Simulations of Hirschsprung's Disease Using Fractional Differential ...
Upload
nguyenphucCategory
view
215download
0
For Peer Review
Hirschsprung's disease prevalence in Europe: a register-
based study
Journal: Birth Defects Research Part A: Clinical and Molecular Teratology
Manuscript ID: Draft
Wiley - Manuscript type: Original Research Article
Date Submitted by the Author: n/a
Complete List of Authors: Best, Kate; Newcastle University, UK, Institute of Health & Society Addor, Marie-Claude; Division of Medical Genetics, Arriola, Larraitz; Subdireccion de Salud Publica, Balku, Eszter; National Institute of Health Development, Dept of Hungarian Congenital Abnormality Registry & Surveillance, Barisic, Ingeborg; Children's University Hospital, Bianchi, Fabrizio; CNR Institute of Clinical Physiology, G Monasterio Tuscany Foundation Calzolari, Elisa; Universitaria Ferrara, Azienda Ospedaliero Curran, Rhonda; University of Ulster, Doray, Berenice; Strasbourg Prospective Study of Congenital Malformations, Draper, Elizabeth; University of Leicester, Garne, Ester; Hospital Lillebaelt, Gatt, Miriam; Department of Health Information and research, Haeusler, Martin; Medical University of Graz, van Kammen-Bergman, Jorieke; Department of Medical Genetics, University of Groningen, Khoshnood, Babak; The Paris Registry of Congenital Malformations, Klyungsoyr Melve, Kari; Medical Birth Registry of Norway, Martos, Carmen; Centro Superior de Investigación en Salud Pública, Materna-Kiryluk, Anna; Center for Medical Genetics, Matias Dias, Carlos; Instituto Nacionale de Saude Dr. Ricardo Jorge, McDonnell, Robert; Health Service Executive, Mullaney, Carmel; Health Service Executive, Nelen, Vera; Provinciaal Instituut voor Hygiene, O'Mahony, Mary; Health Service Executive, Queisser-Luft, Annette; Universitatskinderklinik Mainz, Randrianaivo-Ranjatoelina, Hanitra; Naitre Aujourd'hui, Rissman, Anke; Otto-von-Guericke University, Malformation Monitoring Centre Saxony-Anhalt, Medical Faculty Rounding, Catherine; University of oxford, National Perinatal epidemiology Unit Sipek, Antonin; Thomayer University Hospital, Department of Medical Genetics Thompson, Rosie; St Michael's Hospital, Institute of Child Life and Health Tucker, David; Public Health Wales, Wellesley, Diana; Princess Anne Hospital, Wessex Clinical Genetics Service Zymak-Zakutnya, Natalya; OMNI-Net Ukraine Birth Defects Program, Rankin, Judith; Newcastle University, UK, Institute of Health & Society
Key Words: congenital anomaly, congenital aganglionic megacolon, epidemiology,
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
prevalence, trends
Page 1 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
1
Hirschsprung's disease prevalence in Europe: a register based
study
Kate E Best MSc1, Marie-Claude Addor
2,
Larraitz Arriola
3, Eszter Balku
4, Ingeborg
Barisic5, Fabrizio Bianchi
6, Elisa Calzolari
7,
Rhonda Curran
8, Berenice Doray
9, Elizabeth
Draper10
, Ester Garne
11, Miriam Gatt
12, Martin Hauesler
13, Jorieke van Kammen-Bergman
14,
Babak Khoshnood15
, Kari Klungsoyr16
, Carmen Martos17, Anna Materna-Kiryluk18
, Carlos
Matias Dias19
, Bob McDonnell20
, Carmel Mullaney21
, Vera Nela22
, Mary O’Mahony23
,
Anette Queisser-Luft24
, Hanitra Randrianaivo25
, Anke Rissman26
, Catherine Rounding27
,
Antonin Sipek28
, Rosie Thompson29
, David Tucker30
, Diana Wellesley31
, Natalya Zymak-
Zakutnya32
, and Judith Rankin PhD1*
1 Institute of Health & Society, Newcastle University, Newcastle upon Tyne, England, UK.
2 Service de Genetique Medicale Maternite, CHUV, Lausanne, Switzerland
3 Subdireccion de Salud Publica, San Sebastian, Spain
4 Dept of Hungarian Congenital Abnormality Registry and Surveillance, National Institute of
Health Development, Hungary5 Children’s University Hospital of Zagreb, Clinical Hospital
