HIV/AIDS POST-BARCELONA: TREATMENT COSTS …€¦ · v6 million people in need of drugs and only...
34
The PHRplus Project is funded by U.S. Agency for International Development and implemented by: Abt Associates Inc. and partners, Development Associates, Inc.; Emory University Rollins School of Public Health; Philoxenia International Travel, Inc. Program for Appropriate Technology in Health; SAG Corp.; Social Sectors Development Strategies, Inc.; Training Resources Group; Tulane University School of Public Health and Tropical Medicine; University Research Co., LLC. HIV/AIDS POST HIV/AIDS POST - - BARCELONA: BARCELONA: TREATMENT COSTS EXAMINED TREATMENT COSTS EXAMINED Gilbert Kombe, MD, MPH Senior HIV/AIDS Technical Advisor American Public Health Association Seminar Series Washington, DC December 12, 2002
Transcript of HIV/AIDS POST-BARCELONA: TREATMENT COSTS …€¦ · v6 million people in need of drugs and only...

The PHRplus Project is funded by U.S. Agency for International Development and implemented by:
Abt Associates Inc. and partners, Development Associates, Inc.; Emory University Rollins School of Public Health; Philoxenia International Travel, Inc. Program for Appropriate Technology in Health; SAG Corp.; Social Sectors Development Strategies, Inc.; Training Resources Group; Tulane University School of Public Health and Tropical Medicine; University Research Co., LLC.
HIV/AIDS POSTHIV/AIDS POST--BARCELONA:BARCELONA:
TREATMENT COSTS EXAMINEDTREATMENT COSTS EXAMINED
Gilbert Kombe, MD, MPH
Senior HIV/AIDS Technical AdvisorAmerican Public Health Association Seminar Series
Washington, DCDecember 12, 2002
Overview of Presentation
v Purpose of presentation
v Global Antiretroviral (ARV) Issuesv Changing landscape in HIV/AIDS Treatment
v Why cost information on HIV/AIDS treatment is needed
v PHRplus’ experience in estimating costs of ARV treatmentv Mexico v Application of AIDSTREATCOST (ATC) model in Zambiav Costing of HIV/AIDS within basic health care package
v Discussion

v To share PHRplus’ experience in providing technical assistance to national governments
v To share tools for estimating costs of antiretroviral treatment programs
Purpose of Presentation

