Hypertension inPregnancy - American Society of …jasn.asnjournals.org/content/9/2/314.full.pdf ·...
8
DISEASE OF THE MONTH Hypertension in Pregnancy MARK S. PALLER University of Minnesota, Minneapolis, Minnesota. Notwithstanding its obvious benefits, pregnancy will remain a risky business as we enter the next millennium (1 ). No doubt, many of the historically significant adverse outcomes of preg- nancy have been eliminated by modern medical care. For example, acute renal failure occurring in pregnancy as a con- sequence of septic abortion, abruptio pbacentae, and even pre- eclampsia, has almost disappeared as a clinical entity. Never- thebess, maternal death complicates childbirth in approximately nine of I 00,000 deliveries. The three leading causes of mater- nal death are pregnancy-induced hypertension, hemorrhage, and pulmonary embolism. Hypertension complicates an esti- mated 6 to 8% of all pregnancies. More importantly, hyper- tension is responsible for approximately 15% of maternal deaths. In addition, almost one-quarter of pregnant women require hospitalization for complications before delivery, rep- resenting a substantial health care burden. For the nephrobogist, the impact of pregnancy on preexistent renal disease or chronic hypertension will be encountered more often than new cases of renal disease developing de novo during pregnancy. However, pregnancy is often the first sustained contact between young women and the health care system. Therefore, asymptomatic renal disease or hypertension may be recognized initially dur- ing a pregnancy. Hypertension in Pregnancy Hypertension may be classified as chronic if it is recognized before 20 weeks of gestation or as pregnancy-induced if it occurs only in the second half of pregnancy. This separation is clinically useful because almost all hypertension occurring in the first half of pregnancy is a result of underlying chronic hypertension (essential hypertension or secondary hyperten- sion due to hyperaldosteronism or pheochromocytoma) or re- nab disease. Hypertension developing in the second half of pregnancy is more complex and is the result of either a preg- nancy-specific process or a complex interplay of pregnancy with renal disease or chronic hypertension resulting in exacer- bation of hypertension. Normal pregnancy is characterized by a decrease in periph- eral vascular resistance and, to a lesser extent, a decrease in blood pressure, which occur soon after conception. This de- crease in vascular resistance is due to increased synthesis of vasodilatory prostaglandins, particularly prostacyclin. and en- Correspondence to Dr. Mark S. Paller. University of Minnesota. 420 Delaware Street SE., Box 736. Minneapolis, MN 55455. l()46-6673/0902-03 14$03.00/() Journal of the American Society of Nephrology Copyright tO 1998 by the American Society of Nephrology dothelial-derived nitric oxide. These vasodilators also engen- der resistance to circulating vasoconstrictors such as angioten- sin II and norepinephrine, and to locally produced vasoconstrictors such as endothelin. After an initial decrease in blood pressure to average values of I 03 ± 11 mmHg systolic and 56 ± 10 mmHg diastolic in the first trimester, blood pressure begins to increase slightly after the 28th week of gestation. Although 140/90 mmHg is a convenient criterion for epidemiologic studies, perinatal mortality increases for each increment in blood pressure, particularly when diastolic blood pressure exceeds 85 mmHg. Similarly, perinatal mortality in- creases when mean arterial pressure is greater than 82 mmHg at mid-pregnancy or greater than 92 mmHg at the beginning of the third trimester. Because a blood pressure of 1 20/80 mmHg represents a mean arterial pressure of 93 mmHg, it is apparent that blood pressure values during pregnancy must be inter- preted differently than values in the nonpregnant state. Previ- ously, the American College of Obstetrics and Gynecology considered a pregnancy-related increase in systolic blood pres- sure of 30 mmHg or pregnancy-related increase in diastolic blood pressure of 15 mmHg as also representing hypertension in pregnancy. These criteria have been abandoned because of the considerable variability of blood pressure in normotensive women. Endothelial Cell Injury and Pregnancy-Related Diseases A variety of diseases of relevance to the nephrologist whose manifestations include consequences of diffuse endothelial cell injury occur during pregnancy. Postpartum acute renal failure, also known as postpartum hemolytic uremic syndrome, is one such condition. This disease, characterized by hypertension and coagulation abnormalities, including microangiopathic he- molytic anemia, occurs 1 or 2 days to several months after delivery. Its major manifestation is thrombotic microangio- pathic acute renal failure. Postpartum acute renal failure has many similarities to thrombotic thrombocytopenic purpura and hemolytic uremic syndrome. Of great interest, preeclampsia, the HELLP syndrome (hemolysis, elevated liver enzymes, low platelets), and acute fatty liver of pregnancy also have features consistent with endothelial injury. This suggests the possibility of a continuum of disease resulting from endothelial cell injury during pregnancy, perhaps initiated through distinct pathways. Why the endothelium should be so susceptible to injury during pregnancy remains unclear. A form of hemolytic uremic syn- drome similar to postpartum acute renal failure occurs in women receiving oral contraceptives. This finding suggests a hormonal etiology for the endothelial susceptibility to injury.
Transcript of Hypertension inPregnancy - American Society of …jasn.asnjournals.org/content/9/2/314.full.pdf ·...

DISEASE OF THE MONTH
Hypertension in Pregnancy
MARK S. PALLERUniversity of Minnesota, Minneapolis, Minnesota.
Notwithstanding its obvious benefits, pregnancy will remain a
risky business as we enter the next millennium ( 1 ). No doubt,
many of the historically significant adverse outcomes of preg-
nancy have been eliminated by modern medical care. For
example, acute renal failure occurring in pregnancy as a con-
sequence of septic abortion, abruptio pbacentae, and even pre-
eclampsia, has almost disappeared as a clinical entity. Never-
thebess, maternal death complicates childbirth in approximately
nine of I 00,000 deliveries. The three leading causes of mater-
nal death are pregnancy-induced hypertension, hemorrhage,
and pulmonary embolism. Hypertension complicates an esti-
mated 6 to 8% of all pregnancies. More importantly, hyper-
tension is responsible for approximately 15% of maternal
deaths. In addition, almost one-quarter of pregnant women
require hospitalization for complications before delivery, rep-
resenting a substantial health care burden. For the nephrobogist,
the impact of pregnancy on preexistent renal disease or chronic
hypertension will be encountered more often than new cases of
renal disease developing de novo during pregnancy. However,
pregnancy is often the first sustained contact between young
women and the health care system. Therefore, asymptomatic
renal disease or hypertension may be recognized initially dur-
ing a pregnancy.