Sisters of Mercy, Zagreb, Croatia
6 Unit of Epidemiology, IFC CNR (Tuscany Registry of Birth Defects), Pisa, Italy
7 IMER Registry (Emila Romagna Registry of Birth Defects),
8 EUROCAT central registry, University of Ulster, Jordanstown.
9 Dept de Genetique Medicale, Hopital de Hautepierre, Strasbourg, France
10 University of Leicester, UK
11 Hospital Lillebaelt, Kolding, Denmark
12 Department of Health Information and Research, Guardamangia, Malta
13 Medical University of Graz, Austria
14 Department of Medical Genetics, University of Groningen, Netherlands
15 Paris Registry of Congenital Malformations, INSERM U953, Paris, France
16 Medical Birth Registry of Norway, Bergen, Norway
17 Centro Superior de Investigación en Salud Pública, Valencia. Spain
18 Polish Registry of Congenital Malformations, Poznan, Poland
19 Centro de Estudos e registo de A C, Av Padre Cruz, Lisbon, Portugal
20 Health Service Executive, Dublin, Ireland
21 Specialist in Public Health Medicine, Public Health Department, HSE South, Lacken,
Kilkenny, Ireland
22 Provincial Institute for Hygiene, Antwerp, Belgium
23 Health Service Executive, Cork, Ireland
24 Birth Registry Mainz Model, Childrens Hospital, University Medical Center, Johannes
Gutenberg-University, Mainz, Germany
25 Naitre Aujhourd'hui, Saint Denis Cedex, Ile de la Reunion
26 Malformation Monitoring Centre Saxony-Anhalt, Medical Faculty Otto-von-Guericke
University, Magdeburg, Germany
27 National Perinatal Epidemiology Unit, University of Oxford, UK
28 National Registry of Congenital Anomalies, Department of Medical Genetics, Thomayer
Hospital, Prague, Czech Republic
29 St Michaels Hospital, Bristol, UK
Page 2 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
2
30 Public Health Wales, Wales, UK
31 University Hospitals Southampton, Faculty of Medicine and Wessex Clinical Genetics
Service, UK
32 OMNI-Net Ukraine Birth Defects Program, Rivne- Khmelnytskyy, Ukraine
Short title: Hirschsprung's disease in Europe
*Corresponding Author: Prof. Judith Rankin
Address: Institute of Health & Society, Baddiley-Clark Building, Newcastle University,
Newcastle upon Tyne, NE2 4AX, England, UK.
Tel: +44 (0)191 208 5267
Fax: +44 (0)191 222 8211
Email: [email protected]
Word count (abstract excluding key words): 250/250
Word count (excluding title page, abstract, references, figures and tables): 2,796
References: 16
ACKNOWLEDGEMENTS
We thank the many people throughout Europe involved in providing and processing
information, including affected families, clinicians, health professionals, medical record
clerks, and registry staff.
FUNDING
The EUROCAT Joint Action is co-funded by the EC, under the framework of the EU Health
Programme 2008-2013, Grant Agreement 2010 22 04 (Executive Agency for Health &
Consumers). EUROCAT registries are funded as fully described in Paper 6 of Report 9 -
EUROCAT Member Registries: Organization and Activities (Birth Defects Research (Part
A), 91, S51-S100). The responsibility for the interpretation of data and/or information
supplied is the authors’ alone. This paper reports on an independent study which is part-
Page 3 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
3
funded by the Policy Research Programme in the Department of Health, UK. The views
expressed are not necessarily those of the Department.
Page 4 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
4
ABSTRACT 1
Background: 2
Hirschsprung’s disease is a congenital gut motility disorder, characterised by the absence of the 3
enteric ganglion cells along the distal gut. The aim of this study was to describe the 4
epidemiology of Hirschsprung’s disease, including additional congenital anomalies, total 5
prevalence, trends and association with maternal age. 6
Methods: 7
Cases of Hirschsprung’s disease delivered during 1980-2009 notified to 31 European 8
Surveillance of Congenital Anomaly registers formed the population-based case-series. 9
Prevalence rates and 95% confidence intervals (CIs) were calculated as the number of cases per 10
10,000 births. Multilevel Poisson regression was performed to investigate trends in prevalence, 11
geographical variation and the association with maternal age. 12
Results: 13
There were 1,322 cases of Hirschsprung’s disease among 12,146,210 births. The total 14
prevalence was 1.08 (95% CI: 1.03-1.15) per 10,000 births and there was a small but significant 15
increasing trend in prevalence over time (relative risk (RR)= 1.01, 95% Credible interval (CrI): 16
1.00-1.02; p=0.004). There was evidence of geographical heterogeneity in prevalence (p<0.001). 17
