Heroes & Saints: Issue 1 - June 2012
16
HEROES SAINTS WELCOME from the Medical Director | STEMI TRANSPORT | Trauma Talk NEWS FOR EMS TEAMS AT SAINT ALPHONSUS ISSUE 1 | JUNE 2012
-
Upload
saint-alphonsus-heroes-saints -
Category
Documents
-
view
221 -
download
0
description
News for EMS teams at Saint Alphonsus
Transcript of Heroes & Saints: Issue 1 - June 2012

HEROES SAINTS
WELCOME from the Medical Director | STEMI TRANSPORT | Trauma Talk
News For eMs TeaMs aT saiNT alphoNsus
ISSuE 1 | JuNE 2012

Want to share your story? [email protected]
Saint alphonSuS | emS newSletter
LETTER FROM THE EdITOR
Etymology of Heroes - Coined in English 1387, during the time of King Arthur’s round table, the word hero comes
from the Ancient Greek. “Hero, warrior”, literally “protector” or “defender”. It is also thought to be a cognate of the
Latin verb servo (original meaning: to preserve whole) and of the Avestan verb haurvaiti (to keep vigil over).
Heroes and Saints is a publication designed to
promote education, enhance dialogue, stimulate
discussion, and celebrate the sacred work you
do. We appreciate the stressful and immediate
tasks EMS providers face when they get the
call to respond to a need for urgent help.
Without your 24/7 dedication, training, and
commitment there would no doubt be more
fatalities – and the loss of significant quality
of life for many.
You don’t get to choose where you go, or
what you’ll find when you get there, but you
go hoping for the best, and prepared for the
worst. Those you serve hope they never have
to see you, but are incalculably grateful when
you arrive on the scene. You’ve experienced
horrors most can’t imagine, and know that
when tomorrow comes, you may not have seen
the worst. You are an extraordinary group of
people. Like our title suggests, you are “Heroes
and Saints.”
When I researched the background of
“Heroes” it seemed clear that in our present
day, “Heroes” and “Saints” have a lot in
common. It’s also evident that you need both
“Heroes and Saints” to save a life, offer hope,
and speed healing for those in need. Thus, the
title of this publication emerged to represent
our teamwork and our passion to serve
our communities.
The Editorial Board for this publication
includes our Trauma Surgeons, Medical
Directors from Idaho Emergency Physicians,
and other physicians, providers and staff who
oversee our most critical services. We want
this publication to be a dialogue, and a way to
provide feedback from our staff to yours.
I’ve truly enjoyed being out in the field
meeting so many of you, and appreciate the
feedback and orientation to the various stations
in Ada and Canyon County. Next month I plan
to head toward Ontario and Baker City to start
meeting EMS providers across our region. I
hope all of you felt appreciated and honored
during National EMS Week May 20 – 26.
Don’t miss the photo collage you’ll see on the
pages inside that represent honors bestowed on
your EMS brothers and sisters, as well as a few
photos I took while visiting various stations.
Saint Alphonsus Health System would
like to thank all EMS personnel for their
commitment to enhance the health and quality
of life of those we serve. YOU help make the
Critical Difference.
Welcome to the inaugural edition of the
“HEROES ANd SAINTS”
AIMEE STEIN
sIsTEr bETH MuLvANEy
Emergency & Trauma services relationship Manager & Editor
“YOU help make the
CritiCal DifferenCe.”
“Heroes.” “saints.” They have a lot in common.
When the Catholic Church names someone a saint, it is official recognition that during the person’s lifetime, he or she was outstanding in the way they responded to God’s love and demonstrated it to others. saints respond to needs. saints overcome all kinds of obstacles to make good things happen. saints often put other people’s hopes ahead of their own.
Yes, our present day emergency medical responder “Heroes” and the “saints” as described above, have a lot in common.
reflections from