Hypertension in PregnancyHypertension may be classified as chronic if it is recognized
before 20 weeks of gestation or as pregnancy-induced if it
occurs only in the second half of pregnancy. This separation is
clinically useful because almost all hypertension occurring in
the first half of pregnancy is a result of underlying chronic
hypertension (essential hypertension or secondary hyperten-
sion due to hyperaldosteronism or pheochromocytoma) or re-
nab disease. Hypertension developing in the second half of
pregnancy is more complex and is the result of either a preg-
nancy-specific process or a complex interplay of pregnancy
with renal disease or chronic hypertension resulting in exacer-
bation of hypertension.
Normal pregnancy is characterized by a decrease in periph-
eral vascular resistance and, to a lesser extent, a decrease in
blood pressure, which occur soon after conception. This de-
crease in vascular resistance is due to increased synthesis of
vasodilatory prostaglandins, particularly prostacyclin. and en-
Correspondence to Dr. Mark S. Paller. University of Minnesota. 420 DelawareStreet SE., Box 736. Minneapolis, MN 55455.
l()46-6673/0902-03 14$03.00/()
Journal of the American Society of Nephrology
Copyright tO 1998 by the American Society of Nephrology
dothelial-derived nitric oxide. These vasodilators also engen-
der resistance to circulating vasoconstrictors such as angioten-
sin II and norepinephrine, and to locally produced
vasoconstrictors such as endothelin. After an initial decrease in
blood pressure to average values of I 03 ± 1 1 mmHg systolic
and 56 ± 10 mmHg diastolic in the first trimester, blood
pressure begins to increase slightly after the 28th week of
gestation. Although 140/90 mmHg is a convenient criterion for
epidemiologic studies, perinatal mortality increases for each
increment in blood pressure, particularly when diastolic blood
pressure exceeds 85 mmHg. Similarly, perinatal mortality in-
creases when mean arterial pressure is greater than 82 mmHg
at mid-pregnancy or greater than 92 mmHg at the beginning of
the third trimester. Because a blood pressure of 1 20/80 mmHg
represents a mean arterial pressure of 93 mmHg, it is apparent
that blood pressure values during pregnancy must be inter-
preted differently than values in the nonpregnant state. Previ-
ously, the American College of Obstetrics and Gynecology
considered a pregnancy-related increase in systolic blood pres-
sure of 30 mmHg or pregnancy-related increase in diastolic
blood pressure of 15 mmHg as also representing hypertension
in pregnancy. These criteria have been abandoned because of
the considerable variability of blood pressure in normotensive
women.
Endothelial Cell Injury and Pregnancy-RelatedDiseases
A variety of diseases of relevance to the nephrologist whose
manifestations include consequences of diffuse endothelial cell
injury occur during pregnancy. Postpartum acute renal failure,
also known as postpartum hemolytic uremic syndrome, is one
such condition. This disease, characterized by hypertension
and coagulation abnormalities, including microangiopathic he-
molytic anemia, occurs 1 or 2 days to several months after
delivery. Its major manifestation is thrombotic microangio-
pathic acute renal failure. Postpartum acute renal failure has
many similarities to thrombotic thrombocytopenic purpura and
hemolytic uremic syndrome. Of great interest, preeclampsia,
the HELLP syndrome (hemolysis, elevated liver enzymes, low
platelets), and acute fatty liver of pregnancy also have features
consistent with endothelial injury. This suggests the possibility
of a continuum of disease resulting from endothelial cell injury
during pregnancy, perhaps initiated through distinct pathways.
Why the endothelium should be so susceptible to injury during
pregnancy remains unclear. A form of hemolytic uremic syn-
drome similar to postpartum acute renal failure occurs in
women receiving oral contraceptives. This finding suggests a
hormonal etiology for the endothelial susceptibility to injury.

Pregnancy: A Risky Business
The Shwartzman reaction that occurs after admission of endo-
toxin to experimental animals is enhanced when animals are
pregnant. A possible explanation for that phenomenon is an
impaired capacity of endothelial cells to synthesize nitric oxide
during pregnancy. Impaired endothelial synthesis of nitric ox-
ide and prostacyclin then predisposes to vasoconstriction and
coagulation.
PreeclampsiaPreeclampsia, a life-threatening illness specific to preg-
nancy, is poorly understood. Major manifestations of pre-
eclampsia include hypertension, edema, proteinuria, and sei-
zures. The disease is termed eclampsia when seizures occur,
but this distinction is not important because death due to
cerebral hemorrhage or cardiac failure can occur in the absence
of seizures. Preeclampsia is a fascinating disease because of its
association with first pregnancies and complicated pregnan-
cies. Depending on the population surveyed, preeclampsia
complicates between 5 and 22% of pregnancies. In addition to
nulliparity, other risk factors for the development of pre-
eclampsia include age greater than 40 years (advanced in terms
of reproductive age), familial history of pregnancy-induced
pregnancy hypertension, smoking, obesity, and diabetes mel-
litus. Pregnancies complicated by fetal hydrops. multiple ges-
tation, preexisting hypertension. antiphospholipid syndrome,
renal disease, and vascular disease are also at increased risk of
preeclampsia (Table 1 ). The relative risk of preeclampsia de-
veloping in women with chronic renal disease is 20 to 1 . and
the risk of preeclampsia developing in women with essential
hypertension is 10 to I . In these instances, preeclampsia affects
multiparous, as well as nulliparous, women. Moreover, pre-
eclampsia complicating these conditions may develop earlier
than 32 weeks of gestation, whereas “usual” preeclampsia
affecting nulliparous women develops in the third trimester
(usually after 32 weeks of gestation). One should be alert to the
possibility that preeclampsia occasionally presents as late as 48
hours postpartum.
The clinical manifestations of preeclampsia support the con-
tention that this is a systemic disease. Hypertension is the most
prominent feature of preeclampsia and may be severe. Hyper-
Table 1. Risk factors for the development of preeclampsia
Nulliparity
Age greater than 40 years (advanced age in reproductive
terms)
Familial history of pregnancy-induced pregnancy
hypertension
Obesity
Diabetes mellitus
Fetal hydrops
Multiple gestation
Hypertension
Renal disease
Antiphospholipid syndrome
Vascular disease
tension is caused by an increase in peripheral vascular resis-
tance and is associated with overactivity of the sympathetic
nervous system. Abnormalities in peripheral vascular reactivity
can be demonstrated before the development of overt hyper-
tension. Ordinarily in pregnancy there is a shift in production
of vasoactive substances by the endothelium, favoring vasodi-
bation. This increase in production of prostacyclin and nitric
oxide causes pregnant women to be less sensitive to the pressor
effects of substances such as angiotensin II. In women destined
to become preeclamptic in the third trimester. loss of this usual
resistance to the pressor effects of infused angiotensin II can be
demonstrated in mid-pregnancy when blood pressure is still
normal.
Vasoconstriction in preeclampsia may also cause a decrease
in cardiac output and a decrease in renal blood flow and GFR.