Excluding 146 (11.0%) cases with chromosomal anomalies or genetic syndromes, there were 18
1,176 cases (prevalence= 0.97, 95% CI: 0.91-1.03 per 10,000 births), of which 137 (11.6%) had 19
major structural anomalies. There was no evidence of a significant increased risk of 20
Hirschsprung’s disease in cases born to women aged ≥35 years compared to those aged 25-29 21
(RR=1.17, 95% CrI: 1.01-1.35; p=0.355). 22
Page 5 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
5
Conclusion: 23
This large population-based study found evidence of a small increasing trend in Hirschsprung's 24
disease and differences in prevalence by geographic location. There was also no evidence of an 25
association with maternal age.26
Page 6 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
6
INTRODUCTION 27
Hirschsprung’s disease (or congenital aganglionic megacolon) is the most common congenital 28
gut motility disorder, characterised by the absence of the enteric ganglion cells (aganglionosis) 29
along the distal gut, which causes functional intestinal obstruction (Puri and Shinkai, 2004). 30
Previous estimates of the live birth prevalence of Hirschsprung’s disease have ranged between 31
1.63 to 2.60 per 10,000 live births in the UK, USA and Columbia (Best et al, 2012; Goldberg, 32
1984; Spouge and Baird, 1985). While a recent study found evidence of a small increasing trend 33
of Hirschsprung's disease prevalence in the North of England, two older studies in the USA and 34
Columbia, did not (Best et al, 2012; Goldberg, 1984; Spouge and Baird, 1985). 35
Hirschprung's disease is of neural crest origin (Martucciello, 1997) and has known associations 36
with a variety of chromosomal anomalies and genetic syndromes, including Down syndrome 37
and Waardenburg syndrome (Amiel et al, 2008; Goldberg, 1984; Moore, 2006; Spouge and 38
Baird, 1985). Therefore, it is considered to be of genetic origin.(Amiel et al, 2008; Badner et al, 39
1990; Martucciello, 1997; Puri and Shinkai, 2004). But despite this possible genetic aetiology, 40
there is limited research around the association with advanced maternal age (Amiel et al, 2008; 41
Badner et al, 1990; Martucciello, 1997; Puri and Shinkai, 2004). In several studies, maternal 42
age has been examined as a potential risk factor, but these studies have only compared the 43
proportion of older mothers in cases with the study population; producing conflicting results. 44
Goldberg (1984) for example, found a higher proportion of mothers aged ≥30 years among cases 45
compared to the general population of Baltimore, USA whereas both Ryan et al (1992) and Best 46
et al (2012) found no significant differences in proportions in Boston, USA and the North of 47
England (Best et al, 2012; Goldberg, 1984; Ryan et al, 1992). Few other risk factors have been 48
identified although there is a suggestion of an association with ethnicity, with the offspring of 49
white women possibly at increased risk (Goldberg, 1984). Additionally, a male preponderance 50
has consistently been reported (Goldberg, 1984; Ryan et al, 1992; Spouge and Baird, 1985). 51
Page 7 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
7
The aim of this study was to investigate the epidemiology of Hirschsprung's disease in Europe 52
during 1980-2009 using high quality population-based register data. We describe the presence of 53
additional congenital anomalies, pregnancy outcomes, one-week survival, diagnosis, association 54
with maternal age, total prevalence, trends in total prevalence and variation in prevalence 55
according to geographic location.56
Page 8 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF
For Peer Review
8
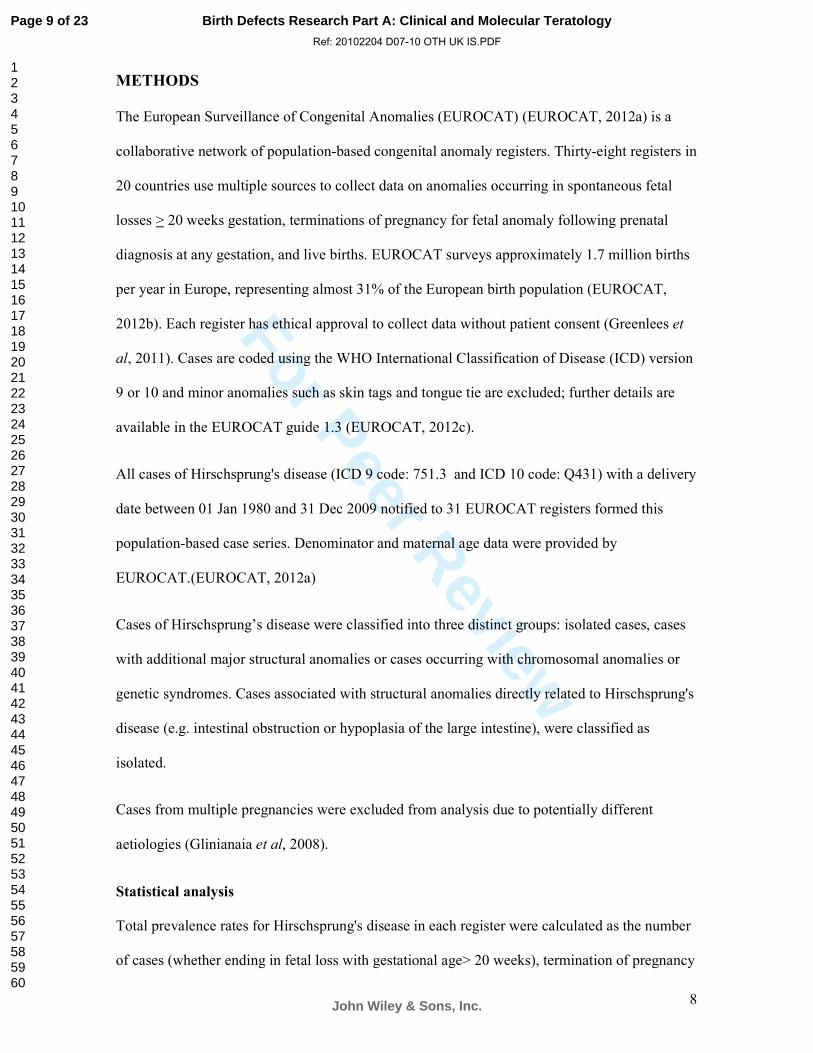
METHODS
The European Surveillance of Congenital Anomalies (EUROCAT) (EUROCAT, 2012a) is a
collaborative network of population-based congenital anomaly registers. Thirty-eight registers in
20 countries use multiple sources to collect data on anomalies occurring in spontaneous fetal
losses > 20 weeks gestation, terminations of pregnancy for fetal anomaly following prenatal
diagnosis at any gestation, and live births. EUROCAT surveys approximately 1.7 million births
per year in Europe, representing almost 31% of the European birth population (EUROCAT,
2012b). Each register has ethical approval to collect data without patient consent (Greenlees et
al, 2011). Cases are coded using the WHO International Classification of Disease (ICD) version
9 or 10 and minor anomalies such as skin tags and tongue tie are excluded; further details are
available in the EUROCAT guide 1.3 (EUROCAT, 2012c).