June 2012 3
sarmc.org
John Fogg Sr. opened Ada-Boi Ambulance
in 1980 with four Cadillac coach ambulances.
Of the four, he kept and refurbished this 1970
Superior Coach to continue the memory.
John stated with a chuckle, “I wish we still
used these rigs. They ride like a Cadillac
Limousine where today’s rigs ride like
dump trucks.”
HIgHLIgHTS
2 LETTEr froM THE EDITor
3 HIGHLIGHTs 4 MEDICAL
DIrECTor GrEETInG
5 CArDIAC CArE
6 TrAuMA TALK
8 LooKInG AT us
12 nEuro/sTroKE
14 EAGLE Er
15 AWArDs & rECoGnITIon
16 MAp of LoCATIons
STROkE CASE REvIEW 3rd Wed. of every month 7am-9am Coughlin Conference room 2
TRAuMA ROuNdS 7am-8am Coughlin Conference room 2 June 13 & 27 July 11 & 25 August 8, 22, 29 september 12 & 26
EMS ROOFTOP BBQ september 27 3pm-7pm
uPCOMINg EvENTS
EdITORIAL BOARd
ABOuT THE COvER
AIMEE STEIN emergency & trauma Services relationship manager & editor
kRISTEN MICHELETTI Communications Director & editor
dR. BILLy MORgAN trauma medical Director
NANCy TAyLOR aprn-np/CnS hospitalist Cardiac Care
SISTER BETH MuLvANEy mission education
dR. BEN CORNETT iep/ada County medical Director
dR. kARI PETERSON iep/Canyon County medical Director
dR. EdWARd MCEACHERN iep executive Director/CeO
dR. ERIC ELLIOTT iep/eagle er medical Director
NICHOLE WHITENER mSn, Cnrn, ne-BC neuro/Stroke Director
JANE SPENCER CnS neuro institute
JANA PERRy rn, mSn trauma /General Surgery Director
RICH TRuMP pa-C trauma
ALISHA HAvENS Saint alphonsus nampa
LAuRA HuggINS Saint alphonsus Baker City
LEANNA BENTz Saint alphonsus Ontario
TEd RyAN SarmC emergency Department Director
PAT BERgEy rn, BSn
SNOW THANk yOu“Snowboarding with Jeff ” is the true account
of an adventure on Bogus Basin that goes
wrong. Go online and watch the video to see
how Jeff thanks Saint Alphonsus Eagle Health
Plaza Emergency Room for their great work!
http://vimeo.com/37383291
Canyo
n C
ounty
Para
med
ic

Want to share your story? [email protected]
Saint alphonSuS | emS newSletter
MEdICAL dIRECTOR gREETINg
Idaho is beginning to make great stirrings
in the area of a Trauma System and its
development. As the Southwestern Idaho
Trauma Center, Saint Alphonsus Regional
Medical Center is combining forces with
Eastern Idaho Regional Medical Center in
Idaho Falls, the Idaho Medical Association,
and the Idaho Hospital Association to
explore, in conjunction with the State EMS
Director and the Department of Health and
Welfare, the options that would best suit the
formation of a statewide Trauma System
for Idaho. From the EMS standpoint, it is
important that each of you be able to voice
your opinions on this matter. No system can
exist in a vacuum. We need your input and
your support to accomplish this for Idaho and
its many geographically distanced communities
so that each Idaho citizen can receive the same
excellent Trauma care. You will be hearing
more about this in the future, so for now, this
is just an opening statement on this subject.
Each of you works incredibly hard and
often, we, as the clinicians accepting your
patient’s, fail to remember the environment
that you frequently find yourselves working
in on a daily basis. I would like to say that I
appreciate and value each of you and the daily
sacrifices you make, the enormous educational
piece that you must accomplish and, the
professionalism and dedication you exhibit
with each patient encounter. Thank you to
each and every one of you.
HELLO ANd WELCOME to my first installment in the “EMs newsletter.”
bILL MORgAN, MD
Trauma Medical Director
“We neeD YOUr
inpUt anD
YOUr SUppOrt....”
Meet the region’s only Level 2 Trauma Center Team
top: mD trauma and General Surgery: Daele Strawn, mD, Steven Casos, mD, harry Stinger, mD, George munayirji, mD
Bottom: rhoda lynch, pa-C, richard trump, pa-C, Jana perry, rn, mSn trauma /General Surgery Director

