falls from a height.
The relative frequency of rupture of the intestine in cases of kickfrom a horse has been variously stated by different authors. Surgeon-Major Cahier, in an excellent recent article on injuries of the abdomendue to kicks, has shown that of 15 or 16 cases in which the injuryseemed at first to be grave, in only 2 was laparotomy required for alesion of the intestine. Pech collected 71 cases of injury to the abdomenfrom kicks, treated at the military hospital at Luneville in twenty years,and found that 69 recovered without operative interference and only 2died fromu ruptured intestine. On the other hand, civil hospital surgeonswho deal with cases of kicks from horses probably see a larger propor-tion of severe cases than do the inilitary surgeons.
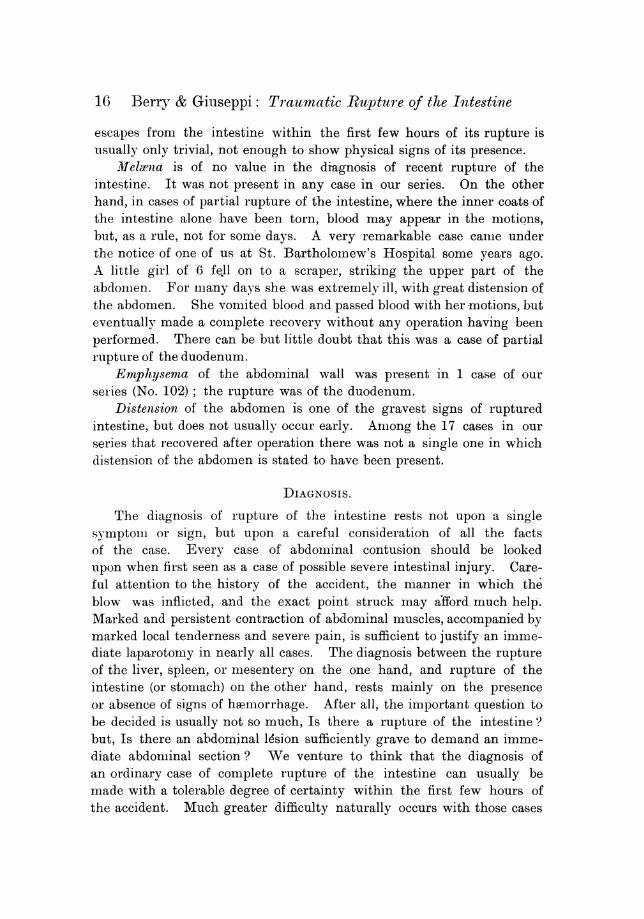
The conditions under which the intestine is ruptured are almostinvariably the sudden and violent impact of a hard substance against thebony portions of the posterior abdominal wall. The prominent verticalridge of the lumbar spine and, to a less extent, the iliac bones are thoseagainst which the intestine is violently crushed. As regards the largeintestine, a glance at Table VIII will show that it is precisely thoseportions that lie normally in front of these bones, namely the transversecolon, cecum, and sigmoid flexure, that are most liable to injury. AsMr. Makins has pointed out, those parts of the intestine that are mostexposed to injury are those which lie in the lower half of the abdomen.An important exception, however, is to be found in the duodenum,which, fromn its fixed position in front of the lumbar spine, is especiallyliable to injury. Of our 132 cases the duodenum was the part affectedin no fewer than 24 (see Table VIII). It is remarkable that amongMr. Makins's 21 cases there should have been only one of rupturedduodenum.
TABLE VII-SITE OF RUPTURE.
Berry and Giuseppi Hertle Curtis(ten London hospitals, (literature, (literature,
1893 to 1907) recent) older)Duodenum ... ... 24 ... 15 ... 6Duodeno-jejunal flexure ... 3 ....Within 3 ft. of duodenum or
ileo-caecal valve ... 27 ... ... 25Within 50 cm. (20 in.) of duo.
denum or ileo-caecal valve - ... 28Intervening small intestine ... 37 .. 43 ... 57Small intestine" (exact siteunknown) ... ... 25 ... 32 .. 21
116 118 109
7

8 Berry & Giuseppi: Traumatic Rupture of the Intestine
As regards the rest of the small intestine, our figures and those ofHertle and Curtis seem to show that there is some truth in the old beliefthat the parts of the small intestine that are most liable to injury arethe upper part of the jejunum and the lower part of the ileum, that is,those parts that are comparatively near fixed points, have a shortermesentery, and are more likely to be found lying in front of the lumbarspine and less likely to be able to slip aside and thus escape an im-pending blow. The rather large number of cases, however, in whichthe exact seat of rupture in the small intestine is not stated rendersconclusions on this point of comparatively little value. All parts ofthe small intestine are undoubtedly liable to injury. The situationof the lesion in our series of cases is shown as far as possible inTable VIII.
TABLE VI1I-SITUATION OF THE RUPTURE.
Berry and Giuseppi HertleLarge initestinie:
Ceecum ... ... ... 2Ascending colol ... ... 2Hepatic flexureTransverse coloini ... 3 ... 2Splenic flexure .... 1 ...'Descending colon -... 1Sigmoid flexure ... ... 4 ... 3Rectum ... ... ... - 1
10 11Small initestine onlv:
Duodenum ... 23' ... 12'Duodeno-jejunal flexure ... 3Jejunum .. 32 ... 29Ileum ... ... 32 ... 40Small intestine" ... 25 31
115' -- 112Large and small intestine ... 4Partial rupture (not involving lumen):
Large intestine ... ... 2 ...
Duodenum ... ... 13
132 123
Of Hertle's series of 134 cases 20 were multiple.
Three theories as to the production of a rupture of the intestinehave been brought forward, namely, that it is due to crushing, tobursting, and to traction. That direct traction is occasionally the causeof rupture is perhaps shown by the rather rare cases in which the tear
I This case was retroperitoneal.2Three of these cases were retroperitoneal.3Seven of these cases were retroperitoneal.I Eighteen of these cases were multiple.

SSurgical Section9
occurs at the duodeno-jejunal flexure, as in three of our cases (Nos. 64,72 and 75). Bursting, we venture to think, is a rare cause of rupture;it can scarcely occur except when the intestine contains an unsuallylarge amount of fluid. Hertle's series of interesting experiments on theproduction of rupture by bursting were carried out on living animalsand dead human subjects. They show how the intestine can thus beruptured. They are vitiated, however, in our opinion in that a pre-liminary ligature was applied to both ends of a coil of intestine prior tothe application of violence. This condition of complete closure ofboth ends of a coil of intestine is one which, in our opinion, can seldomoccur in the living huinan subject at a moment of injury. Hertle'sexperiments are of great value, however, in showing the kind of rentproduced by bursting and crushing injuries respectively. In crushinginjuries the muscular and mucous layers are those which are most easilydamaged; the submucous layer is more resisting, and the peritoneumthe most resisting of all. This is a point of great importance in con-nection with partial and secondary ruptures. All the coats of theintestine may be ruptured except the peritoneal or submucous, and thepatient will then have few or no symptoms of injury. It is not untilthe peritoneal or submucous coat has given way secondarily thatextravasation occurs and acute symptoms set in.
In Hertle's bursting experiments, on the other hand, it was shownthat the submucous layer was usually the last to give way, the peritonealbeing torn early. This is in accordance with what we so often see inextreme distension of the cwEcum due to stricture, rents of the peritonealcoat often preceding the actual perforation into the lumen. A carefulexamination of the rent in the intestine will somnetines enable us to saywhether or not the injury has been produced by bursting. For our ownpart we believe that rupture of the intestine in the human subject isalmost invariably produced by direct crush, and not by bursting. One ofthe rare exceptions, Case 68, in which the rupture was caused bythe violent reduction of a hernia, is probably one in which the rupturewas produced by bursting. The examination of museum and post-miiortemspecimens, as well as our necessarily very liiited experience on theliving subject, appears to us to bear out this contention. It is to beregretted that the notes of hospital records are usually not sufficientlyfull to enable us to draw conclusions from them on this point.
Multiple ruptures are by no means uncommon, as will be seen fromTable IX. In 22 of our cases the intestine was ruptured in two ormore places. The ruptures are usually not far apart. In 44 of our
9

10 Berry & Giuseppi: Traumatic Ruptuire of the Intestine
cases the notes make mention of the direction of the wound in theintestine. In 38 of these it was transverse, in the remaining 6 it waslongitudinal. Of the 38, in 15 the rent involved the whole circum-ference of the intestine, while in 7 more it involved more than two-thirdsof the circumference. In at least 15 cases the mesentery as well as theintestine was involved -in the laceration. Partial rupture not includingall the coats of the intestine was present in 3 out of the 132 cases.Retroperitoneal rupture occurred in 4 cases. Of these, three involvedthe duodenum and 1 the splenic flexure of the colon.
TABLE IX.
Multiple ruptures present in 22 cases out of 132 (Berry and Giuseppi)20 134 (Hertle)
42 266
In 24 cases out of 132 the rupture of the intestine was complicatedby the coexistence of other severe injuries. These complications were:Fracture of pelvis, 6 cases; fractures in other situations, 4 cases; rup-ture of liver, 4 cases; rupture of pancreas, 3 cases; rupture of stomach,2 cases; rupture of kidney, 1 case; rupture of lung, 1 case; rupture ofspleen, 1 case; of superior mesenteric and common iliac arteries, 1 each.
SYMPTOMS.
We come now to a far more important part of our subject, namely,the symptoms caused by rupture of the intestine. In 59 of our casesthe notes are sufficiently full to enable us to draw conclusions withregard to the relative frequency of the more important symptoms (seeTable X).
TABLE X-DIAGNOSTIC SYMPTOMS IN 59 CASES OF RUPTURF, OF THE INTESTINES,WITH FULL NOTES.
Presenit AbsentPain .... ... ... ... 51 ...-Vomiting ... ... ... 43 ... 2Shock ... ... ... ... 28 ... 6
Local tenderness ... ... 35 ... 2Rigidity ... ... ... 50 ...4
Distension .. ... ... 11 .. 14Added dulness ... ... 18 ... 14Rising pulse ... ... ... 37 ... 6Loss or diminution of liver dulniess 6
It need hardly be said that if treatment is to be efficacious the diagnosismust be made early, within the first hours after the injury. We venture