All cases of Hirschsprung's disease (ICD 9 code: 751.3 and ICD 10 code: Q431) with a delivery
date between 01 Jan 1980 and 31 Dec 2009 notified to 31 EUROCAT registers formed this
population-based case series. Denominator and maternal age data were provided by
EUROCAT.(EUROCAT, 2012a)
Cases of Hirschsprung’s disease were classified into three distinct groups: isolated cases, cases
with additional major structural anomalies or cases occurring with chromosomal anomalies or
genetic syndromes. Cases associated with structural anomalies directly related to Hirschsprung's
disease (e.g. intestinal obstruction or hypoplasia of the large intestine), were classified as
isolated.
Cases from multiple pregnancies were excluded from analysis due to potentially different
aetiologies (Glinianaia et al, 2008).
Statistical analysis
Total prevalence rates for Hirschsprung's disease in each register were calculated as the number
of cases (whether ending in fetal loss with gestational age> 20 weeks), termination of pregnancy
Page 9 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
9
for fetal anomaly, or live birth) per 10,000 live and stillbirths. 95% confidence intervals (CIs)
were derived from the binomial distribution.
Descriptive statistics were produced for: additional major congenital anomalies (including
chromosomal anomalies, genetic syndromes and structural anomalies), sex, pregnancy outcome
(classed as late miscarriage, stillbirth, termination of pregnancy for fetal anomaly or live birth)
and survival beyond one week of age (classed as yes or no). Figures for survival beyond one
week refer to live births only, of which 86% had known survival status.
Multilevel Poisson regression (with two levels) was performed to model total prevalence over
time. The number of cases per year (level 1) were nested within register (level 2) and modelled
with a random intercept (to better account for variation between registers), an offset equal to the
log of the total births, and year as a continuous predictor. Heterogeneity between registers was
tested by analysing the model’s change in deviance (using a chi square test on the estimated
difference in parameters) between the null model and the model incorporating the random
intercept. Similarly, the models were also refitted to include additional random effects to
examine inter-regional differences in trends over time.
Random intercept multilevel models were refitted to include maternal age (in years, categorised
as <20, 20-24, 25-29, 30-34 and ≥35) as well as year of delivery. The following registers had
>5% of their maternal age denominator data uncategorised: South Portugal, Saxony Anhalt,
Reunion, Thames Valley, Northern England and Valencia Region and so these registers were
excluded from this analysis on maternal age. Tuscany and Strasbourg did not have denominator
data from 1995 and 2006 respectively, so these years were removed from this analysis for these
two registers. There were a further 71 cases with missing maternal age data, which were also
excluded.
Multilevel model parameters were estimated using a random walk (Metropolis-Hastings)
Markov Chain Monte Carlo (MCMC) algorithm. Assuming diffuse uniform priors, the
Page 10 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
10
procedure was run for a burn-in sample of 5,000 observations, and an analysis sample of
1,000,000 thinned by 10 (numbers guided by Raftery-Lewis calculations) (Raftery and Lewis,
1992). Bayesian 95% Credible Intervals (CrIs), analogous to frequentist 95% CIs, were obtained
from the posterior distribution for each parameter. All models were checked for overdispersion
(by comparing model fit after the addition of another variation term) and trajectories for
parameters and variance were checked to ensure appropriate mixing.
Statistical analyses were performed using Stata version 12, including the runmlwin command.
P<0.05 was considered statistically significant.
Page 11 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
11
RESULTS
A total of 1,374 cases of Hirschsprung's disease were notified to the 31 EUROCAT registers. Of
these, 33 (2.4%) cases occurring in twin pregnancies and 19 (1.4%) occurring in pregnancies
with unknown number of fetuses were excluded from further analysis (figure 1). Hence, there
were 1,322 singleton cases among a population of 12,146,210 singleton total births between
1980 and 2009.
Additional anomalies
Of the 1,322 singleton cases, 146 (11.0%) occurred with a non-structural anomaly: fifteen
(1.1%) with genetic syndromes (including microdeletions) and 131 (9.9%) with chromosomal
anomalies (figure 1). The most common genetic syndromes were Smith-Lemli-Opitz and
Waardenburg syndrome and the majority (93.9%) of the cases associated with chromosomal
anomalies were Down syndrome (table 1)
Excluding cases with chromosomal anomalies or genetic syndromes, there were 1,176 cases
remaining (figure 1). Of these, 137 (11.6%) were associated with additional major structural
anomalies (table 1) and 1,039 (88.4%) were cases of isolated Hirschsprung's disease.
Sex distribution
There was a male predominance among all cases of Hirschsprung’s disease (73.5% vs 26.2%)
giving a male to female ratio of 2.8:1, which remained the same after excluding cases associated
with chromosomal anomalies or genetic syndromes. The sex ratio of males to females was
slightly higher (2.9: 1) in isolated cases.