This decrease in renal blood flow is responsible for a rise in
plasma uric acid, which usually occurs in advance of any
changes in serum creatinine. Decreased urate clearance result-
ing in hyperuricemia is a useful clinical finding that can serve
to differentiate preeclampsia from other causes of hypertension
that may occur during pregnancy. Because of plasma volume
expansion that occurs during normal pregnancy, serum uric
acid bevels are between 2.5 and 4 mg/dl in pregnancy. A serum
uric acid level greater than 5.5 mg/dl is consistent with pre-
eclampsia. and values exceeding 6.0 mg/dl suggest more seri-
ous disease. Other manifestations of preeclampsia affecting the
kidney include proteinuria, increased serum creatinine, and in
severe preecbampsia oliguria. Although pregnancy causes a
small increase in the fractional excretion of albumin, 24-hour
urinary excretion of protein should not exceed 250 rng. Protein
excretion in excess of this amount suggests either renal disease
or preecbampsia (Table 2).
Women with preeclarnpsia have symptoms that include ap-
prehension: vision problems: and headache and epigastric dis-
comfort related to neurologic and hepatic involvement, respec-
tively. Findings on physical examination in addition to
hypertension include segmental arteriolar narrowing on fundu-
scopic examination and rales and other physical findings con-
sistent with congestive heart failure. Signs of central nervous
system irritability include hyperactive deep tendon reflexes and
generalized seizures. Although peripheral edema at one time
was considered a requirement for the diagnosis of preeclamp-
sia, this finding has little predictive value. Up to 83% of
healthy. pregnant women develop localized edema at some
time during pregnancy. As many as 10% of pregnant women
develop generalized edema without other indications of dis-
ease. Therefore, edema does not predictably differentiate pre-
eclampsia from uncomplicated pregnancy or from pregnancy
complicated by chronic hypertension or renal disease.
Laboratory findings in preecbampsia, in addition to the ele-
vations in serum uric acid and creatinine discussed above,
include indicators of a microangiopathic hemolytic anemia.
These include fragmented red cells on peripheral smear, in-
creased lactate dehydrogenase, and thrombocytopenia. Hepa-
tocellular dysfunction can be recognized by an elevation in
liver enzymes. The HELLP syndrome (/iemolysis, elevated
liver enzymes, low platelets) is a clinical syndrome that rep-
3 16 Journal of the American Society of Nephrology
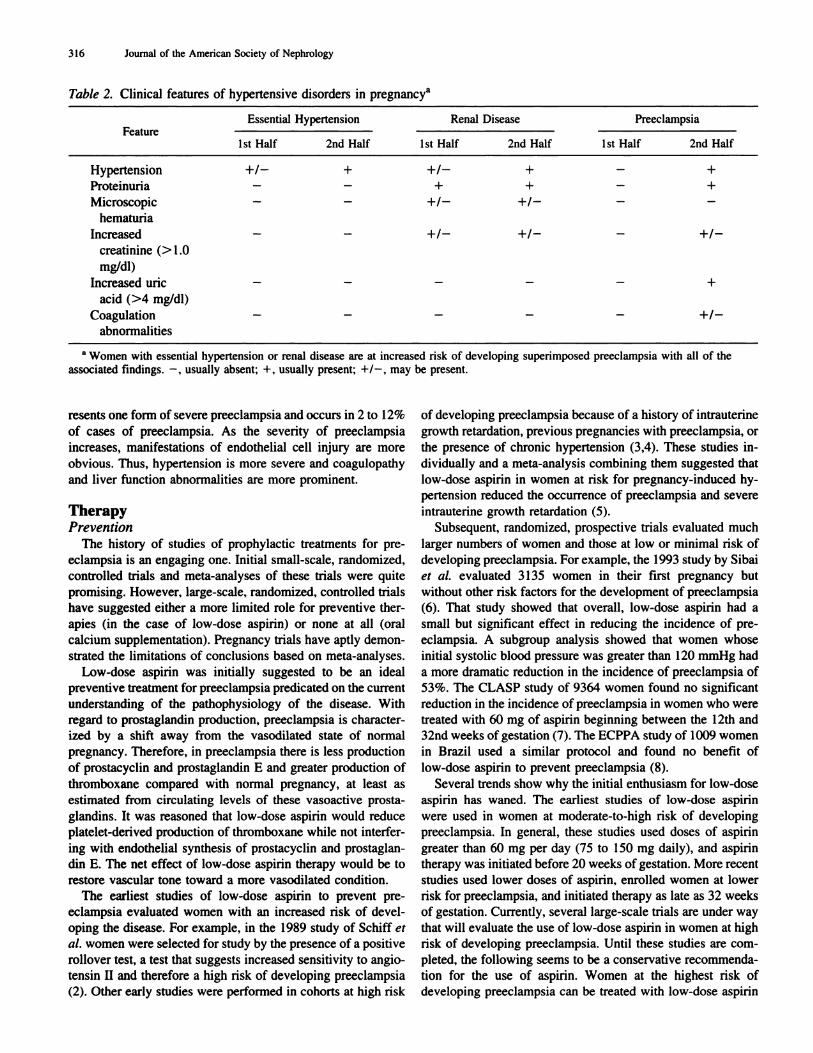
Table 2. Clinical features of hypertensive disorders in pregnancya
FeatureEssential Hypertension Renal Disease Preeclampsia
1st Half 2nd Half 1st Half 2nd Half 1st Half 2nd Half
Hypertension
Proteinuria
+1-
-
+
-
+1-
+
+
+
-
-
+
+
Microscopic
hematuria
- - +1- +1- - -
Increased - - +1- +1- - +1-
creatinine (>1.0
mg/dl)
Increased uric - - - - - +
acid (>4 mg/dl)
Coagulation
abnormalities
- - - - - +/-
a Women with essential hypertension or renal disease are at increased risk of developing superimposed preeclampsia with all of the
associated findings. - . usually absent: +, usually present: +/-. may be present.
resents one form of severe preeclampsia and occurs in 2 to I 2%
of cases of preeclampsia. As the severity of preeclampsia
increases, manifestations of endothelial cell injury are more
obvious. Thus, hypertension is more severe and coagubopathy
and liver function abnormalities are more prominent.
TherapyPrevention
The history of studies of prophylactic treatments for pre-
eclampsia is an engaging one. Initial small-scale, randomized,
controlled trials and meta-analyses of these trials were quite
promising. However. large-scale, randomized, controlled trials
have suggested either a more limited role for preventive ther-
apies (in the case of low-dose aspirin) or none at all (oral
calcium supplementation). Pregnancy trials have aptly demon-
strated the limitations of conclusions based on meta-analyses.