June 2012 5
sarmc.org
Activation of Emergency Medical Services
(EMS) in the care of patients experiencing an
ST elevation myocardial infarction (STEMI) is
critical to early identification of this condition,
as well as effective treatment. In an article
published in Circulation in 2011, Mathews et al.
reported on an observational study of greater
than 37,000 patients suffering from a STEMI
using the National Cardiovascular Registry
data between January 2007 and 2009 where
they looked at patient factors related to EMS
transport versus self-transport. They found
that EMS transport was used only 60% of the
time. Our data shows that we have been closer
to 70% in the past 6 months.
Calling EMS has been shown to decrease
time to treatment and reduces ischemic time.
The long used phrase of “time is muscle”
really is true. The sooner perfusion to the
myocardium is restored, the better the patient
outcome. So who are the patients that call
EMS? Those characteristics identified by the
review of patients in this article revealed those
patients who were older were more likely to call
EMS. In addition, those people living farther
from the hospital were more likely to call. The
last group that seemed more likely to call were
those who were more unstable with greater
hemodynamic compromise. What didn’t
appear to be related to likelihood to call were
race, income, or education level.
How do we get more than 60% of people
to call EMS when they are having symptoms
of a heart attack? The most effective way
to get anyone to change a behavior is by
education. Community programs that teach
the importance of early heart attack care are
essential to changing this statistic. Working
together, we can get the word out and help the
community understand fully the benefits they
reap when they activate EMS.
uSE OF EMS FOR STEMI TRANSPORT
“the SOOner
perfUSiOn
tO the
mYOCarDiUm
iS reStOreD,
the Better
the patient
OUtCOme.”
CARdIAC CARE
Canyo
n C
ounty
Para
med
ics
| B
rush
C. &
Jess
e C
.
nAnCY TAyLORaprn-np/CnS
hospitalist Cardiac Care

Want to share your story? [email protected]
Saint alphonSuS | emS newSletter
Level 3
+ Death of same car occupant
+ Extrication time >20 minutes
+ fall 2X patient’s height
+ Auto vs. bike or Auto vs. pedestrian
+ Motorcycle/ATV/snowmobile/ jet ski “crashes”
+ Horse ejection or rollover
+ >12” intrusion into occupant space or vehicle
+ “star” any window shield
+ rollover
+ broken/bent steering wheel
+ Assault with change in level of consciousness
+ Amputation of one or more digits
+ second or third degree burns <10-20%
Level 2
+ GCs 9 to 13
+ Chest tube in place
+ pelvic fracture (suspected)
+ Two obvious long bone fractures (femur/humerus)
+ flail Chest
+ near drowning
+ Cervical fracture
+ Ejection from an enclosed vehicle
+ burns >20% or involving face, airway, hands, feet, or genitalia
Level 1
+ bp < 90mmHg, or respiratory rate >24, Tachycardia >120 at any time in adult trauma patients
+ Age specific hypotension or tachycardia in children
• <70 mmHg + 2 X age
• Hr >200 or < 60
+ respiratory compromise/obstruction
+ Intubation
+ patients receiving blood to maintain vital signs
+ GCs <8 with mechanism attributed to trauma
+ Major limb amputation
+ Trauma arrest
+ pregnancy >20 weeks gestation with vaginal discharge or bleeding or abdominal pain that also meet a mechanism attributed to trauma.
+ Hanging with loss of consciousness or any neurological deficits
+ penetrating injury to abdomen, head, neck, chest or proximal limbs including knee and elbow.
+ spinal cord injury with neurologic abnormality
TRAuMA TALk
standardizing Trauma Triage
SAINT AL’S THREE LEvELS OF TRIAgE
We encourage the EMS agencies locally and
throughout the region to utilize this trauma
triage criteria when transporting a patient to
our facility. This mobilizes all the appropriate
resources for an injured patient to the ER.
The Trauma Service suggests presenting the
criteria to your supervising physicians for
consideration to add to your local protocols
and when you call in you can give a level
assignment with your patient history and
our access center mobilizes the in house
resources. It would be appropriate to give
strong consideration to air lifting patients from
remote areas from the Trauma Center if they
meet a level 2 criteria or greater. Please never
hesitate to contact the Trauma Center for any
questions or concerns at 367-3674.
Change from a level 3 to a Level 2
+ Transfer from another facility
+ Extremes of cold or heat with prolonged exposure
+ Extremes of age <12 or >65
+ Co-morbidities (Anti-coagulant use, CopD, diabetes, CHf, etc.)
+ presence of intoxicants or illicit drugs
rICHArD TRuMPpa-C trauma
Lif
e F
light
Netw
ork
Bo
ise F
ire S
tati
on #
5

