Herpes Zoster Oticus in Emergency Medicine

of 6
Transcript of Herpes Zoster Oticus in Emergency Medicine
-
7/31/2019 Herpes Zoster Oticus in Emergency Medicine
1/6
Herpes Zoster Oticus in Emergency
Medicine Overview of Herpes Zoster Oticus
Author: Christina Bloem, MD; Chief Editor: Steven C Dronen, MD, FAAEM more...
Updated: Mar 29, 2011
Overview of Herpes Zoster Oticus
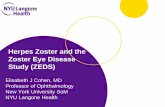
Herpes zoster oticus (HZ oticus) is a viral infection of the inner, middle, and external ear. HZ oticus manifests assevere otalgia and associated cutaneous vesicular eruption, usually of the external canal and pinna. When associated
with facial paralysis, the infection is called Ramsay Hunt syndrome. (See the image below.)
Herpes zoster oticus. Image courtesy of Manolette Roque, MD, Ophthalmic Consultants Philippines Co, EYE REPUBLIC OphthalmologyClinic.
Ramsay Hunt syndrome accounts for up to 12% of all facial paralyses and generally causes more severe symptoms
and has a worse prognosis than Bell palsy.[1, 2, 3]
Return-to-baseline neurologic function is predicted partially by
severity of paralysis. In several studies, only 10-22% of individuals with significant facial paralysis had complete
recovery. In one study, however, 66% of patients with incomplete paralysis had complete recovery.
An additional complication of herpes zoster viral infection is postherpetic neuralgia.
The incidence rates of HZ oticus in males and females are equal, and incidence increases significantly in patients
older than 60 years.
Pathophysiology of HZ Oticus
Reactivation of the varicella-zoster virus (VZV) along the distribution of the sensory nerves innervating the ear, whichusually includes the geniculate ganglion, is responsible for herpes zoster (HZ) oticus. Associated symptoms, such ashearing loss and vertigo, are thought to occur as a result of transmission of the virus via direct proximity of cranial
nerve (CN) VIII to CN VII at the cerebellopontine angle or via vasa vasorum that travel from CN VII to other nearby
cranial nerves.
Clinical Manifestations of HZ Oticus
Patient history
Medscape Reference
Reference
News
ReferenceEducation
MEDLINE
pes Zoster Oticus in Emergency Medicine http://emedicine.medscape.com/article/1952189-overview
6 05/05/2012 10:03
-
7/31/2019 Herpes Zoster Oticus in Emergency Medicine
2/6
Typically, patients present with severe otalgia. Complaints include the following:
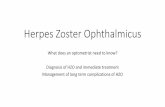
Painful, burning blisters in and around the ear, on the face, in the mouth, and/or on the tongue (see the imagebelow)
Herpes zoster oticus. Image courtesy of Manolette Roque, MD, Ophthalmic Consultants Philippines Co, EYE REPUBLICOphthalmology Clinic.
Vertigo, nausea, vomitingHearing loss, hyperacusis, tinnitusEye pain, lacrimation
Onset of pain may precede the rash by several hours or days. Also, in patients with Ramsay Hunt syndrome, vesiclesmay appear before, during, or after facial palsy (zoster sine herpete). When asked, patients may recall a distant history,
perhaps in childhood, of chickenpox (varicella). A minority of patients (< 10%) give a history of previous herpes zosterviral infection.
Physical examination
Physical examination shows a vesicular exanthem, usually of the external auditory canal, concha, and pinna. The rashalso may appear on postauricular skin, lateral nasal wall, soft palate, and anterolateral tongue.
Vertigo and sensorineural hearing loss may be noted, and paralysis of the facial nerve, mimicking Bell palsy, may be
present. Complete loss of the ability to wrinkle the ipsilateral brow distinguishes a peripheral lesion of cranial nerve VIIfrom a central lesion of the same nerve, which spares the forehead.
Associated findings include the following:
Dysgeusia (alteration in taste)Inability to fully close the ipsilateral eye, which may lead to the occasional presentation of drying and irritation ofthe cornea.
