DICOM Activities - BRAZIL Alair Santos – CBR ( Brazilian College of Radiology) Nikko – 18/4/2012.
Upload
truongphucCategory
view
219download
2
Hw
BE
a
A
R
R
A
K
R
H
I
S
H
C
D
W
1
Hssoei
1d
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 S ( 2 0 0 7 ) S425–S432
journa l homepage: www. int l .e lsev ierhea l th .com/ journa ls / i jmi
L7 and DICOM based integration of radiology departmentsith healthcare enterprise information systems
ojan Blazona ∗, Miroslav Koncarricsson Nikola Tesla d.d., Zagreb, Croatia
r t i c l e i n f o
rticle history:
eceived 7 January 2007
eceived in revised form 8 May 2007
ccepted 8 May 2007
eywords:
adiology Information System
ospital Information System
ntegrated Healthcare Information
ystem
ealth Level 7 (HL7)
linical Document Architecture
ICOM
ADO
a b s t r a c t
Purpose: Integration based on open standards, in order to achieve communication and infor-
mation interoperability, is one of the key aspects of modern health care information systems.
However, this requirement represents one of the major challenges for the Information and
Communication Technology (ICT) solutions, as systems today use diverse technologies, pro-
prietary protocols and communication standards which are often not interoperable. One
of the main producers of clinical information in healthcare settings represent Radiology
Information Systems (RIS) that communicate using widely adopted DICOM (Digital Imaging
and COmmunications in Medicine) standard, but in very few cases can efficiently integrate
information of interest with other systems. In this context we identified HL7 standard as the
world’s leading medical ICT standard that is envisioned to provide the umbrella for medical
data semantic interoperability, which amongst other things represents the cornerstone for
the Croatia’s National Integrated Healthcare Information System (IHCIS). The aim was to
explore the ability to integrate and exchange RIS originated data with Hospital Information
Systems based on HL7’s CDA (Clinical Document Architecture) standard.
Methods: We explored the ability of HL7 CDA specifications and methodology to address the
need of RIS integration HL7 based healthcare information systems.
Results: We introduced the use of WADO service interconnection to IHCIS and finally CDA
rendering in widely used Internet explorers. The outcome of our pilot work proves our orig-
inal assumption of HL7 standard being able to adopt radiology data into the integrated
healthcare systems.
Conclusion: Uniform DICOM to CDA translation scripts and business processes within IHCIS
is desired and cost effective regarding to use of supporting IHCIS services aligned to SOA.
these issues by defining business processes in care delivery
. Introduction
ealthcare delivery environments are under constant pres-ure to rationalize the cost of care provisioning while at theame time having to preserve or even increase the quality
f care pathways and clinical processes. In the process ofvaluation how to address this stringent set of requirements,ntegration and integrated personalized care based on the∗ Corresponding author at: Krapinska 45, p.p. 93, HR-10002 Zagreb, CroaE-mail address: [email protected] (B. Blazona).
386-5056/$ – see front matter © 2007 Elsevier Ireland Ltd. All rights resoi:10.1016/j.ijmedinf.2007.05.001
© 2007 Elsevier Ireland Ltd. All rights reserved.
well-founded Information and Communication Technology(ICT) solutions are recognized as the major quality component[1]. In that sense, Hospital Information Systems (HIS) and inte-grated healthcare information infrastructures need to address
tia. Tel.: +385 1 365 3266.
settings, and identify the integration mechanisms that includebusiness scenarios and use cases, semantics and communica-tion technology.
erved.

a l i n
S426 i n t e r n a t i o n a l j o u r n a l o f m e d i cIn the process of integration, high quality data manage-ment based on open standards represents the stepping stonein achieving the goals of integrated care. Electronic patientrecord represents the heart of any healthcare services deliverysettings, where the ICT systems that support clinical deliv-ery processes need to “pump” the blood into the heart ofthese systems in an efficient and interoperable manner. Inthat context, we have recognized radiology systems as oneof the major medical data generators that produce a largequantity of important clinical information, which needs to beefficiently integrated in patients’ medical records. Having thatfact in the focus of our work, in this paper we evaluate a pilotapproach to develop a generic framework for the integrationof DICOM (Digital Imaging and COmmunications in Medicine)based Radiology Information Systems (RIS) to the integratedHL7v3 (Health Level 7 ver. 3) enabled Healthcare InformationSystems (HIS). The goal of this research was to define andimplement a reliable and efficient transformation service thatwill bridge DICOM and HL7 standards differences, and enablethe integration of radiology data to the HL7 founded clinicalsettings.
