Hepatocytes as Immunological Agents · Hepatocytes as Immunological Agents Ian N. Crispe...
6
of February 2, 2019. This information is current as Hepatocytes as Immunological Agents Ian N. Crispe http://www.jimmunol.org/content/196/1/17 doi: 10.4049/jimmunol.1501668 2016; 196:17-21; ; J Immunol References http://www.jimmunol.org/content/196/1/17.full#ref-list-1 , 15 of which you can access for free at: cites 54 articles This article average * 4 weeks from acceptance to publication Fast Publication! • Every submission reviewed by practicing scientists No Triage! • from submission to initial decision Rapid Reviews! 30 days* • Submit online. ? The JI Why Subscription http://jimmunol.org/subscription is online at: The Journal of Immunology Information about subscribing to Permissions http://www.aai.org/About/Publications/JI/copyright.html Submit copyright permission requests at: Email Alerts http://jimmunol.org/alerts Receive free email-alerts when new articles cite this article. Sign up at: Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved. Copyright © 2015 by The American Association of 1451 Rockville Pike, Suite 650, Rockville, MD 20852 The American Association of Immunologists, Inc., is published twice each month by The Journal of Immunology by guest on February 2, 2019 http://www.jimmunol.org/ Downloaded from by guest on February 2, 2019 http://www.jimmunol.org/ Downloaded from
Transcript of Hepatocytes as Immunological Agents · Hepatocytes as Immunological Agents Ian N. Crispe...

of February 2, 2019.This information is current as
Hepatocytes as Immunological Agents
Ian N. Crispe
http://www.jimmunol.org/content/196/1/17doi: 10.4049/jimmunol.1501668
2016; 196:17-21; ;J Immunol
Referenceshttp://www.jimmunol.org/content/196/1/17.full#ref-list-1
, 15 of which you can access for free at: cites 54 articlesThis article
average*
4 weeks from acceptance to publicationFast Publication! •
Every submission reviewed by practicing scientistsNo Triage! •
from submission to initial decisionRapid Reviews! 30 days* •
Submit online. ?The JIWhy
Subscriptionhttp://jimmunol.org/subscription
is online at: The Journal of ImmunologyInformation about subscribing to
Permissionshttp://www.aai.org/About/Publications/JI/copyright.htmlSubmit copyright permission requests at:
Email Alertshttp://jimmunol.org/alertsReceive free email-alerts when new articles cite this article. Sign up at:
Print ISSN: 0022-1767 Online ISSN: 1550-6606. Immunologists, Inc. All rights reserved.Copyright © 2015 by The American Association of1451 Rockville Pike, Suite 650, Rockville, MD 20852The American Association of Immunologists, Inc.,
is published twice each month byThe Journal of Immunology
by guest on February 2, 2019http://w
ww
.jimm
unol.org/D
ownloaded from
by guest on February 2, 2019
http://ww
w.jim
munol.org/
Dow
nloaded from

Hepatocytes as Immunological AgentsIan N. Crispe
Hepatocytes are targeted for infection by a number ofmajor human pathogens, including hepatitis B virus,hepatitis C virus, and malaria. However, hepatocytesare also immunological agents in their own right. Insystemic immunity, they are central in the acute-phaseresponse, which floods the circulation with defensive pro-teins during diverse stresses, including ischemia, physicaltrauma, and sepsis. Hepatocytes express a variety of in-nate immune receptors and, when challenged with path-ogen- or damage-associated molecular patterns, candeliver cell-autonomous innate immune responses thatmay result in host defense or in immunopathology. Im-portant human pathogens have evolved mechanisms tosubvert these responses. Finally, hepatocytes talk directlyto T cells, resulting in a bias toward immune tolerance.The Journal of Immunology, 2016, 196: 17–21.
