




Anatomy & Physiology of Cells Chapters 3 & 4 Anatomy & Physiology
LECTURE #4
1
HUMAN ANATOMY AND PHYSIOLOGY
• The Nervous System
• The Endocrine Glands
• The Hemopoietic System
• The Circulatory System
• The Respiratory Tract
• The Digestive Tract
• The Urinary Tract
• The Reproductory System
• The Locomotor System
• The Skin
E. MORAN - 2016 2
THE NERVOUS SYSTEM
• The Central Nervous System (CNS)
• The Peripheral Nervous System
• The Autonomous Nervous System
E. MORAN - 2016 3
E. MORAN - 2016 4
Components of the Brain:
Cerebrum & Cranial nerves
Cerebellum
Brain Stem
Medulla Oblongata
Meninges
THE CENTRAL NERVOUS SYSTEM

5
E. MORAN - 2016 6
Two hemispheres interconnected
Left part – Reasoning
Right part – Sensation, imagination
Frontal lobes – executive functions, personality, reasoning, abstract thought, planning, self-control, motor area, speech area.
Parietal lobes – Sensory areas, reading, language, attention, spatial cognition, arithmetic
Occipital lobes - Visual reception, visual-spatial processing
Temporal lobes - Auditive, forming and retrieving memories
THE HUMAN BRAIN
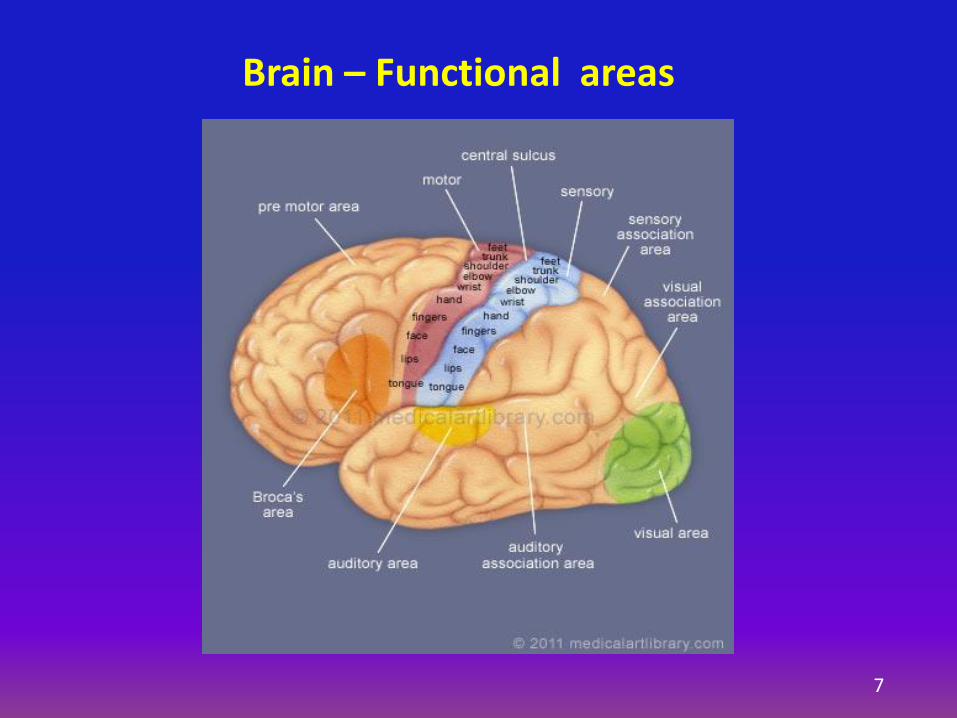
Brain – Functional areas
7
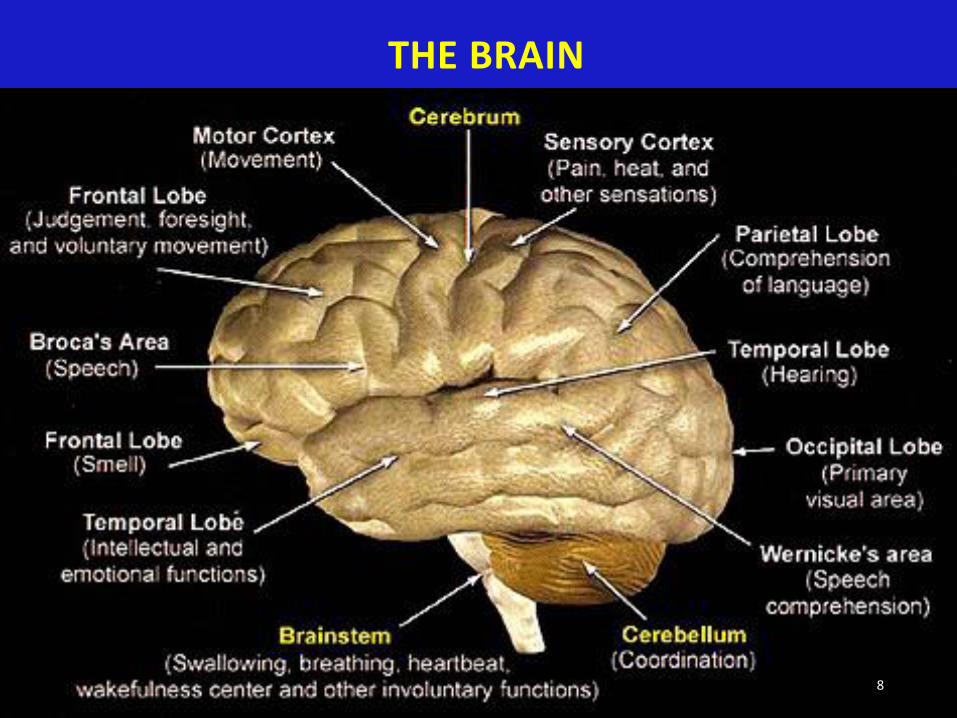
THE BRAIN
8

E. MORAN - 2016 9
Weight: About 3 lbs.
Convoluted cortex with gyri and sulci to expand surface
Grey matter – Nerve cells (neurons) and
White matter - The nerve fibers with myelin sheathing
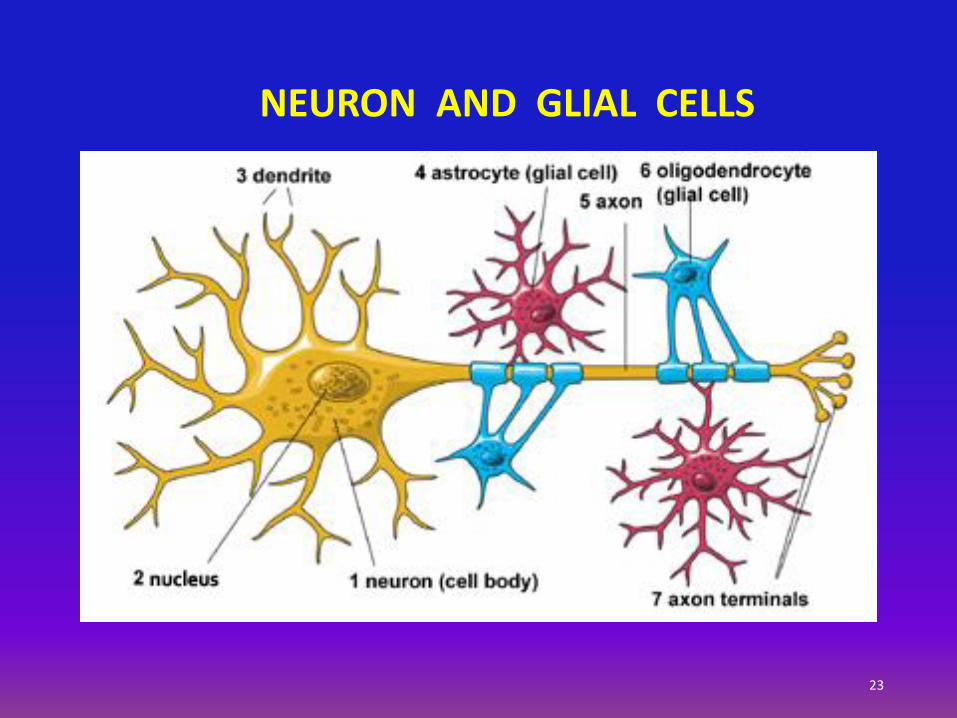
Neurons, glial cells, and blood vessels
86 billion neurons and 84 billion of non-neuronal cells in the adult human brain
Blood - Brain barrier and Blood - CSF barrier
THE HUMAN BRAIN - STRUCTURE