SurXgical Section1
to think that in imany of the cases in oui list the diagnosis was not nmadeas early as it might have been. We should like especially to direct theattention of general practitioners and hospital residents, who see thesecases early, to the fact that rupture of the intestine is often caused bya comparatively slight blow, and that the initial symptomiis often do notsuggest to the mind of the inexperienced that so serious an injury asa rupture of the intestine can have been sustained.
There is a tendency, and a very natural one on the part of a housesurgeon, when face to face with a case of abdominal contusion whichmay possibly be one of ruptured intestine, to wait and watch for pro-nounced symiiptoim-s. When these latter have set in he sends for thesurgeon, who thus only too often does not get the opportunity of seeingthe patient until the mlost favourable timie for operation has passed away.
In these days almost everyX hospital surgeon is in telephonic comn-munication with his hospital. We venture to think that it is the dutyof every house surgeon, as soon as he has satisfied hiimiself that hispatient has received a severe blow on the abdomen, to telephone forth-with to his surgeon and to give the latter the opportunity of askingfurther questions, and, if necessary, of at once going to see the patienthimself.
Even when the blow upon the abdomen appears to have been aslight one the samiie course should be adopted if the patient is coill-plaining of severe and persistent pain. This leads us to the statementthat of the very early symptoms of rupture of the intestine pain isby far the most iilmportant. Again and again do we find it recordedthat within the first few hours the patient suffered froim- "great"pain, " severe " pain, "intense " pain, and so forth, and that the painwas continuous. In cases where there is profound shock, often due tothe presence of other inj'uries as well, pain imay be slight, but these arenot the cases in which the serious nature of the accident is likelv to beoverlooked (see Case 70).
There is yet another class of case in which pain is not necessarilya very imarked feature, naimuely, those in which the rupture is incom-plete. The pain is due to extravasation of irritating intestinal contents,and it is possible, although very unusual, for no extravasation to takeplace in the first few hours after the injury. It is well known that ina small rupture of the intestine the protruding imlucous membrane mllaytemporarily occlude the opening and prevent extravasation. Even incases of coimplete transverse rupture there is no doubt that extravasationof intestinal contents is som--etimnes delayed for sonle hours.
11

12 Berry & Giuseppi: Traatnatic Rapture of the Intestine
Dambrin, in his interesting monograph on " Lesions of the Intestine,"quotes the theory of Jobert Lamballe, who affirnms that the two cut endsof intestine retract, so as to narrow the lumen. He goes on to say thathis experiments confirm this theory: "We have always seen imlmledi-ately after the injury the neighbouring intestine contract over a lengthof several centimetres, thus obliterating the lumen; the mucous meni--brane usually protruded."
We believe that complete rupture of the intestine with extravasationis always accompanied by severe pain, except in certain rare cases, whenthe patient is profoundly collapsed or is unconscious as the result ofother injuries. Whether a patient with comlplete rupture, but withoutextravasation, can be quite free from pain is, we think, open to doubt,and we hope to elicit expressions of opinion upon this point frommembers of the Society. There can be little or no doubt that whena patient who has ruptured his intestine renlains free froin pain forsome little time after the injury this immunity is due to the rup-ture being incomplete. One or other of the intestinal coats, usuallythe peritoneal or submucous, has not been completely ruptured.
The following case came under the notice of one of us solmie yearsago: A boy received a severe injury to the abdomen. He walked tothe nearest hospital, but he seemed in so little pain and seemlled sowell that he was allowed to go home. Here he proceeded to eat agood supper, but immediately afterwards he was seized with severepain in the abdomen and other symptolmis of intestinal perforation.For these he was admitted to St. Bartholomew's Hospital, where heshortly afterwards died. At the post-mortem, performed by one ofus, an extensive rupture of the duodenum was discovered. The pern-toneal coat was much less torn, however, than the others, and hadevidently given way secondarily.
In no fewer than 51 of the previously mentioned 59 cases it isdefinitely stated that pain was an early symptom, and it was usuallysevere. In the other 8 no inention is made of this symptom. In only3 of the whole series of 132 cases is it definitely stated that pain wasnot present in the first few hours after the accident. Of these casesone (Case 70) was that of profound collapse already mentioned.Another was Case 83, in which there were two small perforations ofthe jejunum, and in this case the symptomns of rupture did not set inuntil the day after the accident ; here the rupture was almost certainlya secondary one. The third case was No. 63, a remarkable case of sub-mucous rupture of the duodenum without involvement of the peritoneum.

Surgical Section
The specimen froml this case is in the nmuseum at St. Bartholomew'sHospital (No. 204OAi), and by the kindness of the Curator we are ableto show it to you to-night.
The patient was a boy aged 15, who was run over across theabdomen by a fire-escape. He was at once br,ought to the hospitalin a state of collapse. He vomnited several times. On the followingday he seemed to have almiiost completely recovered, and conjplainedonly of a little abdominal pain and tenderness. Later vomiting againset in, and the boy died of intestinal obstruction on the fourth day. Atthe post-mortem, which was performed by one of us, a subperitonealrupture of the duodenuiim was found. A clot of blood as large as ahen's egg lay between the peritoneal and the miuscular coats, andcompletely blocked the second part of the duodenum.
A point that miiay be of imuch assistance in the diagnosis of ruptureof the intestine is the shifting of the pain from one part of the abdomento another. This is well illustrated by Case 48, under the care ofone of us at the Royal Free Hospital. A man, aged 29, was struckin the epigastrium by the pole of a cart, and was brought at once to thehospital. He was suffering severe pain in the epigastrium and left hypo-chondriunm, but was not thought by the resident medical officers to beseriously injured. Somrle four hours later, when seen by one of us, hewas still in good condition, but his abdominal muscles were extremelyrigid, he had vomited several times, and his pain, which had been con-tinuous since adimiission, had now shifted from the upper to the lowerpart of the abdomen. A slight abrasion of the skin on the epigastriumlafforded clear evidence of the exact seat of injury. The shifting of thepain downwards seeimied to point to extravasation of irritating fluid,which had gravitated downwards. On the strength of these sym-ptomiis the diagnosis of ruptured intestine was made and the abdo-nen. iiiiiediately opened. A very extensive rupture of the duodenumwas found, which was sutured with great difficulty, and the patientdied ten hours after the operation. The case is also interesting inthat the man's general condition some three or four hours after theinjury was so good that the house surgeon, in reporting the admissionof the case, expressly said that he did not think that any operationwas called for. He reported its admission, he said, merely becausehe knew that the surgeons of the Royal Free Hospital liked to betold of abdominal injuries at an early date. A somewhat similarcase, in which the shifting of the seat of pain afforded material helpin diagnosis, has been recorded by Mr. Battle in th6 British MedicalJournal, June 13, 1908, i, p. 1412.
13

14 Berry & Giuseppi: Traumatic Ruptmure of the Intestine
Shock, as a symptom of ruptured intestine, is of very little value. Itis often present, but it need scarcely be said that it is also very commonin abdominal contusions of all kinds, quite apart from ruptured intestine,whereas severe and continuous pain is not. In many of our cases shockwas entirely absent. Several of the patients walked home after theaccident (i.e., Cases 94, 100, and 113); some of them walked to thehospital (Cases 65, 82, and 110). Two of the patients went on with theirwork. Case 124 remained at work for four hours, and Case 131 wheeledhis barrow home before coming to the hospital. Aimong our 59 cases itwas definitely stated that shock was present in 28 cases and absent in 6.
Vonmiting is an important symptom, and is generally present withinthe first few hours. Repeated vomiting after an abdom-linal contusionstrongly suggests rupture of the intestine. On the other hand, vomitingmay be delayed for some hours in cases of undoubted primary rupture.Case 52 was that of a man crushed between a tramcar and a wall;severe and continuous pain set in immediately, but vomiting did notbegin until seven hours later. Later still he was brought to thehospital, and, when first seen by one of us, he was already in a moribundcondition. The post-mortem showed a complete circular rupture of theileum. In Cases 2, 67, 75, 100, and 123 vomiting was delayedfor fromn two to twenty-four hours, but in all these cases pain set ininmediately, and extensive, evidently primary, ruptures were foundat the post-mnortem or operation. Of the 59 cases, early vomiting waspresent in 43 cases and absent in 2. Vomiting of blood is a raresymptom, recorded in only 3 of our cases (Nos. 28, 70, and 84).All these were cases of injury to the duodenum.
Tenderness at the seat of lesion is, of course, comlimon. Deep tender-ness especially is an almost invariable accompaninment of an intestinalrupture. In our 59 cases tenderness is recorded as having been presentin 35 cases and absent only in 2.
Rigidity of the abdominal muscles is of the utmost imnportance as asign of severe abdominal lesion. It was present in no fewer than 50 ofthe 59 cases previously mentioned and absent in only 4. Hartmann statesthat out of 37 cases of abdominal injury that had come under his noticerigidity was present in 17. In all of these a visceral lesion was found.In the remaining 20 no rigidity was present, and the patients recoveredwithout operation. Hertle compares the contraction of abdominalmuscles in cases of visceral injury with the fixation of the hip in inflain-matory disease of that joint.
A sign that nlay help in the diagnosis is that of added dulness,

Surgical Section1
especially local dulness at the seat of injury. Dulness due to the presenceof free fluid in the abdominal cavity soon after an injury generally meansblood, and is rnore often due to injury of the liver, spleen, or mesenterythan to rupture of intestine. It may, however, be due to the escape ofintestinal contents, together with peritoneal fluid effused as the result ofirritation and inflammiiation of that membrane. A localized area of dulnessin the immediate neighbourhood of the injured part is at least suggestiveof rupture, and is occasionally useful as an aid to diagnosis. It is probablydue partly to collapse of the intestine in inmmediate proxiimiity to therupture, partly to escape of intestinal fluids, and partly to htermorrhage.In our 59 cases added dulness was present in 18 cases and absent in 14.Of the value of a rising pulse-rate in the diagnosis of ruptured intestineit is not necessary to say much, as it is well recognized by all. We wouldmerely say that in the first few hours the pulse is often not abnormallyrapid. The pulse-rate should be noted every hour in every case ofsuspected abdominal injury, and, if it be found to increase steadily, itaffords one more reason for suspecting a septic lesion, provided that it isnot due to haemorrhage. But in manv cases of rupture of the intestinethe pulse-rate remains at or near the normal for several hours. The samemay be said of temperature, which affords but little help in diagnosis.
We now come to a physical sign of the worthlessness of which in thediagnosis of ruptured intestine we cannot speak too strongly. And yet,if we may judge fromii the stress laid upon it by certain writers, and theeagerness with which it appears to be sought for by dressers, housesurgeons, and others, and the faithfulness with which its absence is dulyinscribed in the notes of case after case in our list, it appears to beconsidered by many to be a sign of much diagnostic value. We refer tothe absence of liver dulness. It is true that this sign is often present inthe later stages of the illness, but as a sign of rupture of the intestinein the early period-at that period at which alone operative interferencecan be undertaken with a reasonable prospect of success-it is, as adiagnostic sign, not only useless, but worse than useless, because decep-tive. Among the 17 cases in our list in which operative interferencewas undertaken with success there is ')ot a single one in wvhlich absenceof liver dulness was recorded. On the other hand, there are several casesin which operation was not undertaken until absence of liver dulness hadbeen noted; not one of these recovered.
Perforation of a large air-containing viscus like the stomiiach oftenpermits of the escape of a large amount of gas into the peritoneal cavity.Perforation of the intestine only rarely does so. The amount of gas that
1.5
16 Berry & Giuseppi: Taumatic Rupture of the Intestine
escapes from the intestine within the first few hours of its rupture isusually only trivial, not enough to show physical signs of its presence.
l4felwna is of no value in the diagnosis of recent rupture of theintestine. It was not present in any case in our series. On the otherhand, in cases of partial rupture of the intestine, where the inner coats ofthe intestine alone have been torn, blood may appear in the motions,but, as a rule, not for somie days. A very remarkable case camiie underthe notice of one of us at St. BartholoiDew's Hospital some years ago.A little girl of 6 fell on to a scraper, striking the upper part of theabdomiien. For mnany days she was extremely ill, with great distension ofthe abdomen. She vomited blood and passed blood with her motions, buteventuallv made a coimiplete recovery without any operation having beenperformed. There can be but little doubt that this was a case of partialrupture of the duodenum.
Emphysema of the abdominal wall was present in 1 case of ourseries (No. 102); the rupture was of the duodenum.
Distension of the abdomen is one of the gravest signs of rupturedintestine, but does not usually occur early. Among the 17 cases in ourseries that recovered after operation there was not a single one in whichdistension of the abdonmen is stated to have been present.
DIAGNOSIS.
The diagnosis of rupture of the intestine rests not upon a singlesymptom or sign, but upon a careful consideration of all the factsof the case. Every case of abdoimiinal contusion should be lookedupon when first seen as a case of possible severe intestinal injury. Care-ful attention to the history of the accident, the manner in which theblow was inflicted, and the exact point struck may afford much help.Marked and persistent contraction of abdominal muscles, accompanied bymarked local tenderness and severe pain, is sufficient to justify an iinme-diate laparotomy in nearly all cases. The diagnosis between the ruptureof the liver, spleen, or mesentery on the one hand, and rupture of theintestine (or stomach) on the other hand, rests mainly on the presenceor absence of signs of hamorrhage. After all, the important question tobe decided is usually not so much, Is there a rupture of the intestine ?but, Is there an abdominal lesion sufficiently grave to demand an imme-diate abdonlinal section ? We venture to think that the diagnosis ofan ordinary case of complete rupture of the intestine can usually bemade with a tolerable degree of certainty within the first few hours ofthe accident. Much greater difficulty naturally occurs with those cases