Hepatocytes are the most abundant cell type in theliver, accounting for perhaps 90% of the biomass.When these cells are infected, whether by a hepato-
tropic virus, a parasite, or an intracellular bacterium, a complexlocal response involves diverse immunologically active cells thatare found in the nonparenchymal fraction: liver sinusoidalendothelial cells, Kupffer cells, and hepatic stellate cells, as wellas trafficking monocytes, dendritic cells (DCs), NK cells,NKT cells, and diverse varieties of CD4+ and CD8+ T cells.Much recent research clarified the roles of each of these celltypes in antiviral, antimalarial, and antibacterial immunity, buthepatocytes are not passive recipients of immune signals fromthese surrounding cells. The purpose of this review is to shiftthe immunological focus to hepatocytes and emphasize theiractive role in both innate and adaptive immunity to manyhepatic insults. Hepatocytes are not simply target cells but areimmunological agents in their own right.Hepatocytes are relatively tractable experimentally. In mice,
they can be manipulated using a transgenic approach, becausethe albumin promoter results in highly cell type–specifictransgene expression. Hepatocyte-like immortalized cell linesreproduce many features of primary hepatocyte activity. Inaddition, well-defined protocols exist for the isolation of he-patocytes from mouse liver, through perfusion of the organwith collagenase, followed by selective depletion of the non-
parenchymal fraction. In the human this task is moredaunting, but the logistical hurdles can be overcome, andprimary human hepatocytes are widely available from severalsources. Therefore, our understanding of the immunology ofhepatocytes comes from in vivo experiments in mice and exvivo experiments with murine and human cell lines and pri-mary cells.
The acute phase
Hepatocytes are central in the systemic innate immune re-sponse to sepsis, which is extensively conserved in vertebratesfrom mammals to bony fish (1). In the acute-phase response,either generalized or localized infection increases the circulat-ing levels of several key cytokines, including IL-1a, TNF-a,and IL-6 (Fig. 1). These mediators result in coordinatedchanges in the transcriptional activity of hepatocytes, with thesecretion of molecules that limit tissue injury and moleculesthat participate in host defense (2). Among the cytokines thatdrive the acute-phase response, IL-6 acts directly on hepato-cytes. In human hepatocytes, rIL-6 induced a classic pat-tern of acute-phase proteins, including serum amyloid A,C-reactive protein, haptoglobin, a1-antichymotrypsin, andfibrinogen. Conversely, the normal hepatocyte secretionproducts albumin, transferrin, and fibronectin were reduced(3). At least some of the IL-6–induced effects appear to behepatoprotective, because elimination of the gp130 compo-nent of the IL-6R in transgenic mice attenuated the acute-phase response and led to an increase in liver injury inhepatitis induced by bacterial endotoxin (4). Many of theacute-phase proteins are counterregulated by hepatocyte growthfactor (HGF), which plays a key role in liver growth and re-generation; however, in primary human hepatocytes, HGF alsosuppressed a1-antichymotrypsin and haptoglobin while in-creasing the synthesis of albumin, transferrin, and fibronectin(5). The coordinated regulation of acute-phase protein genes isregulated, in part, by microRNAs that interact with the con-served 39 untranslated regions of those genes that are differ-entially expressed during the acute-phase response (6).New members of the IL-6–induced class of host defense
proteins continue to be identified. Recently, hepatocytes wereidentified to be the important source of the antibacterialprotein lipocalin-2 (7). Although exogenous IL-6 can drivethe acute-phase response, hepatocytes also synthesize IL-6 in
Department of Pathology, University of Washington, Seattle, WA 98195
Received for publication August 6, 2015. Accepted for publication October 2, 2015.
This work was supported in part by National Institutes of Health Grants R01AI114630,R21AI114827, and R21AI099872.
Address correspondence and reprint requests to Dr. Ian N. Crispe, Department ofPathology, University of Washington, 1595 NE Pacific Street, Seattle, WA 98195.E-mail address: [email protected]
Abbreviations used in this article: DC, dendritic cell; HBV, hepatitis B virus; HCC,hepatocellular cancer; HCV, hepatitis C virus; HGF, hepatocyte growth factor; MDSC,myeloid-derived suppressor cell; STING, stimulator of IFN genes.
Copyright� 2015 by TheAmerican Association of Immunologists, Inc. 0022-1767/15/$30.00
www.jimmunol.org/cgi/doi/10.4049/jimmunol.1501668
Journal ofTh e
ImmunologyBrief Reviews
by guest on February 2, 2019http://w
ww
.jimm
unol.org/D
ownloaded from

response to diverse stimuli, including HGF (8), giving thismolecule a role in activating and in suppressing the acutephase. The acute-phase response is not monolithic; variants ofthis response have been identified during ischemia-reperfusioninjury (9, 10), in liver regeneration following partial hepa-tectomy (11), during abdominal surgery (12), and in nonin-fected bone fractures (13).This brief introduction to a complex topic makes two key
points: that the liver makes a major contribution to systemicinnate immunity and that hepatocytes are both sensors of suchinjury and the principal source of the protective proteins thusinduced.