Complications
Complications of HZ oticus may include the following[4, 5, 6] :
Postherpetic neuralgia
Residual paralysis
Rarely, herpes zoster encephalitis[5]
Etiology of HZ Oticus
Herpes zoster (HZ) oticus is caused by the reactivation of latent varicella-zoster virus (VZV) that has remained dormant
within sensory ganglia (commonly the geniculate ganglion) of the facial nerve. Individuals with decreased cell-mediatedimmunity resulting from carcinoma, radiation therapy, chemotherapy, or HIV infection are at greater risk for reactivationof latent VZV. Physical stress and emotional stress often are cited as precipitating factors.
Differential Diagnosis
The differential diagnosis of herpes zoster (HZ) oticus includes the following:
Bell Palsy
Headache, ClusterHeadache, Migraine
Headache, TensionHerpes ZosterOtitis ExternaOtitis Media
pes Zoster Oticus in Emergency Medicine http://emedicine.medscape.com/article/1952189-overview
6 05/05/2012 10:03
-
7/31/2019 Herpes Zoster Oticus in Emergency Medicine
3/6
Stroke, HemorrhagicStroke, Ischemic
Isolated facial nerve trauma also needs to be considered.
Laboratory Studies
Herpes zoster oticus (HZ oticus) is primarily a clinical diagnosis in the ED.
Prior to initiating treatment with acyclovir, consider a baseline set of the following laboratory studies:
Blood urea nitrogen (BUN)
CreatinineBlood cell countsElectrolytes
Imaging Studies
If diagnosis of Ramsay Hunt syndrome is not established by physical examination alone, consider a head CT scan to
investigate other etiologies of facial paralysis.
Treatment of HZ OticusUntil recently, therapy for herpes zoster (HZ) oticus has been generally supportive, including warm compresses,narcotic analgesics, and antibiotics for a secondary bacterial infection.
Antiviral agents
Antiviral agents clearly play a role in limiting the severity and duration of symptoms if given early in the course of theillness. Early administration (< 72 h) of acyclovir showed an increased rate of facial nerve function recovery andprevented further nerve degeneration. Furthermore, use of antivirals has been shown to decrease the incidence and
severity of postherpetic neuralgia.[7, 8, 9, 4]
Evidence is accumulating that varicella-zoster virus (VZV) may be responsible for many cases of Bell palsy that go
unrecognized because of a lack of cutaneous f indings (zoster sine herpete). Accordingly, the clinician should entertain
more liberal use of antivirals such as acyclovir, valacyclovir, and famciclovir.[2, 3]
Studies have shown no difference
between oral and IV acyclovir in immunocompetent patients with facial nerve paralysis.[10]
Corticosteroids
Systemic corticosteroids are used to relieve acute pain, decrease vertigo, and limit the occurrence of postherpetic
neuralgia. The prevailing wisdom states that treatment with acyclovir plus prednisone has more effective return to facialnerve function and prevention of nerve degeneration than treatment with prednisone alone; however, a recent review
uncovered very little data to support or negate this theory.[7]
Patients treated with acyclovir plus prednisone had betteroutcomes (time to healing of rash, time to cessation of acute neuritis, time to return to usual activity and sleep, and
time to cessation of analgesics) than those treated with either prednisone or acyclovir alone.[11]
No evidence indicates that use of corticosteroids prevents development of postherpetic neuralgia.[8, 9]
Furthermore,
evidence proving benefit attributed specifically to steroids is still limited, with one review showing no randomizedcontrolled trials supporting use of steroids as an adjuvant to antiviral medications in the treatment of Ramsay Hunt
syndrome.[12]
Treatment in HIV patients
For treatment of herpes zoster in patients with HIV, inpatient parenteral regimens should be reserved for those withsevere immunosuppression, trigeminal nerve involvement, ocular lesions, or multidermatomal involvement. Treatment
of VZV is the same for both HIV-seronegative and seropositive patients. For acyclovir-resistant VZV, IV foscarnet isan appropriate alternative therapy (famciclovir and valacyclovir are not effective against acyclovir-resistant VZV). For
outpatient regimens, famciclovir or valacyclovir for 7-10 days is recommended (both have the advantage of easierdosing regimens). Routine use of steroids is discouraged secondary to its immunosuppressive effects.
[13]
Treatment in other situations
Treatment of pregnant women with VZV is the same as that of nonpregnant women.
pes Zoster Oticus in Emergency Medicine http://emedicine.medscape.com/article/1952189-overview
6 05/05/2012 10:03
-
7/31/2019 Herpes Zoster Oticus in Emergency Medicine
4/6
When secondary impetigo is present, a suitable antistaphylococcal antibiotic should be prescribed.