Slt1g/qical Section 1
in which the rupture is at first incolmiplete, those in which symptoms ofrupture supervene many hours or even days after the infliction of theinjury. In such cases as these early- diagnosis often cannot be made.But all cases in which- there is a suspicion that grave injury has beensustained should be imiost carefully watched, and when the secondaryrupture does take place the symptoms will be mluch the same as thoseof priliary rupture. A typical case (No. 51) m-lay here be cited asillustration of secondary rupture. A m-lan, aged 57, was kicked in theatbdomen by a horse. When first seen soon after the accident therewas slight bruising over the left iliac fossa. There were no othersymptoms, and the imian went hoimle. Three hours later he returned tothe hospital complaining of great pain in the abdoiimen; the abdominalmiuscles were retracted and rigid, and the pulse was 84. Death tookplace twenty hours after the accident, and the post-morteml showed asmiiall rupture of the ileumii. Retroperitoneal rupture is seen chiefly inconnexion with the duodenuiml (Cases 49, 102, 121, and 132 illustrate thiscondition), and may be suspected when, after a severe contusion of thisregion, symptoimis of septic absorption occur without symptoms of peri-tonitis.
MORTAJITY.The gross mortality in our whole series of 132 was 115. Some
of the cases were suffering from other extensive injuries as well,some came to hospital when peritonitis was far advanced, a few werealready moribund when addmitted. Of the whole number 84 were sub-
mitted to operation. Of these 17 recovered and 67 died (see Table XI).Of those not operated upon, all died. Of the 47 not operated upon,6. refused operation and 7 were considered to be too bad for operation.It nmust be remembered, however, that should a patient with a small orpartial rupture of the intestine recover without operation the diagnosiscannot be made with any certainty, and the case will not appear in ourlist. Table XII shows what everyone would expect, namely, that foroperations to have a fair chance of success they mlust be undertakenearly, within the first twenty-four hours. The mortality would appearfroml our figures to be slightly higher in the case of operations undertakenin the first six hours. This apparent anomaly is, however, probablyex)lained by the fact that mnany of the very worst cases, in which dia-gnosis presented no difficulty, would be operated upon very early. Onthe other hand, mnany of the slighter cases, in which diagnosis was atfirst doubtful, would not be operated upon until a few hours later. Thepercentage maortality in our series works out at 87 2 per cent. The
N-23
17

18 Berry & Giuseppi: Trautmatic Rupture of the Intestine
percentage mortality of operations for ruptured intestine is usuallystated to be much lower than this. Thus Hertle's series of cases showsa mortality of 76'8; Tavaststjerna's 173 cases, 76'4. But these figures,we venture to think, do not represent the true mortality, since, as' wehave already mentioned, they are drawn mainly from published cases.These almost necessarily contain a higher proportion of successful cases.When we come to consider the mortality at individual hospitals, aremarkable fact becomes apparent, namely, that of the 17 cases thatrecovered after operation no fewer than 8 occurred at one hospital, St.Thomas's. Of the 28 cases of rupture of the intestine that occurredat this hospital, 22 underwent operation and 2 were considered too
TABLE X1-RECOVERY OF 17 CASES (14 MALE, 3 FEMALE).
Recoveries Operation cases Total casesRun over ... ... 9 31 ... 51Blows ... ... 4 ... 16 ... 23Kick ... ... 2 ... 11 ... 16Criish ... ... 1 14 ... 24FalI ... ... 1 ... 8 11
17 80 125
TABLE XII--RESULT OF OPERATION IN 84 CASES (BERRY AND GIusEPPI).
hoursafteraccident Recovered Died Total cases0 to 6 ... ... 5 = 27-7 per cent. ... 33 = 72,3 per cent. ... 187 ,,12 ... ... 8 = 53-3 ,, .. 7 = 46-7 ,, 1513 ,,24 ... ... 1 = 50 ,, ... 19 = 950 ,, ... 2024 ,,28 1= 90 1=91-0 ,, ... 11After 48 ... ... - ... 10 =100-0 , .. 10No statement of time 2 8 ,, ... 10
17 67 84
bad for operation. Eight recoveries out of 22 operations for rupturedintestine is a record of which that hospital may well be proud. Itis true that in 2 of these cases the rupture was only partial, but on theother hand there were 2 cases (Nos. 108 and 116) in which deathoccurred so long after the operation that they might almost be con-sidered as operative successes. We hope that if any of the St. Thomas'ssurgeons are here to-night, they will tell us more about the methodswhich in their hands have proved so successful. In the meantime wewould venture to suggest that the many admirable papers that havebeen written upon ruptured intestine by members of the staff of St.Thomas's (Mr. Makins, Mr. Battle, and others) have duly impressedupon St. Thomas's men the importance of early diagnosis and earlyoperation, and that this has contributed in no small measure to thesuccess obtained. As far as we have been able to gather from the

Surgical Section 19
records of St. Thomas's Hospital, their cases are seen early, diagnosedearly, and operated upon forthwith.
TABLE XIII-DURATION OF LIFE AFTER ACCIDENT.Lived Operated upon Not operated upon
0 hours to 10hours ... 3 ... 411 ,, ,,24 ,, ... ... 20 2225 ,, ,, 3days ... ... 20 ... 73 days and over ... 19 ... 8Not stated ... ... ... 6 ... 6Recovered ... ... ... 17 ...
85 47Shortest time ... ... ... 4i hours ... 4 hoursLongest time ... 26 days ... 10 days
Since the publication of the classical cases of Croft and Moty in 1889and 1890, cases of recovery after operation for rupture of the intestinehave become numerous, and the operation mortality has undergonemarked diminution. The statistics of St. Thomas's Hospital show thatit can be still further diminished. Is it too much to hope that in thenext fifteen years the average mortality after operations of this class inLondon hospitals will be still further reduced, and not continue tostand at the comparatively high figure of 87'2 ?
TREATMENT.
The treatment of ruptured intestine is necessarily closely depend-ent upon diagnosis. If a rupture is diagnosed, or even stronglysuspected, no time should be lost in opening the abdomen and dealingwith the ruptured part. If the svmptoms are not sufficiently clear tojustify this proceeding, the patient should be most carefully watchedand the surgeon be prepared to interfere directly symptoms arise. Inevery case of abdominal contusion the patient should, if possible, be keptat rest, and no food or drink given by the mouth until all suspicion of aserious lesion has passed away. Opium should not be given so long asthe diagnosis is still uncertain. Some cases when first seen are obviouslymoribund, and quite unfit for any operation. The question of how farshock should lead the surgeon to defer operation is an interesting one,and worthy of discussion. Most writers advise that operative interferenceshould be postponed until shock has passed off. We venture to thinkthat, if the diagnosis of ruptured intestine has been made, a moderatedegree of shock should not deter the surgeon from operating. We thinkthat in such cases it is best to treat the shock actively by means ofmassive saline infusions, strychnine, and other suitable remedies, andthen to proceed at once with the operation.

20 Berry & Giuseppi: Traumatic Rupture of the Intestine
When the abdomen has been opened the rupture is usually foundwithout any difficulty. In a considerable minority of cases, however, therupture was not found at the operation. This happened in no fewer than15 of the cases in our list. Of these 15, in no fewer than 7 was the duo-denum the part affected. This suggests that rupture of the duodenumis not suspected as often as, according to our figures, it should be. Prob-ably in most of these 7 cases the rupture would have been found had theduodenum been examined. It should be remembered that the duodenumnshould be exarnined both above and below the transverse mesocolon.
We are far from recommending abdominal section indiscriminatelyin all, or even in most, cases of abdominal contusion. It should alwaysbe remembered that in the great majority of cases of abdominal contusioncomplete recovery takes place without operation. But if a reasonablesuspicion exists, founded upon the presence of such early symptoms aswe have mentioned, that a serious internal lesion has been sustained, thenthe surgeon will do well to operate at once and not wait for furtherconfirmation of his diagnosis.
Into the various methods of closing the rent in the intestine we donot propose to enter at any length. The main point is to effect acomplete mechanical closure of the wound with as little delay as possible.Table XIV shows the various methods adopted in the 84 cases in ourlist. In the 17 successful cases, simple suture was employed in 15. Onecase recovered after the use .of a Murphy's button (No. 8), and one onlyafter excision (No. 3) (out of 12 cases). Treatment by the formationof an artificial anus was uniformly fatal. With regard to the treatmentof the peritoneum, by irrigation or otherwise, by drainage or otherwise,this must to a certain extent depend upon the degree to which theperitoneum has been contaminated by intestinal contents. In our ownsuccessful case the irrigation was brief and not very thorough, in spiteof the extensive effusion of intestinal contents. It is noteworthy that of10 cases treated without irrigation no fewer than 4 recovered. Withregard to drainage, out of 17 cases in which the abdomen was not.drained, 7 recovered.
We should like to raise the question as to the best means of treatingthe terribly fatal cases of extensive rupture of the duodenum. No caseof recovery after operation for rupture of the duodenum appears in ourlist. Indeed, we know of only one single case in surgical literature in whichrecovery followed an operation for ruptured duodenum. This was a caseof Mr. Godwin's, of a cab driver, aged 42, who was run over. Rents ofthe jejunum and third part of the duodenum (the latter being 1 in. inlength) were sewn up.