Global ARV Issues: Changing Landscape I
v Global mobilization of financial resources, e.g.,
vMulti-Country HIV/AIDS Program for Africa (MAP) loans.v $500M for 2001- 13 countries
vDebt relief for 38 HIPC
vFirst funding from Global Fund for AIDS, TB, Malariav 45% of the total awards ($378 million) will pay for drugs
v 21 out of the 28 recipient countries will purchase ARV drugs
v Expand access to 220,000 PLHA (currently 230,000 being treated)
v Global momentum to expand access to HAART in low resource countries
v HIV/AIDS is at the top of the international development agenda
v Rapid fall in drug pricesv 6 million people in need of drugs and only 230, 000 have access to
them (WHO, 2002)
Global ARV Issues: Changing Landscape II
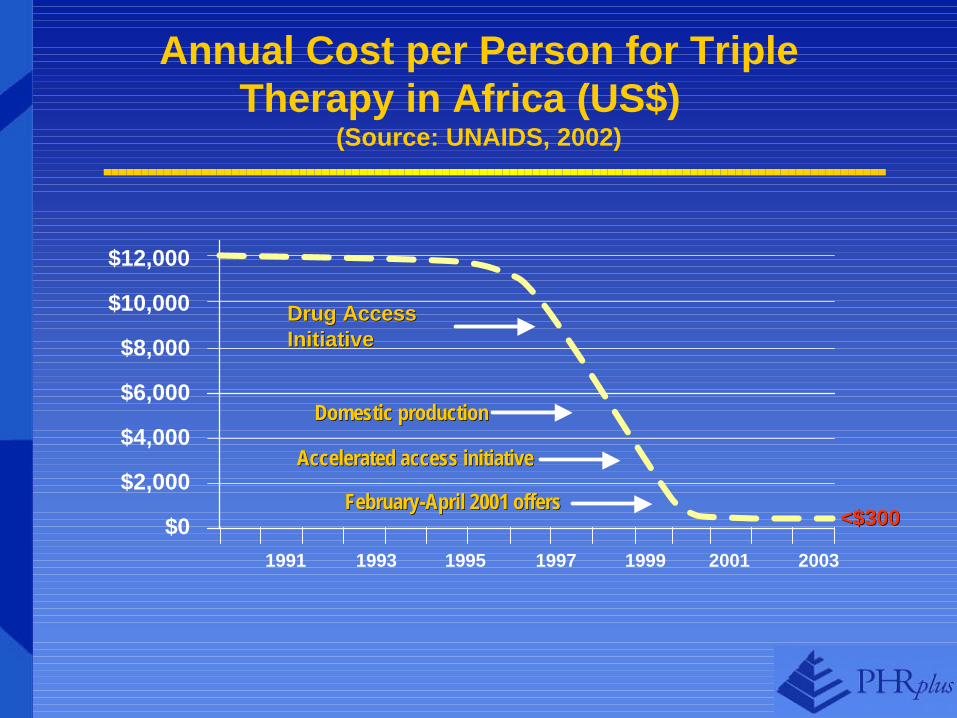
Annual Cost per Person for Triple Therapy in Africa (US$)
(Source: UNAIDS, 2002)
<$300<$300
$12,000
$10,000
$8,000
$6,000
$4,000
$2,000
$01991 1993 1995 1997 1999 2001 2003
Drug Access Drug Access InitiativeInitiative
Domestic productionDomestic production
Accelerated access initiativeAccelerated access initiative
FebruaryFebruary--April 2001 offersApril 2001 offers

What Gains are Countries Expecting by Introducing ART?
Delayed clinical progression
Reduced HIV transmission Reduced OI
Improved quality of life Reduced number of orphans
Return to productive capacity
Reduced hospitalization

Positions on Provision of ARV drugsin Low Resource Countries
SupportNeutral
Oppose

PHRplus Experience with Costing of Antiretroviral Treatment Programs in Mexico
and Zambia
The question is not whether countries are costing ARV treatment but rather what elements of ARV
activities they are costing
Key Policy Questions for Countries Implementing HAART
vWhat will be the maximum number of people willing to use ARV drugs (demand)?
v How many people will benefit from ARV drugs (need)?
v How can ARV drugs be delivered safely, consistently and without delays in the existing systems?
vWhat is the cost of providing these drugs and who will pay for them?

v Growing interest to understand the cost of HIV/AIDS treatment to the health system
v Limited cost information on introduction of antiretroviral treatment into the public health system
v Better costing information is needed to guide management of services and resource allocation
Why is Cost Information on Antiretroviral Treatment Needed?
Elements of ARV Programs that are Being Costed
ARV Drugs
PMTCT
Laboratory Testing
Treatment of Opportunistic
Infections
Training of health providers
Voluntary Counseling
Infrastructure

Mexico ExperienceMexico Experience

Purpose & Objectives of the Study
v To document the Mexican experience in HIV/AIDS treatment in 3 health subsystemsv Ministry of Health (SSA)v Mexican Social Security Institutes (IMSS/ISSSTE)v National Institutes of Health (INS)
v To identify patterns of HIV/AIDS care and treatment and related costs by type of therapy receivedv ARV triple therapy or not
v To estimate the annual care costs per patient byv Subsystemsv Care setting (Inpatient, outpatient)v Level of care (Specialized clinics, secondary and tertiary) v Disease stage (CDC classification)

Study Approach
p Study period from 01/1999-12/2001
p Multi-center retrospective chart review (IRB approval from each site)
p Convenience sampling approach to reflect clinical & treatment criteria of interest
p For patients included in the study, data was captured 3 years retrospectively