Cerebellar cortex structure
10

Brain cortex structure (monkey)
11
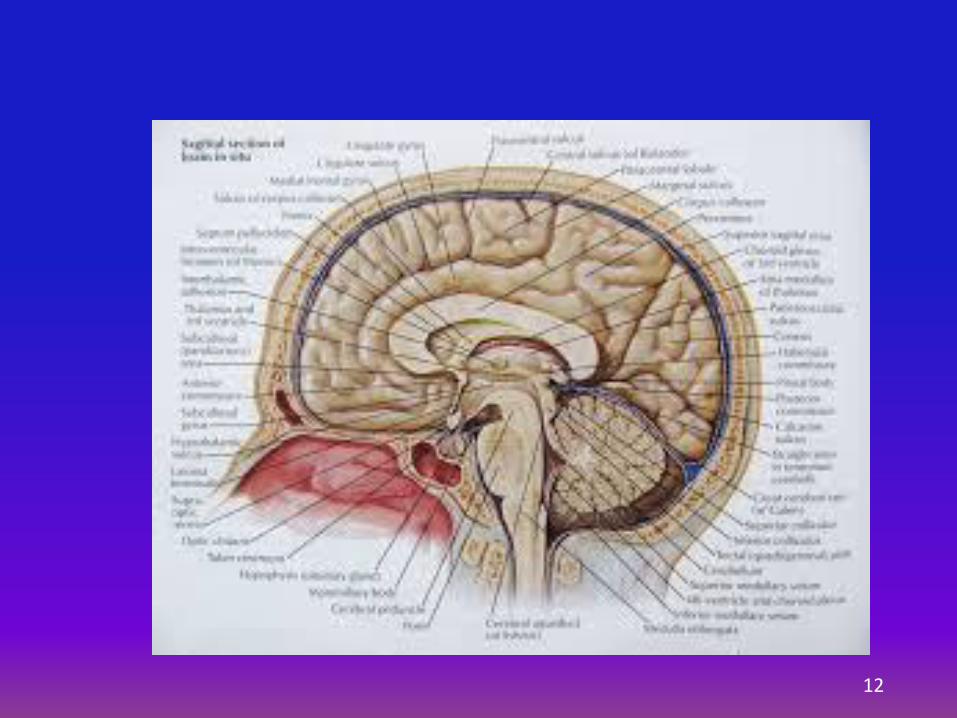
12

E. MORAN - 2016 13
Located at the base of the brain.
Connected to the thalamus in the brain.
Connected to the autonomic nervous system and to the pituitary gland.
Regulates body temperature, breathing, blood pressure, appetite, sleep, and emotional expression.
HYPOTHALAMUS
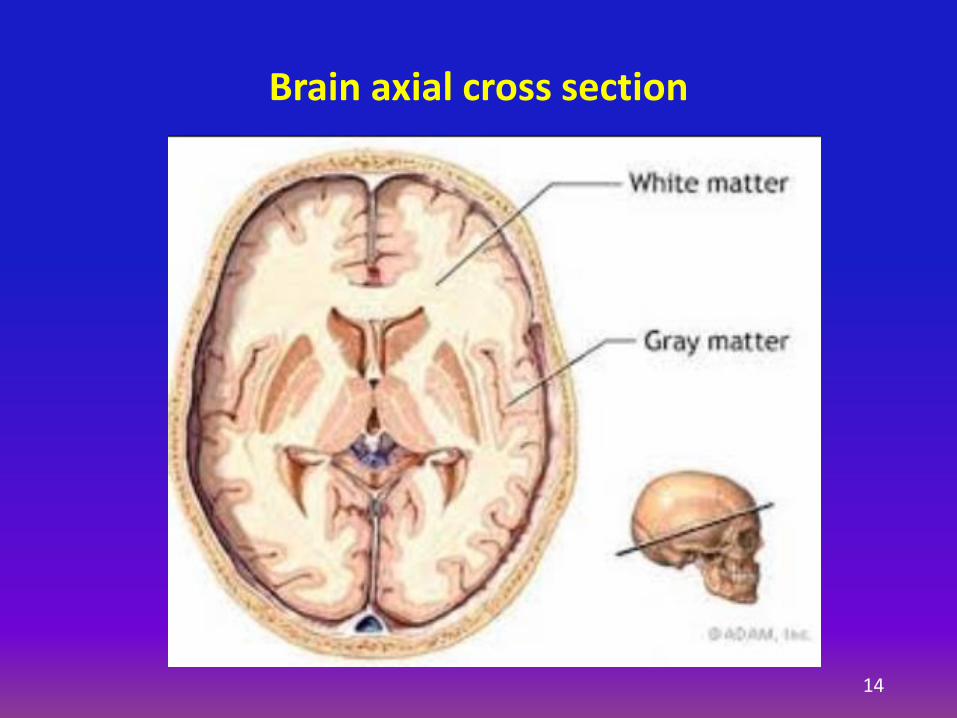
Brain axial cross section
14
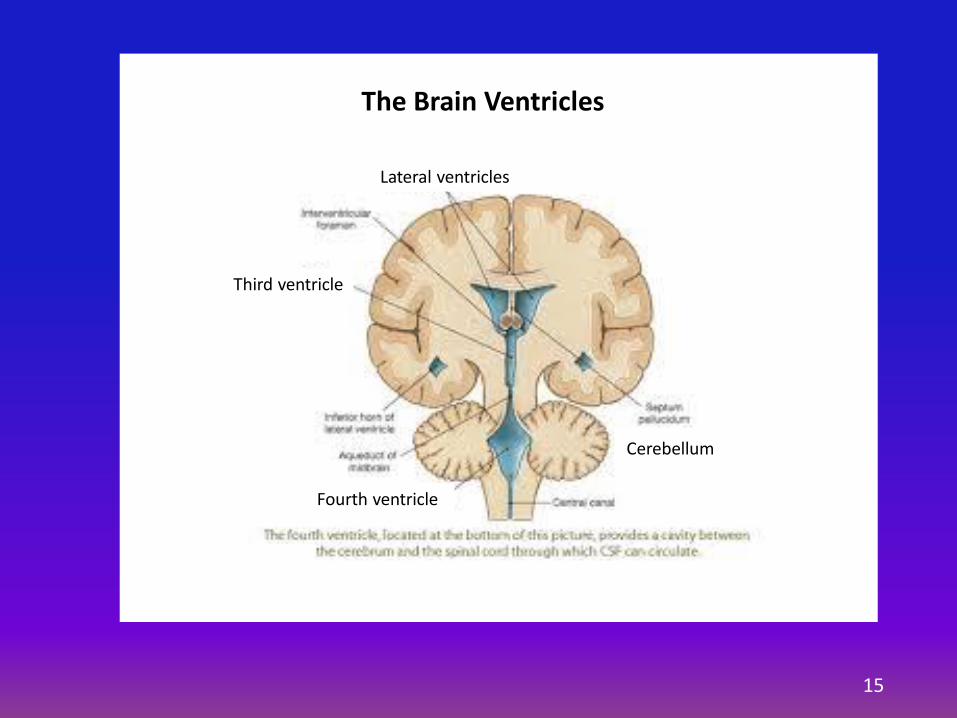
The Brain Ventricles
Lateral ventricles
Third ventricle
Fourth ventricle
Cerebellum
15
E. MORAN - 2016 18
The skull and spinal column
The meninges
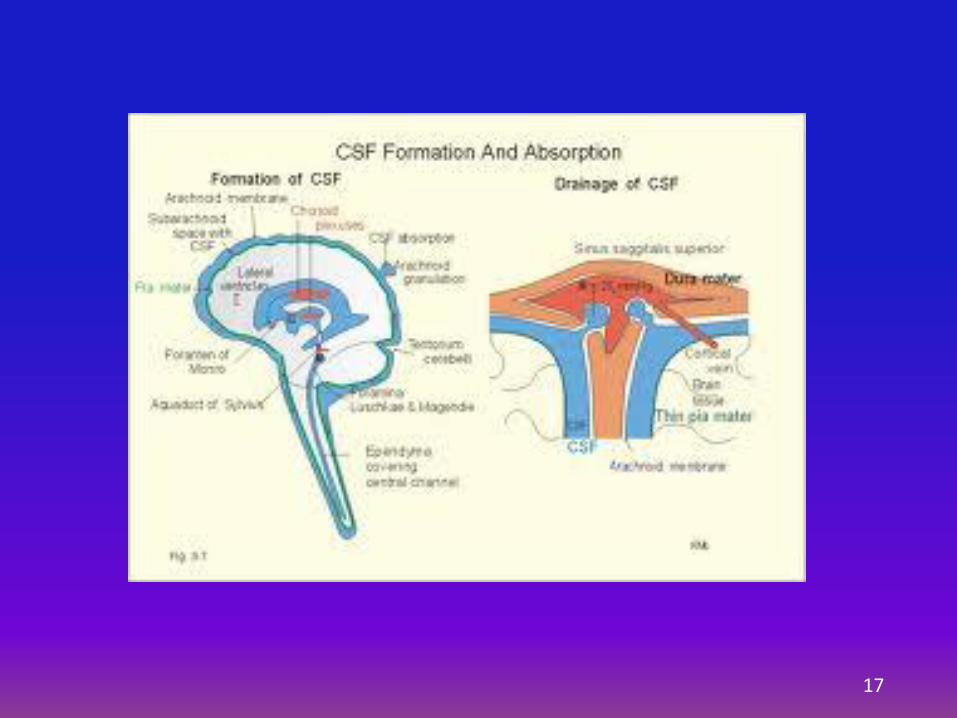
The cerebrospinal fluid
THE PROTECTIVE LAYERS OF THE BRAIN
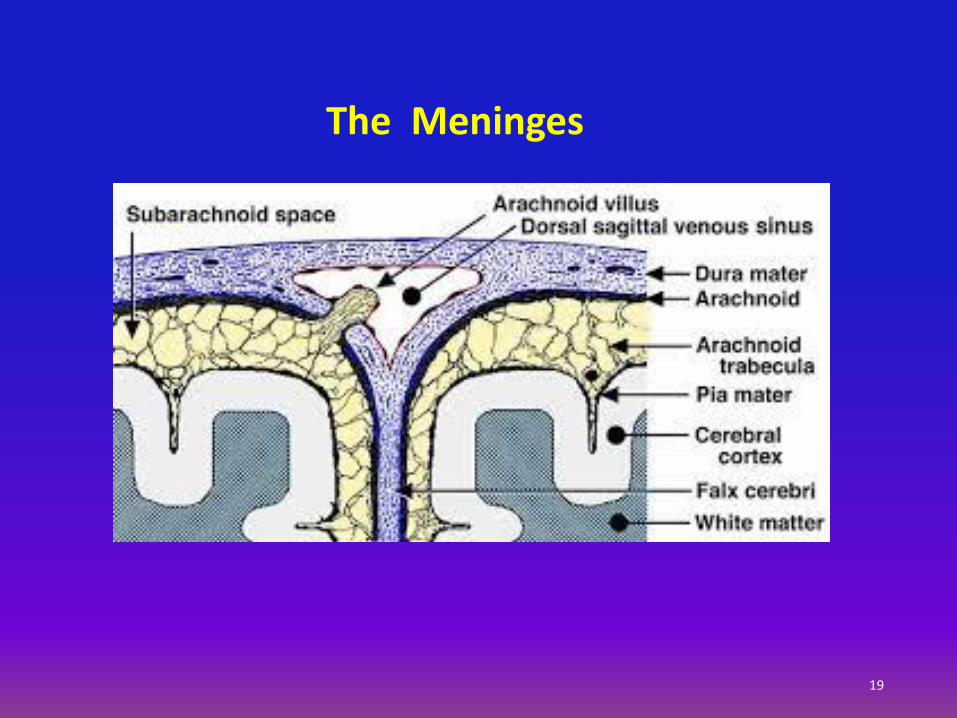
The Meninges
19
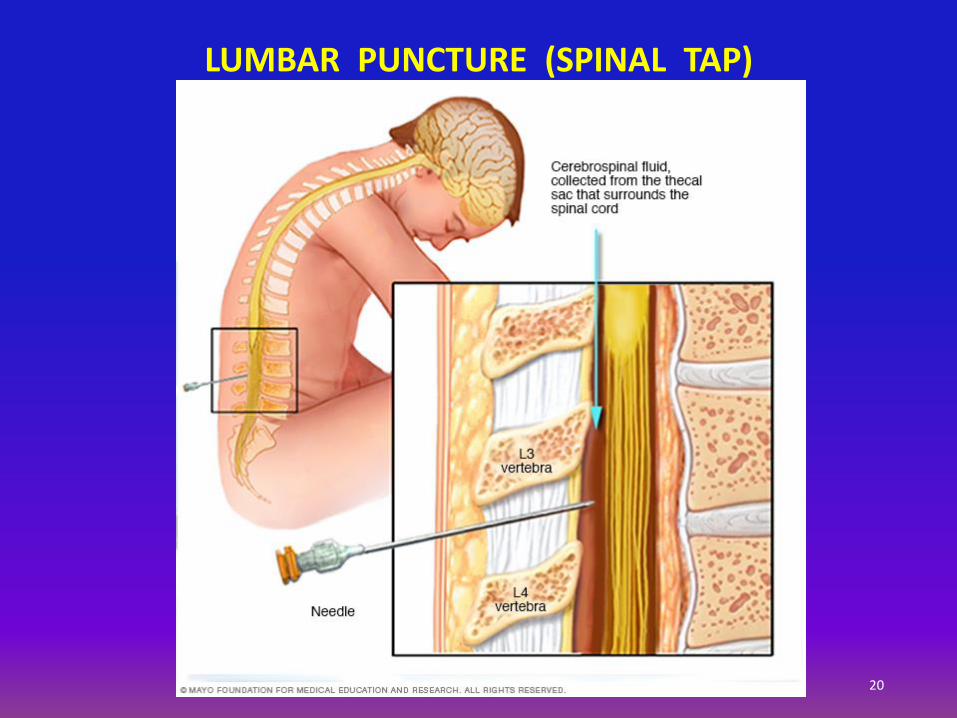
20
LUMBAR PUNCTURE (SPINAL TAP)

