Hy rtro i ar di . y pat y - CORE · Hy rtro i ar di . y pat y VASKEN DILSIZIAN, MD, FACC, ROBERT O....
9
796 Myocardial sc he 1<la DetectedbyThallium it ysr RelatedtoCardiacArrestandSyncopein YoungPatientsWi Ith Hy rtro i ar di .y paty VASKENDILSIZIAN,MD, FACC,ROBERTO . BONOW,MD, FACC, STEPHENE .EPSTEIN,MD,FACC,LAMEHFANANAPAZIR,MD Bethesda,Maryland OhJeLives .Thepurposeofthisstudywastodeterminethe frequencyofmyocardialischemiaasapotentialmechanismfor cardiacarm .tandsyncopeInyoungpatientswithhypertrophic c - thywhoexperle suchcomplications. ie rund,Suddencardiacdeathandsyncopeoccurfre- quendyinpatientswithhypertrophiccardlomyopatlay .Although ventriculararrhythaniasaccountformostoftheseeventsinadult patients,themechanism responsible forcardiacarrestandsyn- cope inyoungpatientshasnotbeenestablished. Me" .Twenty-threepatientswithhypertrophlccardiomy- opaathy,aged6to23years,withpreviouscardiacarrest(n W 8), syncope(a=7)orafamilyhistoryofsuddencardiacdeath(n 8)wereevaluatedtodeterminetheprevalenceofspontaneous ambulatoryventriculartachycardia(24®to72-helectrocardio- graphic(ECG)monitoring),exercise-inducedmyocardial isch- emia(thalliumscintigraphy)andinducibilityofventriculartachy- (el physiologic studies) . Results .ThreeofIS patientswithahistoryofcardiacarrestor syncopehadventricular ycardiaonambulatoryECGmoni- Hypertrophiccardiomyopathy in childhoodisassociated withapoorprognosis (1-6) ; approximately50%ofpatients inwhomthediagnosisisestablishedbetweentheagesofl and14years diesuddenlywithin9yearsofdiagnosis (1,3,5,6). Thishighmortalityrateobservedinprevious studiesoccurreddespiteselectioncriteriathatexcluded childrenwithafamilyhistoryofmultiplesuddendeaths . Inthepastfewyears,severalpotentialmechanismsfor cardiacarrestandsyncopehavebeenidentifiedinpatients withhypertrophiccardiomyopathy (7-13) .Inadults,ventric- ulararrhythmiasareveryprevalentandarebelievedtobe themostimportantcauseofsuddencardiacarrestand syncope ;abouthalfoftheadultpatientswithprevious cardiacarrestorsyncopehavenonsustainedventricular FromtheCardiolyBranch, NationalHeart,Lung,andBloodInstitute andtheDepartmentofNuclearMedicine,NationalInstitutesofHealth, Bethesda,Maryland . ManuscriptreceivedJannary29,t992 ;revisedmanuscriptreceivedFeb- ruary18,1993,acceptedMarch2,1993, fm' cone ence ; VaskenDilsizian,MD, National Institutes ofHealth,Building10,Room7B-13,Bethesda .Maryland20892 . c1993bytheAmericanCollegeofCardiology JACCVol .22,No . 3 September1993:796-504 HYPERTROPHICCARDIO YOPATHY toting .However,all15patients,hadinducibleischemiaby thalliumscintigraaphycomparedwithonly3(37%)ofIpatients withnosuchhistory(p<0 .01) . lot contrast,ventriculartachy- cardlainductionwasuncommoninalloftheyoungpatients(27 Inthosewithcardiacarrestorsyncope,0 intheothers) .During therapyforischemiawithverapamilaloneorincombinationwith beta-adrenergicblockingagents,only4ofthe15patientswith cardiacarrestorsyncopehadfurtherepisodes .Inthreeofthe fourpatients,theseeventsweretemporallyrelatedtodiscontinu- ationofverapamil .Amongeightpatientswhohadarepent exercisethalliumstudywhilereceivinganti-ischemictherapy, seven ( %)hadimprovedregionalthalliumuptake,ofwhom threehadnormalthalliumstudies, Conclusions . Thesedatasuggestthatinyoungpatientswith hypertrophiccardiomyothy,suddencardiacarrestorsyncope isfrequentlyrelatedtoischemiaratherthantoaprimaryarrhyth . mogenicventricularsubstrate . (JAmCollCordial1993,22 :796--804) tachycardiaduringambulatoryelectrocardiographic(ECG) monitoring,andmorethantwothirdsofcardiacarrest survivorshaveaninducible,sustainedventriculartachycar- diabyprogrammedelectricalstimulation(11,12) .However, inyoungpatientswithhypertrophiccardiomyopathywho havesustainedapreviouscardiacarrest,ventricularar- rhythmiasareinfrequentonambulatoryECGmonitoring (3-5' ;,suggestingthattheprimarymechanismforsudden deathinyoungpatientsdiffersfromthatinadults . Anginaandmyocardialischemiaareprominentfeatures ofhypertrophiccardiomyopathyinadultpatients,andevi- dencesuggeststhatischemiacanbepresenteveninyoung asymptomaticpatients(12-18) .Itisthereforepossiblethat ischemiamaycontributetothedevelopmentofsyncopeand suddencardiacarrestinsuchpatients .Theobjectivesofthis study,therefore,weretodetermineI)thefrequencyof myocardialischemiaasapotentialmechanismofcardiac arrestandsyncopeinyoungpatientswithhypertrophic cardiomyopathywhoexperiencedsuchcomplications,and 2)whetheranti-ischemicmedications,suchasbeta- adrenergicorcalcium-channelblockingagents,canprevent 0735-10971931$6.00
Transcript of Hy rtro i ar di . y pat y - CORE · Hy rtro i ar di . y pat y VASKEN DILSIZIAN, MD, FACC, ROBERT O....
796
Myocardial sc he 1<la Detected by Thallium
i t y s rRelated to Cardiac Arrest and Syncope in Young Patients WiIth
Hy rtro i ar di . y pat y
VASKEN DILSIZIAN, MD, FACC, ROBERT O . BONOW, MD, FACC,
STEPHEN E . EPSTEIN, MD, FACC, LAMEH FANANAPAZIR, MD
Bethesda, Maryland
OhJe Lives. The purpose of this study was to determine thefrequency of myocardial ischemia as a potential mechanism for
cardiac arm. t and syncope In young patients with hypertrophicc
- thy who experle
such complications.ie r und, Sudden cardiac death and syncope occur fre-
quendy in patients with hyp ertrophic cardlomyopatlay . Althoughventricular arrhythanias account for most of these events in adultpatients, the mechanism responsible for cardiac arrest and syn-cope in young patients has not been established.Me". Twenty-three patients with hypertrophlc cardiomy-
opaathy, aged 6 to 23 years, with previous cardiac arrest (n W 8),syncope (a = 7) or a family history of sudden cardiac death (n8) were evaluated to determine the prevalence of spontaneousambulatory ventricular tachycardia (24® to 72-h electrocardio-graphic (ECG) monitoring), exercise-induced myocardial isch-emia (thallium scintigraphy) and inducibility of ventricular tachy-
(el
physiologic studies) .Results. Three of IS patients with a history of cardiac arrest or
syncope had ventricular
ycardia on ambulatory ECG moni-
Hypertrophic cardiomyopathy in childhood is associatedwith a poor prognosis (1-6) ; approximately 50% of patientsin whom the diagnosis is established between the ages of land 14 years die suddenly within 9 years of diagnosis(1,3,5,6). This high mortality rate observed in previousstudies occurred despite selection criteria that excludedchildren with a family history of multiple sudden deaths .