Self-defense at the cellular level
Hepatocytes express a wide variety of pattern recognition re-ceptors, including cell surface receptors (e.g., TLR4), endo-somal receptors (e.g., TLR3), and cytoplasmic receptors (e.g.,stimulator of IFN genes [STING], retinoic acid induciblegene-1 (RIG-1), and nucleotide-binding oligomerization do-main (NOD) family members) (14). Isolated hepatocytesrespond directly to microbial products (15) and to endoge-nous signals, such as heat shock protein 72, via their TLR2and TLR4 receptors (16). The expression of these receptorsmay be differentially regulated. For example, diverse stimuliupregulate the expression of TLR2, but not TLR4, on he-patocytes (17). TLR2 may mediate liver-protective signals, forexample in parasite infection (18). Conversely, in liver injury
mediated by a TLR9 ligand, IRF7 and type 1 IFN signalingvia the IFN-aR ameliorate liver injury through the action ofIL-1ra, an antagonist of IL-1R signaling (19).The innate immune response of hepatocytes to a major human
pathogen, hepatitis C virus (HCV), is relatively well understood.Viral RNA engages the RIG-1 system, resulting in signaling viaMAVS that activates the transcription factor IRF3 and its target,type 1 IFN. In parallel, dsRNA engages TLR3, signaling via theTRIF adapter protein to activate IRF3. It is clear that both ofthese signaling pathways are important in host defense becausethe virus has evolved a protease, NS3/4a, which can cleave bothTRIF andMAVS, disabling IRF3 activation (20, 21). Therefore,it came as a surprise that primary human hepatocytes infectedwith HCV strain JFH1 were able to synthesize multiple cyto-kines and chemokines, whereas hepatocyte-like Huh7 cells se-creted very few, principally IL-28 (IFN-l). However, efforts toremove the trace numbers of nonparenchymal cells from theprimary hepatocyte culture reduced the secretion of many ofthese chemokines and cytokines (22). Therefore, in the presenceof viral immune-subversion mechanisms, the cell-autonomousself-defense capacity of hepatocytes is curtailed; however, somepathways remain active, whereas others are the task of non-parenchymal cells.Hepatocytes also harbor the capacity to mount cell-
autonomous defense against hepatitis B virus (HBV), butjust as HCV has evolved ways to disable cytoplasmic RNAsensing, HBV acts against cytoplasmic DNA sensing. Specifically,
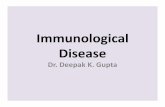
FIGURE 1. Three major aspects of hepatocyte immune activity. On the left, the acute-phase response is activated by diverse system stresses, including sepsis,
sustained by a feed-forward loop in which hepatocytes both make and respond to IL-6, and changes the hepatocytes’ transcriptional profile, resulting in the
secretion of many defensive proteins into the blood. The central region of the figure illustrates some of the main players during innate immunity in hepatocytes,
classified into innate immune sensors, adapter proteins, and effector responses. Innate immune activation in hepatocytes can result in either protein–protein
interactions, as in the inflammasome and the apoptosome, or it can cause gene transcription (e.g., of IFN-a/b and IFN-responsive genes). The expression of genes
encoding both inflammasome and apoptosome components can also be increased, or these structures can nucleate independently of transcription (not shown). On
the right, the diagram represents two distinct ways in which a direct encounter with an Ag-presenting hepatocyte can cause CD8+ T cell tolerance. First, CD8+ T
cell activation on a hepatocyte can result in abortive activation, due to the lack of costimulation or CD4+ T cell help. Second, the hepatocyte can endocytose and
kill the T cell (“suicidal emperipolesis”). Because hepatocytes cells do not express MHC class II, CD4+ T are not directly inactivated by hepatocyte contact.