THE NERVES
21
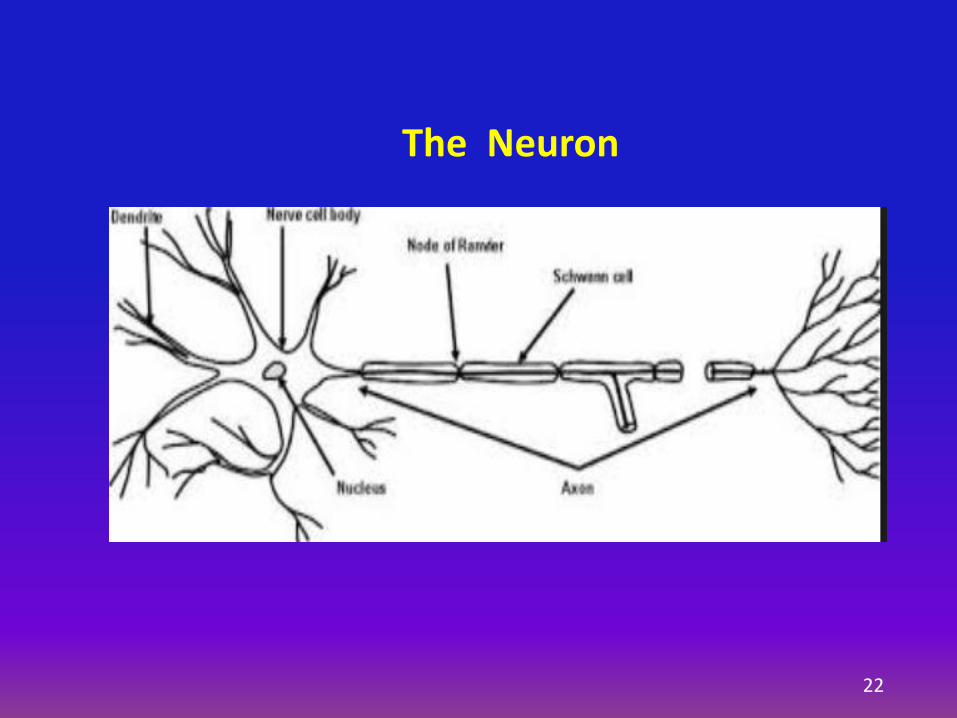
22
The Neuron
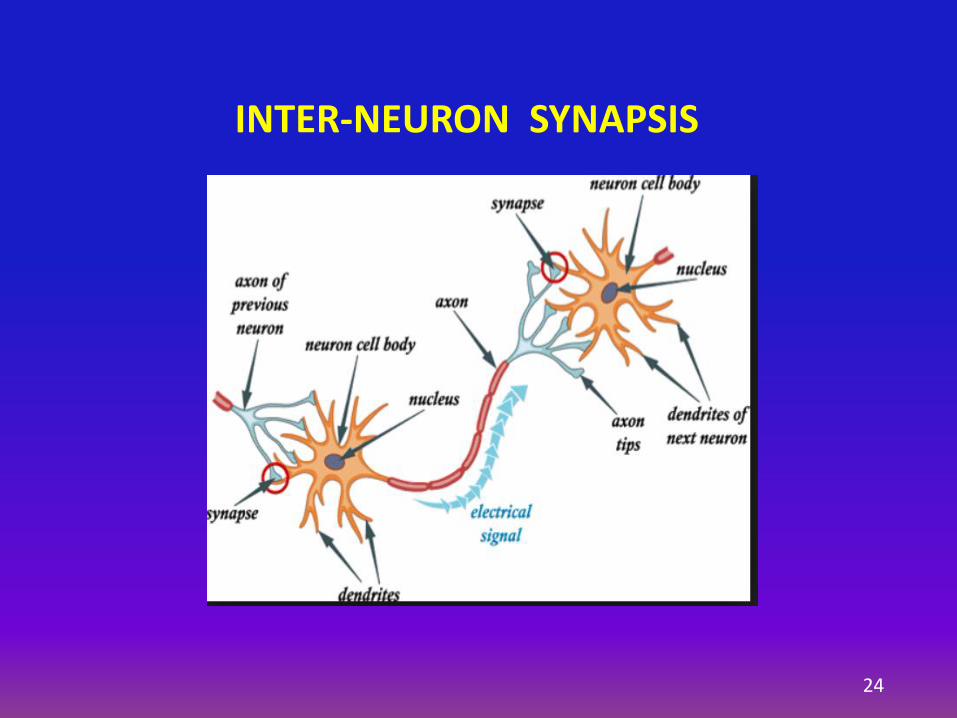
INTER-NEURON SYNAPSIS
24
25
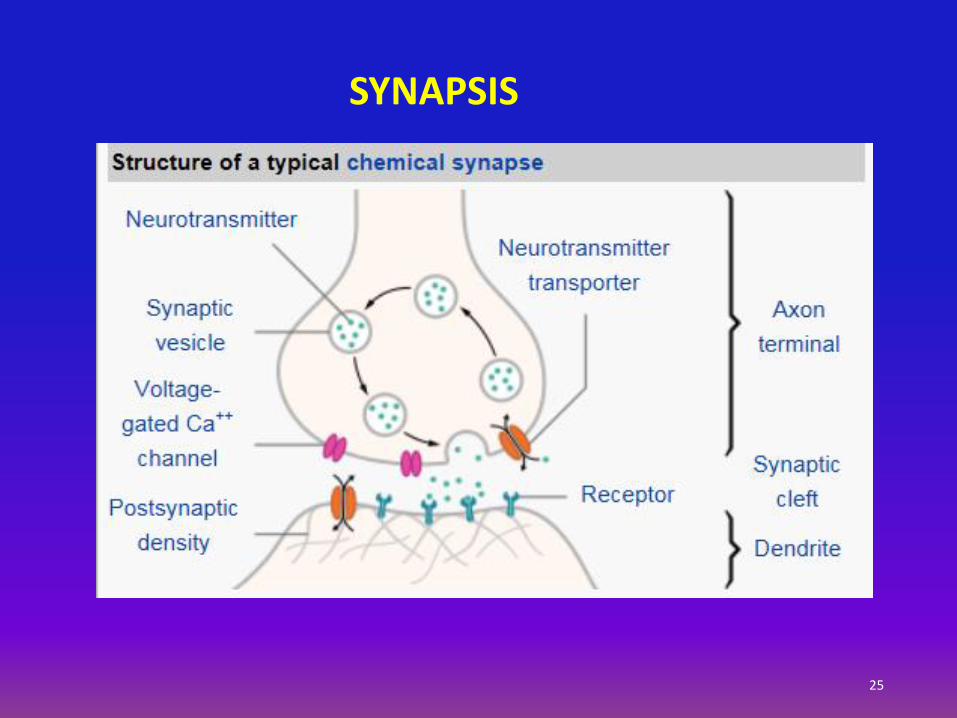
SYNAPSIS
E. MORAN - 2016 26
All cell membranes have an electric voltage difference btw. the interior and the exterior of the cell = membrane potential = -70 mV
Most cells have a constant membrane potential
Electrically active cells (Neurons, muscle cells) the voltage fluctuates = action potential = up-and-down cycles = few ms
Cell membrane consists of a lipid layer with embedded protein molecules channels through which ions can pass into the cell = “voltage-gated ion channels”
NEUROTRANSMISSION
E. MORAN - 2016 27
I. Olfactory – Smell
II. Optic – Vision
III. Oculo-motor - Eye movements
IV. Trochlear - Eye movement downward and in
V. Trigeminal - Facial sensation and motor (jaw)
VI. Abducens – Eye movements
VII. Facial – Mainly motor – facial expression
VIII. Acoustic and Vestibular – Hearing and Balance
IX. Glossopharyngeal – Oral sensation, taste, salivation
X. Vagus – Larynx, pharynx, esophagus, lungs, stomach, bowels
XI. Accessory – Shoulders
XII. Hypoglossal – Tongue movement, facial sensation
CRANIAL NERVES

VAGUS NERVE (X)
28

THE SPINAL CORD
29
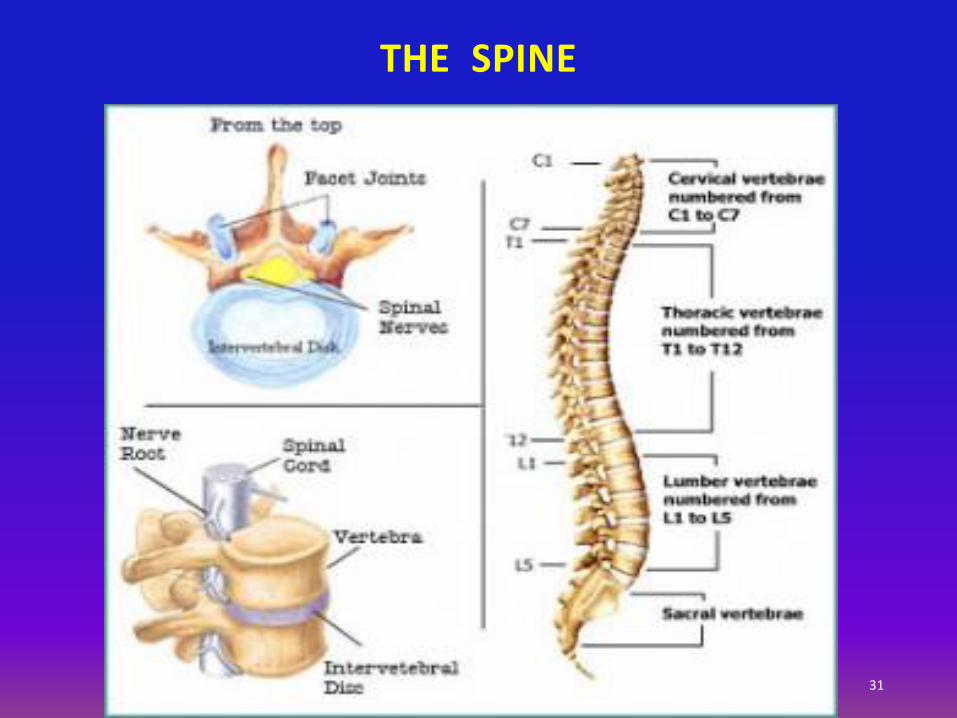
THE SPINE
31

OSTEOARTHRITIS OF THE FACET JOINTS (INTERARTICULAR VERTEBRAL JOINTS)
32
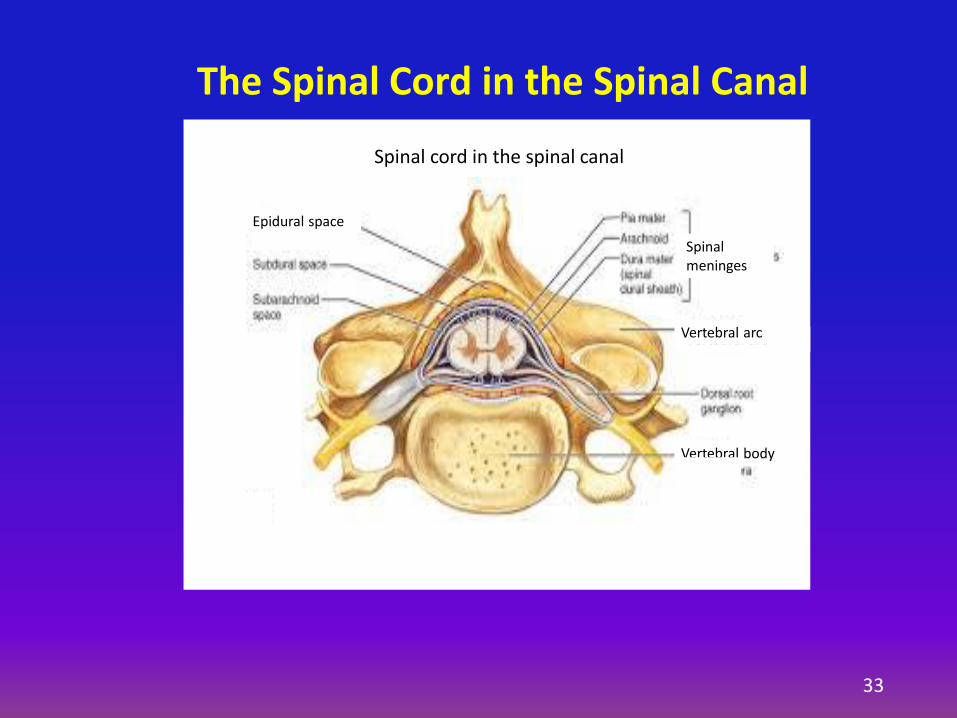
Epidural space
Vertebral body
Vertebral arc
Spinal meninges
Spinal cord in the spinal canal
Vertebral arc
The Spinal Cord in the Spinal Canal
33
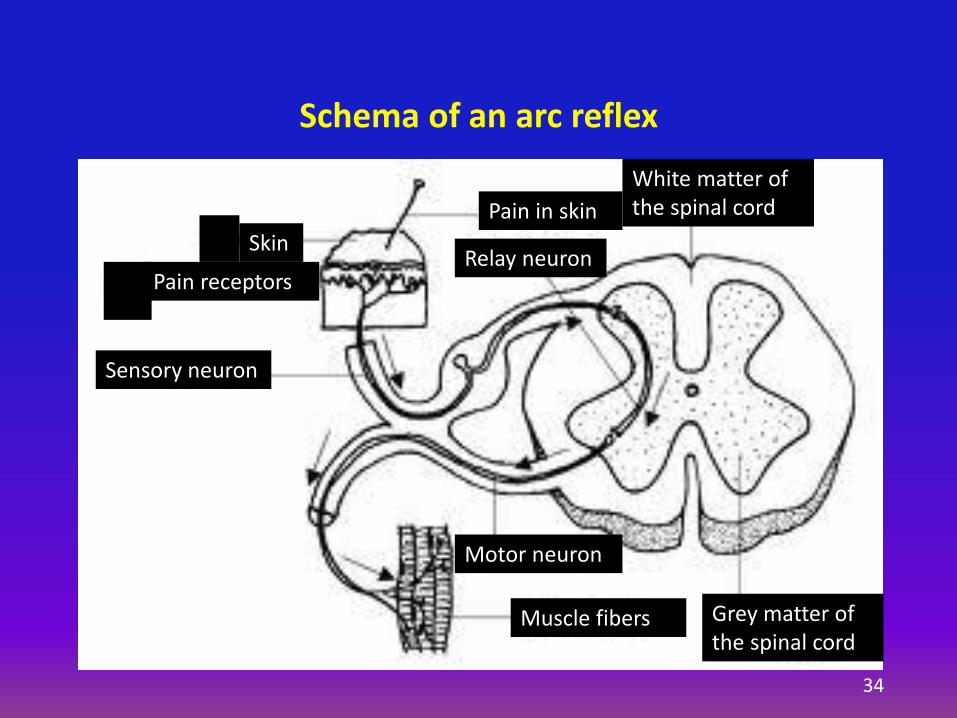
Schema of an arc reflex
Skin
Pain receptors
Sensory neuron
Pain in skin
Relay neuron
Motor neuron
Muscle fibers Grey matter of the spinal cord
White matter of the spinal cord
34
E. MORAN - 2016 35
Motor and sensory function
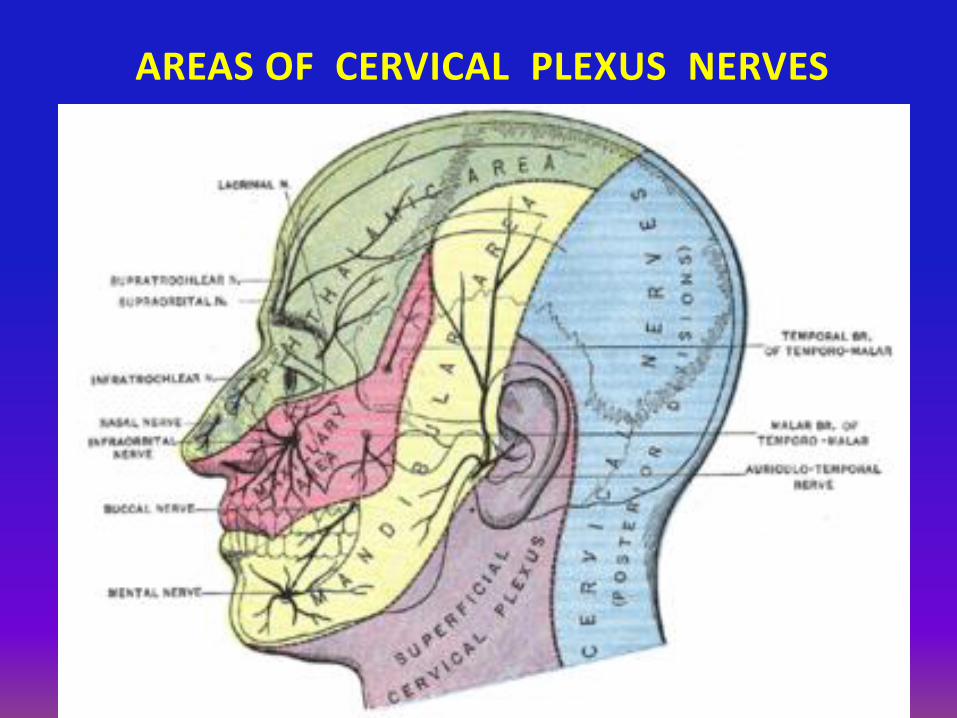
Cervical plexus (C1 – C4) – Head and neck
Brachial plexus (C5 – C8) – Arms, hands
Lumbar plexus (L1 – L4, L5) – Legs, feet
Sacral plexus (L5 – S4, S5) – Sciatic nerve, pelvis
Injuries: Nerve compression, inflammation
PERIPHERAL (SPINAL) NERVES