The paper will elaborate in detail developed DCM-CDA(DICOM-CDA) service that provides efficient transformation ofDICOM objects to CDA (Clinical Document Architecture) con-formant XML (Extensible Markup Language) documents. Theaccess to DICOM images has been implemented and accom-plished using the emerging WADO (Web Access to DICOMPersistent Objects) definition.
It is also important to note that we align all of our work withthe strategy for the next generation Croatian healthcare deliv-ery system officially accepted by the Croatian Government.The foundation for all future care processes in Croatia rep-resent the recently officially released national healthcare ICTinfrastructure that is based on Ericsson Nikola Tesla’s Inte-grated Healthcare Information System solution. Among otherfeatures, this solution implements state of the art health-care standards such as HL7v3 and CEN ENV 13606 which areimportant from the perspective of this work. The details of thestrategy as well as components of the IHCIS solution can befound in referenced literature [2].
2. Radiology and hospital systemsinteroperability needs
The DICOM standard represents the evolution of the histori-cal ACR-NEMA (The American College of Radiology—NationalElectrical Manufacturers Association) sets of recommen-dations [3]. DICOM specifies the network communicationrules and the physical data format to enable communica-tion between modalities and humans through developedsoftware solutions. In this context we are focusing on theDICOM supported datasets exchange, which requires spe-cific connectors and communication enablers that use otherwidely accepted standards like HTTP (HyperText TransferProtocol). This requirement has been identified as one of
the key integration components, and has resulted in newadditions to the DICOM standard known as WADO [4].WADO enables the HTTP communication of DICOM objectsby defining the GET parameters of the HTTP request withf o r m a t i c s 7 6 S ( 2 0 0 7 ) S425–S432
pre-defined types of returning context e.g. image/jpeg andtext/xml.
The HL7 standard today represents the foundation of manyhealthcare information management systems [5]. It specifiesstructures and mechanisms to describe and communicateadministrative and clinical data without focusing on a specifichealthcare domain or communication technology. HL7 stan-dard in its’ third version (HL7v3) focuses on the methodologyhow do the clinical and ICT experts specify the final data setsthat are exchanged between systems, and does so by foundingall its’ artifacts on HL7 Reference Information Model. HL7 RIMrepresents one of the major qualities of HL/v3 standard, whichhas been recently accepted by ISO as the global standard onthe international level (The official title: ISO/HL7 21731:2006- Health Informatics - HL7 Version 3 - Reference InformationModel (RIM) - Release 1).
One of the HL7 standard packages that we refer to in ourwork is CDA. CDA introduces document-based specificationsto exchange various clinical data in healthcare delivery envi-ronments, e.g. laboratory reports, discharge letters etc. Basedon the fact that HL7 CDA is widely used as the informationlayer integration solution for heterogeneous healthcare deliv-ery environments, we have identified the CDA specificationsas the bridge of connectivity between RIS systems based onDICOM standard where we consider only WADO as accesspoint, and HL7 enabled HIS systems. However, today thereare no generic data transformation mechanisms and most ofthe transformations are done on a case-by-case basis, whichmakes this research even more challenging and interesting.
Having identified this state, the starting point to this workrepresents the development of the architectural frameworkfor DICOM/HL7 CDA integration [6], which is clearly sepa-rated of the development and final implementation of theservice itself. The idea behind this approach is to introduce aPlatform Independent Model (PIM) that will identify the infor-mation model mappings, and serve as the input to the servicedevelopment that can be then implemented in any preferredtechnology.