Cyclic antidepressants, anticonvulsants, opioids, and topical analgesics are sometimes used in the treatment of
postherpetic neuralgia.[4] These agents are more appropriately started by a pain management specialist in an
outpatient setting.
Prevention of herpes zoster by vaccination is recommended for all persons older than 60 years, even if they have hadchickenpox or zoster in the past. This age group suffers significant morbidity from zoster and may, therefore, benefit
from the vaccine. Contraindications to vaccine administration include age younger than 60 years, current use of
antivirals, pregnancy, and certain immunosuppressive conditions.
[14]
Ensure that the patient has adequate and timely outpatient follow-up for management of HZ oticus.
Emergency department care
Adequate analgesia is important for individuals with significant pain from herpes zoster. Nausea and vomiting may
require ED treatment. Complications, such as corneal irritation or secondary bacterial infection of the vesicles, shouldbe managed with routine therapies. Involvement of more than one dermatome is atypical and should prompt thesearch for possible immunoincompetence.
Consider admission for any of the following situations:
Severe symptoms
Involvement of multiple (>2) dermatomesImmunocompromise
Consultations
Consider an ophthalmologic consultation if corneal involvement with vesicles is noted, and consider a neurologicconsultation if the etiology of the facial paralysis is unclear. Consultation with an ear, nose, and throat (ENT) specialistmay be appropriate.
Prognosis
Prolonged or permanent facial paralysis is possible. Most patients with partial paralysis fully recover; many with severe
symptoms are left with partial def icits.
Patient Education
Instruct patients how to tape eyes shut if lid paralysis is present.
Contributor Information and DisclosuresAuthorChristina Bloem, MD Assistant Clinical Professor of Emergency Medicine, George Washington University
Disclosure: Nothing to disclose.
Coauthor(s)Maria M Diaz, MD Staff Physician, Department of Emergency Medicine, Memorial Hospital
Maria M Diaz, MD is a member of the following medical societies: American College of Emergency Physicians,Emergency Medicine Residents Association, and Phi Beta Kappa
Disclosure: Nothing to disclose.
Christopher I Doty, MD, FACEP, FAAEM Assistant Professor of Emergency Medicine, Residency ProgramDirector, Department of Emergency Medicine, Kings County Hospital Center, State University of New YorkDownstate Medical Center
Christopher I Doty, MD, FACEP, FAAEM is a member of the following medical societies: American Academy ofEmergency Medicine, American College of Emergency Physicians, American Medical Association, Council of
Emergency Medicine Residency Directors, and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
pes Zoster Oticus in Emergency Medicine http://emedicine.medscape.com/article/1952189-overview
6 05/05/2012 10:03
-
7/31/2019 Herpes Zoster Oticus in Emergency Medicine
5/6
Jon Mark Hirshon, MD, MPH Associate Professor, Department of Emergency Medicine, University of MarylandSchool of Medicine
Jon Mark Hirshon, MD, MPH is a member of the following medical societies: Alpha Omega Alpha, AmericanAcademy of Emergency Medicine, American College of Emergency Physicians, American Public Health
Association, and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Specialty Editor BoardRobin R Hemphill, MD, MPH Associate Professor, Director, Quality and Safety, Department of EmergencyMedicine, Emory University
Robin R Hemphill, MD, MPH is a member of the following medical societies: American College of Emergency
Physicians and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
Francisco Talavera, PharmD, PhD Adjunct Assistant Professor, University of Nebraska Medical Center Collegeof Pharmacy; Senior Pharmacy Editor, eMedicine
Disclosure: eMedicine Salary Employment
Eric L Weiss, MD, DTM&H Director of Stanford Travel Medicine, Medical Director of Stanford Lifeflight, AssistantProfessor, Departments of Emergency Medicine and Infectious Diseases, Stanford University School of Medicine
Eric L Weiss, MD, DTM&H is a member of the following medical societies: American College of Emergency
Physicians, American College of Occupational and Environmental Medicine, American Medical Association,American Society of Tropical Medicine and Hygiene, Physicians for Social Responsibility, Southeastern SurgicalCongress, Southern Association for Oncology, Southern Clinical Neurological Society, and Wilderness Medical
Society
Disclosure: Nothing to disclose.