In the past few years, several potential mechanisms forcardiac arrest and syncope have been identified in patientswith hypertrophic cardiomyopathy (7-13). In adults, ventric-ular arrhythmias are very prevalent and are believed to bethe most important cause of sudden cardiac arrest andsyncope; about half of the adult patients with previouscardiac arrest or syncope have nonsustained ventricular
From the Cardiol y Branch, National Heart, Lung, and Blood Instituteand the Department of Nuclear Medicine, National Institutes of Health,Bethesda, Maryland.
Manuscript received Jan nary 29, t992 ; revised manuscript received Feb-ruary 18, 1993, accepted March 2, 1993,
fm' cone
ence; Vasken Dilsizian, MD, National Institutesof Health, Building 10, Room 7B-13, Bethesda. Maryland 20892 .
c1993 by the American College of Cardiology
JACC Vol . 22, No . 3September 1993:796-504
HYPERTROPHIC CARDIOYOPATHY
toting. However, all 15 patients, had inducible ischemia bythallium scintigraaphy compared with only 3 (37%) of I patientswith no such history (p < 0 .01) . lot contrast, ventricular tachy-cardla induction was uncommon in all of the young patients (27In those with cardiac arrest or syncope, 0 in the others) . Duringtherapy for ischemia with verapamil alone or in combination withbeta-adrenergic blocking agents, only 4 of the 15 patients withcardiac arrest or syncope had further episodes . In three of thefour patients, these events were temporally related to discontinu-ation of verapamil. Among eight patients who had a repentexercise thallium study while receiving anti-ischemic therapy,seven ( %) had improved regional thallium uptake, of whomthree had normal thallium studies,
Conclusions . These data suggest that in young patients withhypertrophic cardiomyo thy, sudden cardiac arrest or syncopeis frequently related to ischemia rather than to a primary arrhyth .mogenic ventricular substrate .
(J Am Coll Cordial 1993,22 :796--804)
tachycardia during ambulatory electrocardiographic (ECG)monitoring, and more than two thirds of cardiac arrestsurvivors have an inducible, sustained ventricular tachycar-dia by programmed electrical stimulation (11,12) . However,in young patients with hypertrophic cardiomyopathy whohave sustained a previous cardiac arrest, ventricular ar-rhythmias are infrequent on ambulatory ECG monitoring(3-5';, suggesting that the primary mechanism for suddendeath in young patients differs from that in adults .
Angina and myocardial ischemia are prominent featuresof hypertrophic cardiomyopathy in adult patients, and evi-dence suggests that ischemia can be present even in youngasymptomatic patients (12-18) . It is therefore possible thatischemia may contribute to the development of syncope andsudden cardiac arrest in such patients . The objectives of thisstudy, therefore, were to determine I) the frequency ofmyocardial ischemia as a potential mechanism of cardiacarrest and syncope in young patients with hypertrophiccardiomyopathy who experienced such complications, and2) whether anti-ischemic medications, such as beta-adrenergic or calcium-channel blocking agents, can prevent
0735-10971931$6.00

JACC VW . 22, No . 3
DILSIZIAN ET AL .September 1993 :796-804
MYOCARDIAL ISCHEMIA IN YOUNG FATIENTS WiTH HYPERTROPHiC CARD OM-VOPATHY
future episodes of cardiac arrest and syncope in thesepatients .
Methods
Patient selection. Twenty-three young patients with hy-pertrophic cardiomyopathy, aged 6 to 23 years, with previ-ous cardiac arrest (n := 8), syncope (n = 7) or a family historyof sudden cardiac death (n = 8) were evaluated to determinethe prevalence of spontaneous ambulatory ventricular tachy-cardia (24- to 72-h ECG monitoring), exercise-induced myo-cardial ischemia (thallium scintigraphy) and inducibility ofventricular tachycardia (electrophysiologic studies) . All pa-tietus underwent a history and physical examination, chestX-ray study, ECG, echocardiography, 24- to 72-h ECGmonitoring, exercise thallium tomography, radionuclide an-giography and electrophysiologic studies . The diagnosis ofhypertrophic cardiomyopathy was based on the echocardio-graphic demonstration of a nondilated, hypertrophied leftventricle (wall thickness ~ 14 mm) in the absence of anothercardiac or systemic cause for the left ventricular hypertro-phy (19). Significant left ventricular outflow tract obstructionwas defined as a left ventricular outflow tract gradient?30 mm Hg under basal conditions or ?50 mm Hg afterprovocative maneuvers (Valsalva maneuver, amyl nitriteinhalation or isoproterenol infusion) . All studies were per-formed after discontinuation of all cardiac medications .There were 14 male and 9 female patients .
All patients consented to undergo exercise thallium to-mography and electrophysiologic studies . The NationalHeart, Lung, and Blood Institutional Committee on HumanResearch approved these studies for patients with hypertro-phic cardiomyopathy under protocol 84-H-232 . The wholebody radiation dose resulting from thallium scintigraphy isl .1 rem, with a cardiac dose of 1 .6 rem .
Exercise thallium singlo-photon emission computed tomo-graphic imaging. Patients underwent exercise thallium-201single-photon emission computed tomography (SPECT), aspreviously described (20) . After an overnight fast, exercisethallium scintigraphy was performed according to a stan-dardized multistage, symptom-limited (i .e ., chest pain,shortness of breath, fatigue) treadmill exercise test withcontinuous monitoring of symptoms, 17-.CG, heart rate andblood pressure . At peak exercise, 1 .5 to 2 mCi of thallium-201 was administered intravenously, and the patient contin-ued exercise for an additional 45 to 60 s . After termination ofexercise, thallium images were obtained using a wide field ofview rotating gamma camera equipped with a low energy,medium resolution, high sensitivity, parallel hole collimator(Apex 415, APC-3, Elscint Co .) centered on the 68-keVphotopeak with a 20% window . The camera was rotated overa 180° arc in an elliptic orbit about the patient's thorax from40° right anterior oblique to 40° left posterior oblique at 6°increments for 30 s each . Images were acquired 3 to 4 h afterexercise and after the administration of 0 .5 to I mCi ofthallium-201 reinjection at rest (20) . From the raw scinti-
graphic data, horizontal long-axis, vertical long-axis andshort-axiss tomograms were reconstructed, and four consec-utive representative slices of each view were selected forinterpretation . The reconstructed stress and reinjection im-ages were then analyzed qualitatively .
egional thallium analysis . The distribution of thalliumuptake was analyzed qualitatively in the three standardorthogonal tomographic imaging planes as follows : the sep-tal, apical and lateral regions in the horizontal long-axis(transaxial) view; the anterior, apical and inferior regions inthe vertical long-axis (sagittal) view, and the anterior, septal,inferior and lateral regions in the short-axis (oblique) view .The stress and reinjection images were normalized to theregion with the maximal myocardial activity in the stressimages . Four consecutive representative slices of each viewwere dispioyed simultaneously for interpretation . The im-ages were graded by two experienced observers, in a blindedmanner, on a 4-point scale from 3 (+++) = markedlyreduced/absent activity to 2 (++) = moderately reduced, I(+) = mildly reduced and 0 H = normal. The gradeassigned to a given region was the lowest regional score fromall tomographic slices and views . A counts-based quantita-tive analysis based on absolute thallium activity was notperformed because the marked regional heterogeneity ofwall thickness in hypertrophic cardiomyopathy would ac-centuate partial volume effects in a region to region compar-ison within one tomographic plane (21) .