Pregnancy outcome
In total, 1,313 (99.3%) of all 1,322 singleton cases resulted in a live birth, two (0.2%) occurred
in late miscarriages and seven (0.5%) cases resulted in termination of pregnancy for fetal
anomaly. Both miscarriages occurred in cases associated with other major structural anomalies.
The terminations of pregnancy were associated with chromosomal anomalies or genetic
Page 12 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
12
syndromes in three cases, major structural anomalies in two cases and isolated cases in two
cases.
Birth weight and gestational age
Of the 1,313 live born children, the median gestational age at delivery was 39 weeks (IQR: 38-
40), with gestational age missing in 77 (5.9%) cases. Of the live born cases, the mean birth
weight was 3276.5 grams (SD=650.7), with birth weight missing in 256 (19.5%). Of the term
cases (gestational age≥ 37 weeks, n=1103), the mean birth weight was 3389.3g (SD=540.6g)
and of the preterm cases (gestational age<37 weeks, n=125) the mean birth weight was 2278.3g
(SD=688.9g).
Total prevalence
Table 2 shows the number of cases and total prevalence of cases of Hirschsprung's disease by
register. Including all 1,322 singleton cases, the total prevalence was 1.08 (95% CI: 1.03, 1.15)
per 10,000 births for all registers combined. Total prevalence ranged from 2.78 (95% CI: 1.89,
3.94) in Malta to 0.07 (0.01, 0.24) per 10,000 total births in South Portugal (figure 2). There was
a significant difference in prevalence between registers (p<0.001)
Excluding cases associated with chromosomal anomalies or genetic syndromes, the total
prevalence was 0.97 (95% CI: 0.91, 1.03) per 10,000 births, and this varied significantly
between registers (p<0.001).
Trends in prevalence
There was a small but significant increase in Hirschsprung's disease prevalence over the study
period (RR= 1.01, 95% CrI: 1.00, 1.02; p=0.004), which ranged from a modelled 1.04 per
10,000 in 1980-1984 to 1.42 per 10,000 in 2005-2009. There was no evidence that trends over
time varied by register (p=0.203).
Excluding cases associated with chromosomal anomalies or genetic syndromes, there was still
evidence of increasing total prevalence over the study period (RR= 1.01, 95% CrI: 1.00, 1.02;
Page 13 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF
For Peer Review
13
p=0.006), which ranged from a modelled 0.93 per 10,000 in 1980-1984 to 1.26 per 10,000 in
2005-2009.
Maternal age distribution
There were 1,098 (83.1%) cases with available maternal age and corresponding maternal age
denominator data. The prevalence was greatest among mothers aged ≥35 but there was no
increased risk of Hirschsprung's disease in this age group compared to mothers aged 25-29
(RR=1.17, 95% CrI: 1.01, 1.35; p=0.355 ) (table 3). Compared to women aged 25-29, there was
no evidence of an association with maternal age in any other age group (table 3). Accounting for
maternal age, there was still a significant difference in prevalence between registers (p<0.001)
and there was still a statistically significant trend over time (RR= 1.01, 95% CrI 1.00, 1.02;
p=0.012).
After excluding cases associated with chromosomal anomalies or genetic syndromes, there were
974 cases. There was no evidence of an association between prevalence and maternal age in any
age group. There was still evidence of a significant difference in prevalence between registers
and a small increase in prevalence over time (RR=1.01, 95% CrI: 1.00, 1.02; p=0.012)
Diagnosis
Time of diagnosis was known in 803 (77.3%) isolated cases. A congenital anomaly was
antenatally detected in 11 (1.4% of 803) cases at a mean gestational age of 31 weeks (inter
quartile range: 22-33). Hirschsprung’s disease was diagnosed at birth in 161 (20.0%) cases, in
the first week in 354 (44.1%) cases, between one and four weeks in 116 (14.4%) cases, between
one and 12 months in 95 (11.8%) cases, after 12 months in 25 (3.1%) cases. The remaining 41
cases were postnatally diagnosed but at an unknown time.
One week survival
There were 1,135 (86.4%) live born cases with known one week survival and eight (0.7%) cases
died in the first week of life. Four of these were isolated cases, two had chromosomal anomalies
Page 14 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
14
(Down syndrome) and two had other structural anomalies (Prune Belly Sequence and hip
dislocation and/or dysplasia).
Page 15 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
15
DISCUSSION
This study is the largest to examine the epidemiology of Hirschsprung’s disease. Using data
from 31 European congenital anomaly registers over a period of 30 years, we found a total
prevalence of 1.08 per 10,000 births and a small but significant increase in Hirschsprung’s
disease prevalence over time. We also found a difference in prevalence by geographic
location and no evidence of an association between prevalence and maternal age.
The primary strength of this study is that it is based on data derived from established, high
quality, population-based congenital anomaly registers. Standard methods of identifying and
classifying cases across all registers and the use of multiple sources of notifications ensure
high case ascertainment. The health services in Europe are organised to deliver care to a
defined population, which allows contributing registers to maximise case ascertainment.