Suwqical Section 21
Mr. Moynihan's case of complete rupture at the duodeno-jejunalfold was treated by closure of the duodenum and implantation of thejejunum into the stomach. The patient recovered well from this opera-tion, but, unfortunately, the Murphy's button which had been employedpassed into the stomach and thence into the duodenum. Here it lodged,and caused a fatal perforation on the 104th day after the operation.
TABLE XIV-METHOD OF TREATMENT IN 84 OPERATIONS.Cases Recoveries
Treatment of intestine:Simple suture ... ... ... 46 ... 15Button ... 14 ... 14 1Excision ... ... ... ... 12 ... 1Artificial anus ... ... ... 4 ...
Treatment of peritoneum:Irrigation ... ... ... 44 ... 10No irrigation ... ... 10 .. 4Drainage after closure of intestinal wound 30 9No drainage ... ... ... 17 ... 7Simple drainage ... .. ... 6 ...
Rupture not found ... ... ... 15 ...
Of the 24 cases of rupture of the duodenum in our list, in 11 nooperation at all was performed; in 6 the rupture was not discovered atthe operation; in 4 suture was performed; in 2 cases a Murphy'sbutton and a Bailey's bone bobbin respectively were employed; theremaining case (No. 116) was the nearest approach to a success; itoccurred at St. Thomas's Hospital. A woman, aged 30, fell on to abaluster thirty-six hours before admission. At the operation a -ruptureof the posterior wall of the duodenum at the junction of its first andsecond parts was found. Suture being found impracticable, drainage-tubes were placed down to the rupture and packed round with gauze.An abundant bile-stained intestinal discharge toQk place, and the patientbegan to emaciate. On the sixth day a second operation was- performed,the duodenum being divided transversely and the ends closed. Posteriorgastro-jejunostomy was performed, but the patient died some days later.
In a case (No. 48) of almost complete transverse rupture of thesecond part of the duodenum, operated on by one of us in 1897, approxi-mation of the ends was effected by means of a Bailey's bone bobbin, butthe patient died ten hours later. In this case the amiount of extravasationof intestinal contents into the retroperitoneal tissue so soon after theinfliction of the injury was very remarkable. We are of opinion that forsmall ruptures of the duodenum simple suture, if it can be effected, isthe best means of treatment. If the rupture is too extensive to permitof this (and it often is), then the best course to pursue is probably that

22 Berry & Giuseppi: Traumatic Rupture of the Intestinie
of closing the duodenum completely and performing gastro-jejunostomny.Finally, in some desperately bad cases, packing round a tube, with subse-quent secondary operation, would seem to be the best line of treatment.
As regards after-treatment in our own case of recovery, the patient'sabdonmen was drained and he was sat up in bed from the time of theoperation. This is merely in accordance with the practice adoptednowadays, we believe, by most surgeons in their operative treatment ofacute peritonitis.
Of the use of massive saline injections, whether by rectum or underthe skin, it is not necessary to dwell, their value being admitted by all.We think that strychnia is also useful in the after-treatment of such cases.
Another question we should like to raise is, What should be thetreatment of those unfortunate patients who are not seen by the surgeonuntil one or two or more days have passed, and great abdominal disten-sion has set in? We are inclined t6 think that in many of these casesextensive operative interference not only does no good, but actuallydestroys the patient's last chance of life. It must be remembered thatin a certain number of cases of undoubted rupture of the intestine(especially incomplete or small ruptures) localization of extravasatedmaterial has taken place, and the patients have recovered with orwithout an abscess.
It is probable that certain rare cases of rupture of the intestine dorecover spontaneously without operation, but it need scarcely be saidthat this applies only to the slighter varieties of the injury. Theprobability of spontaneous recovery taking place is so extremely smallthat it should never deter the surgeon from operation in any case whichis seen by him sufficiently early.
In Table II of the Appendix will be found notes of four cases inwhich it was probable that a rupture of the intestine had occurred, andwhich ended in recovery without operation. For the first two of thesecases we are indebted to our lamented friend the late Mr. Harold Barnard.Both patients were readmitted to the London Hospital four and fivemonths after the accident on account of intestinal obstruction. At theoperations then performed the evidence of previous rupture seemed fairlyconclusive. The third case is one that has been published by Mr. Battlein the St. Thomas's Hospital Reports. In this case the ascending colon,if not actually ruptured at the time of accident, seems to have been soseverely contused that it gave way secondarily. The fourth case, whichwas under the care of one of us, was considered to be almost certainly oneof rupture of the intestine, the rupture being probably only a small one.

Sur'gical Section
A perfectly healthy girl, aged 13, who had never had any symptomlis ofa,ppendicitis or any other abdonminal trouble, was on the evening ofMarch 30, 1905, struck on the uimbilicus by the handle of a barrow.She imimiediately felt siek and ill and sat down for a quarter of an hour.Her last meal had been taken four hours previously. She was neverthe-less able to walk home. On the following morning she had greatabdominal pain and vonited twice. She then came to the Royal FreeHospital, where she was found to have rigidity and tenderness of theabdominal mi-useles and pain at the um--bilicus; liver dulness was nornmal,but her pulse-rate was 125 and the teimperature 99.50F. She wenthome, but returned again in the evening, and was admitted. Whenseen by one of us forty-eight hours after the accident she was extremelyill. The abdomiien was distended, painful and tender, with mnarkedrigidity of the miiuscles, especially on the left side. The liver dulnesswas absent ; pulse 130. The diagnosis of peritonitis following a smallrupture of the intestine was made. Owing to the very grave generalcondition, the distension of the abdoeimen, and the time (forty-eighthours) that had elapsed since the accident, it was thought that anyoperation would deprive her of her last chance of life. She was keptsitting up in bed, was given nothing by the mouth; strychnia wasadministered subcutaneously and saline solution per rectunt. For threedays she rernained acutely ill, then slowly began to recover, andeventually left the hospital quite well.
The prircipal sequelw of operations in cases that do not speedily dieor recover are to be found in various inflamimatory affections of theperitoneum, mainly localized abscess, and intestinal obstruction due tostricture or bands. Illustrations of the former are to be seen in Cases108 and 122, in which subphrenic abscesses formed; and in Case 112, inwhich a pelvic abscess formed. The first of these died on the twenty-fifth day; the other two recovered. Case 110 affords a good illustrationof intestinal obstruction following recovery from operation for rupturedintestine. The patient was a womuan aged 29, who sustained two
ruptures of the jejunuin, closed by suture six hours after the accident.Thlree weeks after leaving the hospital she returned, and was againsuccessfully operated upon for intestinal obstruction due to a band ofadhesions.
The conclusions which we venture to lay before the Society are thefollowing:
(1) That rupture of the duodenum is by no means so unusual as isgenerally supposed.
23

24 Berry & Giuseppi: Traumatic Rupture of the Intestine
(2) That rupture of the intestine is usually produced by direct crush,and not by bursting or traction.
(3) That the early symptoms of complete primary rupture are few,but fairly characteristic.
(4) That of these the most important are severe and continuous pain,rigidity of the abdominal muscles, and vomiting.
(5) That secondary rupture is by no means uncommon, the symptonmsin these cases being often delayed for hours or even days.
(6) That early operation is the only practical means of treatment.(7) That if operation be delayed until the abdomen is distended or
the liver dulness absent the patient has practically no chance of recovery.(8) That after operation the patient should be sat up in bed and
treated with massive saline infusions.
BIBLIOGRAPHY.
BATTLE, W. H. "Traumatic Rupture of the Intestine," Edin. Med. Journ., 1907, N.S.xxi, p. 493.
BRYANT, T. "Rupture of the Intestine," Guty's Hosp. Reports, Lond., 1861-3-5, vii, p. 35;" Ruptured Small Intestine," Lancet, 1882, ii, p. 102.
CAHIER, L. " Contusions de l'abdomen et ruptures de l'intestin par coup de pied de cheval,"Rev. de Chir., Par., 1902, xxvi, p. 16.
CAMPBELL, R. P. " On Rupture of the Intestine," Ann. of Surg., Philad., 1905, xlii, p. 661.CROFT. "Case of Rupture of the Small Intestine without External Wound," Trans. Clin.
Soc., Lond., 1890, xxiii, p. 141.CURTIS, B. F. " Contusion of the Abdomen, with Rupture of the Intestine," Amer. Joaurn.
Med. Sci., Philad., xciv, p. 321.DAMBRIN, C. " Recherches sur l'anatomie pathologique et le traitement des lesions de
l'intestin dans les contusions abdominales," Par., 1903, 126 pp.DEMONS, A. " Des contusions de l'abdomen " (with contributions to the discussion by
MM. LE DENTU, P. MICHAUX, MOTY, TACHARD, TiDENAT, DOYEN, FEVRIER, H. NIMIER,A. GUINARD, G. RISBLANC), Assoc. franc. de chir., llme Congrks, Par., 1897, pp. 68-166.
GODWIN, H. J. " A Case of Traumatic Rupture of the Duodenum and Jejunum," Lancet,1905, ii, p. 1108.
HARTMANN, H. " Contusions de l'abdomen," Bull. et rnmm. Soc. de Chir. de Paris, 1901,xxvii, p. 237.
HERTLE, J. "Ueber stumpfe Verletzungen des Darmes und des Mesenteriums," Beitr. z. kli.Chir., Tub., 1907, liii, p. 257.
MAKINS, G. H. " On Two Cases of Traumatic Rupture of the Colon," Ann. Surg., 1899,xxx, p. 137.
MOTY. " Laparotomy pour rupture traumatique de l'intestin," Bull. et mrm. Soc. de Chir.de Paris, 1890, N.S. xvi, p. 428.
MOYNIHAN, B. G. A. "Case of Gastro-jejunostomy for Complete Rupture of the Intestine atthe Duodeno-jejunal Flexure," Brit. Me(l. Journ., 1901, i, p. 1136.
Ibid. " Abdominal Operations," 1906.PARKER, C. T. " Laparotomy; Rupture of the Intestine; the Opening not found; Recovery,"
Ann. Surg., Philad., 1893, xvii, p. 590.PETRY, E. "Ueber die subkutanen Rupturen und Kontusionen des Magen-darmkanals," Beitr.
2. klin. Chir., Tiib., 1896, xvi, p. 545.
For full bibliographies see HERTLE'S and PETRY'S papers, quoted above, containing severalhundred references.