Electrophysiologic studies . All patients underwent elec-trophysiologic studies involving the assessment of sinusnode function, atrioventricular node and His-Purkinje con-duction, atria( and ventricular refractoriness and pro-grammed ventricular stimulation, as previously described(11). After an overnight fast and sedation with I to 4 mg ofintravenous midazolam, three multiple electrode catheters(5F or 6F, Bard or Mansfield) were introduced percutane . -ously into a femoral vein and positioned under fluoroscopicguidance in the high right atrium, across the tricuspid valvein the region of the His bundle and at the right ventricularapex. A femoral artery was also cannulated for continuousrecording of the systemic arterial pressure. After pro-grammed atrial stimulation, the high right atrial catheter wasrepo°~itioned in the right ventricular outflow tract for pro-grammed ventricular stimulation. The programmed ventric-ular stimulation protocol involved a stepwise increase in"aggressiveness" as follows: 1) insertion of one, two andthree premature stimuli during sinus rhythm at the rightventricular apex ; 2) introduction of one and two prematurestimuli after three paced ventricular drive cycle lengths of600, 500 and 400 ms, first at the right ventricular apex andthen at the right ventricular outflow tract ; 3) introduction ofthree premature stimuli after the three paced drive cyclelengths at the right ventricular apex and right ventricularoutflow tract ; and 4) insertion of one, two, and threepremature stimuli after the three drive cycle lengths at a leftventricular site . The end point of the stimulation protocolwas refractoriness or induction of a sustained ventricular
797

798 DILSIZIAN ET AL.
JACC Vol . 22, No . 3MYOCARDIAL ISCHEMIA IN YOUNG PATIENTS WITH HYPERTROPHIC CARDIOMYOPATHY
September 1993 :796-804
Table 1 . Characteristics of Young Patients With Hypertrophic Cardiomyopathy
arrhythmia (>30-s duration or requiring rapid terminationdue to hemodynamic compromise) .
Patient management and follow-up. All patients with car-diac arrest who had a suitable body habitus were providedwith an implantable defibrillator. All patients with symptomsof impaired consciousness and evidence of exercise-inducedmyocardial ischemia were also treated with verapamil orbeta-blockers, or both . Patients with syncope in whomprogrammed electrical stimulation induced a sustained ven-tricular tachycardia were initially treated with antiarrhyth-mic drugs. If pharmacotherapy did not prevent subsequentinduction of ventricular tachycardia, the patient was pro-vided with an implantable defibrillator . Asymptomatic pa-tients were treated only if programmed stimulation withtwo or fewer premature stimuli resulted in induction ofa sustained ventricular tachycardia. Follow-up consisted of3- to 6-month clinic visits and telephone interrogation ofpatients, their relatives and cardiologists .
Statistical analysis. Data are presented as mean value tSD. Differences between myocardial ischemia by thalliumscintigraphy and inducible ventricular tachycardia by elec-trophysiologic studies in patients with cardiac arrest orsyncope and those with a family history of sudden cardiacdeath were performed by chi-square analysis . Dfferencesbetween patients with and without impaired consciousnesswith respect to age, and results of treadmill exercise, 24- to72-h ECG monitoring, echocardiography, left ventricularend-diastolic pressure measurements, rest and provokableleft ventricular outflow tract gradients and ejection fractionwere analyzed by either two-tailed unpaired t test 4)r chi-square analysis .
Values presented are mean value ± SD or number . ECG = electrocardiographic ; HR = heart rate ; IVSinterventricular septal thickness ; LVEDP = left ventricular end-diastolic pressure ; LVEF = left ventricular ejectionfraction ; LVOT - left ventricular outflow tract ; PW = posterior wall ; RPP = rate-pressure product ; SAM = systolicanterior motion of the mitral valve ; VT = ventricular tachycardia.
ResultsThe data acquired in the 23 patients were analyzed
accordhig to their symptomatic presentation . One groupcomprised patients with a previous history of cardiac arrestor syncope; the other group comprised those who had only afamily history of cardiac arrest (Table 1) . The patients witha previous history of cardiac arrest or syncope achieved alower peak heart rate and rate-pressure product . Six of the15 patients with a history of impaired consciousness hadexercise-induced angina compared with only I of 8 patientswith no such history. Only 3 of 15 patients with a history ofimpaired consciousness had ventricular tachycardia during24- to 72-h ambulatory ECG monitoring . On M-mode echo-cardiography, the interventricular septal thickness, septal/posterior free wall ratio and the incidence of systolic anteriormotion of the mitral valve were not different between thetwo groups. The two groups also did not differ with respectto left ventricular end-diastolic pressure, left ventricularejection fraction and the frequency of significant left ventric-ular outflow tract gradients at rest and during provocation .
Prevalence of myocardial ischemia. The prevalence ofexercise-induced myocardial ischemia by thallium SPECTand of inducible ventricular I lachycardia by electrophysio-logic study in the 23 young patients with hypertrophiccardiomyopathy is presented in Table 2 . All 15 patients witheither cardiac arrest or syncope developed myocardial isch-emia on exercise thallium studies compared with 3 (37%) of8 patients with a family history of sudden cardiac death (p <0.01) .
Details of all exercise treadmill and thallium scintigraphic
Cardiac Arrestor Syncope(n = 15)
Family Historyof Cardiac Arrest
(n = 8) p Value
Age (yr) 15 ± 5 19±4 NSTreadmill exercise
Duration (min) 8 ± 2 10 . 4 NSPeak HR (beats/min) 155 ± 27 181 ± 15 < 0.01RPP (1010 3 ± 5 29±5 <0.001Angina Os 1/8 NS
24-72-h ECG monitor (VT) 315 0/8 NSEchocardiographyIVS (mm) 24 ± 10 NS23±9IVSIPW (mm) 2 .2
0.8 2.1 ± 0 .7 NSSAM 5115 418 NS
CatheterizationLVEDP (mm Hg) 14±7 NS18 . 7LVOT obstructionRest (130 mm Hg) 2/8 NS2/ 15Provocation QM mm Hg) N15 5/8 NS
Radionuclide angiography, LVEF 68 ± 13 79 ± 10 NS

JACC Vol . 22, No . 3September 1993 :796-804
Table 2 . Prevalence of ti rocardial lqchemia by ThalliumScintigraphy and Inducible Wentricular Tachycardia byElectrophysiologic Study
Cardiac arrest or syncope
15115 0013%)*
4115 (27%)Family history of cardiac arrest
318 (37%)*
018 (0%)
DILSIZIA'N ET AL .