June 2012 7
sarmc.org
A new report on accidental deaths among US
children received extensive coverage, mostly
from online sources. Most sources portrayed
the findings as a step in the right direction, but
also emphasized the fact that deaths among
this population due to some factors, like
prescription drug abuse, are on the rise. USA
Today (4/17, Hellmich) reports, “The number
of children and teens who die from any kind
of accidents has dropped nearly 30% from
2000 to 2009, mostly because of a decline
in traffic deaths, says a new report from the
Centers for Disease Control and Prevention.”
However, the gains are “offset by the sobering
news that more than 9,000 young people still
die annually from motor-vehicle accidents,
fires, poisoning, drowning, falls and other
unintentional injuries.” Road traffic fatalities
account for more than 41% of all deaths,
most of those are with the child as occupant,
followed by a vehicle strike of a child as a
pedestrian. Falls, burns, and drowning were the
next most common causes of pediatric death.
The Los Angeles Times (4/17, Maugh)
“Booster Shots” blog reports that “agency
officials fear it may be difficult to lower the
rate further, however, because of sharp
increases in two areas: a 91% increase in
poisoning deaths among teenagers during
the period – primarily from prescription drug
abuse – and a 54% increase in suffocation
deaths among infants.” The report indicated
that “for every accidental death, there were
25 hospitalizations and 925 visits to the
emergency” department (ED). “Every 4
seconds, a child is treated for injury in an ED.”
The AP (4/17, Stobbe) reports, “The
report also looked at trends in individual
states.” The researchers “saw declines in
almost every state, with the biggest drops in
Delaware, Iowa, Oregon and Virginia.”
The Boston Globe (4/17, Kotz) “Daily
Dose” pointed out that “Massachusetts had
the lowest rate in the nation for pediatric
injury deaths in 2009: 4 deaths per 100,000
children up to age 19.” This “compares with
a national average of 11 deaths per 100,000,
with the worst state, Mississippi, having a
death rate of 25 per 100,000 -- more than six
times the rate of Massachusetts. The findings
were published in the Morbidity and Mortality
Weekly Report.”
Accidental Deaths Among u.s. Children
THE gOOd NEWS ANd BAd NEWS
TRAuMA TALk
“StateS With the
lOWeSt Death
rateS tenDeD
tO have mOre laWS
On the BOOkS
aDDreSSinG ChilD
SafetY anD
mOre prOGramS
aimeD at keepinG
ChilDren anD
teenS Safe.”
Continued on page 10
EDWArD MCEACHERN, MDiep executive Director/CeO
Bri
an B
oesi
ger, M
D

Want to share your story? [email protected]
Saint alphonSuS | emS newSletter
LOOkINg AT uS
Ad
a C
ounty
Para
med
ics
Meri
dia
n F
ire D
ep
t.

June 2012 9
sarmc.org
LOOkINg AT uS
Meri
dia
n F
ire D
ep
t.
Nam
pa P
olic
e D
ep
t
Nam
pa F
ire D
ep
tB
ois
e F
ire S
tati
on #
5
Nam
pa E
MS
Bake
r C
ity E
MS
Bo
ise F
ire S
tati
on #
5
Canyo
n C
ounty
P
ara
med
ics