Background of HIV/AIDS in Mexico
v Health spending is 5.3% of GDPv 48% public/52% private
vMexico ranks 13th globally and 3rd in the Americas in total reported HIV cases
v Government estimates 64,000 AIDS cases and 177,000 HIV+ (2000)
v Estimated Adult HIV prevalence 0.29% (1999)

Antiretroviral Treatment Issues
v Mexico started providing ARVs in 1997
v By 1999, 55% of PLWA had regular access to ARVs
v Access to ARV treatment and care varies considerably across socioeconomic groups
v Current SSA services do not include ARVs although federal, states, local provide some coverage
v Official norms state that all patients have the right to prescribed treatment at any facility and in any subsystem
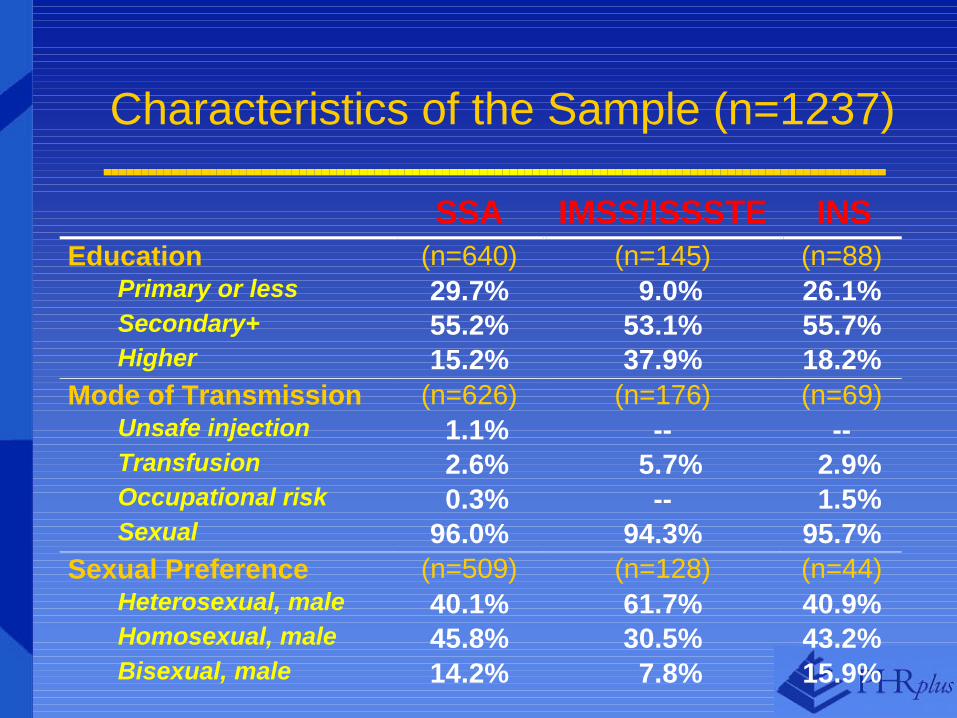
SSA IMSS/ISSSTE INS Education (n=640) (n=145) (n=88)
Primary or less 29.7% 9.0% 26.1% Secondary+ 55.2% 53.1% 55.7% Higher 15.2% 37.9% 18.2%
Mode of Transmission (n=626) (n=176) (n=69) Unsafe injection 1.1% -- -- Transfusion 2.6% 5.7% 2.9% Occupational risk 0.3% -- 1.5% Sexual 96.0% 94.3% 95.7%
Sexual Preference (n=509) (n=128) (n=44) Heterosexual, male 40.1% 61.7% 40.9% Homosexual, male 45.8% 30.5% 43.2% Bisexual, male 14.2% 7.8% 15.9%
Characteristics of the Sample (n=1237)

SSA IMSS/ISSSTE INS Mono, dual therapy 220 5 5
Triple therapy 500 269 97
Deceased 104 22 15
Subtotal (n=1237) 824 296 117
Key Finding #1: Despite the norm, there are patients on mono, dual therapy