F91)MYOCARDIAL ISCHEM9A IN YOUNG PATIENTS MTH HYPERTROPHIC CARDIOMYOPATHY
TI-201 SPELT,
EP Study .Ischemin
Innducible VT
*P < 0 .01 . EP = clectrophysiologic ; SPECT = single-photon emissioncomputed tomography ; T1 = thallium ; VT = ventricular tachycardia .
data are presented in Table 3 . Ischemic ST segment depres-sion during exercise was present in 9 of 15 patients witheither cardiac arrest or syncope, and all 9 patients hadassociated ischemia by thallium scintigraphy . However,thallium scintigraphy identified six additional patients withmyocardial ischemia who had no ECG evidence of ischerniaor tracings that were uttinterprelable for ischemia because ofleft bundle branch block or paced rhythm . Exercise-inducedventricular arrhythmias did not occur in any patient duringtheir supervised treadmill test . Thallium abnormalities oc-curred most commonly in the aateroapical and sepia] regionsof the left ventricle ; 15 of the 18 patients with exercise-induced myocardial ischemia had thallium abnormalitiesin more than one region . Eleven patients had apparentexercise-induced left ventricular cavity dilation and threepatients had increased lung uptake of thallium during exer-cise .
Prevalence of inducible ventricular tachycardia. Only 4(27%) of 15 patients with either cardiac arrest or syncope andnone of 8 patients with a family %istory of cardiac arrest hada sustained ventricular tachycardia induced during pro-grammed electrical stimulation . Ali four patients had sus-tained polymorphic ventricular tachycardia that was induc-ible at a right ventricular site . None of the patients had anyother electrophysiologic abnormalities that would haveplayed a role in their sudden cardiac arrest or syncope .
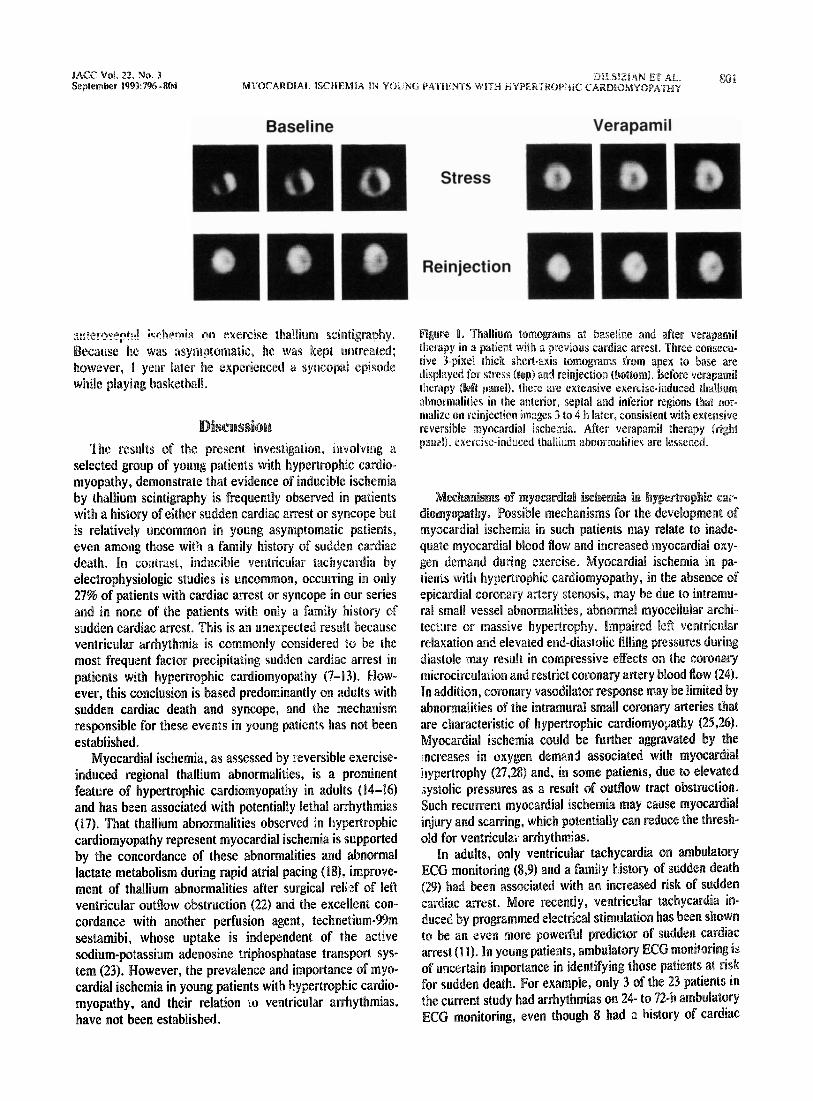
Long-term follow-up and therapeutic response, All pa-tients who had previous cardiac arrest or syncope and whoalso had exercise-induced thallium perfusion defects re-ceived anti-ischemic therapy with verapamil, alone or in com-bination with a beta-blocker. Eight patients had follow-upthallium studies during anti-ischemic therapy. Regional thal-lium defects essened in 18 of 21 regions, associated with areduction in defect severity score from 1 .9 ± 0.6 to 0.6 ± 0.8(p < 0.001). Seven (88%) of the eight patients had improvedregional thallium uptake on medical therapy, of whom threehad completely normal thallium studies . All three patients withexercise-induced left ventricular cavity dilation before therapyhad reduced cavity size on medical therapy . An example of apatient with improvement in exercise-induced myocardial isch-emia and apparent cavity dilation during verapamil therapy isshown in Figure 1 .
Of the nine patients with ischemic ST segment depressionon baseline exercise study, six had follow-up exercise tread-mill studies while they were receiving anti-ischemic therapy .
iwhemic ST segment changes lessened with medical therapyin five (83%) of the six patients, of whom four had no ECGevidence for ischemia . These ECG improvements frombefore to after medical therapy occurred at comparableexercise duration (8 .5 ± 2.0 and 9 .8 ± 2.0, p = NS), heartrate (157 ± 23 and 162 ± 16, p = NS) and rate-pressureproduct (18 X 103 ± 5 and 20 X 10' ± 6, p = NS) . Three ofthe nine patients also had improvement in symptomaticexercise end points .
During a mean follow-up period of 23 ± 6 months, 4 of the15 patients with symptoms of impaired consciousness hadfurther events, only I of whom had beet found on electro-physiologic study to have inducible ventricular tachycardia .The first patient was a 9-year old girl with documentedmyocardial ischemia who had had multiple recurrent epi-sodes of cardiac arrest and syncope before verapamil ther-apy, She had an episode of presyncope about 6 h after failingto take her verapamil dose at home .