38
E. MORAN - 2016 39
Pain is an unpleasant feeling often caused by intense or damaging stimuli, such as stubbing a toe, burning a finger, putting alcohol on a cut.
Three classes of pain according to the pathophysiology of the cause:
Nociceptive pain
Inflammatory pain
Pathological pain
PAIN

E. MORAN - 2016 40
Nociceptive pain - stimulation of peripheral nerve fibers by:
thermal (heat or cold),
mechanical (crushing, tearing, shearing) and
chemical (iodine in a cut, chili powder in the eyes).
Inflammatory pain associated with tissue damage and cellular reaction
Pathological pain caused by:
Damage to the nervous system (neuropathic pain): spine arthritis
Abnormal function (dysfunctional pain), like in fibromyalgia, irritable bowel syndrome, tension type headache, menses
PAIN
AUTONOMIC NERVOUS SYSTEM (ANS)
• Sympathetic (adrenergic)
• Parasympathetic (cholinergic)
• Enteric
E. MORAN - 2016 41

Autonomic Nervous SystemBrain
Weak stimul. salivary
gl.
Dilates pupil
Inhibits stomach motility & secretion
No effect on tear glands
Acceler. heart
Contracts
Dilates bronchi
Inhibits intest. motility
Relaxes bladder
Stimulates ejaculation
Stimul. tear gl.Constricts pupil
Strong stimul. salivary gl.
Acceler. Heart &
Contracts arteries
Dilates bronchi
Inhibits heart heart
Dilates arteries
Stimulates stomach motility and secretion
Constricts bronchi
Stimulates intest. motility
Contracts bladder
Stimulates erection
Parasympathetic Sympathetic
Autonomic Nervous System
42
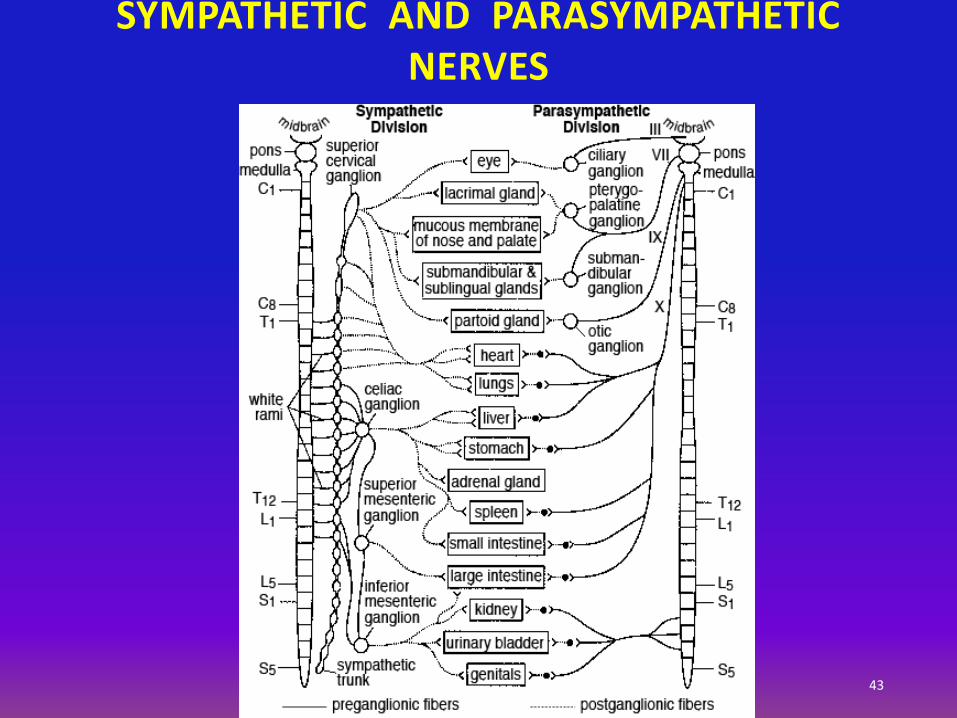
SYMPATHETIC AND PARASYMPATHETIC NERVES
43

E. MORAN - 2016 44
Ischemic events (stroke): Occlusion of an artery by a thrombus or an embolus Hemorrhagic stroke: due to HTN, trauma, low platelets, or coagulation defects Transient ischemic attack (TIA) Cerebral artery aneurysm, ruptured Infections: Encephalitis, meningitis Cancer: Gliomas of various types, slow-growing to rapidly-growing tumors Meningioma Degenerative diseases: Parkinson’s disease, Alzheimer’s disease, ALS, MS
MAJOR DISEASES OF THE BRAIN

E. MORAN - 2016 45
Progressive leukoencephalopathy
Subacute cerebellar degeneration
Encephalomyeilitis, often with unusual topographic distribution
Neuropathy, motor or sensory
Myasthenia syndrome
Myopathy
REMOTE EFFECTS OF CANCER ON THE NERVOUS SYSTEM
Acute - d/t closure of blood supply by a blood clot (thrombus) or by a circulating clot, tumor, gas, fat (embolus)
Chronic - d/t narrowing of arteries by:
• Arteriosclerosis = hardening of arteries
• Atheroma plaque
VASCULAR ISCHEMIC EVENTS (I)
E. MORAN - 2016 46
VASCULAR ISCHEMIC EVENTS (II)
Brain – Transient ischemic attack (TIA) or Cerebral vascular accident (CVA, Stroke)
Heart – Angina, or Heart attack (Myocardial infarct or MI)
Limbs – Claudication, Peripheral vascular insufficiency (PVI)
Lung – Pulmonary infarct
Kidney, Spleen - Infarcts
E. MORAN - 2016 47

E. MORAN - 2016 48
• Sudden or rapidly developing confusion and disorientation
• Inability to speak. Slurred speech.
• Weakness and numbness of an arm or a leg
• Sudden vision impairment
• Severe headache
• Other symptoms depending on the brain area affected
STROKE - SYMPTOMS
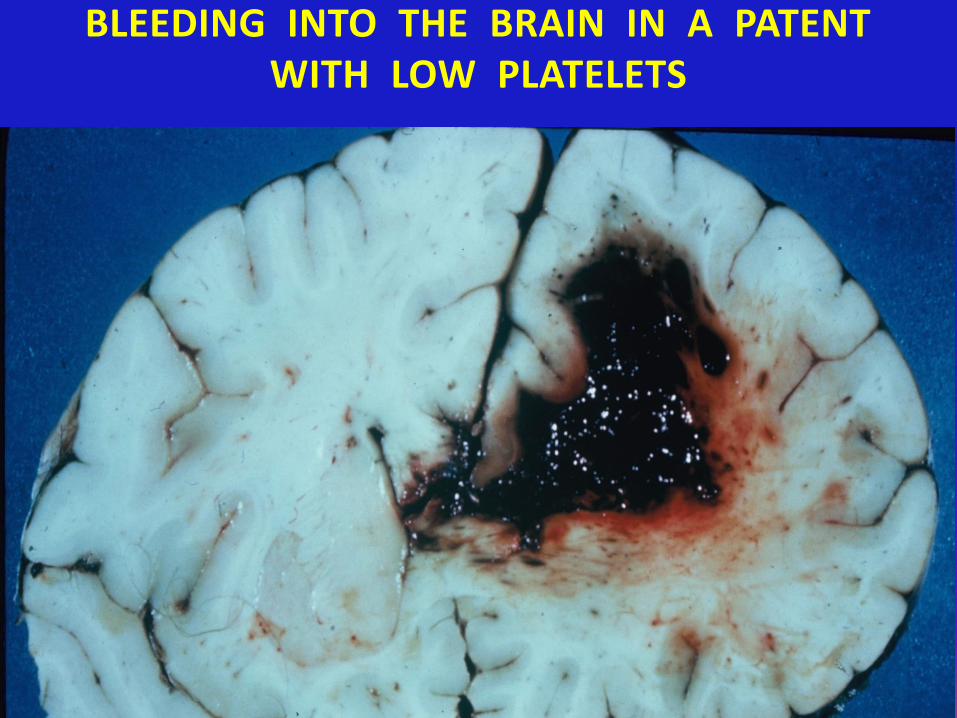
BLEEDING INTO THE BRAIN IN A PATENT WITH LOW PLATELETS
E. MORAN - 2015 49
E. MORAN - 2016 50
Correct diagnosis: Ischemic vs. hemorrhagic stroke
What is urgently needed:
History and physical examination
Carotid artery ultrasound: Narrowing? Thrombus? Electrocardiogram: Arrhythmia?
Echocardiogram: Clots in the heart chambers?
Brain CAT: Ischemic vs. bleeding event
Magnetic resonance angiogram (MRA)
STROKE - DIAGNOSIS
E. MORAN - 2016 51
Stabilize the patient. Time is of the essence
If ischemic stroke:
• Antifibrinolytic medications (tPA)
• Anticoagulant medications (coumadin)
• Antiplatelet medications (aspirin, clopidogrel)
• Oxygen
• BP ?
• Blood sugar ?
STROKE TREATMENT
E. MORAN - 2016 52
Control of arrhythmia (atrial fibrillation, atrial flutter)
Anticoagulants
Antiplatelets
Physiotherapy to start 2 weeks after the stroke. Maximize functionality
Speech therapy ASAP
AFTER THE ACUTE STROKE TREATMENT
E. MORAN - 2016 53
Reduction of blood flow to the brain, transient
Symptoms like in a stroke, but spontaneous recovery
Causes: Arrhythmia, blood clot, drop in BP
Diagnosis: Like for Stroke
TRANSIENT ISCHEMIC ATTACK (TIA)
E. MORAN - 2016 54
A life-threatening disease.
An acute inflammation of the brain coverings (meninges) caused by bacteria, viruses, fungi
Symptoms: fever, headache, confusion, vomiting, neck- stiffening, photophobia
Diagnosis: Spinal tap CSF culture
Treatment: Antibiotics, antivirals
Prognosis: Curable if diagnosed early
MENINGITIS
E. MORAN - 2016 55
Primary or metastatic from lung, breast, and cancer of other organs
Lymphoma in AIDS
Primary: Oligodendroglioma – slow growth
Astrocytoma – low grade
Glioblastoma multiforme – high grade (fast growing)
Meningioma: Usually benign
BRAIN TUMORS
Primary cancer of the brain:
• Oligodendroglioma
• Astrocytomas
• Glioblastoma multiforme
Benign tumors of the meninges: Meningioma
Metastatic tumors of the brain:
Lung, breast, melanoma, lymphoma, sarcomas
CANCER OF THE BRAIN
E. MORAN - 2016 56
E. MORAN - 2016 57
General: Headaches
Mental changes
Explosive vomiting
Focally: Deficiencies depending on the brain area
affected
One mm tumor causes ~2.0 cm area of edema
BRAIN CANCER - SYMPTOMS
Diagnosis: CT scan, MRI
Primary tumors: Surgery – difficult to distinguish btw. the tumor and the normal brain tissue
Optical coherence tomography may help
Radiation/Chemotherapy
Secondary tumors: Radiation
Chemotherapy
Biologicals
BRAIN CANCER – DIAGNOSIS & TREATMENT
E. MORAN - 2016 58