I -4-4 CD ro I - I TA 4-7 00 0 ra -4 0 ;j4.' 41 4, :3 ro0 -I C) 0 W-4 0
10 N -4a 4a "4 0 0C) 4) $4 00 0 0 -43 PA o r., CB - A
P, >-. Ca 0 %4 4D 0 0 0 0 - -N - F.4-) a) biD 0 o bo o0 -4 14- .Q (D 0Q -4 r, rA P4 ce 4D g 0> W-4 4) -4a raCB cn A 0 >0 Ca 42
4z ro 014 -4.2 Ca Ca 0 bo 1-4M 0 >
(D (2) a) 00 Pe -4-2 43 C) Go m o C9 -A (2) 00
IV CB 4.2 ce 4:)-42 rn10 0 rn
'04 rn7-4co
42 o6 0 -&2CB 4.4 P4.14A -4.2r4m Ce 0-4-2 ra -4Zra Cic ro CO 0 00 la) CD rcl4-21
(D rd 92 "..-O A o0 A'a -4 CB 0
42 24 Ct d C$ P4 $.4 Ca M &a IV " -40 .: k ce ce m 0
ro -CB r. ;.-4.rc$ .: .-,a ro Ped CB 10
rc 0 k9 Ca 0 0 (D
CB ro -44a -4-D .4.2
0-4.2 0 0 4a 0 Ca C) -4a 0 $:L4gi
'J.2to 0 Ca CB W co > ),4 0 0 0
C) 42 k ro 04 (1) CB 4-2 0 0 Ca0 CaP4 CB rrjCs C5, o0 CB Ca -0 0 bJD.-W (D bo-4 ro CBW 0 k -. k -4-2 CB o CB (DCa 0) ci 0 o Ca biD g o
> 0 .&O CB Ca 42 rtzP. 0 Q) 0 0 'a)
4) > x p k P 0 ;.., . --4 0442co IV -4 P
00 k 4) 0 a Cs . Cs 4D A Hoo Cs P 0 4-2 P4 P442 tOL, (1) Ca Ca P4 4)C). 4a42 rii 42 biD 05 . rt, .0Ca .'. -0 rr. (1) ro C) (L) biD cD 0 'O 4) 0
Ca 45-4 aoro , 4) 0 ;64 (D -,o t- 1 4 CB;..j A 42 to PbD C'D - . 0 0 C4q 0 Ca
0 4a A N P4 o ce m o >0 rzz$ a) 0 0 0 4w (D42 a tn Mr4 4) >. - ;>CB 4a 0 cq..4 e . 4* $4C) .o 0 0 0 M bJD.,, 04a 0 Co P4 0 CB 0 rtzrn CD P Or. Ca r.d 0 kPA biD ;,. - -i :5 'a)
o A o 03 ;-4 -w Ca 42$4o -4z 0 0 Ca $4
rd ;-4 rdro 0 P ;.., (D0 0 0 .k -;i 0 (Dro a) 0 0 rd ra o $:4 co0 'o Ca 0 $:4 0 Ca$:4 ;-4 42 4a 04-Z 4,2) 42 Ca
0ro -14
f)4. .La 00
0 Cd riz0Ca k 9
+D 4) 0 ce CD 4)W4 10tg 4) ro
0 -4a $4 0Ca ;> 00 O.0 Ca Ca P4 (OD .Q coz rd -+2 (D
0 PT4Cd-W cr.
bll. r--l
4-a o r'-i0 0
0C) C)
0 bbm P4r-4
0 4a o6'r4' C,1-4
,w bom P-4r-l
coz
0 0
0
z