Want to share your story? [email protected]
Saint alphonSuS | emS newSletter
TRAuMA TALk
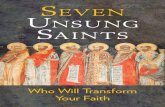
+ The number of unintentional injury deaths for the period 2000 – 2005 was 486; that is an average of 81 deaths per year.
+ The unintentional injury death rate was 19.3 per 100,000 population; this was higher than the national rate of 15.0 per 100,000 population.
+ Most injury deaths (65%) occurred among males 0 to 19 years of age.
+ Children 15 to 19 years of age and those less than 1 year of age had the highest death rates of all age groups (39.6 and 28.9 per 100,000 population, respectively).
+ Transportation-related injuries had the highest death rate among children 0 to 19 years of age in the state of Idaho (13.1 per 100,000 population).
+ The death rate for drowning was 1.6 per 100,000 population, and for suffocation was 1.4.
+ rates based on fewer than 20 deaths may be unreliable. numbers of deaths are presented.
Other unintentional injuries (for example: deaths from machinery or firearm) are not included in this figure therefore total number of injury deaths on the figure does not match the total number of injury deaths.
Find further information on these data, including methods, in the CDC Childhood Injury Report: Patterns of Unintentional Injuries among 0-19 Year olds in the United States, 2000 – 2006.
Continued from page 7
Accidental Death Among Children
IdAHO SLIgHTLy HIgHER THAN NATIONAL AvERAgE
CQ (4/17, Reichard, Subscription
Publication) reports that in a news release,
CDC Director Thomas Frieden said,
“Kids are safer from injuries today than
ever before.”
The Hill (4/17, Pecquet) “Healthwatch”
blog reports, “In conjunction with the report’s
release, the CDC and more than 60 partner
organizations released a National Action Plan
to raise awareness about childhood injury risks,
highlight prevention solutions and mobilize
action in a national, coordinated effort.”
MedPage Today (4/17, Petrochko)
reports that “unintentional injury still
accounted for 37% of all deaths in the
19-and-under age group in 2009 and was
the fifth leading killer of patients younger
than 1, the report said.”
WebMD (4/17, Boyles) reports, “States
with the lowest death rates tended to have
more laws on the books addressing child safety
and more programs aimed at keeping children
and teens safe.” Also covering the story are
the Minneapolis Star Tribune (4/17, Stoxen)
“Health Check” blog, the Wall Street Journal
(4/17, Martin) “Health Blog,” the CNN
(4/17) “The Chart” blog, the Huffington Post
(4/17, Young), Reuters (4/17), HealthDay
(4/17, Gardner), and the CBS News (4/17)
“HealthPop” blog.
Multiple sources cited; from ACEP and other wires
50
Transportation related 330
34
14
9
13
39
NuMBER OF uNINTENTIONAL INJuRy dEATHS By CAuSE, 2000-2005
suffocation
poisoning
fires/burns
falls
Drowning
number of Deaths 100 150 200 250 300 350
5 10
15-19 39.6
10.8
8.6
14.3
28.9
uNINTENTIONAL INJuRy dEATH RATES By AgE gROuP, 2000-2005
10 to 14
5 to 9
1 to 4
Less than 1
Death rate per 100,000 population
Data Source, CDC/NCHS, National Vital Statistics System
15 20 25 30 35 40

June 2012 11
sarmc.org
TRAuMA TALk
+ Teach your children to use a seat belt and never drive with out the proper child restraints in a car.
+ Teach your children common sense around cars and traffic.
+ never leave your child unattended at a pool or around water.
+ be aware of fall risks in your home.
+ Teach your children to swim, and respect water at a young age.
+ Lower the temperature of your water heater at home so that the hot tap water is unlikely to burn a child.
+ Lock all medicines away from areas where children might come in contact with them.
Things that you can do to prevent childhood deaths and injuries:
Lif
e F
light
Netw
ork

Want to share your story? [email protected]
Saint alphonSuS | emS newSletter
NEuRO/STROkE
May was Stroke Awareness month. As we
strive to educate our community about stroke
risk factors, signs and symptoms of stroke,
and the importance of calling 911 if stroke
is suspected, we recognize the vital role that
our First Responders play in the outcome of
those who experience a stroke. Our continued
partnership allows us to provide the highest
quality care and reduce the impact that stroke
has on Southwest Idaho.
Research has proven that treating
ischemic strokes with IV t-PA reduces
death and disability from stroke. Across the
country, the average treatment rate is between
2-3%. At Saint Alphonsus, our IV t-PA
treatment rate has risen from 8.33% in 2008
to 17.24% in 2011! We would like this rate
to be even higher so that more patients can
benefit from this life-saving treatment. First
responders can have a tremendous effect on
the treatment received by stroke patients. The
American Stroke Association has published
recommendations for First Responders who
provide stroke care:
+ Patients should be transported to the highest level of care or the nearest Certified Stroke Center.
+ Pre-notify Saint Alphonsus Medical Access Center with a “brain attack”. This designates an acute stroke and allows our stroke response team to prepare to receive the patient and act quickly.
+ Cincinnati Stroke Scale is a highly reliable tool for identifying a stroke patient. It is also a great communication tool for the ED hand-off.
+ Determine by asking the patient or the witness what time the patient was last known to be normal. This time starts the treatment clock-remember that IV t-PA must be given in 3 hours (4.5 hours for certain patients) and clot extraction must happen within 8 hours.
+ Ask the patient or witnesses if the patient takes warfarin or other anticoagulant medications.
+ First Responders and hospitals should collaborate in EMS training.
To that end, we would like to provide you with
some stroke education that offers free
CE credits! EMS4Stroke.com to learn more
about this great opportunity.
Thank you for all the stellar care that you give
to our patients!
CERTIFIEd STROkE CENTER uPdATE
“at Saint
alphOnSUS,
OUr iv t-pa
treatment rate
haS riSen frOm
8.33% in 2008
tO 17.24% in 2011”
nICHoLE WHITENER
mSn, Cnrn, ne-BC neuro/Stroke Director
photo above: listed left to right
top: vic Garabedian mD, lisa nelson mD, Will farley, adrean Casper, nichole Whitener
middle: ted ryan, Jane Spencer, terry newsome
Bottom: patty huffman, mary river mD, tita petersen, Jackie Whitesell mD
Lif
e F
light
Netw
ork