2.1. DICOM and HL7 information models
The DICOM to CDA transformation consists of semantic map-ping textual and multimedia contexts. We consider the textualdata mappings according to the semantic meaning, and mul-timedia data linking to the defined WADO services. Directlinking to WADO services enables acquiring multimedia subcontext information from DICOM datasets directly from dis-tant radiology departments.
The DICOM information model consists of IOD(Information Object Definition) elements. Each IOD savesdata relevant to the IOD global context. For example, thepatient’s name, sex and ID are encapsulated in the PatientIOD. In HL7 CDA the patient relevant data is saved underthe patient element, and formatted using XSD (XML SchemaDefinition) specifications and rules. Similarities in bothinformation models are evident from the semantic meaning
according to mapping relevant information from the DICOMdataset to the CDA header.The DICOM and CDA information models have slightlydifferent base models (Fig. 1). The DICOM tag and the CDA

i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 S ( 2 0 0 7 ) S425–S432 S427
F t). Inm
ettwe
tbpw
siaios
2c
Csns
ig. 1 – Information model of DICOM (left) and HL7 CDA (righapped to the corresponding place in the CDA hierarchy.
lement pair define the mapping of information relevant tohe CDA header. The CDA header should provide administra-ive information about included clinical data. In our approache define mappings according to the pairs DICOM tag—CDA
lement place.The CDA body element saves clinical data, which can con-
ain textual and multimedia data. All multimedia data shoulde linked according to CDA external data definition. Linkingresents a hyperlink to the multimedia data, and is availableith simple HTTP transfer protocol.
The DICOM datasets must be divided into parts presentingeparate multimedia content, providing support for multiplemages management. Separate multimedia content is thenvailable using the DICOM WADO specification. WADO spec-fies HTTP GET parameters to query and retrieve modalitiesf underling DICOM solutions to retrieve whole data sets oreparate elements (e.g. images) according to the slice number.
.2. DICOM context management for HL7 enabledommunication
orresponding to the HL7 protocol, a “plug-in” DCM-CDA webervice upgrade is required to enable HL7 interfaces commu-ication to DICOM enabled systems. We determine that thiservice should be mediator to enable HL7v3 communication to
Fig. 2 – System architecture enabling HL7 to DICOM
formation in Patient IOD, Visit IOD and Study IOD, is
the DICOM WADO service as illustrated on Fig. 2. Operationsfor query and translation within DCM-CDA service should bemade on the HL7v3 messaging protocol. Our pilot solution usedirect SOAP communication as request to DCM-CDA service,but final output is HL7v3 CDA document. Note that authentica-tion and authorization services for this framework are usuallyimplemented by a third party service provider. In the Croatiancase, directory services and access manager implemented bythe national healthcare infrastructure provide these features.
2.3. Radiology report in HL7 healthcare deliveryenvironment, activity scenario
Acquisition modality is starting point for radiology reportgeneration. All images are saved within Picture Archivingand Communication Systems (PACS) in accordance to DICOMstandard. The business processes usually include radiologyspecialists contacting PACS systems, and after examining cap-tured images they generate report in the textual form, alsousually accompanied with snippets of diagnostic images (seeFig. 3). Report is saved according to the DICOM specifications
to the RIS system as Structured Report (SR) referencing Ser-vice Object Pairs (SOP) instances (images, waveforms, etc.),which would make this system highly important to the inte-grated care processes and patient care pathways. As the nextcommunication through DCM-CDA service.

S428 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 S ( 2 0 0 7 ) S425–S432
ithin
Fig. 3 – Radiology report exchange pattern wstep patients are usually referred back to his family doctor,where the assigned physician would access RIS repositoriesin order to acquire radiologists’ reports or original radiologyimages to identify next steps in the patient cure processes.With this interaction a centralized translation service, in thiscase DCM-CDA would be used to provide necessary RIS repos-itory connection, querying and standard translation to HL7.Once the data is available to the assigned physician, he isauthorized to update patient healthcare record, and define fur-ther actions to be instantiated (e.g. prepare new prescriptionor referral for the patient, etc.).