Most frequent sites relate to the venous blood return:
• Lungs
• Liver
• Bones: from breast, prostate, and lung cancer
Solitary mets. may be removed surgically
CANCER METASTASES
E. MORAN - 2016 59
E. MORAN -2016 60
Death of dopamine - generating cells in the midbrain a degenerative disease of the motor system
Symptoms: Progressive shaking of hands, stooped posture, gait impairment, rigidity. Later, depression and dementia
Cause: Idiopathic or possibly caused by insecticides, pesticides, Agent Orange
Treatment: Dopamine agonists in early disease. Gene? stem cell?
PARKINSON’S DISEASE
61
PARKINSON’S DISEASE
E. MORAN - 2016 62
Two hemispheres interconnected
Left part – Reasoning
Right part – Sensation, imagination
Frontal lobes – executive functions, personality, reasoning, abstract thought, planning, self-control, motor area, speech area.
Parietal lobes – Sensory areas, reading, language, attention, spatial cognition, arithmetic
Occipital lobes - Visual reception, visual-spatial processing
Temporal lobes - Auditive, forming and retrieving memories
THE HUMAN BRAIN
E. MORAN - 2016 63
A chronic degenerative, progressive disorder that attacks the brain's neurons, resulting in:
• Loss of memory,
• Thinking and language skills, and
• Behavioral changes
The neurons, that produce the brain neurotransmitter, acetylcholine, break connections with other nerve cells and ultimately die
Short-term memory fails when AD first destroys nerve cells in the hippocampus
Language skills and judgment decline when neurons die in the cerebral cortex of the frontal lobes
ALZHEIMER DISEASE
E. MORAN - 2016 64
Later: Disorientation (getting lost)
Mood swings
Loss of motivation (loss of self-care)
Behavioral issues
Withdrawal
Death caused by unrelated diseases
Course: 3-9 years
Diagnosis: Cognitive testing. Normal aging (?)
Normal medical imaging and blood tests
Brain biopsy = definitive diagnosis
ALZHEIMER’S DISEASE (cont.)
E. MORAN - 2016 65
Treatment: No medications or supplements are effective
Supporting care. Physical exercises are beneficial
Preventative: Mental and physical activity
Major pressures: Physical, psychological, social, economical
2015 – 48 Mil. people worldwide
Usually starts at > 65 y.o. 6% of people older than 65 y.o.
ALZHEIMER’S DISEASE
E. MORAN - 2016 66
Death of motor neurons
Cause: In 90-95% of cases cause is unknown
In 5-10% of cases – inheritance. Autosomal dominant genes.
Incidence around 60 years of age
Symptoms: Stiff muscles, twitching Muscle weakness
and atrophy Difficulty speaking, swallowing, breathing
No cognitive impairment
Progressive illness. No treatment available. Course 3-4 yrs.
AMYOTROPHIC LATERAL SCLEROSIS (ALS) (LOU GEHRIG DISEASE)
67
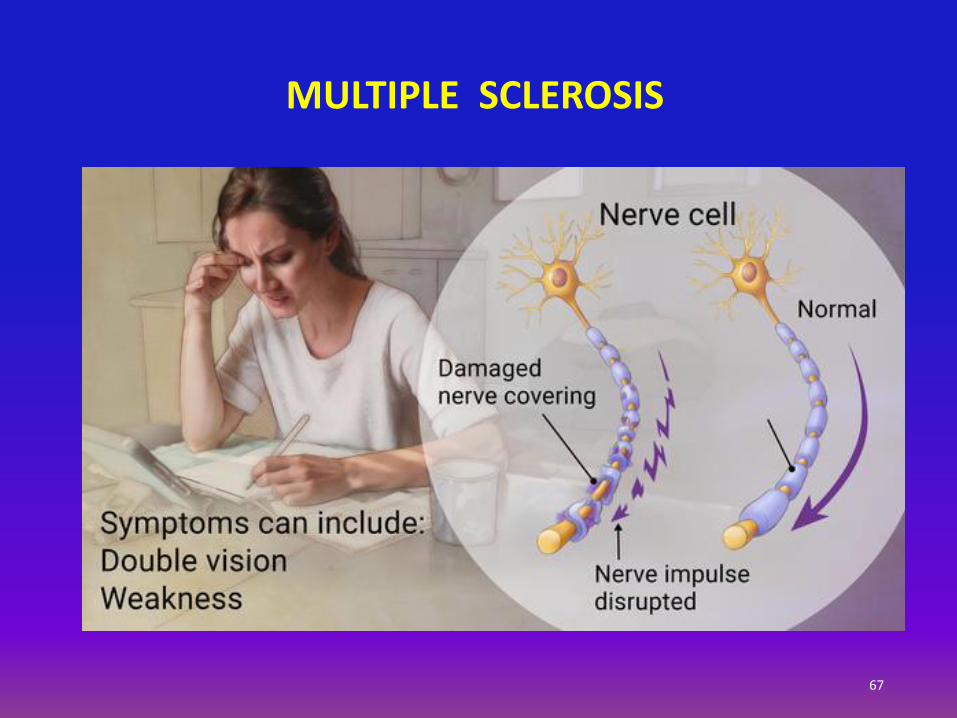
MULTIPLE SCLEROSIS
E. MORAN - 2016 68
A chronic autoimmune disorder in which the immune system attacks the myelin sheath of the nerves
Genetics, the environment, even viruses may play a role
Incidence: 20-40 y.o.
Phases of active disease and latency
Relapsing-Remitting Multiple Sclerosis (RRMS) – 85% of cases
MULTIPLE SCLEROSIS (MS)
E. MORAN - 2016 69
Blurred or double vision
Thinking problems
Clumsiness or a lack of coordination
Loss of balance
Numbness
Tingling
Weakness in an arm or leg
MULTIPLE SCLEROSIS EARLY SYMPTOMS
E. MORAN - 2016 70
Trouble walking
Feeling tired
Muscle weakness and spasms
Blurred or double vision
Numbness and tingling
Sexual problems (vaginal dryness and ED)
Poor bladder or bowel control
Pain
Depression
Problems focusing or remembering
Emotional and cognitive changes
MULTIPLE SCLEROSIS LATER STAGE SYMPTOMS
E. MORAN - 2016 71
Diagnosis: Clinical examination
Nerve conduction
Electroencephalogram (EEG)
Electromyogram (EMG)
MRI
Treatment: Steroids, ACTH, interferon, other meds.
MULTIPLE SCLEROSIS

INTERMISSION
72

73
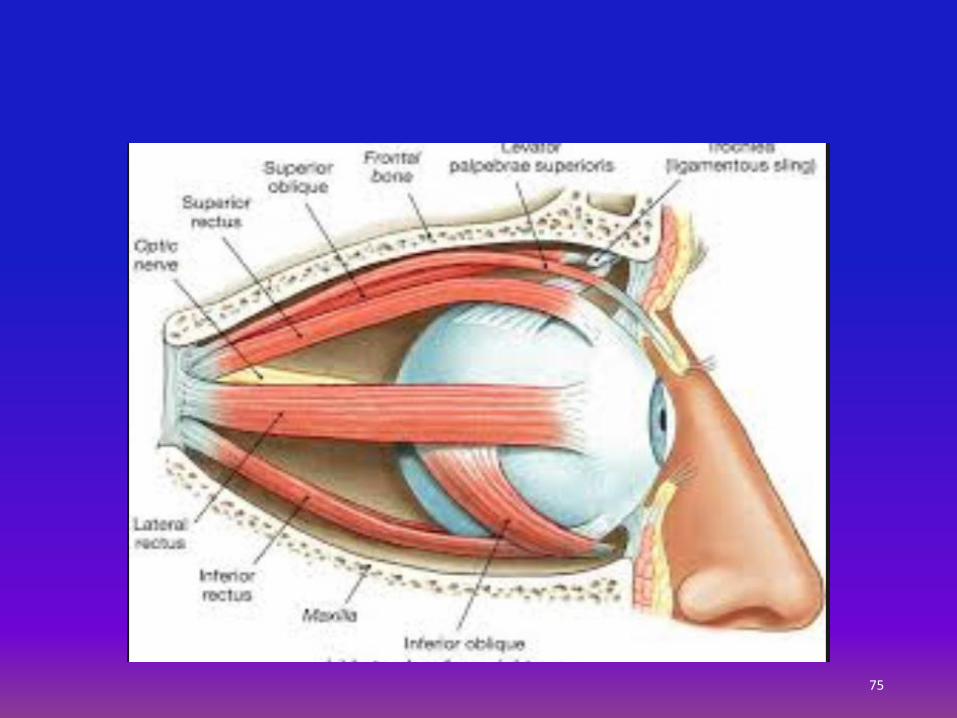
THE EYE
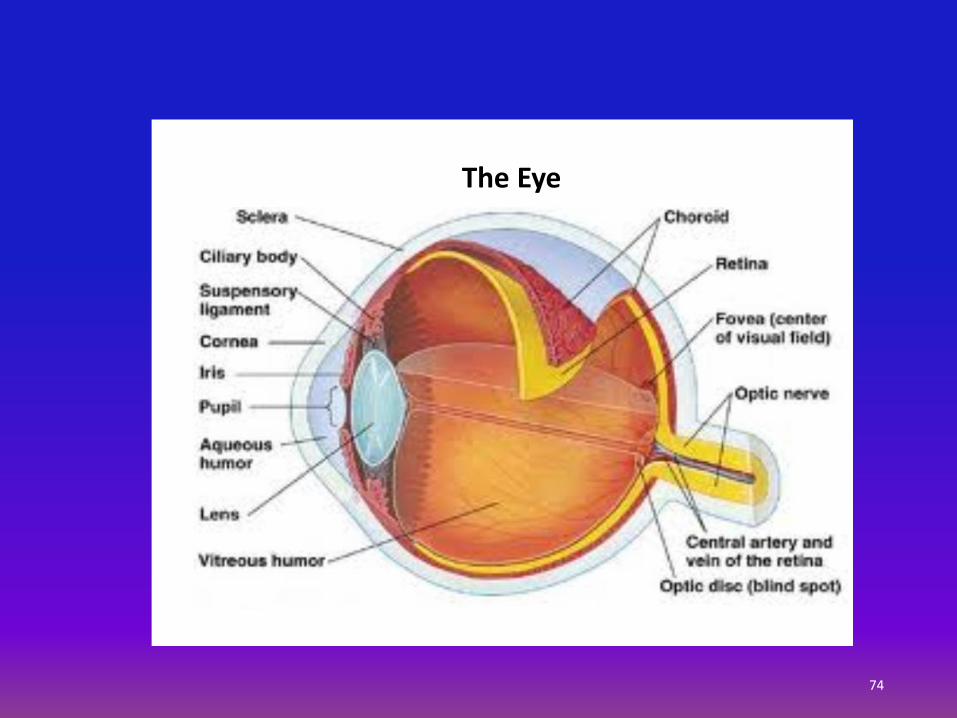
The Eye
74
75

E. MORAN - 2016 76
Cataract – lens opacification
Glaucoma – Increased intraocular pressure. Open-angle and closed-angle glaucoma
Tunnel vision
Diabetic retinopathy
Macular degeneration – “dry” and “wet”
of central vision
DISEASES OF THE EYE