June 2012 13
sarmc.org
NEuRO/STROkE
IT’S gOLd AgAIN FOR SAINT ALPHONSuS
BREAkTHROugH STROkE dEvICE MAkES dEBuT AT SAINT ALPHONSuS
Saint Alphonsus Regional Medical Center has
received the American Heart Association/
American Stroke Association’s Get With
The Guidelines®-Stroke Gold Plus Quality
Achievement Award for the second year in a
row. The award recognizes Saint Alphonsus’
commitment and success in implementing
excellent care for stroke patients, according to
evidence-based guidelines. Saint Alphonsus is
the only hospital in the region to be named.
To receive the award, Saint Alphonsus
achieved an 85 percent or higher adherence to
all Get With The Guidelines-Stroke Quality
Achievement indicators for two or more
consecutive 12-month intervals and achieved
75 percent or higher compliance with six of
10 Get With The Guidelines-Stroke Quality
Measures, which are reporting initiatives to
measure quality of care.
These measures include aggressive use of
medications, such as tPA, antithrombotics,
anticoagulation therapy, DVT prophylaxis,
cholesterol reducing drugs and smoking
cessation, all aimed at reducing death and
disability and improving the lives of stroke
patients.
“The time is right, now more than
ever, for Saint Alphonsus to be focused
on improving the quality of stroke care by
implementing Get With The Guidelines–
Stroke. The number of acute ischemic stroke
patients eligible for treatment is expected to
grow over the next decade due to increasing
stroke incidence and a large aging population.
As the area’s only Joint Commission Certified
Primary Stroke Center, Saint Alphonsus is
committed to providing the most effective
stroke treatment available,” said Nichole
Whitener, RN, MSN, Director, Saint
Alphonsus Stroke Program.
Saint Alphonsus Regional Medical Center is
proud to be the only hospital in the Treasure
Valley to have used the Solitaire FR for the
treatment of acute stroke. In clinical trial,
Solitaire FR showed a 1.7 times improvement
in neurological function and a 55 percent
reduction in mortality at 90 days when
compared to other devices.
This state-of-the-art device works by
expanding into a clot that is blocking a vessel
in the brain and snaring it, then removing the
clot. Compared to other devices, the Solitaire
FR restored 2.5 times as much blood flow to
the brain, which is crucial in the successful
treatment of stroke.
Saint Alphonsus radiology staff is fully
trained to use this device to treat acute stroke.
Physicians have received specialized training
and experience that is unique to the Treasure
Valley. This new advancement is another
addition to Saint Alphonsus’ award-winning,
certified, proven system of care to treat
complex stroke patients.