;-40)
00:39
ci,CII .o
a)4) 00p V-40
C-1 CO(D m00a r-iO.-z6CII c0(D (M
co;3 r-40.-z
:.i-C-1
m
P-..00
to 14) 42 --4 -+..) 4 0 k 0 40 E&aA CaX4 $4 0 04
+3 Q) ID _4 -4'2cn P4 P4Cd o $40 12) 0 0) -0,0 0 0
42 0O 4) A4N N42 (3);j
Cn -4-2
0 42
%-4 P4 0 A0 Ca t) C) 0
Ca W 54
di 4202 O Ca. (2) (a) P4 P444
di o ;--, 0 V0 0 42 P' S-4 0PL4
0: rn-4a q) k 4zcd 0 42
,a§ 2 ca)
Ca 0ce Ca
42 -6-20;-4 Cd ;-4 42 ri oP4 ;4 0 -4 ;4 CD $44- 0 4D 42 0 0ce -4-2 ce 4) 0 4) 0 k -4.2 0,0 ceP4 $a4 W P4A r-d 0 0 Ce .4.4 420 - ce 0 0 42 P, o4z CD r-4 O'" -- O -4- ro0 ;-4 S-4 .a
0 P4 O* 10 (D T Ce 0 4)(t) 0 cq co cn P4 &4 CD A4Z 00 0 42 oCa Ca
0 o 0
42 0 P4,..0 4-'2tko Ca o (D P P4.4'0 4) ce 42 Ca 42 0 tn0 cd pLI-4a CO CB P4 CB Ca
CD 42 'a) ra rn riZ (n CD%-4 ;j riZ 1.4 rIZ -4
-4 m Caro ro M 0 A4 4) 0 0 o 0 ;-4 Cd (DCa -0 ro -4.2 Ca 0 -4a Ca (D40 &Q CD 0 P40 42 Ca er o ro A
42 04 0-4 Ca(D ro P4 0 'a r-C -.4 0 . rtz ro CBdl 4-D ,4D co ro CB .'" EL ;-4 4).2 0 -4 0 4)rd Ca $M4 -1 ro 'a) roCa 0 m 0 .
- ce P4 0-4.2 -4-2 ro0 -40
0 rd -4a Co CD 0;-44) C) CB 0 w
0 cr, 00 -a (DA (D a P- -4 Ca-4 co wC) 0 -4 P4 4-2 0 A CB co :s0 0 0 Ca 0Ca rl 't) A 0 P4 bop$ ;;.. (D bo O (D P4 0 45k-0 ro0,
M -4P' 42 OD - P-.. 02 A C! ro P4 -rd a p4A 0 0boaq k (1) .4 CO M 0 r-d 0
rd 4-2rn -4.2 Ca m o CB 0 rd ce 5 42 &4
-.4 0 0 4)ro 14n roo ) ro (D di C)
0 rc; . 0 d W C) q) (D P4 CB
03 O 43) P. C)C 0 0 C) P4 ro .3P4,0 (1) CB 42 (D a) -4 P4di rc$ > C) -" 4.2 ro rd 4a :3 m93 > cq r-O 0 0 -..4 P4 1.5 .5 -- 4) 0 (ID
0 Cs -4 0 Ca Ca 4D 0 -4.2 -4.203 rt:j rci...4 10 .-O o CB CB 43) = w C) 0 A4 C) m C) rtz -4.202 42 C) r-O S-4 , O 0 (3) rtz (D CB 0 k
L- $4 ,di rd C) -6.2 _4 ;3 - ;j C) ro m 0,0 CB - -CO rd rd-4 C) CB C) 0 Ca rt:$ 4)0 > %4 0 -4 co Ca -4 (D 42ro 0 ;,j ra ;4 ro.-O 1-4 C's06' ro 4) CD (D p, Ca CD No a)CB rd -4 -W P, Ca to 0 42 0. oto 0 J%4bo o o
rd 0 CII ;-4 -4-2 ql -4Ce P4r-q Ca C)o 4) 0 C, P-- -4 ..2 0 m kCa -4.2
0 0 P:4m 0) Ca !4 6rrs P4 rn 0 C.) 4
> -&2 0 ral :Z rd -4.2P-4 &4 -0 &4 .Q 42
0 C-d 0 - CaCa0 as 0 0
P. f-4 4ar. t ;-4
Ca 4-4 42 ce0 4-PL4
,4' C'I MOD cq4 00 00O $64
04
C4q 00 M cq M
00 4 00 00 CB 00P4
17ZCs 6 ctli
cq Cqcq com m -4 ;>.,M P4>1 00 00 XO00 00
ci
cq co
co 00
c) 0
0
C) ~~~~~~~ce
Ce ~~~~~~Ce
. -4
1.-
G1)
C.)
ro
.d4
C)~~~~~~~~~~~C
aq ~~00OCe, -Q,-4
Ca p~~~~~
cq ~ ~ 0q
cq~~~~~~~~c
CaC)
C)0
x
00 I mi
m I eo
C1)
z P
0t 0
6 0)1z
-4 0
Or-0
0C.)4 ) g4-4 °~- P O 0 5DV
5.o ' og
0
0
0
0
0
~0
400
c3
0
dAO0_
. M0
(D0:O
0 4) A 2
Co
0 O*- O O
° oD
0 0 0 0" Q) bjD-44~. - 4:) 0 a)+ .44 1 )-4-3 Q Ct X X ~~~ t t lw wW~Ca n A CawH
o~~~~~~~~~~~~c o- P4 -1 4z4¢00 +4* i 00-=
- ~~~~~~~~~ ~~~~~Ca 42 cz -4. 0qbcM
to n o Q o So wo-4z oQCa-- co
~~0 0 fr0 00 C0
cq CiWq cc
P.O .s 0 OO 0
F V ~ ~ ~ ~~ ~~~~~ mOm
0a r-
ciC4 oc CIIQq c
40 0 b
CcCH UCS CP4~~~~~~~~~~~~~~~~~~~~~~~~-i

I Io .3m rO eoXo Ca
4P
cq.0O
cs 'to.-o
Cll0
cq C
(0CLCi

p 0. --I
04'a')4l P&
0~~~~
c.
0a c0
0;._ 0q n W n
C.- . -
4
ce -4 E $,o P, A¢)
,0
0s4
o40
ceL-.
0)
0
0
E4
CiC~Q0--
;j04
006 ~ C3 )W '1J0 Ca
0 rs o rci00 No o
o o
~-4-44 0-C11 C at-4la O)OO CO Ca
0 c,3 0
P4~~~~~~~~~4O
00 00 ~
rCO 0OCO CO Y)
>~o 00 00 P,0H co cq C
O 0 0 0
CO _
04 0 04 0
rc _o . _
C0 0 CS C
'44 uA
4)00
,v..--4a
P4 fiEz ,-
rn-
(L)9 0
a
-0
.4w .
r-4
OO.Ca
0; 0
Cd c0
I.-,,R - .4 Av

O ~ ~~ ~ ~~~~~~~~~~;P;
o 6 6X-
(D 44P
0
o Ae
03 0
0Cez422
°d --) - - a)*-26fd A 041.
Ca
Poe~4a)In
Co co Ci ) c) Q0 A4 o o
o Coan cqO cq0o
X~~ ~ ~ ~ ~ ~ ~~,Oi:¢ Ca
00 C~~O c0 a
0( OC)~~~~~~
Ca
6~~~~~~~C
0o Cooan SC
Co wlC~o .q0
z
0 0 0 0 0
- 00 O 0 O-m CaCaCCo

-4 -q
_q~~~~~~~ m
4- Q W
CB
CD
4.4 0(a)
C, C
-._
IL4 $4 0 P-
Ce CeWO
._,Cf Qe
Ce
^\,z2 Ca
Ceo - 4
wCe --
CL)0
CD._4
cel
0a)a)
_ 4AS S-S.
P44
0w04M40Ce
04 H0 En
a0 Ca$04Ca
W~ W0,CC
$C44a
Cae;,c3 5_ A
54 %54
;e40 ;i40Cd -4 (a d R w4
P4 °Ji5
W
Ca C4 O
C0 C.)0 s
C3 Q' >) <o~~~~~~~~~~~~~t
D 3-~ g . 'D)t E) o -;
4 P4Ce -4
.
0o ceC,
0Ci
Cli
a)
O*a) aC) 5a) a)- C)- 0-4 Ce
~-
O Cl -q 1- Cl ol CQ0 O O O Oa) * a) a) '.4a a)
Ce-
Co--q0
04-
A
Ca
g O c3
4D P04 0 ;0
'1ZCaCci
-44 04
5P C5 O
o oc
-I04
0In Xj
~0 0
OC,cn A
Co
54a
0
co Cox
.0
ce c
.)o4-3 4-
- - ~~1 - -
o 0 0 0 0 0 0
0 0 0 0 o 0 0o 0 0 0 0 0 0
01 Co 40) C.0 L- 0Co co O o co o co
N-24

,I ce 4 )
0~~~~~~0
o4~ CIOC0a) 0 -0
P..'Or:
a )4C) ) a C ) )o ~~~~~~~~~~~~~~~~~caC) rd--t a)a "I
C.)0~~~~~$400 40C
a) P4 0) r
pJ)4a~~4a
c3 0Ca e,.a$)
0 0 $) D
0 .40-42 4-J
CoC)AE
40DC0
Ca- co
Ca
c3 ~
AoO
rg..^ z
, Ce ;-
0
0d
4:-eq CO
bCo
C--ece co
-cn
CD Cw0
I)-
C) Coo
4DaA 64
04
402
) 4C
X4
0
4')0
* 0);d CCe
eq .di* 0),_O
-~~~~~~~~~~~~ - -14
.4 1- cq0 O
m 0 0
o 0 0m I4G 46 0 0Co '"4
P d
Ca c
C40
Co0
Ca Ca
0
Ce
,0~~~
$40
~ 0
oo
1-4
a)
.0
bo
de IM k
P 4._4
o 0
Coa)
Ca
Q)
._
0z
co
0rrn0
a).0
o C
a)
0
eq0
'-4g-C0!4 -
U: C
O -4 o
--4 ~ a
¢-X
4- _4
Co
E- O
0 0 0
o 0 0
q ~ q~
-iH Cq Co'44'44 '44~~~~~~~~~~~~~d
C2)
CL)
C.
0
G)EtlS
E-4
m
.0
10Go
'c)
z
40
0N
C)
0
'0._
CC
-._
'C)C)
L-.- J.,,,
.1 -
_~~~~~~~~~ "I

4.3 to rA I r-d -4 q) rd 0 0 49tko J., 't Cs rC5 P.
-4 0 .0 0 N --4 t d 0 d,0 SCB ce w Oo 4) 0 k 0 0 k k rd 0) -1.2-4-2Cs 0 0.Ca 4-7 to Ca42 0 04 (D 4kl- $:W.,, 4 42 rn co-4-2 -14 4) v 0 W 04-D o 0 0 k -q -- 0 k UD 0.944 -0 to) 0 0 rtzi 4-) 4) 0 g3 rcs riz 1-4 42 W A 0 0
.,-4 k 14 rA 04) 0 rd a ,,, 0 0 P4 0 -4- 0 -1.2 k 44 4D 42$54 k W 4-. 0 0 .W - 4) 42.0 CB 'a) b]D'4 0 (D 04 0 (1) (D k (DCa a) rcs $4 rd 0 0 I.d P4 -4.2 0 (1) N
(1) (I)IO Q) ,;5 _ CB P4 4. " 0 P, k 42 0A (D k Wr-4 rd -4z -4-'i 0) rd o A 0 0 d99 W 0 rA 4a W 'D 4P ;-4 0 CB 4.1 P4 0 0
.,q ro T) t) rc$ $4 4) ._4 a --4 k rd 0 -+2 Z rd 0 Pt -i-2
4.409 05 CD CO rd k rdZ 0 .4.2 > tq '"P4 P4 $4Z 0 F-4 Ca P o -4-2 O rd IM4 bo
.._ 0 0 0 0 ;J.0 0 0+2 03 o -4z 4D rd 40 co k 4;) 42 Ca C) P4 7-4-4.2 ce P4' CAD W Cd -4.2
E-1rd0 Ca -42 ce -4-.
rd
C02 CD;-4 ;4 CD
-4-3 4m2 42 4.20 410 7-4Q) ;-4Ca ce ce Ca C) -43 0 030 4.2 (1) 0 Ca Ca
Ca rdrd
.13ce 0 co
0 rc$ Q) (1) (n Cn 42 CD (1);..4 ce rt:$ s-4 rn 0
7-4 f-4 S-4 (1) bJD L)C) a) .= ce L4 0 (OD
0 0 .4.2 -4--l ;-4 -4-2 ce04 0 P4 W 0 C) 90 r(Z 'r4 P-4 0 4-0 Ce -,-.
Ca 0 1-4 0 164
.,.IW
k0 &4Ca o
'd rd o0 0 Caco 0 CL) :jP4 Ca0 0 $4 0 Q
-4-2 0 -4.: r,::$ 0 'a) 4) -42
0 -4.2 1.4 ;-4 -4.j CB
ce ce 0 ce 0 rd CDC) 9 0 .1-4 ;-4 rc ",
rd
ce Ca la W 0 Ca bJD k 0 ct 4D -.4 7. 4 o kw
P4 (1) Q) " .- I P4 (1)ro
0 0 0 P40
0 > 0
Ca 0 04 CB -4.2 -.4 rn ce 42 4a 0 $144-2 P-4 P4 0 -4.2 -la 0
rtz 0 4a P C) CD rord s. 0-4 0 ce ..- 0 W o co P3 -, - 0 O'
4QM pq .
bID 0) CD 'o 0 Cag rn
. -z .z 0,Ca
P-40 z0
0 0 rdv o cd 0 k 0
C) Idq (1) $* 4a
P. >P4-- Cd O.. CB
(b, Ca A 10 Ca 04C) O M .l C40 ro OW 0 00 W (L) Ca r-I 0 ra
P4 (Dask Ca0 0 C.0 rxq a) 0 CB
(D 0 Q)0 'a) rcs !z Ca 2, k 42
rd Q) L-40 (D r-4 0 0,0W .Q0 W r-i .62 41a
42 ro rdCa Ca Ca g3 -4
rd W 0 > 00 b.0(1) Cd (D Co -4.-
$4 -4.2 Pro . ro k A $:4 $4 -4.2
0) -, CQ 0 a4 rd 4D 0> - W cn
Ca a) .-O 0 cn 0 P4 +2 co ro 0 0
0 ce W to -4- &4
0 rd C) 4.7 .a 42
.-4 $4 7. 0 0 a) (2) k (2) bo00 Cs
- 0P, bo C) P4 CB >
C.cq (1) - P '- . .j . -
,W P4 mrn 4.20 42W 0 rd
Ca 00 4,1 0 g k
rd a) 0 42 (1) 0 Wq 0) Cs
Ca Q) (2) ra rcs 14C) I 0'- rO CIO 42riz ro 0 C) 4z 42
(D> O
Ca bo,-.4 -.4 42 Ca CB > ol :;4 k d
Ca rc$ ;.4Ca
1.4 C'l -4z
4-. 4)>
rd 0 0 00 14
-4 '0 0 4- 0 -1.F-4 -0 4) -- P-4 g ;-I Ca0 Ca CD 0.. 0 Ca ce
0 0 4- P4
CTCD C.0 r
0 o C)00 00
04
C6 cl. cq
C).l: 00 -4 00 00
r.-4 -4 0 r-I 164
z914
co C4,to to cq to
C) (D C) mm (M ;; 00 00 OC)
r--q 0 r--4 ;-4
z
re;
toco r--4
0 0 0rd ro
ce 0)
0 0 C) ;-40 0 44.4 PA
VI xo 00
-d4 -di

Iq .4- _ -I a, ) -$-
d z CaRo Q0ce~0
0 '20
0 a
c o.*0
-~~~~~~~~~1ci
0
Cq
0~~~~~~~~~~~~~~~
P40
0
.-
34.Ca$-
-6aJ ce Ca .
Ca Ca0°4.2 0 0
r 04
P W,0~00 z
-oCi 0
-1 eq
0Xz I°

i '-E I-m1.3 rc _3YiE33 mo "I- m2 A~~~~~~~~~~~~~~ 0W+
_~ Q
0~~~~~~~~~~~~~~~~~~~~~~~~~~~e
r
ca
.42 ro Ce $4 164 .4.Ca r
~0 '- ro
CD ..a..
r: Ca -O rt:
C='DX CzcoD
-,o42 O
~ ~
,o3 -ed.3 CB*e@
tQ~~~~~~~~~~a)
o~~~~~~~~~~~~C Ce &
0 00 00
C)
*
C,
cq a,
.0,b4_4a
p4-
>
P14
-_ ..
00 ,
0OQ 2 Dp oX r. Ca Ca
0,a,
cq ~~~~~~~~~~~~cq
:.i :2i
--w
cq
o
40 .2~~~~~~~~~0-i 04aa1- o
o0~~~~~~
o4 0'*
,0
4 4
0on
r, r.4
C)J5-C6_
oO
0
'occC,, 0
,14C
Ifo (2) I-Cl~ 0Ca -4. 004 z
-
eq4
0
cq-z
or-Y--
eq r.
0ci-z
X6 c,
q
00C
00r-
CQ=
0o
- Y -
X6r-q d
>4
04 ,
00 I Si Si S4) co qc H
LI I 2imz l Ha C3 P
1 .-4)
00-0 0L .,
a,20
00C3A
,s,,,
aw
A o)
C.0
' 0._s
C6
-r-40
P. P- C02jz l
C)

a) 0
*0- c0
a) C
> Caa l
4 0
a)
0
2C)
._
0
z
Caa.
0k
04
ce e ew (1 la)
0~~~~~
80 0~~~~
~~C
4--
* -~~~~~~,
Ca)Cw-4 a)E 4C
cn ~~ ~ ~ ~ ~ ~ ~
0'- A
0 o cn~~~~~~~
4;
o~~~~~~~~~~r4) CD SC
Cagr4 ^ q
°) (1D a2 X a)s
0 :
L- Co eql
z
0L 40-S.D C
ma)0c 0PC r4 __r-
0
0
-zc3
P"400
cn .rn~4Pt4 laJC-4
$:L
-4m
-'4D
OCor-
40
-z
4; 3)a)2-.2 a -4- 4a
Ca CQ I Ca
4 q Co
u:~~~~~~~~~~~~~~~. e C.0e
C. coe.o Co4r

0amo.~~~~~~~~~~~~~~~~~~~~~~o
~~ ~ ~ -4
0,
S So 43 w
E;Oe cY'e4E1-
c) a) e X,)
-4 C) ce 3d
:^ e e r
C)0
eq L-
.C6
66. -
0o_a C)6 r
U-4-C-~C

062 00
'00
0~~~~~~~~~~~~~~~~~0~~ ~ ~~c
0 40()--
ce M 0~~
0 C~~~~~~ ~~~ .~~~0'a-4
0 0*~~~~~~~~~~~~~~~~~~~~~~~C420CP4 'o '.4~~~~~~~~o 00~C) 0
0~~~~~~~~~~~~~~~~~
0~~~~CoCO ~~~~~~~~~~ 00cA
-& P4 rc$t4. 0 )0 C a 0
o 0~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~Co%
02 rdr 4 F44
cq00 eCs 0PCCCaO00:
0 6~~~~~~~~~~~~~~~0
4) r7c$ co CO ro 4) Co -4 k ~ ~ ~ COC
0- 0-~~~~~~~~~~~~~~~~~~~~~~~~~~10-
0 ~~~~~~~~~000rd Ca ro $,4 bCO O

4z-
~~~Ca a).14 Ca to
r
~ ~ a ~
a)cia) 'a) ca Ca
4CdrO0 "0 Q
-6 e. - 00 b J;Ce Y ;" -4.A a)
a) &4 .,-'D0oa)aP.C)o)..o Pi~z c
a)Iw 5,0 X
a 00 O
+2() +2)__ ¢CC) CI
; a; 1-.So S-4a Oqa)
_a
Ih
I '~~~~~~~~4 -I
4) ~~ ~ ~ ~ ~ C)
Z;__ I zOX0 0 m 0f
-4-_ 2 .
6z
90
ca
a2)P400z
0
S2..z