There are many benefits why the ability of accessing radi-ology reports and DICOM original content outside the RIS oreven HIS bring benefits to the care delivery systems. The mostsignificant ones can be listed as follows:
• Direct access to latest radiology reports for patients inde-pendent of place and time of access, which enablesphysicians to make efficient and correct decisions based onvalid and accurate data.
• Improving the importance and empowering family physi-cians in the patient care processes, which is proved to bringquality improvements and cost savings to the system.
• Patient’s choice of the hospital or private stakeholders totake radiology examination is improved, as the data wouldbe available in an efficient, location and time independentmanner.
Fig. 4 – Testing environment consist of a HIS portal, a DCM-
Integrated Healthcare Information System.
• Simple reuse of cost expensive acquisition modalities andradiology specialists allowing patient guide to earliest freeacquisition modality.
• RIS to RIS integration and sharing of resources, which pro-vides the foundation of knowledge sharing and opinionsexchange between radiology specialists.
• Telemedicine consultations within or outside RIS, HIS,region or other country, which is proven to bring extremequality improvements during the health services provision-ing, both on the cost and quality aspects.
3. Results
The presented integration framework with the DCM-CDA ser-vice upgrade has been implemented in a testing environmentas illustrated in Fig. 4. The testing environment consisted of aDCM-CDA integration component, a web based WADO imple-mentation and a HIS portal web application, which simulatedthe services provided by the Croatian national healthcareinfrastructure. Additional extension to WADO has been imple-mented to enable querying DICOM objects by unique Patient
Identifier, where XML file with resulting DICOM ObjectID’s isreturned as the response to the query. HL7 communicationwith DCM-CDA was facilitated using the Web Service’s imple-mentation (Fig. 5).CDA service and a WADO application implementation.
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 S ( 2 0 0 7 ) S425–S432 S429
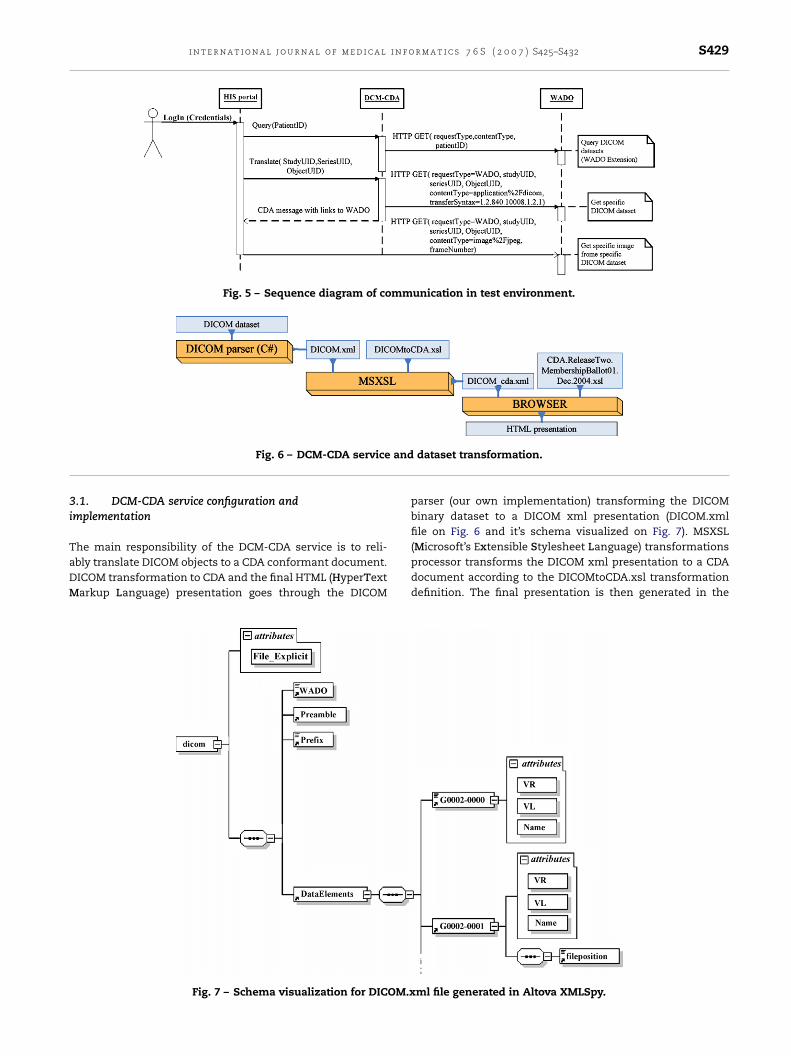
Fig. 5 – Sequence diagram of communication in test environment.