The second patient, I I years old, with a previous cardiacarrest and evidence of exercise-induced myocardial ischemiain the absence of electrophysiologic abnormalities, had twoepisodes of syncope within 12 h of in-hospital discontinua-tion of verapamil and beta-blocker therapy . The syncopalepisodes were precipitated by sinus tachycardia and wereassociated with marked ST segment depression, hypoten-sion and polymorphic ventricular tachycardia that was ter-minated by defibrillator discharges (Fig . 2). An episode ofpresyncope in the same patient was associates with tachy .,cardia and ST segment depression and nonsustained poly .morphic ventricular tachycardia (Fig . 2) .
The third patient, 19 years old, with a previous cardiacarrest and findings of exercise-induced myocardial ischemia(in the absence of electrophysiologic abnormalities), had anepisode of syncope accompanied by a discharge from animplantable defibrillator while standing, about 30 min aftervigorous exercise . At the time of the event she was receivingverapamil (240 mg/day) ; however, after the verapamil dosewas increased to 360 mg/day, she has had no further epi-sodes .
The fourth patient, an 1,1,'-year old woman with a previouscardiac arrest who had both exercise-induced myocardialischerckia and inducible, s ::-rained polymorphic ventriculartachycardia at electrophysiologic study, was provided withan implantable defibrillator and treated medically with abeta-blocker and verapamil . She was otherwise free fromcardiac symptoms . When the medications were discontin-ued, she had a syncopal episode on exercise testing ; this wasassociated with induction of a sustained polymorphic ven-tricular tachycardia that was terminated by a single dis-charge by the defibrillator . After resuming her medication,she had no further episodes during a 2-year follow-up .
In contrast to the patients with impaired consciousness,only one of the eight patients with no such history had anevent on long-term follow-up. This patient was a 14-year oldboy with a normal ambulatory ECG recording and noinducible ventricular tachycardia who developed septal and

Ahk
3.Exercise
Trea
dmiH
and11
mMum
ScintigraphicLiu123Ymmg
FwNts
With
Hype
rtro
phic
Card
kaiy
opaf
t
PI
T
Exer
cise
ion
PeatHR
RPP
Dew
Miractoltum
Time to 2-3MM
KnITBw
AmbM
aMea
l
Cavity
No
.
V
Not
(IMM
AK)
minis
minds
34yotsudial Region
Seve
rity
of
Defe
ct
Uptake
Dilation
V ti 5: t,>
IArr
MApIAUVI-
++/++/++
al
9
7/M Pre
10
P15/Fost,
Vtrp
/BB
Pre
Post; Verp
lPro
cam
11
151M Pre
1217/M Pre
Post, Verp
/BB
13
18/F Pr
e14
21/M Pre
22MPost, Oilt
pre
Past
, Ve
rplProcain
15 16
I
6&/M Pre.wn a
n
6'
130
12.5
Post; VerpMDD pace
6
170
18.7
ITUI
S1301
,
101=
rhyt
hm2
9/F Pre
3130
,
87
10.4
4Po
st;
Verp
/BB
No r
epea
t st
udy
3
11/M Pre
9117
1,
123
9.1
12Po
st-,V
erp/BB
11'44"
137
12.3
0
-4
14/M Pre
10'21"
159
17-3
3
3'31
Post. Verp
/AIC
D
7'16"
148
16-1
2
4'13"
5
IS/F Pr
e
9151,
136
16.9
2
3156
1,6
P19/
17ost,
VerpJAICD
9131
,
07
20.1
-
-
Pre
7'40"
170
24.5
4
0'53
"Post, Verp/AICD
11,0
1,
E74
22b
0
-7
i9/F Pre
6'5"
170
20.7
0
-
8
P19
JFos
t;Ver
p/AI
CD
9119
1,
163
23.5
0
-
Pre
91011
153
15.8
LBBB
-Post, Verp/AICD
No r
epea
t st
udy
14/M Pre
Post
, Ve
rp15/M Pre
15/F Pr
e17/M Pre
20M Pre
22/F Pr
e22
23/M Pr
ePo
st,
Verp
23
23/M Pr
e
17 18 19 20 21
91011
187
15.3
39'30"
147
123
09'30I
178
24. 2
0No
rep
eat
stud
y
4'37"
155
20.8
156
22.6
170
20.2
26.5
6',M"
10,511
,
owl
12'0"
12'38"
V31"
No
repe
at s
tudy
11101
11ITWI
8'5"
9101,
low
,
10,251
,6'75"
6'0"
9101
,
1301
-
10 180
188
152
163
174
20-2
32.1
19.0
24.o
211
31-8
195
192
34.4
is
32.8
187
32.9
163
25.7
164
21.6
165
24.9
182
28.8
Foamhr
Omm ( ok-w
Pro-
COW
ST S
egme
nt D
epre
ssio
n
- - -
T50"
Cache Mmes
shym
-Mil
e
With P
teeF
Thwa
pkit
Dyspnea
ApVAmr-p
+++/
+++/
++
-
++5'
05"
Asy-pt-
AP
+I-/
-
-
+6'
43"
AsymptatzWk
UMMIMp
+1+1+
--
Asy-p-
AYAU&q
+4+P++
-
+
1'06"
Dysp~ea
ApfA-Sep
++/++1++
-
++DYSP-
Ap
-
+
Chest pain
A--/'-PW
++/++I++
-Asymp-
Dyspnea
Ap,'
AnVS
ep
++/++I++
+
+
4'0"
51,08.1
Asyr
ript
o-fi
c-
AMmintonwic
Dysprea
7'05
"
Arm pain
Chest pain
Chest pain
Chest pain
3'30
"
Asys
upta
rabl
eAgnponinaw
Asym
ptom
atic
-
Asym
ptor
natic
Asymplomuc
-
Asym
plom
-ali
c-
Chest pain
3'23"
Asym
pton
iatic
-
Asympsortiat
ic
- - -
-
-
Hist
ory
Asymp--
ApJAPt
+++1
++
Mild c
Asym
ptom
atic
Ap AWSe
pAD
Am/S
ep
++/++
++/++
Ant/
Sep
+1+
ApIAMG-p
++/++/++
=fwnf
++/++/+++/++
thal
lium
sta
y
Ap.
JS-p
flri
f
AM 34
Q%T
Art/Seepiflnf
Ant
ApIS
cp/J
nf
++/++/++
Thal
lium
-201
Sci
atig
raph
ic D
ata
++
+
z
+0+"+++
+++/
++/+
+
+ +
;8
z*N
o patient manifested ventricular arrhythmia was present during exercise.