Key finding #2: Patients start treatment in advanced stages, improvement is gradual
resultado_cd4
cd4year-1 cd4year3
0 500 1000 1500 2000
0
.001
.002
.003
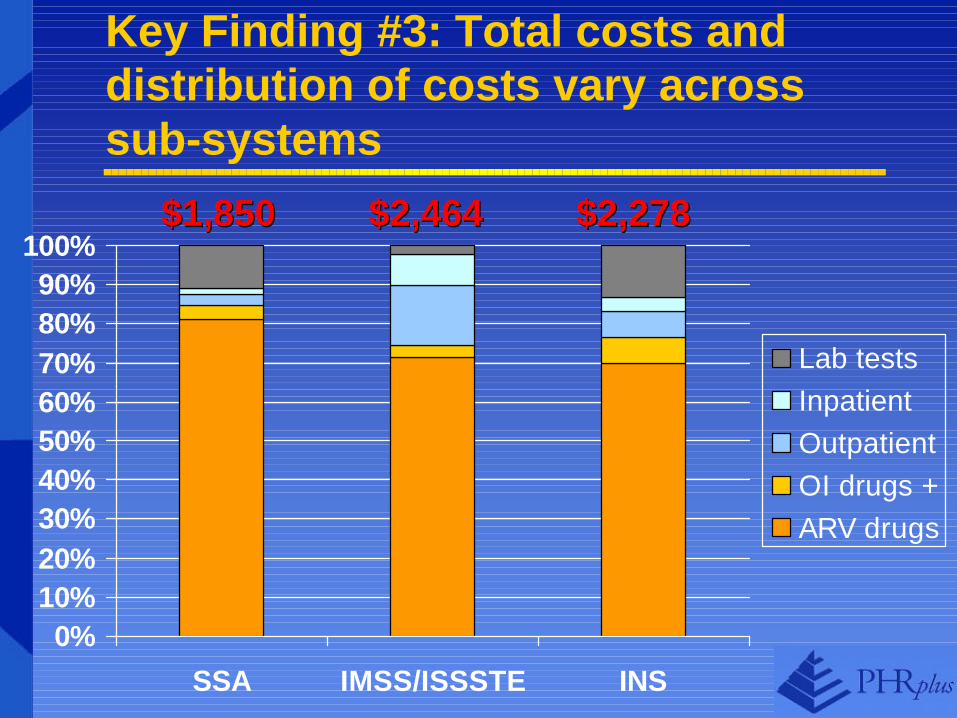
Key Finding #3: Total costs and distribution of costs vary across sub-systems
0%10%20%30%40%50%60%70%80%90%
100%
SSA IMSS/ISSSTE INS
Lab testsInpatientOutpatientOI drugs +ARV drugs
$1,850$1,850 $2,464$2,464 $2,278$2,278

Key Finding #5: Hospitalization costs decrease, outpatient costs increase
0
50
100
150
200
250
300
-3 -2 -1 1 2 3
OutpatientInpatient
initiation of triple therapyinitiation of triple therapy
Zambia ExperienceZambia Experience

Application of the AIDSTREATCOST (ATC) Model in Zambia
PHRplus is providing TA to the government of Zambia to..
v Estimate the total cost of a national ARV treatment program using varying sets of assumptions;
v Support policy decisions, program planning, and budgeting for ARV treatment;
v Facilitate development of strategies to finance ARV treatment programs consistent with budgetary constraints.

Home Screen

Structure of ATC Model
PopulationPolicy Scenarios & Norms
User defined Parameters
MinimumData Set
Assumptions:Epidemiology
Assumptions:Population
Treated
TestingProtocol
TreatmentProtocol
Assumptions:Access &
Compliance
PersonsTested, Treated
Effect on the Epidemic:
Morbidity/Mortality
Utilization ofSpecific Services
And Products
5 year Resource Requirements and Costs
User Set Parameters
Data
Computations
Baseline Situation
CostingAssumptions
& Data
OUTPUT•Training
•Population
•Location
•Financing