Low-dose aspirin was initially suggested to be an ideal
preventive treatment for preeclampsia predicated on the current
understanding of the pathophysiobogy of the disease. With
regard to prostaglandin production. preeclampsia is character-
ized by a shift away from the vasodilated state of normal
pregnancy. Therefore, in preeclampsia there is less production
of prostacyclin and prostaglandin E and greater production of
thromboxane compared with normal pregnancy, at least as
estimated from circulating levels of these vasoactive prosta-
glandins. It was reasoned that low-dose aspirin would reduce
platelet-derived production of thromboxane while not interfer-
ing with endothebial synthesis of prostacyclin and prostaglan-
din E. The net effect of low-dose aspirin therapy would be to
restore vascular tone toward a more vasodilated condition.
The earliest studies of low-dose aspirin to prevent pre-
eclampsia evaluated women with an increased risk of devel-
oping the disease. For example, in the 1989 study of Schiff et
al. women were selected for study by the presence of a positive
rollover test, a test that suggests increased sensitivity to angio-
tensin II and therefore a high risk of developing preeclampsia
(2). Other early studies were performed in cohorts at high risk
of developing preeclampsia because of a history of intrauterine
growth retardation, previous pregnancies with preeclampsia, or
the presence of chronic hypertension (3,4). These studies in-
dividually and a meta-analysis combining them suggested that
low-dose aspirin in women at risk for pregnancy-induced hy-
pertension reduced the occurrence of preeclampsia and severe
intrauterine growth retardation (5).
Subsequent, randomized, prospective trials evaluated much
larger numbers of women and those at low or minimal risk of
developing preeclampsia. For example, the 1993 study by Sibai
et al. evaluated 3 1 35 women in their first pregnancy but
without other risk factors for the development of preeclampsia
(6). That study showed that overall, low-dose aspirin had a
small but significant effect in reducing the incidence of pre-
eclampsia. A subgroup analysis showed that women whose
initial systolic blood pressure was greater than 120 mmHg had
a more dramatic reduction in the incidence of preeclampsia of
53%. The CLASP study of 9364 women found no significant
reduction in the incidence of preeclampsia in women who were
treated with 60 mg of aspirin beginning between the 12th and
32nd weeks ofgestation (7). The ECPPA study of 1009 women
in Brazil used a similar protocol and found no benefit of
low-dose aspirin to prevent preeclampsia (8).
Several trends show why the initial enthusiasm for low-dose
aspirin has waned. The earliest studies of low-dose aspirin
were used in women at moderate-to-high risk of developing
preeclampsia. In general, these studies used doses of aspirin
greater than 60 mg per day (75 to I 50 mg daily), and aspirin
therapy was initiated before 20 weeks of gestation. More recent
studies used lower doses of aspirin, enrolled women at lower
risk for preeclampsia, and initiated therapy as late as 32 weeks
of gestation. Currently, several large-scale trials are under way
that will evaluate the use of low-dose aspirin in women at high
risk of developing preeclampsia. Until these studies are com-
pleted. the following seems to be a conservative recommenda-
tion for the use of aspirin. Women at the highest risk of
developing preeclampsia can be treated with low-dose aspirin

Pregnancy: A Risky Business 317
in the hope of preventing preeclampsia using doses �100 mg
daily. The safety of low-dose aspirin in these women is no
longer contested. Several of the recent large-scale trials eval-
uated safety very carefully and found no increased incidence of
bleeding, abruptio placentae, or other adverse effects, contrary
to anecdotal reports from earlier small studies (9,10). Because
high-risk women may develop early-onset preeclampsia (be-
fore 30 weeks gestation) if low-dose aspirin is used, it should
be initiated between 10 and 14 weeks of gestation. Women
considered at high risk for preeclampsia include those who
have chronic renal disease, particularly with hypertension,
proteinuria, or renal insufficiency, as well as women who have
a history of previous multiple pregnancies complicated by
intrauterine growth retardation or preeclampsia.
Calcium supplementation for prophylaxis of preeclampsia
has a similar history of diminished expectations. Original stud-
ies suggested that 2 grams of elemental calcium daily would
reduce the incidence of preeclampsia. In 1991, Belizan et al.
reported beneficial effects of calcium in 1 194 nulliparous
women (1 1). Calcium was administered beginning the 20th
week of pregnancy. Several additional small-scale studies, as
well as a meta-analysis combining all studies performed before
May 1994, suggested that calcium supplementation reduced
the risk of preeclampsia by 62% (12). Unfortunately, the most
recent large-scale trial of calcium supplementation in 4589
nulliparous women reported by Levine et al. revealed no
beneficial effects of calcium (13). Again, these findings seem
most secure for women at low risk of developing preeclampsia.
It is possible that previous small studies performed at a single
center had evaluated women at moderate or high risk for the
development of preeclampsia. In the absence of clues as to
which women should receive calcium supplementation, cal-
cium cannot be recommended for prophylaxis of preeclampsia
at this time.
Management
The time-tested, definitive treatment for preeclampsia is
delivery. For women at term, this does not represent a major
problem. When preeclampsia occurs between the 32nd and
34th weeks of gestation, obstetricians have some flexibility.
Because long-term fetal outcome is likely to be good, delivery
still remains a feasible option. However, if preeclampsia is not
severe, conservative therapy consisting of bed rest and antihy-
pertensive therapy can be undertaken. Fetal outcome is less
well guaranteed at 28 to 34 weeks of gestation. If preeclampsia
occurs at this time, it is reasonable to attempt medical man-
agement. It must be noted that experience with such an ap-
proach is limited. Conservative management between 1 8 and
28 weeks of gestation has been debated, with some studies
suggesting termination of pregnancy at the expense of the life
of the fetus to prevent maternal morbidity and others suggest-
ing that an initial attempt at conservative management will
occasionally result in prolongation of pregnancy with an ulti-
mately acceptable outcome. Most would agree that pregnancy
should be terminated if preeclampsia develops before the 18th
week of gestation.
Hypertension complicating pregnancy represents a risk for
both the mother and the fetus, both of whom must be consid-
ered when selecting therapy. Hypertension should be treated to
prevent maternal morbidity and mortality due to causes such as
cerebral hemorrhage. The effect of antihypertensive therapy on
fetal outcome is less clear, and there is considerable debate as
to how aggressively blood pressure should be treated. Arguing
against aggressive antihypertensive therapy is the fear that
uteroplacental blood flow will be compromised if maternal
blood pressure falls too quickly because of a limited ability of
the placenta to autoregulate blood flow. Diastolic blood pres-
sure goals have ranged from 90 to 1 10 mmHg, denoting the
lack of unanimity of opinion. The number and size of prospec-
live, randomized, controlled trials of antihypertensive therapy
for women who develop hypertension in the third trimester are
actually quite limited. Most studies do suggest that fetal mor-
bidity and mortality can be reduced when treatment is provided
for diastolic blood pressures >90 mmHg. The outcomes that
can be expected by treating hypertension in the third trimester
include reduction in the incidence of prematurity, intrauterine
growth retardation, and perinatal death. For example, Phippard
et al. aggressively treated pregnancy-induced hypertension in
women with previously normal blood pressure whose mean
blood pressure rose to 1 26/82 mmHg with either clonidine (and
hydralazine if needed) or placebo ( 14). Antihypertensive ther-
apy reduced third trimester complications and prematurity by
80%. Those studies that have demonstrated improved fetal
outcome have instituted antihypertensive therapy in the second
or third trimester of pregnancy. Results may not be comparable
when antihypertensive therapy is begun in the first trimester
(see below).