AICD
-au
toma
tic
intp
lant
able
car
diac
def
ibri
llat
or,
Ant
= an
teri
or; Ap = apical;
BB
= be
ta-a
dren
ergi
c bl
ocki
ng a
gent;
DDD
pace
= d
ual-
cham
ber
paci
ng m
ode; Dat a P
= di
ltia
zem;
F =
fem
ale;
HR = heart rate
; Inf = inferior
; La
t =
late
ral;
Pre
and
Pos
tbefore and after, respectively, thallium tomography and exercise study, Promin
=pr
ocai
mAde
;Pt
= P
atie
nt; RPP = rate-pressure ptoi!vct
; Se
p =
sept
al; Verp
W=
vera
pami
l; V
VI p
ace
= si
ngle
-cha
mber
ven
tric
ular
pac
ing
mode
;-= normal
; +
mild
ly r
educ
ed a
ctiv
ity;
+ + = moderately reduced activity
;...
= markedly
redu
ced/
abse
ntac
tivi
ty.
+++
I
JACC Vol . 22, No . 3September 1993 :796-804
ansenmer"-_E kohem~n on exercise thallium scintigraphy .Because he was asymptomatic, he was kept untreated ;however, I year later he experienced a syncopal episodewhile playing basketball .
Discussion
"The results of the present investigation, involving aselected group of young patients with hypertrophic cardio-myopathy, demonstrate that evidence of inducible ischemiaby thallium scintigraphy is frequently observed in patientswith a history of either sudden cardiac arrest or syncope butis relatively uncommon in young asymptomatic patients,even among those with a family history of sudden cardiacdeath. In contrast, inducible ventricular tachycardia byelectrophysiologic studies is uncommon, occurring in only27% of patients with cardiac arrest or syncope in our seriesand in none of the patients with only a family history ofsudden cardiac arrest . This is an unexpected result becauseventricular arrhythmia is commonly considered to be themost frequent factor precipitating sudden cardiac arrest inpatients with hypertrophic cardiomyopathy (7-13) . How-ever, this conclusion is based predominantly on adults withsudden cardiac death and syncope, and the mechanismresponsible for these events in young patients has not beenestablished .
Myocardial ischemia, as assessed by reversible exercise-induced regional thallium abnormalities, is a prominentfeature of hypertrophic cardiomyopathy in adults (14-16)and has been associated with potentially lethal arrhythmias(17). That thallium abnormalities observed in hypertrophiccardiomyopathy represent myocardial ischemia is supportedby the concordance of these abnormalities and abnormallactate metabolism during rapid atria] pacing (18), improve-ment of thallium abnormalities after surgical relief of leftventricular outflow obstruction (22) and the excellent con-cordance with another perfusion agent, technetium-99msestamibi, whose uptake is independent of the activesodium-potassium adenosine triphosphatase transport sys-tem (23) . However, the prevalence and importance of myo-cardial ischemia in young patients with bypertrophic cardio-myopathy, and their relation to ventricular arrhythmias,have not been established .
DtLSMAN ET AL.
R-0 iMYOCARDIAL ISCHEMIA IN YOUNG PATIFNTS WITH HYPERTROP7iiC CARDIOMYOPATHY
71eir4ection
figure 1 . Thallium tomograms at baseline and after verapamiltherapy in a patient with a previous cardiac arrest . Three consecu-tive 3-pixel thick short-axis tomograms from apex to base aredisplayed for stress (top) and reinjection (bottom) . before verapamiltherapy (left panel), there are extensive exercise-induced thalliumabnormalities in the anterior, septal and inferior regions that nor-malize on reinjection images 3 to 4 h later, consistent with extensivereversible myocardial ischemia . After verapamil therapy (rightpaaet), exercise-induced thallium abnormalities are lessened .
Mechanisms of myocardial ischemia in byptrilrophic car-diognyopathy. Possible mechanisms for the development ofmyocardial ischemia in such patients may relate to inade-quate myocardial blood flow and increased myocardial oxy-gen demand during exercise . Myocardial ischemiaa in pa-tients with hypertrophic cardiomyopathy, in the absence ofepicardial coronary artery stenosis, may be due to intramu-ral small vessel abnormalities, abnormal myocellular archi-tecture or massive hypertrophy. Impaired left ventricularrelaxation and elevated end-diastolic filling pressures duringdiastole may result in compressive effects on the coronarymicrocirculation and restrict coronary artery blood flow (24).In addition, coronary vasodilator response may be limited byabnormalities of the intramural small coronary arteries thatare characteristic of hypertrophic cardiomyopathy (25,26) .Myocardial ischemia could be further aggravated by theincreases in oxygen demand associated with myocardialhypertrophy (27,28) and, in some patients, due to elevatedsystolic pressures as a result of outflow tract obstruction .Such recurrent myocardial ischemia may cause myocardialinjury and scarring, which potentially can reduce the thresh-old for ventriculaiv arrhythmias .
In adults, only ventricular tachycardia on ambulatoryECG monitoring (8,9) and a family history of sudden death(29) had been associated with an increased risk of suddencardiac arrest. More recently, ventricular tachycardia in-duced by programmed electrical stimulation has been shownto be an even more powerful predictor of sudden cardiacarrest (11) . In young patients, ambulatory ECG monitoring isof uncertain importance in identifying those patients at riskfor sudden death . For example, only 3 of the 23 patients inthe current study had arrhythmias on 24- to 72-h ambulatoryECG monitoring, even though 8 had a history of cardiac

802
DILSIZIAN ET AL .MYOCARDIAL ISCHEMIA IN YOUNG PATIENTS WITH HYPERTROPHIC CARDIOMYOPATHY
A.
C.
ft
0.*Aft N
ft*q*"
L LA1114-4. L 1A
4-V 4--k-TV
L"LA44JA.1-"LJAAA
N
ft"
JW 1jV
0"
X
arrest and another 7 had a history of syncope . Similarfindings of extremely low prevalence of ventricular tachy-cardia on ambulatory ECG monitoring in young patientshave been previously reported by McKenna et al . (8) . Inaddition, and as mentioned earlier, only 4 of the 15 patientswith proved cardiac arrest or syncope had ventricular tachy-cardia induced by programmed electrical stimulation .
Identification of inducible myocardial ischemia by thal-lium scintigraphy in 37%, of patients who had no symptomsof impaired consciousness but had a family history of suddencardiac arrest may identify the subgroup of young, asymp-tomatic patients with hypertrophic cardiomyopathy who areat risk for a future cardiac event . One of the asymptomaticpatients in our series who had a positive thallium test had asubsequent syncopal episode several months later . In addi-tion, repeated episodes of ischemia in young patients may
NamMO0LLL_LULLl
L44j-"
***i-rvrrvv
E .
