Herpes in a Newborn
19
Morning Report Leah Farley, PGY-2 10/25/2013
-
Upload
emily-eresuma -
Category
Documents
-
view
217 -
download
0
Transcript of Herpes in a Newborn

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 1/19
Morning Report
Leah Farley, PGY-2
10/25/2013

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 2/19
Case
•7 day old female transferred from an OSH for
respiratory distress
•Birth History Uncomplicated pregnancy with normal prenatal
ultrasound
Born at 38 weeks via NSVD
Mom was GBS positive, other prenatal labs
reassuring
Infant observed for 48 hours in nursery and then
discharged home with parents

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 3/19
•About 12 hours of being home she had anepisode of apnea associated with emesis that
resolved with stimulation
•An hour later parents went to feed her but she
seemed limp and she had another period of
apnea
•She was stimulated and started breathing,
however shortly afterward had another episodeof apnea
•911 called and she was admitted to OSH

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 4/19
Hospital Course
•Developed oxygen need on hospital day 2
•Blood cultures drawn and started on amp/gent
•Worsening hypoxia, respiratory distress and
continued apneic episodes so she was started
on HFNC
•LifeFlight was called for transport
Noted significant respiratory distress requiringintubation
Hypotensive requiring fluid bolus and Dopamine

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 5/19
History
•FH:Paternal relatives with history of heart murmur.
Dad and older half-brother with OSA 2/2
hypertrophied tonsils and adenoids.Mom and older half-sister healthy
Dad with schizophrenia
•SH: Lives in UT with both parents. 2 dogs at
home. Mom and Dad smoke outside.

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 6/19
Physical Exam
Temp 35.5-36.2, P 150s-130s RR 32 on vent, BP 60s/30s, sats 92% on 70%
FiO2, Weight 2.7 kg (2%ile)
GENERAL: Sedated, intubated, non-irritable.
EYES: PERRL, conjunctivae clear, sclerae nonicteric,
HENT/MOUTH: NC/AT, AFSF, orally intubated MMM,
LYMPH: Neck supple, no LAD.
LUNGS: coarse bilaterally, no increased WOB, good aeration, no adventitious
sounds, not breathing over the vent.
CV: RRR, no M/R/G, nl perfusion and pulses.
ABD: Soft, ND, liver edge palpable, nl BS, no masses
GU: Nl external genitalia, nl Tanner stage for age, Foley catheter in place.BACK: Unable to examine
MSK/EXTREMITIES: No C/C/E. No e/o joint swelling or erythema.
SKIN: Pale. No rashes, jaundice, cyanosis.
NEURO: Somewhat hypotonic. Does awaken slightly and move head.

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 7/19
Differential Diagnosis?
7 day old female with respiratory
failure and hypotension.

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 8/19
Differential Diagnosis
ID Pertussis
RSV
Enterovirus
Sepsis GBS
E. coli
Listeria
Enterococcus
HSV
TORCH
Pneumonia Chlamydia
GBS
Aspiration
CV HLHS
Aortic coarctation
Truncus arteriosis
TAPVR
Transposition of the
great arteries
Pulmonic
atresia/stenosis
Tricuspid atresia Aortic stenosis
Tetralogy of Fallot
DILV
FEN/GI TE fistula
GER
Viral hepatitis
Neuro Seizures
Pulm RDS
Pulmonary
hemorrhage
Other NAT
DIC

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 9/19
Labs/Work-up
•CMP - BUN 3, Cr 0.29, Albumin 1.4, Bilirubin
4.3, Alk. Phos. 56, ALT 100, AST 260
•UA – 1+ glucose, neg LE, nitrite, ketone,
protein, Hgb •PTT - 36 PT/INR: 17.2/1.4 Fibrinogen: 165
•Serum HSV PCR – pos
•CSF HSV PCR –
pos •Tracheal aspirate – HSV pos
•Conjunctival swab – HSV pos
•

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 10/19

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 11/19
Neonatal HSV - Epidemiology
•Incidence 1 in 3,000 to 1 in 20,000 live births
•Risk greater with primary infection
Esp when acquired close to delivery
•Transmission most commonly direct contact with infected
vaginal secretionsIncreased risk with longer ROM
•Transmission can also occur in utero or post-natally
•3 types
Skin, Eyes, Mouth ~45% CNS disease ~33%
Disseminated ~25%

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 12/19
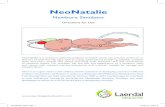
Skin, Eye, Mouth HSV
•Present ~10-12 days of life
•High rates of progression to CNS or
disseminated if not treated
•Clustering vesicular lesions with erythematous
base
•Eye infection usually asymptomatic but may
have watering, crying from eye pain,conjunctival erythema

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 13/19
aapredbook.aappublications.org

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 14/19
CNS HSV
•2nd-3rd week of life
•Presentation: Seizures, lethargy, irritability,
tremors, poor feeding, temp instability, full
anterior fontanelle, DIC, apnea, shock •Diagnosis: CNS normal or with mononuclear
cell pleiocytosis and elevated protein
60-70% will have skin lesions

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 15/19
Disseminated HSV
•Usually present in 1st week of life
•Can involve: Adrenals, CNS, eye, liver, lung,
mouth and skin
60-75% have CNS involvement Skin vesicles are usually late finding and 20% do not
have any skin manifestations
Serious complications – severe coagulopathy, liver
dysfunction, pulmonary involvement
•Mortality >80% if untreated

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 16/19
Diagnosis
HSV PCR on blood, CSF and specimen
from skin vesicle
Viral Culture
Swab specimens from mouth, nasopharynx,conjunctiva, anus
Specimens from skin vesicles and CSF
Most cultures will grow within 5 days
Whole blood measurement of ALT

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 17/19
Treatment
PreventionC-section for women with lesions resembling HSV
Avoid scalp monitors in women with HSV lesions
High dose Acyclovir (60 mg/kg/day div q8hrs)
for at least 21 days (14 days for SEM)
Ocular involvement – topical 1% trifluridine,
0.1% iododeoxyuridine or 3% vidarabine
Suppressive therapy: 6 months of oralacyclovir 3,000 mg/m2
Improves neurologic outcomes in CNS disease
Prevents skin recurrences in all classifications

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 18/19
Outcomes
Mortality29% for Disseminated HSV
4% for CNS HSV
Percent of survivors with normal neurologicdevelopment
98% for SEM
83% for disseminated
31% for CNS

7/27/2019 Herpes in a Newborn
http://slidepdf.com/reader/full/herpes-in-a-newborn 19/19
References
Thompson, C and R Whitley. “Neonatal Herpes
Simplex Virus: Where are We Now?” Advances
in Experimental Medicine and Biology. 2011; 697: 221-230.
Robinson, JL, Vaudry, WL, Forgie, SE, et al. “Prevention,
recognition and management of neonatal HSV infections.”Expert review of anti-infective therapy. 2012; 10(6): 675-685.
Uptodate. “Neonatal Herpes Simplex Virus Infection.”
AAP RedBook