Treatment of mild hypertension (diastolic blood pressure
<95 mmHg) usually commences with bed rest. One needs to
ascertain that there is no evidence of serious disease such as
proteinuria (>500 mg/24 h), renal function impairment (cre-
atinine > 1 .0 mg/dl), or hyperuricemia. Development of these
or other complications is an indication for delivery, especially
when pregnancy is at or beyond 32 weeks of gestation. Mod-
erate hypertension (diastolic blood pressure 95 to I 00 mmHg)
should lead to the use of any one of several suitable antihy-
pertensive agents if delivery is not desirable because of pre-
maturity (Table 3).
Methyldopa has been used extensively in pregnancy and is
often the agent of first choice. Although this agent has been
largely abandoned for general use in essential hypertension
because of the side effects of orthostatic hypotension and
fatigue, methyldopa is both safe and effective in pregnancy. In
a trial of methyldopa versus placebo to treat hypertension in
pregnancy by Redman et al. , methyldopa effectively controlled
blood pressure (15). Methyldopa therapy also yielded better
fetal outcome (fewer mid-pregnancy abortions), but had no
effect in preventing preeclampsia. An initial concern was that
infants born to mothers who had received methyldopa had
smaller head circumference for gestational age. When these
infants were evaluated at 1 year, all head sizes were normal
( 1 6). More importantly, infants born to women who had re-
ceived placebo scored worse on the Denver Developmental
Screening Test than did infants whose mothers received active
3 18 Journal of the American Society of Nephrology
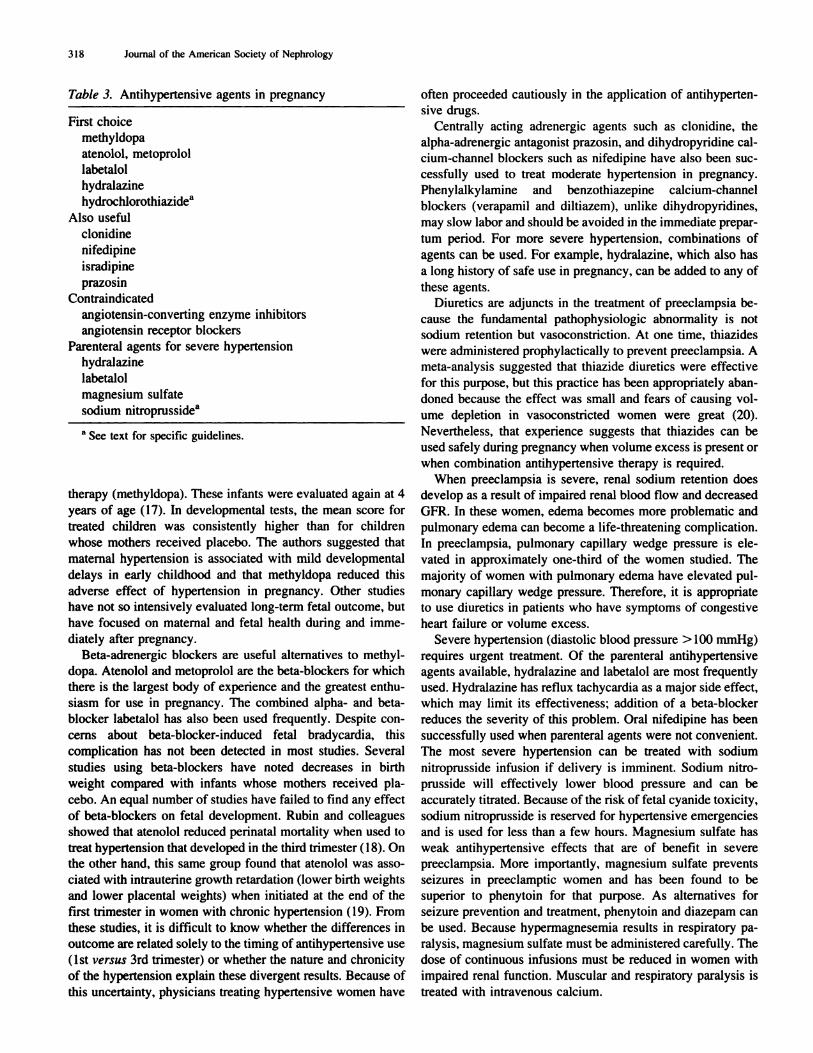
Table 3. Antihypertensive agents in pregnancy
First choice
methyldopa
atenobol, metoprobol
labetabol
hydralazine
hydrochborothiazidea
Also useful
cbonidine
nifedipine
isradipine
prazosi n
Contraindicated
angiotensin-converti ng enzyme inhibitors
angiotensin receptor blockers
Parenteral agents for severe hypertension
hydralazine
labetalol
magnesium sulfate
sodium nitroprussidea
a See text for specific guidelines.
therapy (methyldopa). These infants were evaluated again at 4
years of age ( I 7). In developmental tests. the mean score for
treated children was consistently higher than for children
whose mothers received placebo. The authors suggested that
maternal hypertension is associated with mild developmental
delays in early childhood and that methyldopa reduced this
adverse effect of hypertension in pregnancy. Other studies
have not so intensively evaluated long-term fetal outcome, but
have focused on maternal and fetal health during and imme-
diately after pregnancy.
Beta-adrenergic blockers are useful alternatives to methyl-
dopa. Atenobol and metoprolol are the beta-blockers for which
there is the largest body of experience and the greatest enthu-
siasm for use in pregnancy. The combined alpha- and beta-
blocker labetabol has also been used frequently. Despite con-
cerns about beta-blocker-induced fetal bradycardia, this
complication has not been detected in most studies. Several
studies using beta-blockers have noted decreases in birth
weight compared with infants whose mothers received pla-
cebo. An equal number of studies have failed to find any effect
of beta-blockers on fetal development. Rubin and colleagues
showed that atenobol reduced perinatal mortality when used to
treat hypertension that developed in the third trimester ( 1 8). On
the other hand, this same group found that atenolol was asso-
ciated with intrauterine growth retardation (lower birth weights
and lower placental weights) when initiated at the end of the
first trimester in women with chronic hypertension ( I 9). From
these studies, it is difficult to know whether the differences in
outcome are related solely to the timing of antihypertensive use
( 1 st versus 3rd trimester) or whether the nature and chronicity
of the hypertension explain these divergent results. Because of
this uncertainty. physicians treating hypertensive women have
often proceeded cautiously in the application of antihyperten-
sive drugs.