44u
i*y{;tr+,LL) LL.LdJ '
. . . . . . . . . . . -111-1
A
A
JACC Vol . 22, No . 3September 1993 :796-804
Figure 2. Electrocardiograms(ECGs) from an I I -year old boy Whowas referred because of a history ofrecurrent cardiac arrests . A, Thebaseline ECG shows minor ST-Twave abnormalities commonly seenin patients with hypertrophic cardio-myopathy . S, During treadmill exer-cise, 12-mm ST segment depressiondeveloped in the inferolateral leads .C, Serial telemetry ECG recordingsfrom the same patient at rest revealthe development of sinus tachycar-dia first associated with significantST segment depression, followed bya nonsustained polymorphic ventric-ular tachycardia . D, An episode ofpresyncope was associated with sus-tained polymorphic ventriculartachycardia that was terminated byan electric shock from an implant-able cardiac defibrillator . E, Anotherepisode of marked ST -,egment de-pression that was associated withhypotension (brachial artery pres-sure 60/40 nun Hg) and light-headed-ness was treated successfully withintravenous (iv) infusion of I mg ofpropranolol (Inderal) .
result in small areas of myocardial fibrosis . In those whosurvive to adulthood, such fibrotic areas may serve as focifor reentrant pathways responsible for the ventricular ar-rhythmias commonly encountered in adults with hypertro-phic cardiomyopathy . Thus, although definitive data arelacking, it would appear reasonable to treat young, asymp-tomatic patients with verapamil if they have evidence ofinducible ischemia and hypotension by stress thallium scin-tigraphy . This proposal is based on the evidence in this studyand others (16) that verapamil reduces the prevalence andseverity of ischemia during exercise .
Treatment of patients with hypertrophic cardiomyopathy .Medical treatment of hypertrophic cardiomyopathy has con-sisted primarily of administration of beta-blockers and cal-cium channel blockers. The mechanism responsible for thesalutary effects of beta-blocker therapy may relate to the

JACC Vol . 22, No . 3September 1993 :796-804
AutontaldeWC
11,311'b 111~11 'A a 1,
IndueffilLVentricularFachyeardia
Ahtomatlemptwmwcamwc
RAWK "
D:LSIZIAN ET AL .MYOCARDIAL SCHEMA IN YOUNG PATIENTS WITH HYPERTROPFUC CARDIOYOPATHY
StressTWMm
Symptoms eImpaired
donsciousnes
stressThWWm
Verapamil
Arrow
Seem forOther
TreatableCause
Syncope
LFallu
AutomaticImplabilaWeCardiac
ElectrolphpWVcSCardiac
L_(C -
I
Positive I
It
Beta!docker
Asymptomatic
FamiN Kieloryof
Cardiac Arrest
StressThallium
0~101RMEMOMM
Electrop"shloocstudy)Cardiac
Cathelerizallon
NoraoduciblevelltrimalawTachycardia
Search for otherTreatable Cannesia heart Much
bradpwAlaWPMOWWWW~mm"amm
inhibition of sympathetic stimulation of the heart and dimi-nution of myocardial oxygen requirements by reducing heartrate, left ventricular contractility, outflow tract obstructionand myocardial wall stress during exercise (30) . The firstevidence suggesting that beta-blockers may have a protec-tive effect against premature sudden death in young patientswith hypertrophic cardiomyopathy was provided by Fidleret al . (2) in 1978 . In their retrospective analysis of childrenwith hypertrophic cardiomyopathy, 7 (54%) of 13 children(with a mean outflow gradient of 41 mm Hg) who received notherapy died within a mean of 5 .2 years . In contrast, none ofthe seven children who received propranolol therapy (meanoutflow gradient 42 mm Hg) died .
Over the past decade, calcium channel blockers such asverapamil have also been shown to be effective therapeuticagents in hypertrophic cardiomyopathy (16,31-34) . Themechanism responsible for the beneficial effects of verapamilmay be partly due to diminished myocardial oxygen con-sumption and left ventricular contractility, similar to thatobserved with beta-blockers ; however, unlike beta-blockers,verapamil has also been shown to improve indexes of leftventricular relaxation and rapid diastolic filling (32-34) asso-ciated with enhanced exercise performance and reducedsymptoms (34) . Verapamil also has the capacity to dilatesmall arteries, an action that may have salutary effects inpatients with hypertrophic cardiomyopathy, who have beenshown to have both anatomic and functional abnormalities ofthe small coronary arteries (24,26) .
In the present study, 11 (73%) of 15 young patients whopresented with cardiac arrest or syncope had no furtherevents during treatment with verapamil alone or in combi-
MOMIDVentricular
Tachyeardia
AntiarrhythmicTherapy
NoninducibleVentricular =I I tIormalTachycirdia
Search for OtherTreatable Causes
.e . Imart blockMciparclasuprummmlartachycardla
outflowobstruction
3
----------------------------------------------
Figure 3. Schematic flow diagram for the management of youngpatients with hypertrophic cardiomyopathy .
nation with beta-blockers during a mean follow-up period of-2 years . In three of the four patients with events, the eventoccurred shortly after verapamil was discontinued . Further-more, 88% of patients who had a repeat exercise thalliumstudy while receiving anti-ischemic therapy had either re-duced or no myocardial ischemia . Thus, therapy with eithera beta-blocker or verapamil may diminish the likelihood ofinducible ischemia and thereby of recurrent syncope orcardiac arrest in young patients with hypertrophic cardiomy-opathy . However, a survivor of cardiac arrest who hadmyocardial ischemia on exercise thallium study, and who didnot have spontaneous or inducible ventricular arrhythmias,had an episode of exercise-induced syncope associated withdischarge by an implantable defibrillator during treatmentwith verapamil (240 mg/day) . Hence, it would appear pru-dc.nt to provide all children with cardiac arrest, who are ofsuitable body habitus, with an implantable defibrillator inaddition to anti-ischemic medical therapy . A proposed man-agement scheme for young patients with hypertrophic car-diomyopathy presenting with cardiac arrest, syncope orstrong family history of sudden cardiac death is outlined inFigure 3 .
Summary. The results of our study in a small group ofyoung patients with hypertrophic cardiomyopathy referredfor risk stratification suggest that cardiac arrest or syncope isfrequently related to myocardial ischemia rather than to aprimary arrhythmogenic left ventricular substrate . Further-more, anti-ischemic medications, such as beta-blockers and
JACC Vol. 22, No. 3MYOCARDIAL ISCHEMIA IN YOUNG PATIENTS WITH HYPERTROPHIC CARDIOMYOPATHY
September 1993 :796-1304804
DILSIZIi~N ET AL .
verapamil, appear to lessen symptoms and reduce the like-lihood of future episodes of sudden cardiac arrest in suchyoung patients .
References
1 . Maron BJ, Henry WL, Clark CE, Redwood DR, Roberts WC, EpsteinSE. Asymmetric septa] hypertrophy in childhood . Circulation 1976 ;53 :9-19.
2 . FidlerGi, TaJik AL Weidman WH, McGoon DC, Ritter DG, Giuliani ER .Idiopathic hypertrophic subaortic stenosis in the young . Am J Cardiol1978,42 :793-9 .
3 . McKenna WJ, Deanficid J, Faruqui A, et al . Prognosis in hypertrophiccardlomyopathy : role of age and clinical, electrocardiographic . and he-modynamic features . Am J Cardiol 1981 ;47 :532-8.
4 . Ma, vn BJ, Roberts WC, Epstein SE . Sudden death in hypertrophicca Kiomyopothy : a profile of 78 patients . Circulation 1982 :67 :1388-94 .
5, McKenna WJ, Deinfield JE . Hypertrophic cardiomyopathy : an importantcause of sudden death . Arch Dis Child 1984 :39 :971-5 .