and
3i
TaDM
Fig. 6 – DCM-CDA service
.1. DCM-CDA service configuration andmplementation
he main responsibility of the DCM-CDA service is to reli-bly translate DICOM objects to a CDA conformant document.ICOM transformation to CDA and the final HTML (HyperTextarkup Language) presentation goes through the DICOM
Fig. 7 – Schema visualization for DICOM.x
dataset transformation.
parser (our own implementation) transforming the DICOMbinary dataset to a DICOM xml presentation (DICOM.xmlfile on Fig. 6 and it’s schema visualized on Fig. 7). MSXSL
(Microsoft’s Extensible Stylesheet Language) transformationsprocessor transforms the DICOM xml presentation to a CDAdocument according to the DICOMtoCDA.xsl transformationdefinition. The final presentation is then generated in theml file generated in Altova XMLSpy.

S430 i n t e r n a t i o n a l j o u r n a l o f m e d i c a l i n f o r m a t i c s 7 6 S ( 2 0 0 7 ) S425–S432
Fig. 8 – DICOM to CDA transformation.
rme
Fig. 9 – Sample of DICOM dataset transfoclient’s user interface, which, in this case, is a simple browser.The DICOM CDA presentation is rendered according to theCDA to HTML transformation published with the CDA stan-dard (Fig. 6).
3.2. DICOM to CDA transformation flow
The DICOM datasets are first transferred to a simple XMLformat, as annotated in the previous chapter. The XML rep-resentation of the DICOM object represents the input forDICOMtoCDA.xsl transformation. The DCM-CDA service then
Fig. 10 – Web access porta
d to CDA and rendered in web browser.
generates the final DICOM CDA presentation based on thisinput. The DICOM to CDA transformation consists of severaltransformations, where each transformation element handlesa different CDA sub domain (Fig. 8). That makes the servicemodular and easy to maintain.
3.3. User-end presentation of the CDA document
The HTML presentation of the CDA translated DICOMdataset is generated according to the pre-defined XSLT(Extensible Stylesheet Language Transformations) transfor-
l to DCM-CDA service.

i n f o r m a t i c s 7 6 S ( 2 0 0 7 ) S425–S432 S431
manufeEws
3
Saiads
dsIfa
4
TtcoBombhapaOmmXarti
soiihtwihaa
The following table shortly lists our main conclusionsand lessons learned that are primarily based on the gen-erated results as discussed above
Summary of conclusion and lessons learnedfrom this project
Main conclusion Lessons learned fromproject
• Well defined serviceinterface for exchangeof radiology reportsthrough HL7 enabledinformation systemsmakes the careprovisioning moreefficient, timely andaccurate.
• Web services providereasonable choicefor this serviceimplementationsince WS-*standards givedesired level ofupgradeability andfull SOA integration.
• DCM-CDA service fitswell with the businessprocesses for imagequery, translation andretrieval, which isimportant from theoverall adoptionperspective.
• The simplestbusiness process upto the DCM-CDAservice and betweenDCM-CDA serviceand whole RIS,prepare this servicefor full SOA adoptionwithin IHCIS.
• Division of theDCM-CDA translationscript to IODMODULES and DICOMDictionary simpledatabase and othertranslation subscripts.
• Cost effectivesolution regarding tomaintenance anduse of supportingservices whichaffects final cost (e.g.security).
• Readiness for fullintegration withinCroatian nationalinfrastructure as oneof our major goals.