Chief EditorSteven C Dronen, MD, FAAEM Chair, Department of Emergency Medicine, LeConte Medical Center
Steven C Dronen, MD, FAAEM is a member of the following medical societies: American Academy of EmergencyMedicine and Society for Academic Emergency Medicine
Disclosure: Nothing to disclose.
References
Bauer CA, Coker NJ. Update on facial nerve disorders. Otolaryngol Clin North Am. Jun 1996;29(3):445-54.
[Medline].
1.
Murakami S, Hato N, Horiuchi J, Honda N, Gyo K, Yanagihara N. Treatment of Ramsay Hunt syndrome with
acyclovir-prednisone: significance of early diagnosis and treatment. Ann Neurol. Mar 1997;41(3):353-7.[Medline].
2.
Sweeney CJ, Gilden DH. Ramsay Hunt syndrome. J Neurol Neurosurg Psychiatry. Aug 2001;71(2):149-54.
[Medline]. [Full Text].
3.
Pavan-Langston D. Herpes zoster antivirals and pain management. Ophthalmology. Feb 2008;115(2
Suppl):S13-20. [Medline].
4.
Eskiizmir G, Uz U, Taskiran E, Unl H. Herpes zoster oticus associated with varicella zoster virus encephalitis.Laryngoscope. Apr 2009;119(4):628-30. [Medline].
5.
Adour KK. Otological complications of herpes zoster. Ann Neurol. 1994;35 Suppl:S62-4. [Medline].6.
Uscategui T, Dore C, Chamberlain IJ, Burton MJ. Antiviral therapy for Ramsay Hunt syndrome (herpeszoster oticus with facial palsy) in adults. Cochrane Database Syst Rev. Oct 8 2008;CD006851. [Medline].
7.
Whitley RJ, Weiss H, Gnann JW Jr, Tyring S, Mertz GJ, Pappas PG, et al. Acyclovir with and withoutprednisone for the treatment of herpes zoster. A randomized, placebo-controlled trial. The National Institute of
Allergy and Infectious Diseases Collaborative Antiviral Study Group. Ann Intern Med. Sep 1
8.
pes Zoster Oticus in Emergency Medicine http://emedicine.medscape.com/article/1952189-overview
6 05/05/2012 10:03
-
7/31/2019 Herpes Zoster Oticus in Emergency Medicine
6/6
Medscape Reference 2011 WebMD, LLC
1996;125(5):376-83. [Medline].
Wood MJ, Johnson RW, McKendrick MW, Taylor J, Mandal BK, Crooks J. A randomized trial of acyclovir for 7days or 21 days with and without prednisolone for treatment of acute herpes zoster. N Engl J Med. Mar 31
1994;330(13):896-900. [Medline].
9.
Furuta Y, Ohtani F, Mesuda Y, Fukuda S, Inuyama Y. Early diagnosis of zoster sine herpete and antiviraltherapy for the treatment of facial palsy. Neurology. Sep 12 2000;55(5):708-10. [Medline].
10.
Murakami S, Honda N, Mizobuchi M, Nakashiro Y, Hato N, Gyo K. Rapid diagnosis of varicella zoster virus
infection in acute facial palsy. Neurology. Oct 1998;51(4):1202-5. [Medline].
11.
Uscategui T, Doree C, Chamberlain IJ, Burton MJ. Corticosteroids as adjuvant to antiviral treatment in
Ramsay Hunt syndrome (herpes zoster oticus with facial palsy) in adults. Cochrane Database Syst Rev. Jul
16 2008;CD006852. [Medline].
12.
Benson CA, Kaplan JE, Masur H, Pau A, Holmes KK. Treating opportunistic infections among HIV-infected
adults and adolescents: recommendations from CDC, the National Institutes of Health, and the HIV MedicineAssociation/Infectious Diseases Society of America. MMWR Recomm Rep. Dec 17 2004;53:1-112.
[Medline].
13.
Harpaz R, Ortega-Sanchez IR, Seward JF. Prevention of herpes zoster: recommendations of the Advisory
Committee on Immunization Practices (ACIP). MMWR Recomm Rep. Jun 6 2008;57:1-30; quiz CE2-4.
[Medline].
14.
pes Zoster Oticus in Emergency Medicine http://emedicine.medscape.com/article/1952189-overview