Baseline Assumptions Editor
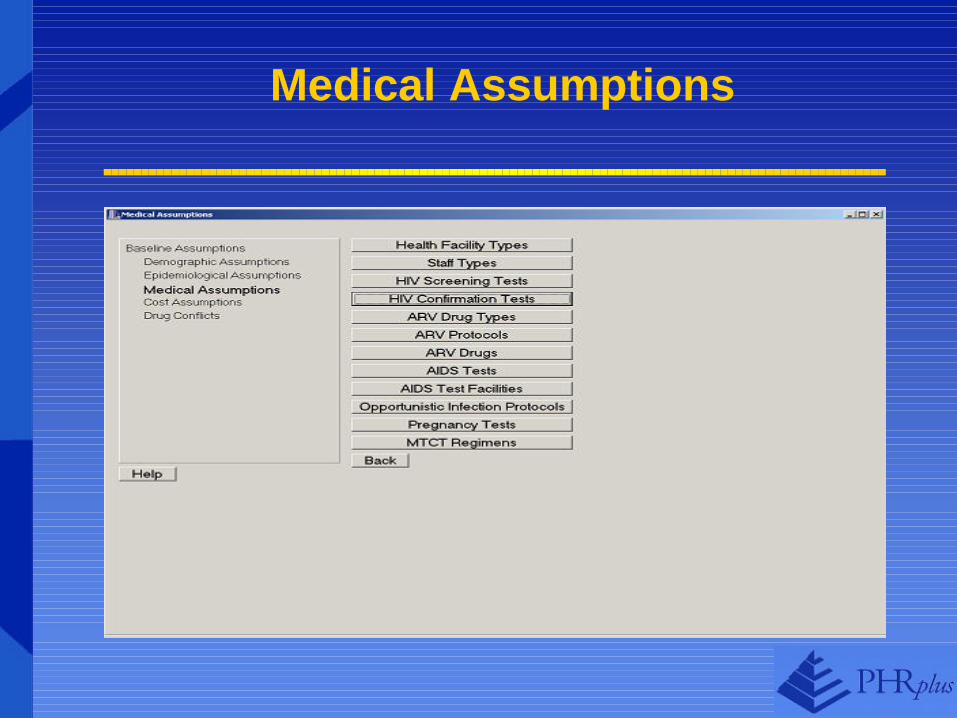
Medical Assumptions

Graph 1: Total Cost of High and Low-Cost ARV Treatment Programs, by Year

Graph 2: Cost of ARV Treatment in a Single Program, by Year

Summary of Pre- and Post Barcelona Changes
PrePre--BarcelonaBarcelona
v National & Regional mobilization of resources
v Very few lessons of providing ARVs in low/middle income countriesv Limited access to ARVs
v High prices of ARV drugs
PostPost--BarcelonaBarcelona
v Global mobilization of resources
v More lessons emerging on ART provision in low resource countriesv Expanded access
v Reduced prices of ARVs

Take Home Messages
v Antiretroviral treatment does not equal to ARV drugs alone
v The total cost of treatment is not the number of people multiplied by the cost of drugs per person.
v Antiretroviral treatment will shift the pattern of care from inpatient to outpatient

Acknowledgements
v PHRplusvA.K. Nandakumar, Kathleen Novak, Miriam Mokuena, Caroline
Quijada, Stephen Musau, Owen Smith, Alison Comfort, Jonathan Wilwerding, Charlotte Leighton
vMexican Institute of Public HealthvStefano Bertozzi, Sergio Bautista, Juan Pablo Gutierrez
vMinistry of Health- Zambiav USAID colleaguesvGlobal Bureau/Office of HIV/AIDS, LAC Bureau
Sponsored by the U.S. Agency for International DevelopmentContract No. HRN-C-00-00-00019-00
The PHRplus Project is funded by U.S. Agency for International Development and implemented by:
Abt Associates Inc. and partners, Development Associates, Inc.; Emory University Rollins School of Public Health; Philoxenia International Travel, Inc. Program for Appropriate Technology in Health; SAG Corp.; Social Sectors Development Strategies, Inc.; Training Resources Group; Tulane University School of Public Health and Tropical Medicine; University Research Co., LLC.
Thank YouThank You