Additionally, this is one of very few studies to investigate prevalence of Hirschsprung’s
disease according to maternal age and to determine the relative risk of Hirschsprung’s disease
in young women and women of advanced maternal age.
We have used advanced methods of analysis to analyse the trends in Hirschsprung’s disease
prevalence over time and the association with maternal age. The multilevel methods utilised
provide more accurate standard error estimates for the nested data than classical approaches
and limit the potential for confounding due to registers contributing data from different time
points (Austin, 2001).
A further strength of the study is that we had detailed information on associated anomalies.
Thus we could investigate the epidemiology of Hirschsprung’s disease both including and
excluding cases with chromosomal anomalies or genetic syndromes which may have
different aetiologies.
Page 16 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
16
However this study also has some limitations. The increasing trend in prevalence could be
caused by improved ascertainment due to the registers becoming more established over the
study period or due to improvements in diagnosis and coding over time. Additionally
heterogeneity in prevalence between registers may be related to differences in ascertainment,
especially as some of the registers (such as Paris and Emilia Romagna) have been in
existence for almost 30 years whilst others have only been collecting data for 5-10 years.
While most registers include cases diagnosed by age one (and older in some registers,
including registers in the North of England and Vaud), several only include cases diagnosed
in the first month (e.g South Portugal register) or first week (e.g Emilia Romagna register) of
life. This may be a source of heterogeneity because Hirschsprung’s disease is not always
picked up in the neonatal period. However, trends and geographic variation in prevalence
may reflect true differences, perhaps related to differing exposures between regions.
Although we were able to adjust for maternal age, we did not have access to data on other
variables such as ethnicity, which may be associated with Hirschsprung’s disease prevalence
(Goldberg, 1984).
With few cases occurring in terminations of pregnancy, late miscarriage or stillbirth, it is not
too surprising that our total prevalence was not greater than the live birth prevalences of 1.63,
1.76 and 2.60 per 10,000 live births, reported by other studies (Best et al, 2012; Goldberg,
1984; Spouge and Baird, 1985). With Goldberg (1984) reporting a higher prevalence in non-
whites compared to whites, other factors such as ethnicity may account for some of the
variation between these studies.
This study found a small but significant increasing trend in the total birth prevalence of
Hirschsprung’s disease, which was similar to that reported in our previous study, set in the
North of England over a similar time period (1990-2008) (Best et al, 2012). However, this
trend should be interpreted with caution; although our large sample size enabled us to detect a
Page 17 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
17
very small, statistically significant increase in prevalence, this increase may not be of clinical
significance. Goldberg (1984) and Spouge and Baird (1985) found no evidence of trends over
time between the 1960s-80s in Baltimore and British Columbia, respectively. However, these
are smaller studies which may not have had the power to detect a small increase in
prevalence. Moreover, these are older studies performed outside of Europe and so the
population and environments may not be easily comparable to our study.
We found no evidence of an increased risk of Hirschsprung’s disease in cases born to women
aged over 35 when chromosomal anomalies and genetic syndromes were included or
excluded. This corresponds with Best et al’s (2012) findings, where the proportion of mothers
aged over 35 was not significantly greater in cases compared to the general population.
Goldberg (1984) found a significantly greater proportion of cases to mothers aged over 30
compared to the general population but examined only 33 cases, and Ryan et al (1992) found
no difference in proportions at all. Therefore, there is little evidence that increased maternal
age is a risk factor for Hirschsprung’s disease despite the anomaly having a known genetic
element. However, there is some evidence of an interaction with ethnicity, with Goldberg
identifying some association with increased maternal age in white women but not in non-
white women (Goldberg, 1984). This interaction may need to be further investigated before
maternal age is ruled out completely as a risk factor.
Page 18 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
18
REFERENCES
Amiel J, Sproat-Emison E, Garcia-Barcelo M, Lantieri F, Burzynski G, Borrego S, Pelet A,
Arnold S, Miao X, Griseri P, Brooks AS, Antinolo G, de Pontual L, Clement-Ziza M,
Munnich A, Kashuk C, West K, Wong KK, Lyonnet S, Chakravarti A, Tam PK,
Ceccherini I, Hofstra RM, Fernandez R, Hirschsprung Disease Consortium. 2008.
Hirschsprung disease, associated syndromes and genetics: a review. Journal of
Medical Genetics 45(1):1-14.
Austin PC. 2001. An introduction to multilevel regression models. Canadian Journal of
Public Health 92(2):150-154.
Badner JA, Sieber WK, Garver KL, Chakravarti A. 1990. A genetic study of Hirschsprung
disease. American Journal of Human Genetics 46(3):568-580.
Best KE, Glinianaia SV, Bythell M, Rankin J. 2012. Hirschsprung's disease in the North of
England: Prevalence, associated anomalies, and survival. Birth Defects Research
Part A: Clinical and Molecular Teratology 94(6):477-480.
EUROCAT. 2012a. http://www.eurocat-network.eu/. (Accessed January 2014)
EUROCAT. 2012b. http://www.eurocat-network.eu/aboutus/memberregistries.
(Accessed January 2014)
EUROCAT. 2012c. www.eurocat-network.eu/content/EUROCAT-Guide-1.3.pdf.
(Accessed January 2014)
Glinianaia SV, Rankin J, Wright C. 2008. Congenital anomalies in twins: a register-based
study. Human Reproduction 23(6):1306-1311.