6. McKenna WJ, Franklin RCG, Nihoyannopoulos P, et al . Arrhythmia andprognosis in infants, children and adolescents with hypertrophic cardio-myopathy. J Am Coll Cardiol 1988 ;11 :146-53 .
7, McKenna WJ, Chetty S, Oakley CM . Goodwin JF. Arrhythmia inhypertrophic cardiomyopathy : exercise and 48 hour ambulatory clectro-catiliographic assessment with and without beta adrenergic blockingtherapy. Am J Cardiol 1980,45 :1-5 .
8 . McKenna WJ, England D, Doi YL, Deanfield JE, Oakley CM, GoodwinJF . Arrhythmia in hypertrophic cardiomyopathy . I . Influence on progno-sis . Br Hew J 1981 ;46 :168-72 .
9. Macon BJ, Savage DD, Wolfson JK, Epstein SE . Prognostic significanceof 24 hour ambulatory electrocardiographic monitoring in patients withhypertrophic cardiomyopathy : a prospective study . Am J Cardiol 1981 ;48 :252-7 .
10, Nicod P, Polikar R, Peterson KL . Hypertrophic cardiomyopathy andsudden death, N Engl J Med 1988 ;318 :1255-7 .
11 . Fananapazir L, Tracy CM, Leon MB, et al . Electrophysiologic abnor-malities in patients with hypertrophic cardiomyopathy : a consecutiveanalysis in 155 patients . Circulation 1989;80 :1259-68 .
12, Fananapazir L . Epstein SE . Hemodynamic and electrophysiologic eval-uation of patients with hypertrophic cardiomyopathy surviving cardiacarrest . Am J Cardiol 1991 ;67 :280-7,
13 . Fananapazir L, Chang AC, Epstein SE . McAreavey D. Prognosticdeterminants in hypertrophic cardiomyopathy : prospective evaluation ofa therapeutic strategy based on clinical, Holter, hemodynamic, andclectmAysiological findings . Circulation 199.),,86,730-40 .
IC Pitcher D, Wainwright R, Maiscy M . Curry P, Sowton E. Assessment ofchest pain in hypertrophic cardiomyopathy using exercise thallium-201myocWW scintipphy, Br Heart J 198OA4 :650-6 .
I& O'Gara PT, Bonow RO, Maron BJ, et al . Myocardial perfusion abnor-malities in patients with hypertrophic cardiomyopathy : assessment withthdRum4ml emission computed tomography . Circulation 1987 ;76,,1214-23.
16 , Udtlson JE, Bonow RO, O'Gara PT, et al . Verapamil prevents silentmyocardial perfusion abnormalities during exercise in asymptomaticpatients with hypertmphic cardiomyopathy. Circulation 1989 ;79 :1052-60 .
17 . von Dohlen TW, Prisant LM, Frank ML Significance of positive or
negative thallium-201 scintigraphy in hypertrophic cardiomyopathy . Am JCardiol 1989 ;64:498-503 .
18 . Cannon RO, Dilsizian V, O'Gara PT, et al. Myocardial metabolic,hemodynamic and electrocardiographic significance of reversiblethallium-201 abnormalities in hypertrophic cardiomyopathy . Circulation1991 ;83 :1660-7 .
19 . Maron BJ, Epstein SE . Hypertrophic caidiomyopathy : a discussion ofnomenclature. Am J Cardiol 1979 ;43:1242-4 .
20 . Dilsizian V, Rocco TP, Freedman NM, Leon MB, Bonow RO . Enhanceddetection of ischemic but viable myocardium by the reinjection ofthallium after stress-redistribution imaging . N Engl J Med 1990,323 :141-6 .
21 . Hoffman EJ, Huang SC, Phelps ME . Quantitation in positron emissiontomography . 1 . Effect of object size . J Comput Assist Tomogr 1979;3 :299-308 .
22 . Cannon RO, Dilsizian V, O'Gara IT, ct al. Impact of operative relief ofoutflow obstruction on thallium perfusion abnormalities in hypertrophiccardiamyopathy . Circulation 1992 ;85 :1039-45 .
23 . Dilsizian V, Sineltzer WR, Dextras R, Simon TR, Bonow RO . Regionalthallium abnormalities in hypertrophic cardionryopathy : myocardial isch-cmia or disturbed cellular active cation uptake? (ibstr) . Circulation1990200 .
24 . Cannon RO Ill, Rosing DR, Maron BJ, et al . Myocardial ischemin inpatients with hypertrophic cardiomyopathy: contribution of inadequatevasodilator reserve and elevated left ventricular filling pressures, Circu-lation 1985 ;71*234-43 .
25. James TH. Marshall TK . De subitaneis mortibus . XII . Asymmetricalhypertrophy of the heart . Circulation 1975;51 :1149-66 .
26. Maron BJ, Wolfson JK, Epstein SE, Roberts WC . Intramural ("smallvessel") coronary artery disease in hypertrophic cardiomyopathy. J AmColl Cardiol 1986,6 :545-57 .
27 . Marcus ML, Doty DB, Hiratzka LF, Wright CB, Eastham CL . Decreasedcoronary reserve : a mechanism for angina pectoris in patients with aorticstenosis and normal coronary arteries . N Engl J Med 1982 :307 :1362-6.
28. Opherk D, Mall G, Zebe 11, et al . Reduction of coronary reserve : amechanism for angina pectoris in patients with arterial hypertension andnormal coronary arteries, Circulation 1984 ;69:1-7 .
29. Maron BJ, Lipson LC . Roberts WC, Savage DD, Epstein SE . "Malig-nant" hypertrophic cardiomyopathy: identification of a subgroup offamilies with unusually frequent premature death . Am J Cardiol 1978,41 :1133-40.
30. Thompson DS, Naqvi N, Juul SM, et al . Effects of propranolol onmyocardial oxygen consumption, substrate extraction, and hemodynam-ics in hypertrophic obstructive cardiomyopathy . Br Heart J 1980-.44 :488-98 .
31 . Rosing DR, Kent KM . Maron BJ, Epstein SE. Verapamil therapy : a newapproach to the pharmacologic treatment of hypertrophic cardiomyopa-thy . 11. Effects on exercise capacity and symptomatic status. Circulation1979,60.1208-13 .
32 . Bonow RO, Rosing DR, Bacharach SL, et al . Effect of verapamil on leftventricular systolic function and diastolic filling in patients with hyper-trophic cardiomyopathy . Circulation 1981 ;64 :787-%.
33 . Alvares RF. Shaver JA, Gamble WH, Goodwin JF . Isovolurnic relaxationperiod in hypertrophic cardiomyopathy . J Am Coll Cardiol 1984 ;3:71-81 .
34 . Bonow RO, Dilsizian V, Rosing DR, Maron BJ, Bachaiach SL, GreenMV. Verapamil-induced improvement in left ventricular diastolic fillingand increased exercise tolerance in patients with hypertrophic cardiomy-opathy : short- and long-term effects . Circulation 1985 ;72 :853-64 .