Want to share your story? [email protected]
Saint alphonSuS | emS newSletter
The Emergency Department at the Saint
Alphonsus Eagle Health Plaza was the first
of its kind in Idaho, and has proven to be a
valuable resource for the Eagle community.
We provide care close to home for patients
of all ages, with a range of diagnoses, from
urgent to emergent. As an EMS provider, you
are probably familiar with the facility, but it’s
important to understand the nuances of the
free-standing ER.
The Eagle ER is a full-service facility
with the capability to handle a broad range
of emergent conditions. Staffed 24/7
with a board-certified emergency medicine
physician and certified emergency medicine
nurses, we are always ready to receive EMS
arrivals. The facility is equipped to care
for patients with high-risk problems such
as chest pain, abdominal pain, headaches,
COPD exacerbations, asthma attacks, fever,
anaphylaxis, closed fractures, and Level 3
traumatic injury. Many patients with these
problems are treated and discharged from
the ER, so it makes sense to keep them close
to home. And if a patient needs admitted
from the Eagle ER, transport by ambulance is
provided free of charge to any local hospital
of the patient’s choice.
There are a few patients who should not
be transported to the Eagle ER, but rather
go directly to the nearest hospital capable of
definitive treatment for their condition. As a
general rule, these are patients with emergent
conditions that need immediate treatment by
a specialist in a hospital setting. These would
include patients with STEMI, acute stroke,
pre-hospital intubation, and Level 1 or Level
2 traumatic injury. Also, patients with open
fracture, unstable active GI bleeding, and
contractions or labor during pregnancy.
The Eagle ER is always ready to assist
with resuscitation. If you have a patient
who is receiving CPR or needs emergent
intubation, do not hesitate to come directly
to the Eagle ER for assistance with initial
management and stabilization.
Thank you for all you do. We look
forward to partnering with you in providing
care for our community, keeping patients close
to home.
EAgLE ER kEEPINg PATIENTS CLOSE TO HOME
“eaGle’S OnlY er
iS a fUll ServiCe
faCilitY. patientS
WhO reqUire
aDmiSSiOn Or
COnSUltatiOn Will
Be tranSferreD
expeDitiOUSlY tO
Saint alphOnSUS
reGiOnal meDiCal
Center at nO
aDDitiOnal COSt
tO the patient.”
EAgLE ER
ErIC ELLIOTT, MDiep/eagle er medical Director
Sain
t A
lpho
nsu
s E
ag
le E
R

June 2012 15
sarmc.org
AWARdS & RECOgNITION
ExCELLENT JOB kuNA EMS! We value your work and appreciate you keeping our community safe.pat Bergey, rn, BSn
The Trauma Service Team would like to express thanks to Kuna Fire for a job well done. Kuna
ambulance transported two patients to Saint Alphonsus in the early morning hours of February
14. Both patients, a 41 and 42 year-old male were involved in a high-speed rollover collision in
the desert by Swan Falls. The less injured patient extricated himself from the vehicle, and pulled
a sleeping bag out to cover the other more seriously injured patient who was ejected from the
vehicle. The Kuna ambulance service did an outstanding job. The patients received excellent
care, and were “packaged” appropriately for transport. The crew called in the appropriate
information, which allowed the Access Center to activate the trauma team members necessary
for the level of care. Good job Kuna, great teamwork!
If you would like to have further follow up on your patients hospital course, please have a
representative of your agency contact me by phone or email, and I will be happy to provide a
more complete report. Contact: 208.367.6435 or [email protected]
gREAT JOB TO THE AdA COuNTy PARAMEdICS
for their Trauma Leveling skills!
Through the efforts of the Ada County Paramedics, the Saint Alphonsus Access
Center, and the Saint Alphonsus Emergency Department, trauma under triage level
has been 3% or less over the past 8 months! Thank you!
2012 ACP EMS AWARdS
SUperviSOr Of the Year
CLInTon WOLF
reServe Of the Year
AMon RAE
phYSiCian Of the Year
MArK HENzLER,MD
parameDiC Of the Year
MArK BABSON
emt Of the Year
GEorGE WINg
emt Of the Year
GEorGE WINg
BUSineSS OffiCe
emplOYee Of the Year
KArEn MARTIN
aDminiStrative Of the Year
AMY FuLLER
Joe L
ink, P
aul S
chep
per, J
on T
illm
an
TJ
Law
rence
, Sean S
tear
Sain
t A
lpho
nsu
s E
ag
le E
R

BOISE 1055 n. Curtis rd. 208.367.2121
EMERgENCy dEPTS.
BAkER CITy 3325 pocahontas rd. 541.523.6461
EAgLE 323 E. riverside Dr. 208.367.5300
NAMPA 1512 12th Ave. rd. 208.463.5000
ONTARIO 351 sW 9th st. 541.881.7000
Saint Alphonsus Regional Medical Center 1055 N Curtis Road Boise, ID 83706
N
S
E W