Centrally acting adrenergic agents such as clonidine, the
alpha-adrenergic antagonist prazosin. and dihydropyridine cab-
cium-channel blockers such as nifedipine have also been suc-
cessfully used to treat moderate hypertension in pregnancy.
Phenylalkylamine and benzothiazepine calcium-channel
blockers (verapamil and diltiazern), unlike dihydropyridines,
may slow labor and should be avoided in the immediate prepar-
turn period. For more severe hypertension. combinations of
agents can be used. For example, hydralazine. which also has
a long history of safe use in pregnancy, can be added to any of
these agents.
Diuretics are adjuncts in the treatment of preeclampsia be-
cause the fundamental pathophysiologic abnormality is not
sodium retention but vasoconstriction. At one time, thiazides
were administered prophylactically to prevent preeclampsia. A
nieta-analysis suggested that thiazide diuretics were effective
for this purpose. but this practice has been appropriately aban-
doned because the effect was small and fears of causing vol-
ume depletion in vasoconstricted women were great (20).
Nevertheless, that experience suggests that thiazides can be
used safely during pregnancy when volume excess is present or
when combination antihypertensive therapy is required.
When preeclampsia is severe, renal sodium retention does
develop as a result of impaired renal blood flow and decreased
GFR. In these women, edema becomes more problematic and
pulmonary edema can become a life-threatening complication.
In preecbampsia, pulmonary capillary wedge pressure is ele-
vated in approximately one-third of the women studied. The
majority of women with pulmonary edema have elevated pul-
monary capillary wedge pressure. Therefore, it is appropriate
to use diuretics in patients who have symptoms of congestive
heart failure or volume excess.
Severe hypertension (diastolic blood pressure > 100 mmHg)
requires urgent treatment. Of the parenteral antihypertensive
agents available, hydralazine and labetalol are most frequently
used. Hydralazine has reflux tachycardia as a major side effect,
which may limit its effectiveness: addition of a beta-blocker
reduces the severity of this problem. Oral nifedipine has been
successfully used when parenterab agents were not convenient.
The most severe hypertension can be treated with sodium
nitroprusside infusion if delivery is imminent. Sodium nitro-
prusside will effectively lower blood pressure and can be
accurately titrated. Because of the risk of fetal cyanide toxicity,
sodium nitroprusside is reserved for hypertensive emergencies
and is used for less than a few hours. Magnesium sulfate has
weak antihypertensive effects that are of benefit in severe
preeclampsia. More importantly, magnesium sulfate prevents
seizures in preeclamptic women and has been found to be
superior to phenytoin for that purpose. As alternatives for
seizure prevention and treatment, phenytoin and diazepam can
be used. Because hypermagnesemia results in respiratory pa-
ralysis, magnesium sulfate must be administered carefully. The
dose of continuous infusions must be reduced in women with
impaired renal function. Muscular and respiratory paralysis is
treated with intravenous calcium.

Pregnancy: A Risky Business 319
Outcome
Preeclampsia is associated with an increase in perinatal
morbidity and mortality. A major feature of preeclampsia is
decreased uteroplacental blood flow because of vasoconstric-
tion. Pathologic changes are most apparent in the spiral arteries
of the placenta, a consequence of impaired prostaglandin pro-
duction by trophoblasts. Impaired uteroplacental perfusion
leads to intrauterine growth retardation. Fetuses are also at risk
in preeclampsia because of an increased incidence of abruptio
placenta.
Women who develop preeclampsia in a first pregnancy but
who are normotensive in subsequent pregnancies have no
long-term morbidity or mortality related to the initial episode
of preeclampsia. Epidemiologic studies have found that these
women have no increased prevalence of hypertension and have
a normal life expectancy. In marked contrast, women who
develop preeclampsia in a second pregnancy or in multiple
pregnancies have an increased prevalence of hypertension and
greater mortality than age-matched control subjects. When
women with multiple episodes of preeclampsia were evaluated
20 to 40 years after their initial pregnancy, the prevalence of
hypertension was approximately twice that of the control pop-
ulation. Hypertension is believed to be the cause of the excess
vascular disease and premature death in such women. This
observation is consistent with our current understanding of
preeclampsia. “Idiopathic” or “primary” preeclampsia is a dis-
ease that occurs in nulliparous women. Major risk factors for
recurrent or “secondary” preeclampsia are chronic hyperten-
sion, renal disease, and diabetes. These diseases persist long
after pregnancy has ended, and their associated morbidity and
mortality accrues. When preeclampsia occurs in the first half of
pregnancy, it is more likely to be secondary to one of these
diseases (21,22). For such women, there are long-term health
risks. Women who develop preeclampsia late in a first preg-
nancy and who have no evidence of hypertension or renal
disease between and during subsequent pregnancies can be
reassured of a favorable long-term outcome.
Hypertension Complicating Renal DiseaseDiagnosis
Renal disease is one manifestation of preeclampsia. On the
other hand, renal disease predisposes to the development of
superimposed preeclampsia. This distinction is made more
difficult if a woman has not been evaluated before pregnancy
or early in gestation. Even subtle renal disease may predispose
to the development of preeclampsia. For example, women with
a history of reflux during childhood but with normal renal
function have an increased incidence of preeclampsia and
perinatal complications. Urinary abnormalities in the first tn-
mester should suggest underlying renal disease. Although the
fractional excretion of albumin increases during pregnancy,
protein excretion is usually not greater than 250 mg/24 h.
Protein excretion in excess of this amount can be caused by
either intrinsic renal disease or preeclampsia. Hematunia is not
a usual finding in preeclampsia and suggests glomerubonephri-
tis. Table 2 outlines those findings that help to differentiate
preeclampsia from chronic hypertension or hypertension asso-
ciated with renal disease.
Pregnancy Outcome
Fetal loss, intrauterine growth retardation, and prematurity
are the major fetal consequences of maternal renal disease. The
most important risk factor for these undesirable fetal outcomes
is hypertension, although renal insufficiency and high-grade
proteinunia also portend a less favorable outcome. With severe
hypertension (> 175/1 10 mmHg). fetal loss rates greater than
60% have been reported. The risk of developing superimposed
preeclampsia during pregnancy in women with renal disease
varies between 20 and 40%. For this reason, it seems reason-
able to begin low-dose aspirin early in pregnancy in women
with renal disease in expectation of preventing preeclampsia.