Goldberg EL. 1984. An epidemiological study of Hirschsprung's disease. International
Journal of Epidemiology 13(4):479-485.
Greenlees R, Neville A, Addor MC, Amar E, Arriola L, Bakker M, Barisic I, Boyd PA,
Calzolari E, Doray B. 2011. Paper 6: EUROCAT member registries: organization
and activities. Birth Defects Research Part A: Clinical and Molecular Teratology
91(S1):S51-S100.
Martucciello G. 1997. Hirschsprung's disease as a neurochristopathy. Pediatric Surgery
International 12(1):2-10.
Moore SW. 2006. The contribution of associated congenital anomalies in understanding
Hirschsprung's disease. Pediatric Surgery International 22(4):305-315.
Puri P, Shinkai T. 2004. Pathogenesis of Hirschsprung's disease and its variants: recent
progress. Seminars in Pediatric Surgery 13(1):18-24.
Raftery AE, Lewis S. 1992. How many iterations in the Gibbs sampler. Bayesian Statistics
4(2):763-773.
Ryan ET, Ecker JL, Christakis NA, Folkman J. 1992. Hirschsprung's disease: associated
abnormalities and demography. Journal of Pediatric Surgery 27(1):76-81.
Spouge D, Baird PA. 1985. Hirschsprung disease in a large birth cohort. Teratology
32(2):171-177.
Page 19 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
Table 1: Frequencies of congenital anomalies that occurred in addition to Hirschsprung’s disease*
Chromosomal anomalies
and genetic syndromes,
Group & Subtype
N % of all cases
Chromosomal anomalies
45 X (Turner Syndrome)
Trisomy 2, Mosaicism
Trisomy 7
Trisomy 8 Mosaicism
Trisomy 21 (Down Syndrome)
Deletion of long arm chromosome 13
Other
131
1
1
1
1
123
1
3
9.9
0.1
0.1
0.1
0.1
9.3
0.1
0.2
Genetic Syndromes and Microdeletions
Di George Syndrome
Microdeletion 13
Adams Oliver Syndrome
Mowat Wilson Syndrome
Smith-Lemli-Opitz-Syndome
Marfan Syndrome
Waardenburg Syndrome
15
2
1
1
1
4
1
5
1.1
0.2
0.1
0.1
0.1
0.3
0.1
0.4
Total 146 11.0
Structural anomalies**,
Group & Subtype
N % of all structural
anomalies
Associations
Goldenhar
1
1
0.5
0.5
Sequences
Pierre Robin
Prune Belly
2
1
1
1.0
0.5
0.5
Nervous System 20 9.7
Eye 7 3.4
Congenital heart disease
Ventricular Septal Defect
Atrial Septal Defect
42
17
15
20.4
8.3
7.3
Respiratory System 7 3.4
Oro-facial clefts/palates 8 3.9
Digestive System
Duodenal atresia
Jejunoileal atresia
Ano-rectal anomaly
34
3
6
14
16.5
1.5
2.9
6.8
Abdominal wall defect 3 1.5
Urinary System
Hydronephrosis
Posterior urethral valve
32
15
4
15.5
7.3
1.9
Genital
Hypospadias
13
8
6.3
3.9
Limb
Hip dislocation/ dysplasia
Syndactyly
17
3
4
8.3
1.5
1.9
Musculo-skeletal 8 3.9
Other 12 5.8
Total 206 100.0
*Cases occurring in multiple pregnancies were excluded**Cases occurring with chromosomal anomalies, genetic
syndromes or microdeletions are excluded. Structural anomalies with n<3 not shown.
Page 20 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
Table 2: Total prevalence including and excluding cases associated with chromosomal anomalies or genetic syndromes
Register Years
contributed
Total
births Casesa
Prevalence
(95% CI) per
10,000 total
birthsa
Cases
excluding
non-
structural
anomaliesb
Prevalence
(95% CI) per
10,000 total
birthsb
Odense (Denmark) 1980-2009 159594 26 1.63 (1.06, 2.39) 20 1.25 (0.77, 1.94)
Paris (France) 1981-2009 977753 74 0.76 (0.59, 0.95) 69 0.71 (0.55, 0.89)
Tuscany (Italy) 1980-2009 595632 14 0.24 (0.13, 0.39) 13 0.22 (0.12, 0.37)
Dublin (Ireland) 1987-2009 659837 124 1.88 (1.56, 2.24) 102 1.55 (1.26, 1.88)
North Netherlands 1981-2009 479241 73 1.52 (1.19, 1.92) 65 1.36 (1.05, 1.73)
Emilia Romagna (Italy) 1981-2009 789425 30 0.38 (0.26, 0.54) 28 0.36 (0.24, 0.51)
Strasbourg (France) 1982-2007 335962 61 1.82 (1.39, 2.33) 53 1.58 (1.18, 2.06)