E. MORAN - 2016 77
• Over age 40
• African-American, Irish, Russian, Japanese, Hispanic, Inuit, or Scandinavian descent
• Family history of glaucoma
• Diabetes
• Steroid medications, such as prednisone
• History of trauma to the eyes
GLAUCOMA RISK FACTORS
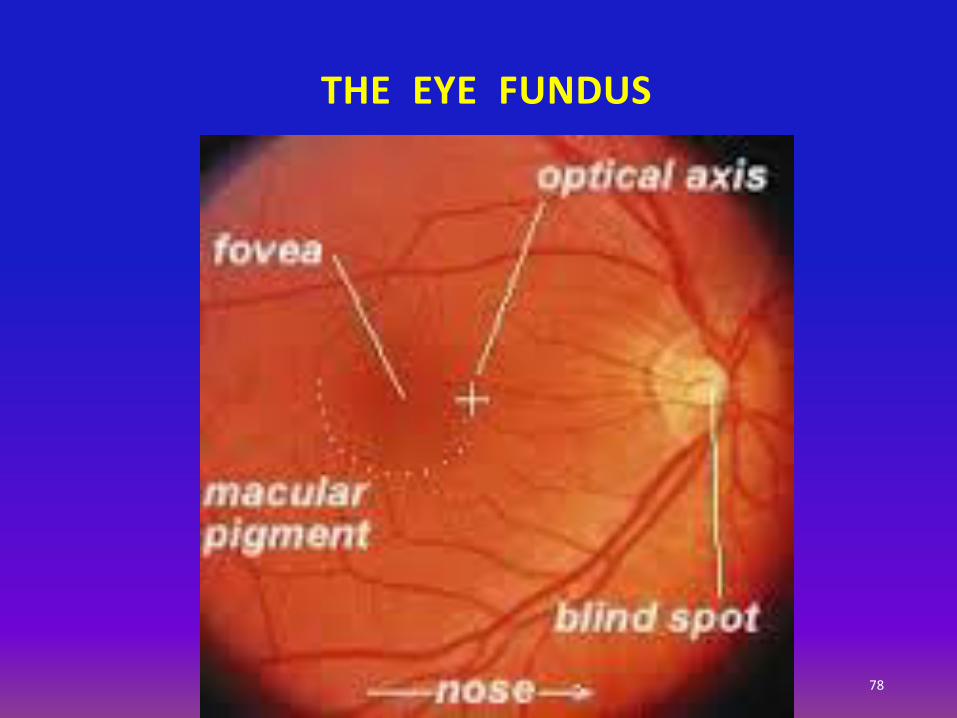
THE EYE FUNDUS
78
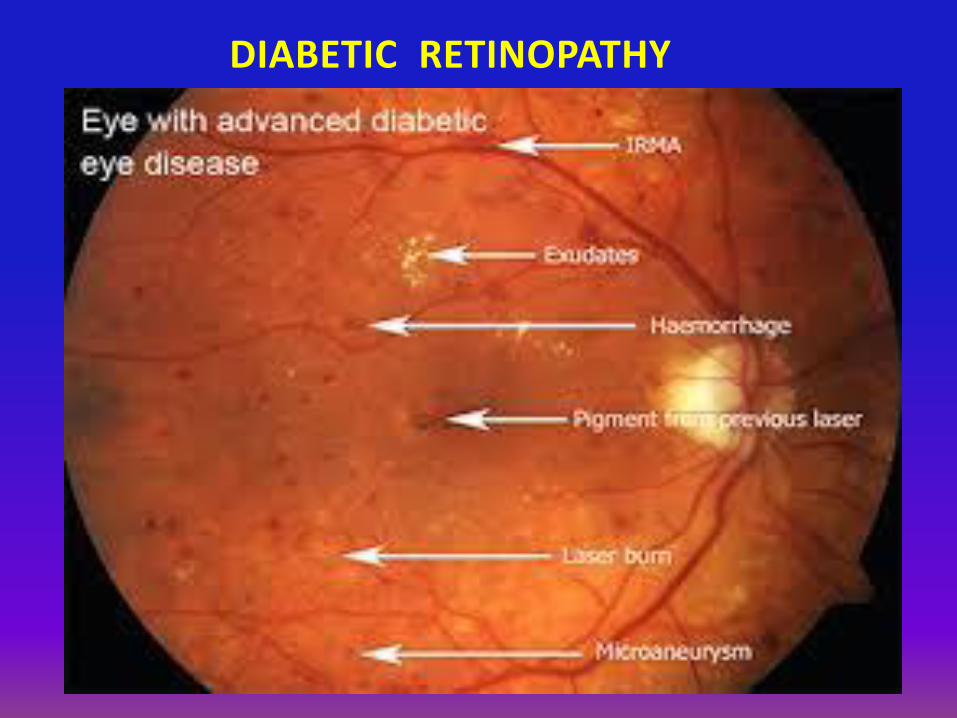
DIABETIC RETINOPATHY
79
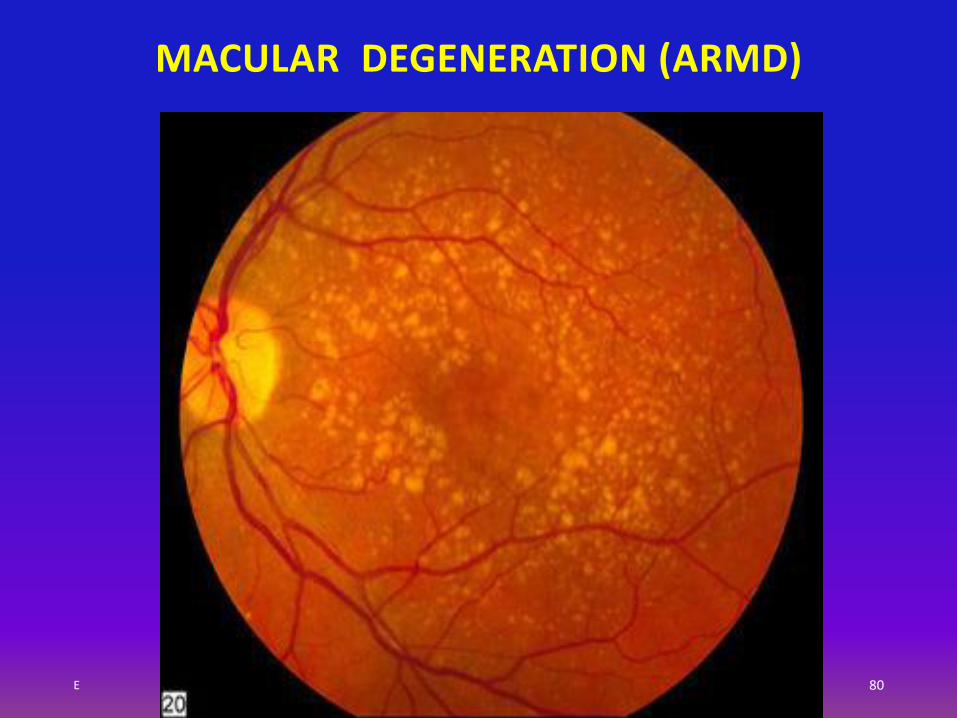
MACULAR DEGENERATION (ARMD)
E 80
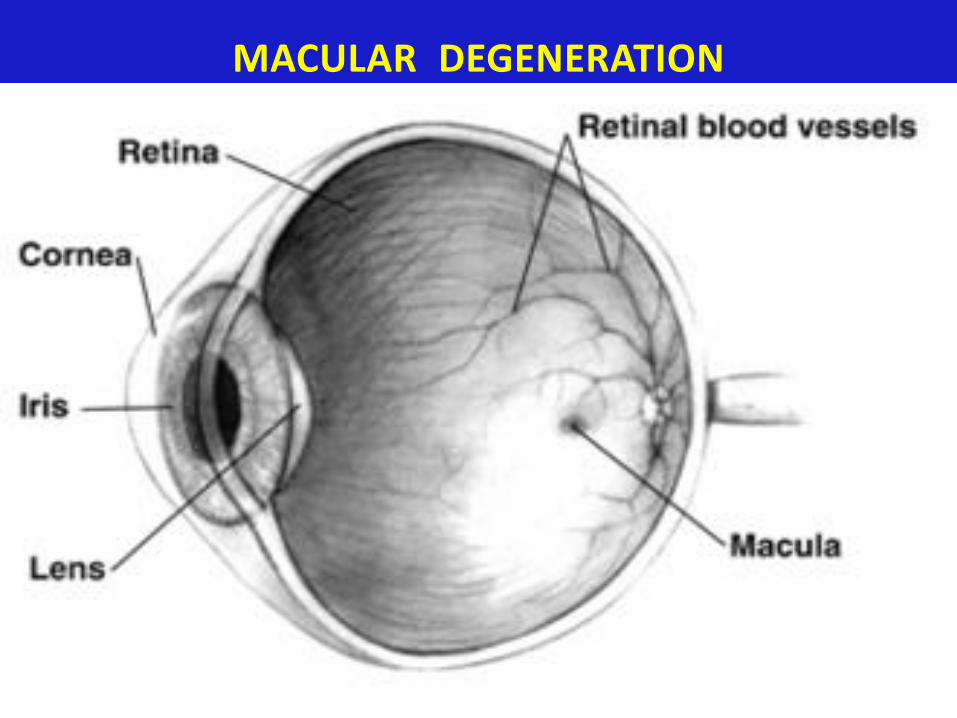
MACULAR DEGENERATION
81
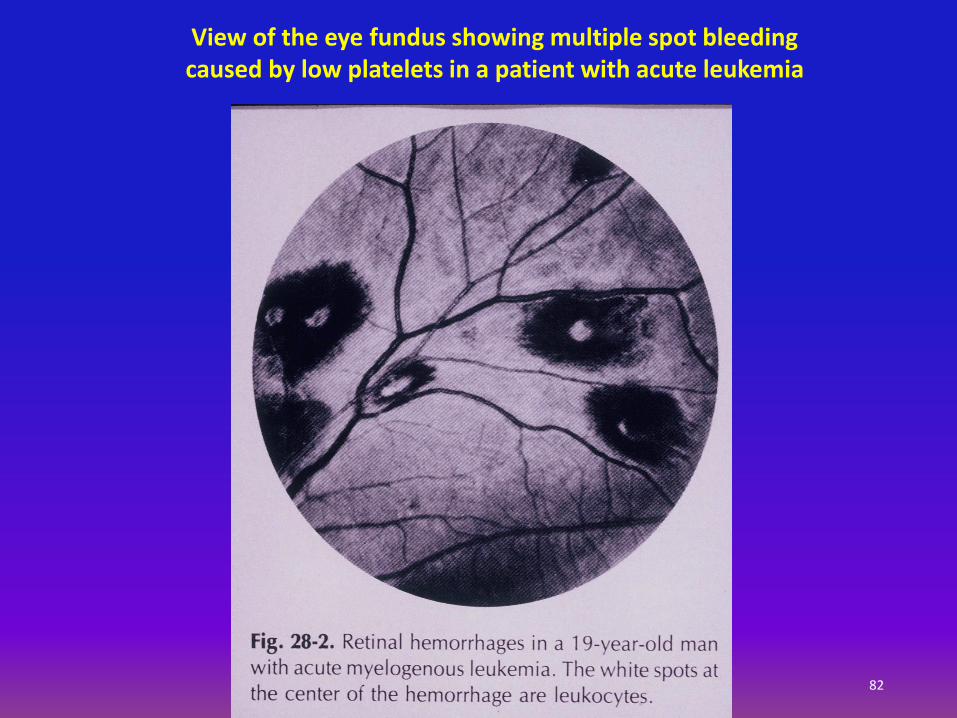
82
View of the eye fundus showing multiple spot bleeding caused by low platelets in a patient with acute leukemia

84
THE EAR
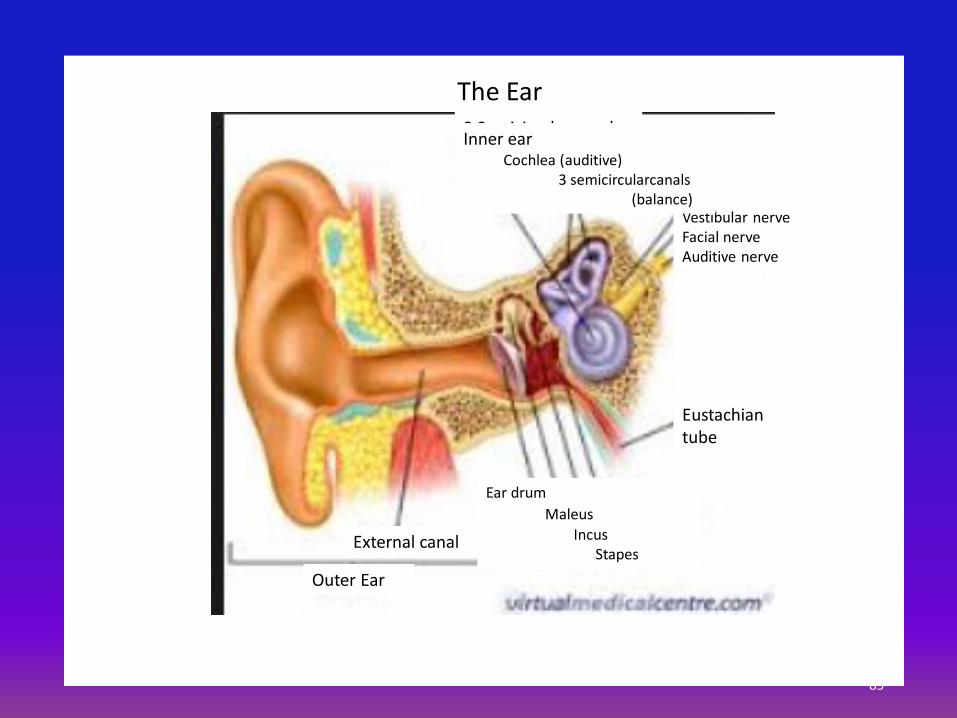
Outer Ear
External canal
Ear drum
Maleus
IncusStapes
Eustachian tube
Vestibular nerveFacial nerveAuditive nerve
3 Semicircular canalsInner ear
Cochlea (auditive)3 semicircularcanals
(balance)
The Ear
85