Renal Outcome: Testing the Hvpeifiltration Hypothesis
Pregnancy is a potential test of the hyperfiltration hypothe-
sis, originally articulated by Hostetter, Brenner, and col-
leagues, proposing that an increase in glomerular capillary
hydrostatic pressure is a central factor in the inexorable pro-
gression of chronic renal diseases. Pregnancy might be partic-
ularly risky in this regard because renal vasodilation is char-
actenistic of pregnancy. In the presence of systemic
hypertension, a greater portion of systemic blood pressure
would be transmitted into the glomerulus, potentially exacer-
bating injury. To test this hypothesis, one would first need to
ascertain whether pregnancy results in an irreversible detenio-
ration in renal function in women with chronic renal insuffi-
ciency. Although the general answer to that question is yes
with the following provisos, it has not been possible to study
mechanisms of injury in women. Pregnant rats have been
studied, but may not be a suitable model for the human expe-
nience. For example, the spontaneously hypertensive rat does
not develop the expected afferent arteriolar vasodilatation of
pregnancy, does not experience the usual pregnancy-induced
increase in GFR, and also does not develop increased intraglo-
merular pressure during pregnancy or progressive renal failure.
On the other hand, in experimental gbomerulonephnitis pro-
duced by injecting rats with Adriamycin, systemic hyperten-
sion did exacerbate proteinuria. possibly indicating irreversible
renal injury.
Women with renal disease who have normal GFR, normal
blood pressure, and no proteinunia do not suffer renal impair-
ment during pregnancy. In contrast, approximately one-third of
women who have renal insufficiency when they become preg-
nant suffer an irreversible, accelerated deterioration in renal
function (23,24). Hypertension has often been found to be an
additional risk factor for this deterioration during pregnancy.
The hyperfiltration hypothesis has not been fully tested, how-
ever, because there has been no adequate demonstration (or
lack thereof) that aggressively treating hypertension to prevent
intraglomerular hypertension necessarily prevents irreversible
deterioration of renal function during pregnancy in these high-
risk women.

320 Journal of the American Society of Nephrology
Management
Current practice is to continue antihypertensive therapy
when pregnancy develops, but the exact goal for blood pres-
sure control has not been established. Too low maternal blood
pressure potentially puts the fetus at risk, whereas too high
blood pressure endangers both mother and child. As noted
above, there is a wide range of antihypertensive agents that can
be safely used during pregnancy. An important exception to the
rule of continuing current therapy when pregnancy develops is
the use of angiotensin-converting enzyme inhibitors (ACEI).
ACE! have been associated with increased fetal loss in exper-
imental animals and with fetal renal tubular dysplasia, perinatal
acute renal failure, and other congenital anomalies. The moth-
ers of these unfortunate infants have all consumed ACE! in the
second or third trimester of pregnancy, or both. A recent
post-marketing survey of ACE! in the United States, Canada,
and Israel revealed no adverse fetal outcomes because of use of
ACE! in the first trimester only (25). Therefore, when women
receiving ACE! become pregnant, they should be switched to
other antihypertensive agents. However, when exposure is
limited to the first trimester, it does not appear necessary to
intentionally terminate the pregnancy. One must assume that
angiotensin I! receptor blockers are similarly contraindicated
for use during pregnancy. Angiotensin type 2 (AT2) receptors
are involved in development of the fetal kidney. It is not clear
whether blocking only type 1 receptors (AT,) would also put
the fetus at risk, but with the large number of acceptable
alternatives these agents should not be used.
Chronic HypertensionEssential Hypertension
Essential hypertension is a major risk factor for the devel-
opment of superimposed preeclampsia. Some women with
essential hypertension fail to have the decrease in blood pres-
sure that is a manifestation of vasodilatation in early preg-
nancy. When blood pressure determinations before pregnancy
are not available, the early lack of a decrease in blood pressure
will be missed and the diagnosis of chronic hypertension
sometimes may not be certain until postpartum follow-up.
Hypertension due to preeclampsia resolves within 7 days after
delivery. Some women with essential hypertension will have
resolution of hypertension immediately after delivery but will
develop hypertension in later years or during a subsequent
pregnancy. Table 2 highlights the clinical features of hyper-
tensive disorders and demonstrates how essential hypertension
can sometimes be differentiated from the other causes of hy-
pertension in pregnancy.
Women already receiving antihypertensive therapy are usu-
ally continued on their medication during pregnancy. This
includes continuation of a diuretic when it is part of the usual
regimen. ACE! and angiotensin !I receptor blockers should be
discontinued as soon as pregnancy is recognized. The devel-
opment of mild hypertension, even early in pregnancy, presents
a more controversial issue. Small elevations in blood pressure
are not likely to be harmful to mother or fetus. However, more
severe elevations in blood pressure are risky to both the mother
and fetus. Maternal risks are largely related to cerebral hem-
orrhage. Fetal risks include intrauterine growth retardation and
death. Most practitioners would agree with starting antihyper-
tensive therapy when diastolic blood pressure exceeds 100
mmHg. Because fetal mortality is increased when blood pres-
sure exceeds 85 to 90 mmHg, some would argue for the
initiation of antihypertensive therapy at these levels of blood
pressure. However, prospective, randomized, controlled trials
have not consistently demonstrated maternal or fetal benefit for
treatment of mild hypertension in pregnancy (14,26). Many
epidemiologists have argued that the reported studies have
been too small to demonstrate small beneficial effects of anti-
hypertensive therapy. However, many studies are also too
small to demonstrate possible infrequent detrimental effects of
too aggressive antihypertensive therapy. The reader should be
reminded that the debate centers mostly on therapy of mild
hypertension. Experts now recommend the use of antihyper-
tensive therapy for moderately severe hypertension complicat-
ing pregnancy (27).
Secondary Hypertension
Secondary causes of hypertension occasionally present in-
teresting problems in pregnancy. Progesterone has the capabil-
ity of antagonizing the kaliuretic effect of mineralocorticoids.
In women with hyperaldosteronism, the antagonism of miner-
alocorticoids by progesterone during pregnancy is variable.
Some women with primary hyperaldosteronism have reversal
of potassium wasting and less hypertension during pregnancy.
In others, hypertension due to sodium retention is exacerbated
by pregnancy and occasionally results in severe hypertension.
Pheochromocytoma is notable for its ability on rare occa-
sions to have a dramatic presentation during pregnancy with
fatal or near-fatal complications. Unrecognized, maternal and
fetal mortality in pheochromocytoma approaches 25%. With
appropriate use of aipha-adrenergic blockers, maternal mortal-
ity can be prevented, although some risk to the fetus persists.