• Ease of use,upgradeable, easymaintainable andfull versioningsolution for furtherstandard upgrades.
• Proof of conceptsystem developed in
r
i n t e r n a t i o n a l j o u r n a l o f m e d i c a l
ation scheme used by the client’s web browser (Fig. 9)nd browsers internal XSL processor like MSXML for Inter-et Explorer. To meet with the performance and bandwidthtilization requirement, all images are retrieved directly
rom the WADO web application, according to the gen-rated external resource elements in the CDA document.xternal resources are transformed to a HTTP requestith GET method required attributes according to WADO
pecification.
.4. Simple web access to DCM-CDA service
ervice for standard transformation (like DCM-CDA) is simplydopted in HIS system or exposed to physician systems by giv-ng a simple access to radiology reports through HL7 standardnd Web Services. Fig. 10 shows login to HIS portal, with cre-entials (in production site this is provided through token ormartcard).
Physician is uniquely identified according to his/her cre-entials and he/she can start Radiology report query forpecific patients radiology report according to patients uniqueD. After some time service respond with all radiology reportsor patient from all locations for which DCM-CDA service haveccess.
. Conclusion
he primary target of this research has been the evalua-ion of the standard based methodology and tools to enableross-communication of patient information between radiol-gy systems and general sense hospital information networks.ased on the results provided we can conclude that the devel-ped DCM-CDA represents an easy to use, configurable andodular component which facilitates the main integration
ridge from the medical imaging management solutions to theealthcare information networks. This bridge is envisioneds one of the major quality components when it comes toatient care delivery, which improves overall patient safetynd decreases the cost of the care processes and services.ur solution starts with the detailed analysis of informationodels, and facilitates WADO definitions to provide accessechanisms from patient clinical data to diagnostic images.
SLT based transformation gives the advantage of upgrades inccordance with most recent specific standard changes. Ouresults also prove the technical correctness of this componento be fully aligned with the needs of RIS/HIS integration basedn the DICOM and HL7 standards.
It is also important to note that the decision to use HL7tandard has been heavily influenced by the wide adoptionf HL7 recommendation, including the national healthcare
nfrastructure in Croatia. Although at this stage IHCIS facil-tates the support for primary care processes only, Croatiaas over the years had many successful telemedicine pilotshat have proved a high value of the concept for a countryith over 1000 islands and other areas that are not so eas-
ly reachable. IHCIS is envisioned to represent the healthcareighway in the future that includes telemedicine applicationss well. In that context we see the importance of this works being a fully feasible technical bridge between radiology
[
[
test environment.
sessions supported by the patient medical history containedin IHCIS.
e f e r e n c e s
1] Crossing the Quality Chasm: A New Health System for the21st Century, Institute of Medicine (IOM), 2001, ISBN0-309-07280-8.
2] M. Koncar, D. Gvozdanovic, Primary healthcare informationsystem—the cornerstone for the next generation healthcare

a l i n
[
[
S432 i n t e r n a t i o n a l j o u r n a l o f m e d i c
sector in republic of croatia, Int. J. Med. Inform. 75 (2006)306–314.
3] NEMA, DICOM standard 2004,
http://medical.nema.org/dicom/2004.html (online, accessedJanuary 2006).4] E. Cordonnier, B. Hervault, K. Rommelse, D. Harvey, F.M.Behlen, Early Implementations of WADO Web Access toDICOM Persistent Object, ISO TC125/DICOM, San Diego, 2004,
[
[
f o r m a t i c s 7 6 S ( 2 0 0 7 ) S425–S432
http://medical.nema.org/Dicom/minutes/WG-10/2004/2004-01-24/WADO-implementations-20040123.ppt (online,accessed January 2006).
5] HL7 Inc. Official Web Page, http://www.hl7.org (online,accessed January 2006).
6] B. Blazona, M. Koncar, Osnove za komunikaciju izmenuDICOM i HL7 normi, Med. Inform., 2005, Rijeka, Croatia, pp.47–53, ISSN 1330-1799.