86
The Ear
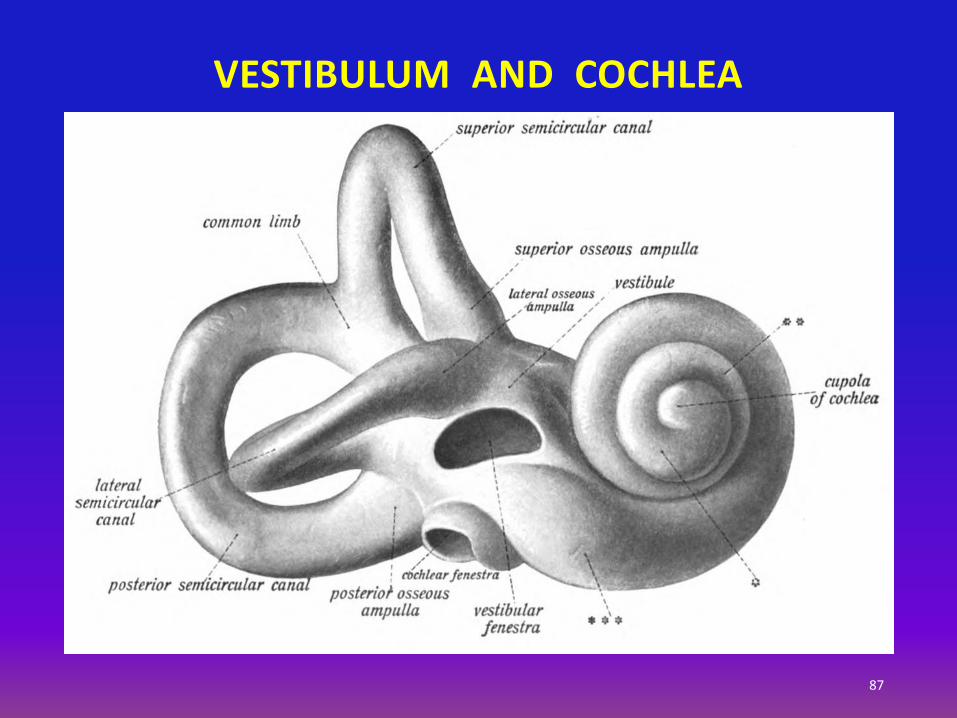
VESTIBULUM AND COCHLEA
87

Audiogram
88
HUMAN ANATOMY AND PHYSIOLOGY
• The Nervous System
• The Endocrine Glands
• The Hemopoietic System
• The Circulatory System
• The Respiratory Tract
• The Digestive Tract
• The Urinary Tract
• The Reproductory System
• The Locomotor System
E. MORAN - 2015 89

(Glands with Internal Secretion)
THE ENDOCRINE GLANDS
90

• High blood sugar
• Brain
• Insulin
HOMEOSTASIS FEEDBACK MECHANISMS
Example Phases
• Sensor mechanism senses disruption in homeostasis
• Control center
• Effector mechanism to restore homeostasis
E. MORAN - 2015 91
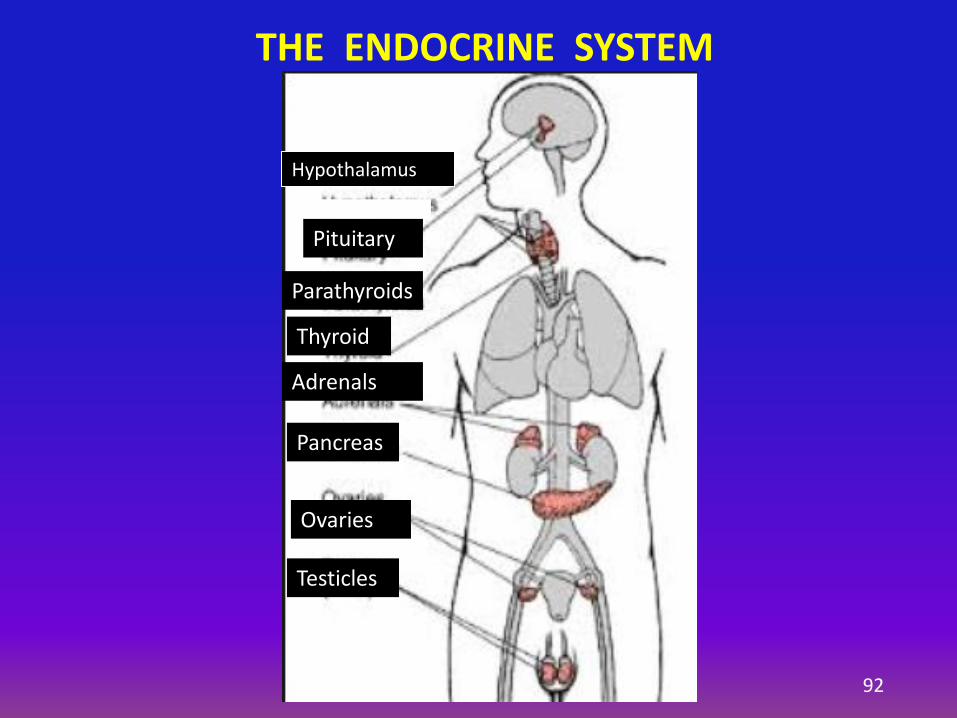
THE ENDOCRINE SYSTEM
Hypothalamus
Pituitary
Parathyroids
Thyroid
Adrenals
Pancreas
Ovaries
Testicles
92

The Nervous vs. the Endocrine Systems
93
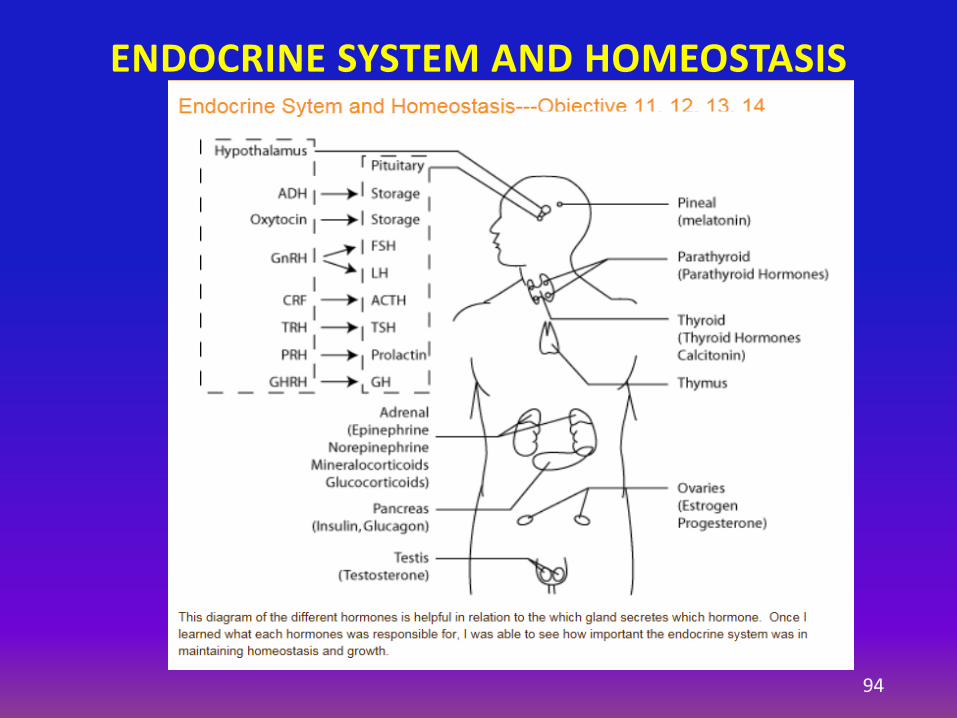
ENDOCRINE SYSTEM AND HOMEOSTASIS
94
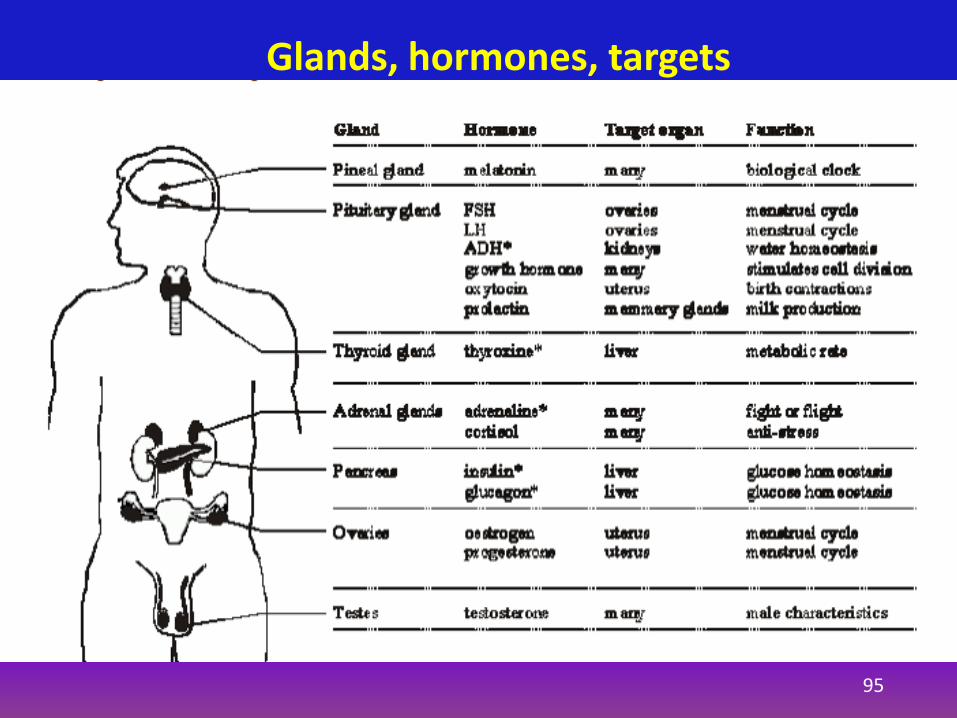
Glands, hormones, targets
95
1. Gland’s poor response to feedback
2. Insufficient or increased secretion
3. Destructive process: Tumor or inflammation
CAUSES OF ENDOCRINE DISORDERS
E. MORAN - 2015 96