References1. Grimes DA: The morbidity and mortality of pregnancy: Still
risky business. Am J Obstet Gynecol 170: 1489-1494, 1994
2. Schiff E, Peleg E, Goldenberg M, Rosenthal T, Ruppin E, Ta-
makin M, Barkai 0, Ben-Baruch G, Yahal I, Blankstein J,
Goldman B, Mashiach 5: The use of aspirin to prevent pregnan-cy-induced hypertension and lower the ratio of thromboxane A2
to prostacyclin in relatively high risk pregnancies. N EngI J Med
32: 351-356, 1989
3. Uzan 5, Beaufils M, Breat G, Bazin B, Capitant C, Paris I:
Prevention of fetal growth retardation with low-dose aspirin:
Findings of the EPREDA trial. Lancet 337: 1427-1431, 1991
4. Beaufils M, Uzan 5, Donsimoni R, Colau IC: Prevention of
pre-eclampsia by early antiplatelet therapy. Lancet i: 840-842,
1985
5. Imperiale TF, Petrulis AS: A meta-analysis of low-dose aspirin
for the prevention of pregnancy-induced hypertensive disease.
JAMA 266: 260-264, 1991
6. Sibai BM, Caritis SN, Thom E, Klebanoff M, McNellis D, Rocco
L, Paul RH, Romero R, Witter F, Rosen M, Depp R: Prevention
of preeclampsia with low-dose aspirin in healthy, nulliparous
pregnant women. N Engl J Med 329: 1213-121 8, 1993
Pregnancy: A Risky Business 321
7. Collaborative Low Dose Aspirin Study in Pregnancy (CLASP)
Collaborative Group: CLASP: A randomised trial of low-dose
aspirin for the prevention and treatment of pre-eclampsia among
9364 pregnant women. Lancet 343: 619-629, 1994
8. ECPPA Collaborative Group: ECPPA: Randomised trial of low
dose aspirin for the prevention of maternal and fetal complica-
tions in high risk pregnant women. Br J Obstet Gynaecol 103:
39-47, 1996
9. Sibai BM, Caritis SN, Thom E, Shaw K, McNellis D: Low-dose
aspirin in nulliparous women: Safety of continuous epidural
block and correlation between bleeding time and maternal-neo-
natal bleeding complications. National Institute of Child Healthand Human Developmental Maternal-Fetal Medicine Network.Am J Obstet Gynecol 172: 1553-1557, 1995
10. CLASP Collaborative Group: Low dose aspirin in pregnancy and
early childhood development: Follow-up of the Collaborative
Low Dose Aspirin Study in Pregnancy. Br J Obstet Gynaecol
102: 861-868, 1995
1 1. Belizan JM, Villar I, Gonzalez L, Campodonico L, Bergel E:
Calcium supplementation to prevent hypertension disorders ofpregnancy. N Engi J Med 325: 1399-1405, 1991
12. Bucher HC, Guyatt GH, Cook RI, Hatala R, Cook DI, Lang ID,
Hunt D: Effect of calcium supplementation on pregnancy-in-duced hypertension and preeclampsia: A meta-analysis of ran-
domized controlled trials. JAMA 275: 1 1 13-1 1 17, 1996
13. Levine RJ, Hauth IC, Curet LB. Sibai BM, Catalano PM, Morris
CD, DerSimonian R, Esterlitz JR. Raymond EG, Bild DE, Cle-mens JD, Cutler IA: Trial of calcium to prevent preeclampsia.
N Engl J Med 337: 69-76, 1997
14. Phippard AF, Fischer WE, Horvath IS, Child AG, Korda AR,
Henderson-Smart D, Duggin GG, Tiller DI: Early blood pressure
control improves pregnancy outcome in primigravida womenwith mild hypertension. MedfAust 154: 378-382, 1991
15. Redman CWG, Beilin LI, Bonnar I, Ounsted MK: Fetal outcome
in trial of antihypertensive treatment in pregnancy. Lancet ii:
753-756, 1976
16. Mutch LMM, Moar VA, Ounsted MK, Redman CWG: Hyper-tension during pregnancy, with and without specific hypotensive
treatment. II. The growth and development of the infant in the
first year of life. Early Hum Dev 1: 59-67, 1977
17. Ounsted MK, Moar VA, Good Fl, Redman CWG: Hypertension
during pregnancy, with and without specific hypotensive treat-
ment: The development of the children at the age of four years.
Br J Obstet Gynaecol 87: 19-24, 1980
18. Rubin PC, Butters L, Clark DM, Reynolds B, Sumner DI,
Steedman D, Low RA, Reid IL: Placebo-controlled trial of
atenolol in treatment of pregnancy-associated hypertension. Lan-
cet I: 431-434, 1983
19. Butters L, Kennedy S. Rubin PC: Atenolol in essential hyper-tension during pregnancy. Br Med J 301: 587-589, 1990
20. Collins R, Yusuf 5, Peto R: Overview of randomised trials of
diuretics in pregnancy. Br Med J 290: 17-23, 1985
21. Ihle BU, Long P. Oats I: Early onset pre-eclampsia: Recognition
of underlying renal disease. Br Med J 294: 79- 8 1 , 1987
22. Reiter L, Brown MA, Whitworth IA: Hypertension in pregnancy:
The incidence of underlying renal disease and essential hyper-
tension.Am J Kidney Dis 24: 883-887, 1994
23. Hou SH, Grossman SD, Madias NE: Pregnancy in women with
renal disease and moderate renal insufficiency. Am J Med 78:
185-194, 1985
24. lones DC, Hayslett IP: Outcome of pregnancy in women with
moderate or severe renal insufficiency. N Engl J Med 335:
226-232, 1996
25. MMWR: Postmarketing surveillance for angiotensin-converting
enzyme inhibitor use during the first trimester of pregnancy:
United States, Canada, and Israel, 1987-1995. Morb Mortal
Weekly Rep 46: 240-242, 1997
26. Sibai BM, Mabie BC, Shamsa F, Viblar MA, Anderson GD: A
comparison of no medication versus methyldopa or labetalob in
chronic hypertension during pregnancy. Am J Obstet Gynecol
162: 960-966, 1990
27. Committee on Technical Bulletins of the American College of
Obstetricians and Gynecologists: ACOG technical bulletin: Hy-
pertension in pregnancy (Number 219, January 1996). mt J
Gynaecol Obstet 53: 175-183, 1996







![Index [assets.cambridge.org]assets.cambridge.org/97805211/96611/index/9780521196611_index.pdf · Index More information ... inpregnancy,55,56 alemtuzumab,477,563,564,572, 623 sideeffects,573](https://static.fdocuments.in/doc/165x107/5b0803d37f8b9a3d018b96c2/index-more-information-inpregnancy5556-alemtuzumab477563564572-623.jpg)