18 BRIEF REVIEWS: HEPATOCYTE IMMUNOLOGY
by guest on February 2, 2019http://w
ww
.jimm
unol.org/D
ownloaded from

the viral polymerase interacts directly with the STING DNAsensor, inhibiting its function (23). Conversely, direct stim-ulation of STING using a synthetic agonist resulted in cyto-kines dominated by type 1 IFN and an antiviral effectthat suppressed HBV replication (24). Thus, understandinghepatocyte innate immune pathways may lead to novel ap-proaches to antiviral therapy.Cells may respond to insult by undergoing programmed cell
death, of which the principal recognized forms are apoptosis(initiated by caspases), necroptosis (initiated by RIP kinases),and pyroptosis (initiated by activation of the inflammasome).Hepatocyte-resident innate immune pathways can contributeto cell death in immunopathology that occurs in the absence ofa hepatocellular pathogen. Thus, ethanol-associated liver in-jury depends on TLR4, IRF3, and STING (25, 26) to triggerthe mitochondrial pathway of apoptosis via Bax. Hepatocytesmay undergo different varieties of programmed cell death inresponse to diverse insults. Thus, ethanol-induced liver injuryalso involves necroptosis mediated via RIPK3 (27). Similarly,inhibition of RIPK1 protects mice from acetaminophen-induced injury (28), but acetaminophen also acts via TLR9and the NALP3 inflammasome, implicating pyroptosis. Thisled to the striking result that aspirin, an inhibitor of inflam-masome activation, suppressed acetaminophen toxicity (29).Hepatocellular cancer (HCC) frequently arises in the con-
text of chronic liver inflammation, but the links between theinflammation and the cancer are complex. Innate immuneresponses of hepatocytes modify the response to carcinogenesis.In a mouse model of HCC, TLR2 expressed on hepatocytessuppressed the expression of IL-18, whereas IL-18 was re-sponsible for the accumulation of myeloid-derived suppressorcells (MDSCs). Thus, in the absence of this signaling pathway,HCC growth was enhanced; when a TLR2 agonist was ad-ministered, HCC was suppressed (30). Both TLR3 and TLR7are underexpressed in hepatoma cells, and there exists ahepatocyte-specific regulatory region in the TLR-7 pro-moter (31). Further, IL-7 expression in hepatoma cellswas suppressed by IFN-g. The TLR2–IL-18 and IFN-g–TLR7 pathways establish links between liver inflammationand HCC.Therefore, hepatocytes are active participants in cell-
autonomous innate immune responses that may suppresspathogens but also result in immunopathology, including theactivation of cell death pathways. In HCC, some aspects ofinnate immunity seem to be harmful (IFN-g, IL-18), butother pathways enhance anticancer immunity (TLR2, andperhaps TLR7).
Afferent and efferent innate immune signals
The major circulatory input to the liver is the portal vein;therefore, innate immune signals from the intestinal micro-biota impinge strongly on hepatic biology. One clear exampleis the impact of LPS endotoxin from Gram-negative bacteria,which supports the capacity of the liver to sequester activatedand apoptotic T cells from the circulation (32). In addition,the intestinal microbiota has been implicated in liver disease.Specifically, changes in the microbiota impact diverse liverpathologies, including diet-induced liver inflammation (33),autoimmune hepatitis (34), antiviral immunity (35), fibrosis(36), and even liver cancer (37). Given the wide array of in-nate immune receptors expressed on hepatocytes, it is likely
that they play a central role in these responses; however, in-formation is limited, and this is an important topic for futureresearch.In addition to cell-autonomous responses and the systemic
acute-phase response, hepatocytes interact locally with innateimmune cells. Thus, hepatocytes express the NK cell targetsMIC-A and MIC-B; this is biologically significant in hostdefense, because HBsAg modulates their expression throughthe induction of cellular microRNAs (38). Similarly, the ca-nonical NKT cell restriction element, CD1d, is expressed onhepatocytes and upregulated in chronic HCV infection (39).In mice, CD1d promotes liver injury and fibrosis, arguingfor an important role for the hepatocyte–NKT cell axis inimmunopathology (40). Finally, hepatocytes may modulateinnate immune cells through the acute-phase response. Spe-cifically, the gp130–STAT3 signaling axis promotes recruit-ment of immature myeloid cells (MDSCs) that regulateinnate immune inflammation (41). In a further link betweenthe acute-phase response and innate immunity, MDSCs canbe induced by HGF (42).