Vaud (Switzerland) 1989-2007 157993 25 1.58 (1.02, 2.34) 25 1.58 (1.02, 2.34)
Zagreb (Croatia) 1983-2009 168518 13 0.77 (0.41, 1.32) 13 0.77 (0.41, 1.32)
Malta 1986-2009 111677 31 2.78 (1.89, 3.94) 29 2.6 (1.74, 3.73)
South Portugal 1990-2009 301084 2 0.07 (0.01, 0.24) 2 0.07 (0.01, 0.24)
Antwerp (Belgium) 1990-2009 298827 68 2.28 (1.77, 2.89) 63 2.11 (1.62, 2.7)
Basque Country (Spain) 1990-2009 356578 54 1.51 (1.14, 1.98) 48 1.35 (0.99, 1.79)
Saxony Anhalt (Germany) 1987-2009 318575 21 0.66 (0.41, 1.01) 15 0.47 (0.26, 0.78)
Mainz (Germany) 1990-2009 69179 11 1.59 (0.79, 2.85) 10 1.45 (0.69, 2.66)
Styria (Austria) 1985-2009 296249 56 1.89 (1.43, 2.46) 51 1.72 (1.28, 2.26)
Cork & Kerry (Ireland) 1996-2008ф 99930 18 1.8 (1.07, 2.85) 15 1.50 (0.84, 2.48)
Wales 1998-2009 394394 87 2.21 (1.77, 2.72) 80 2.03 (1.61, 2.52)
Norway 1999-2008 587490 59 1 (0.77, 1.3) 54 0.92 (0.69, 1.2)
Ukraine 2005-2009 146055 12 0.82 (0.43, 1.44) 12 0.82 (0.43, 1.44)
Reunion (France) 2002-2009 117673 28 2.38 (1.58, 3.44) 25 2.13 (1.38, 3.14)
Wielkopolska (Poland) 1999-2009 399014 32 0.8 (0.55, 1.13) 28 0.7 (0.47, 1.01)
Thames Valley (UK) 1996-2009 231041 25 1.08 (0.70, 1.60) 22 1.04 (0.67, 1.55)
Wessex (UK) 1994-2009 429871 68 1.58 (1.23, 2.01) 55 1.28 (0.96, 1.67)
East Midlands & South
Yorkshire (UK)
1998-2009 770634 70 0.91 (0.71, 1.15) 62 0.81 (0.62, 1.03)
Northern England (UK) 2000-2009 314267 57 1.81 (1.37, 2.35) 52 1.66 (1.24, 2.17)
Hungary 1998-2009 1169857 67 0.57 (0.44, 0.73) 62 0.53 (0.41, 0.68)
South East Ireland 1997-2009 85801 11 1.28 (0.64, 2.29) 9 1.05 (0.48, 1.99)
Czech Republic 2000-2009 1029164 67 0.65 (0.51, 0.83) 61 0.59 (0.45, 0.76)
South West England (UK) 2005-2009 239840 25 1.04 (0.68, 1.54) 21 0.88 (0.54, 1.34)
Valencia Region (Spain) 2007 55055 13 2.36 (1.26, 4.04) 12 2.18 (1.13, 3.81)
Total 1980-2009 12146210 1,322 1.08 (1.03, 1.15) 1176 0.97 (0.91, 1.03)
a all singleton cases b all singleton cases excluding cases occurring with a chromosomal anomaly, genetic syndrome or microdeletion.
ф Cork and Kerry did not contribute data in 2007
Page 21 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
Table 3: Prevalence according to maternal age category*
Age All cases Excluding non-structural anomalies†
N (%) Prevalence
(95% CI) per
10,000
RR (95% CrI) P-
value
N (%) Prevalence
(95% CI) per
10,000
RR (95% CrI) P-
value
<20 45 (4.1) 0.96 (0.7, 1.29) 0.89 (0.67, 1.2) 0.445 41 (4.2) 0.88 (0.63, 1.19) 0.90 (0.67, 1.22) 0.508
20-24 200 (18.2) 1.05 (0.91, 1.21) 0.93 (0.80, 1.09) 0.380 181 (18.6) 0.95 (0.82, 1.1) 0.96 (0.82, 1.14) 0.666
25-29 340 (31.0) 0.97 (0.87, 1.08) 1.00 (Reference) - 319 (32.8) 0.91 (0.81, 1.02) 1.00 (Reference) -
30-34 317 (28.9) 0.99 (0.88, 1.11) 0.93 (0.79, 1.09) 0.363 279 (28.6) 0.87 (0.77, 0.98) 0.90 (0.76, 1.07) 0.226
35+ 196 (17.9) 1.17 (1.01, 1.35) 1.09 (0.91, 1.31) 0.355 154 (15.8) 0.92 (0.78, 1.08) 0.94 (0.78, 1.15) 0.563
Year - - 1.01 (1.00, 1.02) 0.012 - - 1.01 (1.00, 1.02) 0.012
*Cases occurring in multiple pregnancies were excluded. As stated in methods, several registers/years were excluded from this analysis.
†Excluding cases occurring with chromosomal anomalies, genetic syndromes or microdeletions
Page 22 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
Flowchart of cases included in the study
164x123mm (220 x 220 DPI)
Page 23 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF

For Peer Review
Total prevalence of Hirschsprung’s disease by register 164x123mm (220 x 220 DPI)
Page 24 of 23
John Wiley & Sons, Inc.
Birth Defects Research Part A: Clinical and Molecular Teratology
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
Ref: 20102204 D07-10 OTH UK IS.PDF