THE PITUITARY
E. MORAN - 2015
97

Hypothalamus, pituitary, and thyroid
98

99
The thyroid gland
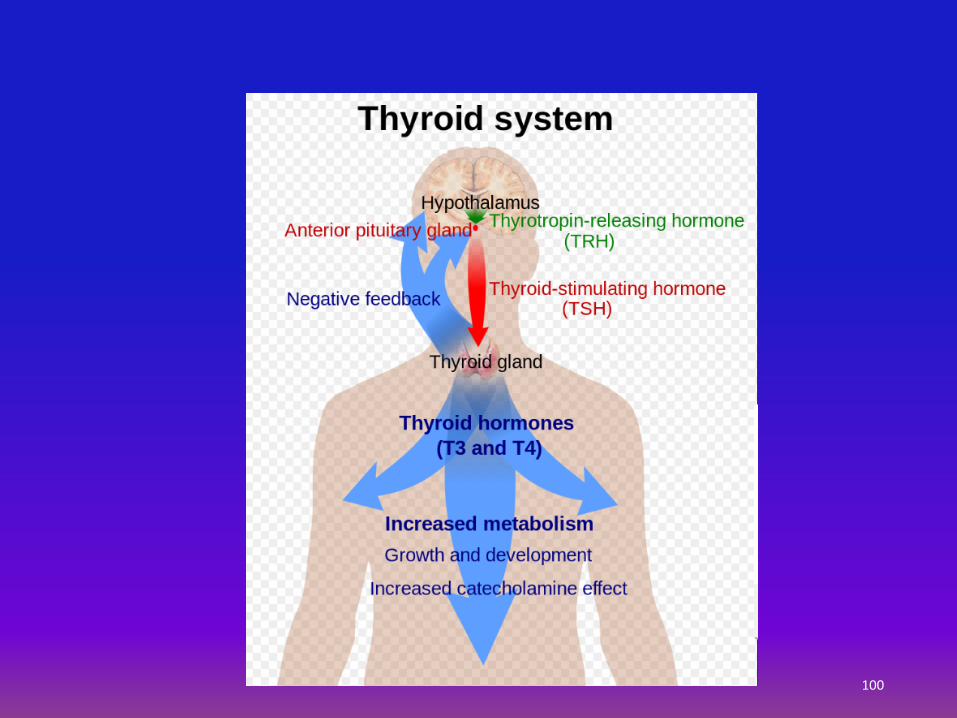
100

E. MORAN - 2015 101
Functions: Heart rate
Blood pressure
Body temperature
Metabolism
THYROID GLAND
• F > M
• Aging
• Autoimmune diseases
• Hashimoto thyroiditis
• Hypothalamus-Pituitary dysfunction
• Thyroid Surgery
• Graves’ disease
• Toxic nodular adenoma
• Toxic multinodular goiter
• Postpartum thyroiditis (PPT)
• Ingestion of Amiodarone (antiarrhythmic drug)
• Ingestion of algae (kelp) (contain iodine)
ABNORMAL THYROID FUNCTION - CAUSES
Hyperthyroid Hypothyroid
E. MORAN - 2015 102
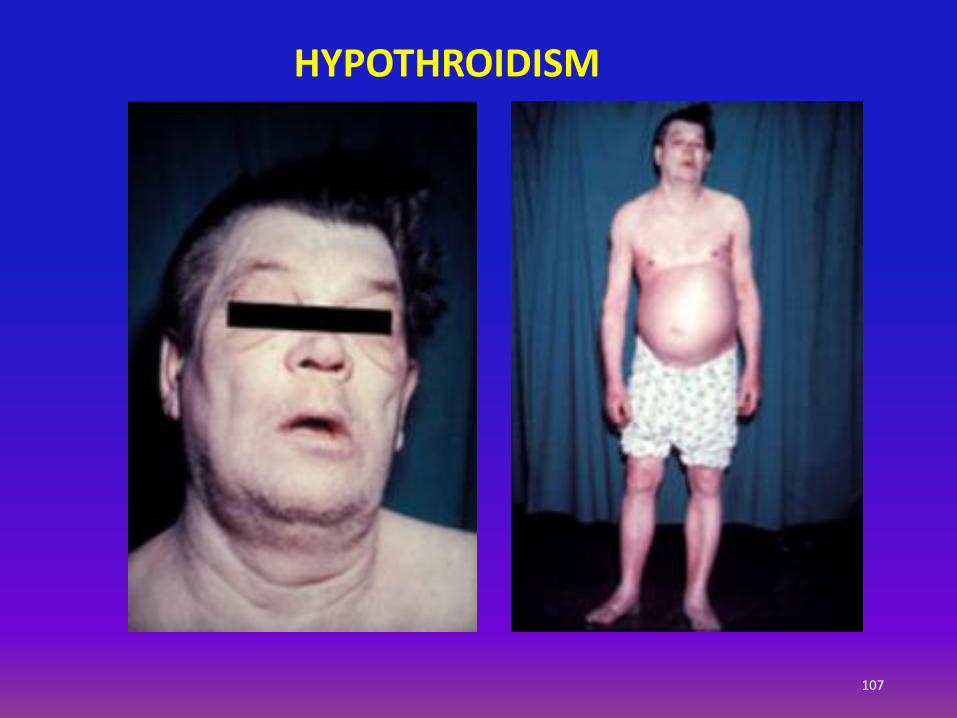
• Changes in the menstrual cycle
• Constipation
• Depression
• Dry hair , hair loss, dry skin
• Fatigue
• Greater sensitivity to cold
• Slow heart rate
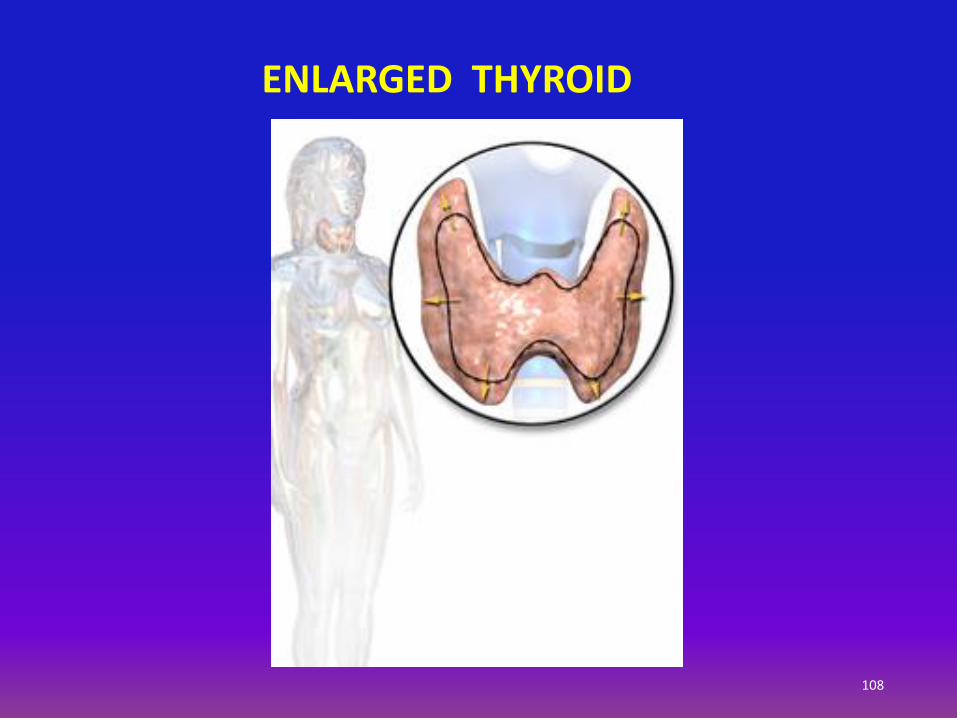
• Swelling of the thyroid gland (goiter)
• Unexplained weight gain or difficulty losing weight
• Carpal tunnel syndrome
Nervousness, anxiety, and irritability. Shaky hands
Difficulty sleeping
Eyes that bulge out, or "protrude" (in patients with Graves' disease)
Hair brittle, and loss of hair
Irregular heart beat, especially in older adults
Rapid heartbeat, usually over 100/min.
Menstrual cycle changes, including lighter bleeding and less frequent periods
Muscle weakness, especially in the thighs and upper arms
Rapid fingernail growth
Sweating and thinning skin
Weight loss despite increased appetite
ABNORMAL THYROID - SYMPTOMS Hyperthyroid Hypothyroid
E. MORAN - 2015 103

104
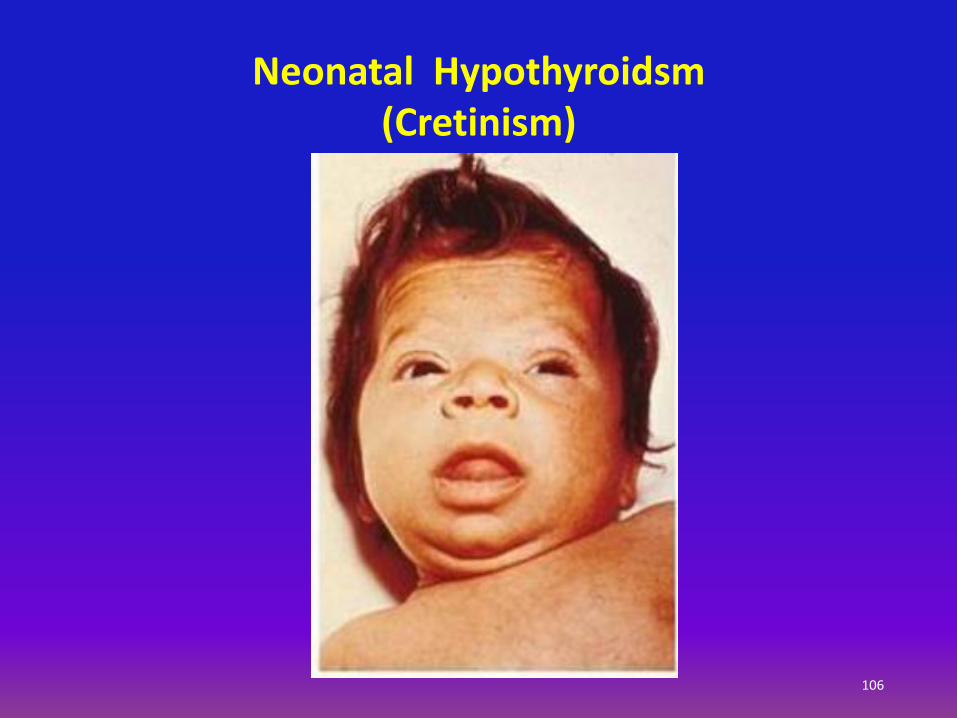
HYPOTHYROIDISM
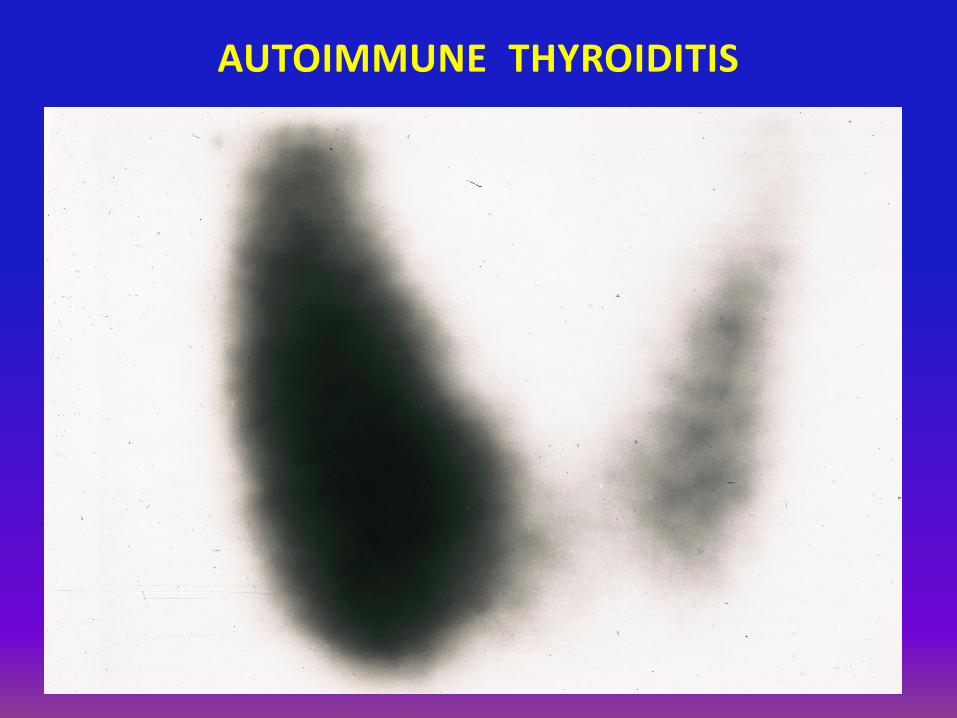
AUTOIMMUNE THYROIDITIS
E. MORAN - 2015 105
107
HYPOTHROIDISM

E. MORAN - 2015 109
Lumps in the thyroid gland
90% are benign
Cause: Unknown
Hashimoto thyroiditis
Iodine deficiency
Diagnosis: Ultrasound
Thyroid scan
Thyroxine (T4) level
Thyroid-stimulating hormone (TSH)
Fine needle biopsy
THYROID NODULES
E. MORAN - 2015 110
Diagnosis:
Physical examination
Ultrasound
Thyroid I131 scan
Treatment:
Anti-thyroid medication (PTU)
Radioactive iodine medication
Surgery
Beta-blockers
DIAGNOSIS AND TREATMENT OF HYPERTHYROIDISM

E. MORAN - 2015 111
Burden of suffering: US 2015 Est. 62,450 new cases
Risk factors: 25 - 65 y.o.
Female
Neck radiation in childhood
Past history of goiter
Family history of thyroid cancer
Genetic conditions of multiple endocrine neoplasia
THYROID CANCER
E. MORAN - 2015 112
Diagnosis: Physical examination
Laryngoscopy
Ultrasound
CT scan
PET-CT scan
Blood tests and hormonal profile (TSH)
Fine needle biopsy
Excisional biopsy
Treatment: Thyroidectomy + Hormonal replacement
THYROID CANCER

113
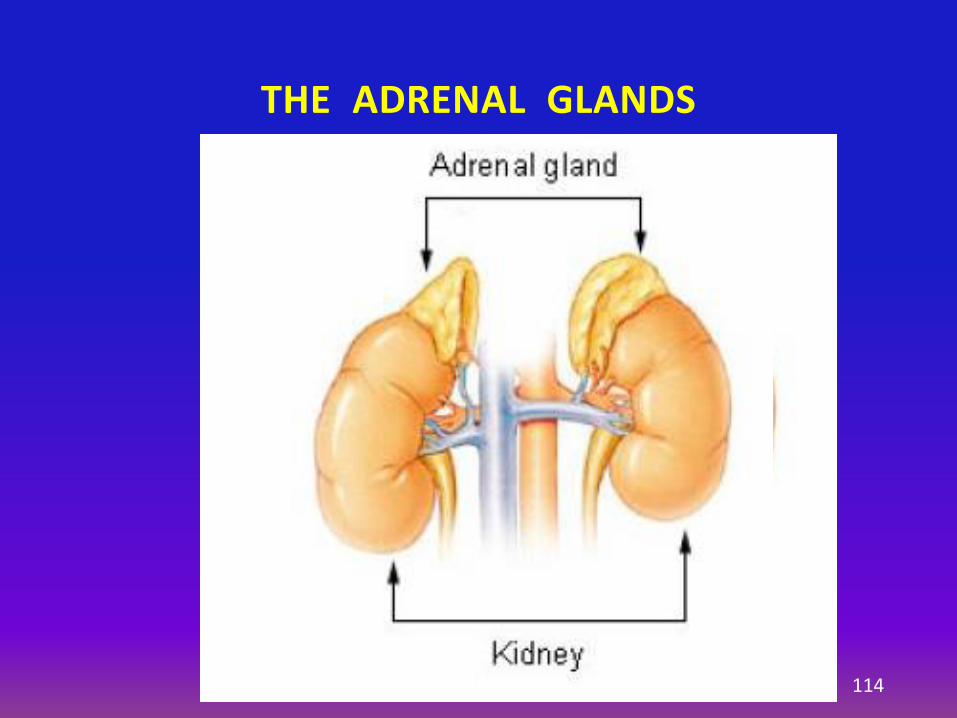
THE ADRENAL GLANDS
114
Cortex: Glucocorticosteroids
- Gluconeogenesis
- Suppress immune response
Mineral corticosteroids - Aldosterone
Androgens – sex 2° characteristics
Estrogens – sex 2° characteristics
Medulla: Epi- and nor-adrenaline
Stress response
THE ADRENAL GLANDS
E. MORAN - 2016 115
END OF LECTURE #4
116


