CC-2 ,-
04
o . 'eC)
cn ;~~~~~~~~~c
Ce
#~a)'Q
X ~~~~~~~~~~~CCC)
I a 1%~. . I ) &a 0
a..9 o.,-z ,2 0 42 CB°2i._~~~~~~~$
-4 Ca m 42C
~~ Ca ce--.
~ ~ ~
C)C CsV> >~~~~~~~~~~~~1
52fc i
a) 0~~~~~~~~~~~~~~~~~~~~C
4S P4W ;E to 0
40 m-{~~0 sCO0~~~~~16 4
Ca la)a
r,-4 ~co
-o~~~~~~~~~~~~~~-
Ci O^~~n IaCo
,-4 r,
;',- Q) (1.
-U' 0- 0-
;,
.4- 1 P. 0
i~~~~~~~a sH0s ° * Q~~~~~C
03 EC (3H .
05 o 'k Ca 4 05 la~~~~~~*~~~~~~P -14H
, c12i2 CC*C **0 ~ ~ ~~~0 0~
CO XO 0: Cri 1-4 St_ Cn $4

II a . 4
,Q XXA o
cno^
c3p o
C)
o6z
-- CD-.!I
0
C >W_r) X l)
Ca' C C°C
ci 0~~~~~c
C~~~~~~~~a)~~~ ~~CCO,..C^g
Co Aoo00)
Co~~~~~~~~~~~~~~~~~C
00 1)O0CO ^- 0
cocD ° 0q
oQ6 m
CO
Q) -
C6
ea -ri2 CX Oo Ca C0c 0 0 o0 0-
1 4)4 404 4)PA. ) 0 4
Nl co OC000o 00 CoCo
oi. o $ 4 o 0 *4o40 0 C
$07 c3e$D:4s
CsC
.0
0 row
CadO C)
DCa 0V O
0
Ce g
0cr-
s0
~ ~
Ca -4 0'a)
O 0 42~~~~e
I:-
w0en
0)
7

a) D nIe *naC)
o: fCn s.4 °A-4' °- Ca M0 PZ °4 Cd CDzV0
&IQ
P4 o o
Eq --4
0CCd.
p.,Ca0 ce0 b.0 O
ci..;4 - 4
o *zv 0p c3.00
;0
C-
1c
Co
oc$C) -4,0
-4
0
Co
o-4
Co
co
0
0: ~
Ie - -
0 0. bD w
CD CO 0
0 0Co C
P CD a)* -4 Ao
S Yo Y:CO 00
aw )
ceg3 0
0
0
Ca
'a) '.
A 0
0 A
-4
4) c°
P
(ma)r-I~~~~~~~~~~

Ca)o
Ca~
o*Z P3.'.I a
A4
A- >A
a))0r
i4A3d -4B
o E
Ca
4) C)O
C co
s-I
co
OD

a dCCL
0 40$.4C
OC) .. bjD
C)0
~~~~~~~~~0
A )-4;14
¢i,
CQ CO a o
,4'~~~~0 .0
oo ~ ~ ~~~~~~~~~oa)
C14CO -
o0 ~~~~~~~~~~~~~~~~00
E4
Cl)0H
FI
NO25N-25

00
CD la).+
C) O) g ,
o
04
0
0 a -ou0e.
--^ * ^) ' p.
ce
C in PS P4XC0 14 Pi
ce g
0 c
00*4
eo 4 C) ;g
-4- =;
. ...Sr
z *__
;e 0
Ce~~ ~~~~~cO ed O0
az ~~z
Co Xo
0
CoCOr-
0CCo
C6
4o
oq

W 00 c- rnp4 0 0'
CB~
L-
00
a-as4
l xo -e s o-4 04 ~4;l4* 4
A, p * o £ 0
I:-c0
-4Q9U'I
60
E-4C0
cd
E-4r-
cO-a e
E-4ci0
-
:4m mNdi r-4
L-m00r-4
t-m00r-i
t-m00r-i

0 .,0 0 ! ~o0
) ro
-4z 40CB~
0
0.
V-
Co
cn
H9

0)0
0~~~~~~~~~~~~~~~~~~~~0~420Ca~~~~~~~~~~~~~~~~~~~~~~~~~~~~4-
e0 o r
;, ()CB0P
0a
C,a,
a,
00
OD
00
ri
Eqto
00CO
a)
0,a,aD
'-I
CD
c0
00
a,
0,
a)
'-4
a,
0,
0,
.
00
'-4
EC~o
o

. -I
' o1 ;> <D
ij
RI 8 f
c3 0 Q q) 0
10
1
Ca 0v
r=d
0
Po0
C zSoW n
() c
0~~~~r;cee ;-4g rO
CO
- C5-4 00
c14 i,) 0 ~ QCP4-4 0
0C
r-
:2i
CDfi
CD o
E-A?

'e 'e0
ro
¢ Cr -C xC4 n o
CDm *
0
~~~~~~~~~0 c
C0~~~~~~~~~~C
0~~~~~~
az
a)0
r-
aoCz
ODc34
* f
Eq
Pi
I W %J 'S4~0 0 .,-a) CO 'dq 44 c
0
'-4
0
ci
'-4
8 °a
r-
.4.
co 0GQo
'-4001)
'-40
'--4
0'-4
oq
'-4
aS* s
GQ ,
C)

Ca
0
a)a)04)ba)c
a
Na) a))I
00 0
4a
~Ca Ca
a)4a)0Ce H 0
(a =O
I_^ 16,I.S
I- a). 4 a)~ -4A
I ~.0a)
a) Ka4'>-4r
~ c
CeOQCe
0 04a a
CCaa4- o 4 $
-42 ( -t a 4 a) C.
da E4
.4,a Ca C *
a)
a).-.~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~
0 O
4z0 00e
eW-
C)~~~~~~a
0C
0~~~0 j jD
oq0C)'-4
0 r
C)
0C)'-4
oq0'-4
'A)ce
rn
F-4
* 0Ao
4S 4la 0
o 2v0 '.
a)Go
* 4)UW _
0
0
la)
a 0Cs .-,- C
Qa
Pg48 °E0
o .Fa)r e
,0
nIae
P4Ca
)PO0
0o
la)
0
4.'. 4
0 .
z .2014.
a)C)
eazI--
04*P0
zoI z
0C)
'r-
z
rI oAIp
" "',-
L.
I
I~~~~~~~~~~~~~~~~~~
I.e%
10 .. 4 M $44-2 ce 0ce0 (1) 12) .-4
-+4 -_4 +2 -4-D a).0. o 4-1 P4 "ce ce0 4!.

ClI~rl:
0C)
t=42 RvD0 0 C
eC)
cC 0C)Oo . ma0 0 1
O tO-cC040$4%~0 P4
0.!oe0-. d r
0cC0 ~~~
CQ X al S ~~~Ic3 CO *
4.40
04 ;4
-4~¢-r-Co
H CO
*oiO C
C6.0
CdcC.
C)) Ca 0 cC
WAB
D
ce3 e
_DCC
04.0 412 0 CB
P41
CD
CC-C4su
P4
0 CD C-
co cE C0
C C C
co L-
Ca $ QQC1) 7.
cC°;C n 9
4.l-
-
0 C
0)
01)
'-4

-~~~~~~~~~ 0
0 ; ._eh4(
. ro Cs Ca° X*
ce Cac
C/ | Cf) 0 me
Q Q) S. q s. O
o 0-
riD
0o
-~~~D 0
0 5
o°o0r°
oc=Q o.r 0 d
a s ;4 s
P-D P-. t_, P B r
-o EB -,0 ` P.dN 74 c
*n fU*-) ^ C
Ca 6zr- -CB ."Ca O- OC
.0 >
V-CaoCC' .)
Ca r00PC0 CO ,,0O ~~~~~~~~~O4
ca _1 r- _.I- C) ." Ci
I cn o.0 A (Ca -4 -4 W C =r-~~~~~~~~~~r
r.ot7010003m
.5
0 .5-E
bmI
._
E
4z
I._C)C0m
oE-4
V-- C-p,.,
6z C4
.i- 0 $4 .-4 * " -+*.
M
n
A,Ca ._.Z2 0C
0
0
-i2
o
4)
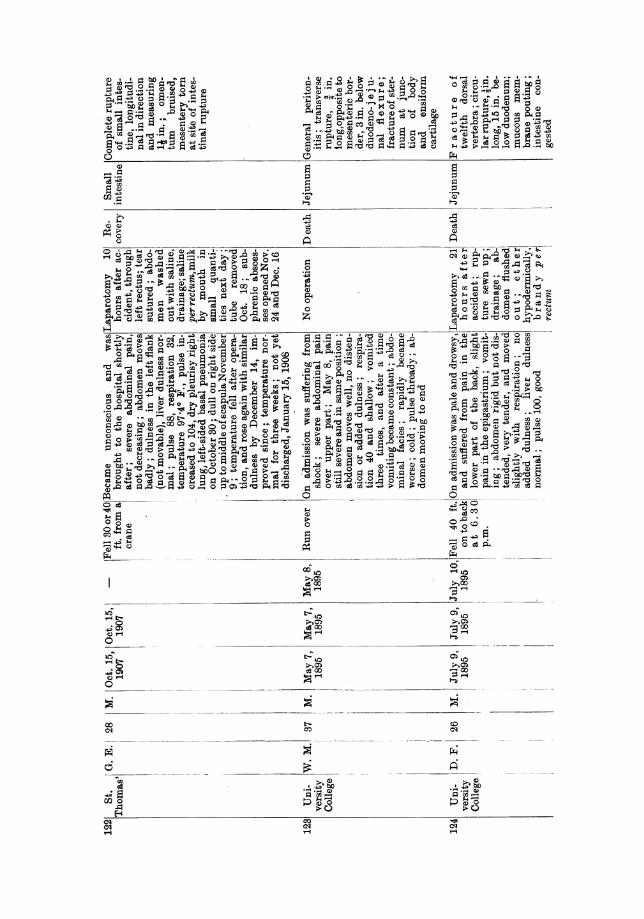
0' '~~~~~~~~~~~~'''~~~~~~~' so~~~~~2 *0 'b''S.--I 1P, I.-I-I
0 -14 CD Q) 0 ea) "4-D 0
0 i
o a 0 4 r
cII~~~~~~~~ 0 0~0 O O C
o * e e C --I 0 ',r
o __~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~42-4, b 1
Ca 4Q " g ~ ~ 4 0s
0 ~ ~ ~ ~ 0
Cd -40"a, 0r g0Ce
Cd la)riz ce 0 0-~ 0 Ccex
Ca w w
0 42 (),,0 ( 0 00Ce o,4 0 A~~0 0 Cew-r-z 4z
ow 6 Cd D -W 0CB 40C
000 Otr 0Ca C 4
0Ca~
4C ~~ ~ ~ ~ ~ - Cea C )-~-80~~~~~~~~~~~~~~
0 Ce~~~~~~~~~~~~~~~~~~~~~~~~~~~~~ &
o ~~~~~~~~~~~~~~-4>- o )o
C,
Ce-aO Ca $ ~ oo 14r
eq Co~~~~~~~~~~~~~~asw'eq eq~~~~~~~~~~~~~~~C:4m~

-iz 0 C.) p4
Ca 'a)C~ -4-EC) .4.2 Ca Ca~~C
CD~~~~~~~~~C
r-O - a) )U4" ) 444).
d erAc,oC c icC
4+
c3i q P
. 00
D P-^^^ O* :q>
C)0
0z
I:-
bO~
'-4
. o
r 8-.4
;4 4
0 (14-Q =*x-ta -4
c340B 84a
00 )) 0)-
00 m ao
Cx

I t'
Q)i r
IAD
0~~~~
;-4 0 00 4C.
C.) d P4U P$
rd.
H ce r3 oe o :3O-4, . O 0 W o Ca C ^-Oset =
E0 .4.°2 .,- 4 s EXm °B°2 m 4 m_ 2-.*:: ;
ro Ca 0 d , c c3t 3 *6cna ;c0AOm 3
4a Ca
44a0
4-2
7 ai r
0% co $
_i_ Co_____________ CC
ci,1 Cs '4 c as 00z.°
b ~~~~Oa
>0 00~~~~~
CiHH5)Cq
- ¢
fiq

c .1X a : :. /
S~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~t _0
S 1 2 2 2 o sS m ODY;ro(Z
75 DX (DA. 'z a) ' ;..CAOt X
PQ~~~~~~~~~~~~~l:_ - c toe. a();
l_~~~~~~~~~~~~~~~~~~e CBto(
a~~~~~~~~~~~M 0 Ca.-Iaq0C1 Ca
X~~~~ ~ ~~~~~~~~es mV
;4sowco
Cae- C
bOD Q) D
a q)
10.-
0o d

CD g3 4)O
;j 2 .,I a.o--P4 A4 4
O 4.4 0 c0 $:40-
oY B Ca3
lua roOC
>,OCa
P4
siCO;4
Cdr-
ro
Co wQ
co
Pi

64 Berry & Giuseppi: Traumatic Rupture of the Intestine
DISCUSSION.
The PRESIDENT (AMr. Warrington Haward) said he was sure everyone wouldagree that the Section had had the privilege of listening to a most interestingpaper, prepared with Mr. Berry's usual care and industry. Any contributiontowards the early diagnosis of abdominal injuries must be most valuable to allsurgeons, and the clear manner in which the authors had pointed out thesymptoms which were chiefly to be depended on for the diagnosis of rupture ofthe intestine would be remembered by them all as a most useful addition toknowledge. He hoped surgeons present would relate any similar experienceswhich they might have had.
Mr. G. R. TURNER desired to relate a case which was not included in thepresent paper. It was that of a boy in whom the rectum was ruptured withoutany external wound. He was not able to say exactly how it was ruptured, asthe history was very confused. The boy was said to have been jumping over abroomstick, which passed up his anus and into the abdominal cavity, causingrupture. When admitted into St. George's Hospital he had the ordinarysymptoms of collapse-vomiting, and a very rigid lower abdomen, the upperpart, however, remaining quite supple. The case was diagnosed as a rupture ofthe rectum, and this could just be felt on examining the lower bowel in theusual way. He did a laparotomy, and found feecal matter in the pelvis andabdominal cavity. He removed this and stitched up the wound in the rectum,which was in the upper part, as best he could, passing the stitches through allthe coats of the bowel as rapidly as possible. He afterwards packed the partswith cyanide gauze, but did not use any drain. He treated the injury to thebowel as one would treat an abscess of the appendix. He thought it in thiscase inadvisable to do any washing out. The boy made a good recovery, andhis bowels were opened naturally on the fifth or sixth day; they were notstimulated to do so by means of purgatives or enemata. Subsequent examinationof the rectum, as far as it could be felt, showed that there was nothing in thenature of a stricture, and he believed the patient was still alive and well; hesaw him some months after the operation, but not very recently. He believedthe success of the treatment was due to the fact that the case was seen early,and operation was undertaken within six hours of the injury. He had alsobeen lucky enough to have another successful case, which was included in thepresent table, and was said to have taken one and quarter hours for the anaestheticadministration and operation. It was a case of hernia, in which a weight fellon the rupture, and the diagnosis of ruptured bowel was made and operationwas urged on the patient; but it was not until three or four hours afterwards,when his increasing pain compelled him, that consent was given. He cut downfirst on the hernial sac, and found also tense hydrocele. In addition to havingeventually to open the abdomen and suture the bowel, he dealt with the hernia
Surgical Section 65
and the hydrocele. He removed the sac of the hernia and did a radical cure.The patient never gave any anxiety at all. He was not fed by the mouth forfive days, and the bowels were left to act naturally. The authors advocatedputting the patients in the sitting posture; Mr. Turner thought the importantpoint was to keep them in one position, not allowing them to turn or twistabout. That was of great consequence in all cases where there had been anextravasation of abdominal contents or where an abscess had -been dealt with.The President and he some thirty years ago saw a case of the late Mr. Pollockof'ruptured duodenum long before it became the fashion to open the abdomen.The patient lived for some five days without taking anything by the mouth.When it was thought to be safe to feed in this way he was given a little milk,and only then did the acute peritonitis supervene which carried him off. Thatcase made a very great impression on his mind as showing the necessity of-starvation in cases of suspected rupture of bowel.
Mr. S. G. KIRKBY-GOMES said the following' case came under his ownobservation. When he was surgeon-in-charge of a Government general hos-pital in British Borneo, a Chinaman who had been thrown off a trolley wasbrought in. He hit his shoulder against -a rail, and had an extensive bruise onhis right side. The house surgeon detected a fracture of the right humerusand dislocation of the shoulder on the same side. As the man was in greatpain he was given opium, though it was against the rules to permit opiumsmoking by Chinamen in hospital except under very exceptional circumstances.He vomited once in the hospital. Mr. Kirkby-Gomes came to the hospitalfour hours after the admission of the patient and found the latter moribund.There was increased dulness over the right hypochondrium, and the spleen wasmuch enlarged. A ruptured liver was suspected. He died an hour after Mr.Kirkby-Gomes got to the hospital. At a post-mortem examination, made formedico-legal purposes, he discovered a ruptured duodenum. He mentioned thecase to emphasize the danger of giving opium in such cases and also for itsinterest in the fact that the diseased spleen (ague-cake) was not ruptured, as itwas apt to mislead the surgeon and put him off the correct diagnosis in casesof ruptured intestine.
Mr. PERCY SARGENT said he thought few could be found who wouldquarrel with Mr. Berry's admirable summary of the main points in such cases.He agreed that absence of liver dulness was of no practical value, and hewould be inclined to place rather more emphasis than the authors had doneon the pulse-rate. A steadily increasing pulse was of the very greatest value,and in some of the cases he had seen it had been practically the only symptompointing to the necessity for operation. In one case in particular-one of bulletwound in the abdomen, near the umbilicus-there were no symptoms of peri-tonitis beyond the gradually accelerated pulse-rate; there was no pain, rigidity,vomiting, or dulness. The pulse-rate gradually went up from 90 to 120, andon that symptom alone the abdomen was opened, and several perforations werefound in the small intestine. With regard to the rather striking difference in
N-25a

66 Berry & Giuseppi: Traumatic Rupture of the Intestine
the mortality figures at St. Thomas's as compared with other hospitals, hesuggested that it might be due to the fact that there was a resident surgeonon the spot, which, until quite recently, had not been the case at other hos-pitals. This circumstance would conduce to the earlier recognition of theinjury and operation, either by the surgeon-in-charge or by the residentsurgeon, at the earliest possible moment. In all cases of peritonitis no doubtthe date of operation was the prime factor.
Mr. GIUSEPPI, in reply, said the authors were much indebted to Mr.Turner for his remarks. They did not include the first case he mentionedas it was regarded as a case of perforation through the rectum. There wererecords of several other cases at London hospitals of the same kind, princi-pally from falls on spikes. In one, the rectum was perforated by the sig-moidoscope, and that also was regarded as a case of perforation.
Mr. BERRY, in reply, said he would like to corroborate the view thatopLum should not be given so long as the diagnosis was doubtful, and tomention a case which occurred at the Royal Free Hospital some years ago.The house surgeon had correctly diagnosed a rupture of the intestine, and atonce telephoned for his surgeon. Then he gave the patient opium to relievethe pain, and when the surgeon arrived the man seemed so extremely wellthat operative measures were postponed for several hours, and much valuabletime was thereby lost. He hoped Mr. Sargent did not think the authors under-valued the importance of a rising pulse-rate, but they had perhaps said lessabout it than they might have done because it was already so well known.The symptom upon which they particularly wished to lay stress was pain,the importance of which as a diagnostic sign was perhaps not sufficientlyrecognized. The authors were much obliged to those who had discussed thepaper.




![fileProduct Cauliflower Onions Parsley (Herb) Peas Product Cert. No] 00064- PTKPT_ 0005 00064- PTKTF- 0005 00064- p TKNX- 0005 00064- p TKTT- 0005](https://static.fdocuments.in/doc/165x107/5e07c61b61631c3fb5083934/cauliflower-onions-parsley-herb-peas-product-cert-no-00064-ptkpt-0005-00064-.jpg)