T cells, priming, and tolerance
In addition to innate signals from the intestinal microbiota, theliver encounters a wide range of Ags among the products ofdigestion, and it creates more through hepatocellular meta-bolism. Therefore, it is clear that a bias toward immune tol-erance to hepatocellular Ags serves a valuable purpose inpreventing futile immunity to nonhazardous molecules.Immune tolerance associated with Ags present in the liver
may be due, in part, to the ambiguous relationship of hepa-tocytes to T cells. The structure of the liver sinusoidal en-dothelium features small openings (fenestrae) grouped intosieve plates, and these openings permit direct interaction be-tween hepatocytes and the blood space (43). Because T cells donot need to extravasate to make contact with hepatocytes, theopportunities for hepatocytes to talk to naive T cells are en-hanced. The outcome of such a conversation is usually to theT cell’s disadvantage. Ex vivo, Ag-specific CD8+ T cells di-rectly confronted with antigenic hepatocytes undergo initialactivation (44, 45), followed by loss of function and prema-ture cell death. This might be due to the lack of either co-stimulatory signals or CD4+ T cell help, because it can bepartially reversed with exogenous IL-2 (46). More dramati-cally, the hepatocytes may endocytose and kill CD8+ T cellsthat recognize them, a process known as suicidal emperipol-esis (47). Because hepatocytes express MHC class I, and notMHC class II, CD4+ T cells are not impacted directly bythese hepatocyte-based tolerance mechanisms.These mechanisms may act primarily to abort the activation
of naive CD8+ T cells. In vivo, introduction of naive Ag-specific CD8+ T cells results in T cell proliferation and hep-atitis; however, in general, the Ag persists, accompanied byT cell clonal exhaustion (48, 49). The level of Ag expressionmodulates this, and experiments that restrict Ag to rare he-patocytes may result in strong immunity if high-affinity CD8+
T cells are present (50); this cannot be a general conclusionbecause malaria parasites, which infect very few hepatocytes,normally induce little liver-stage–specific immunity. How-ever, the introduction of Ag-specific CD8+ T cells into atransgenic mouse that expresses hepatocyte Ags readily resultsin inflammation accompanied by hepatocyte death. This is
The Journal of Immunology 19
by guest on February 2, 2019http://w
ww
.jimm
unol.org/D
ownloaded from

most clearly seen in mice expressing HBV as a hepatocellulartransgene (51). Therefore, however immune failure arises, itdoes not necessarily protect the liver from injury.The direct access of naive CD8+ T cells to hepatocellular
Ags via fenestrae raises the question of how such CD8+ T cellsmight interact with CD4+ T cell help. A major pathway bywhich CD4+ and CD8+ T cells interact is the licensingmechanism whereby CD4+ and CD8+ T cells both interactwith DCs. The CD4+ T cell, acting via CD40, induceschanges in the DCs, including increased expression of co-stimulatory molecules, such as CD80, CD86, and CD70, allof which facilitate optimum CD8+ T cell activation (52).However, if CD8+ T cells receive their primary activationsignals from hepatocytes, they are engaging a cell that lacksMHC class II expression and so cannot be licensed. It followsthat, for the delivery of efficient CD4+ T cell help to a CD8+
T cell for a hepatocellular Ag, that Ag must be cross-presentedby a different cell type (53).Hepatocytes themselves may impose a barrier to such cross-
presentation. The process is mediated by secreted Ags, Ag-carrying exosomes, and apoptotic fragments derived fromdead and dying cells. Such fragments are readily taken up byneighboring hepatocytes (e.g., via the asialoglycoprotein re-ceptor) (54). This may explain why, in a radiation bonemarrow chimera, there was no evidence of cross-presentationby bone marrow–derived cells of hepatocellular Ags encodedby an adeno-associated virus vector (55). Ags acquired fromdying hepatocytes and cross-presented by their neighborswould be subject to the same constraints as Ags in their he-patocyte of origin: CD8+ T cell engagement by an APC thatcannot receive licensing signals.
ConclusionsHepatocytes are active participants in innate immune re-sponses. They are central drivers of the systemic acute-phaseresponse and can respond to diverse insults, including stressand infection, resulting in either host defense or programmedcell death. In CD8+ T cell immunity, they mostly promotetolerance, but this is not a passive process; instead, hepatocytesabortively activate and may actively kill CD8+ T cells that rec-ognize them, and their inherent capacity to take up hepatocytedebris effectively subverts the mechanisms of cross-presentationthat are essential for the delivery of CD4+ T cell help.
DisclosuresI.N.C. received a research grant from Janssen Sciences to study liver immunology
in human cells, including hepatocytes. This has had no influence on the content
of this Brief Review.
References1. Lin, B., S. Chen, Z. Cao, Y. Lin, D. Mo, H. Zhang, J. Gu, M. Dong, Z. Liu, and
A. Xu. 2007. Acute phase response in zebrafish upon Aeromonas salmonicida and
Staphylococcus aureus infection: striking similarities and obvious differences with
mammals. Mol. Immunol. 44: 295–301.2. Bauer, M., A. T. Press, and M. Trauner. 2013. The liver in sepsis: patterns of re-
sponse and injury. Curr. Opin. Crit. Care 19: 123–127.3. Castell, J. V., M. J. Gomez-Lechon, M. David, T. Hirano, T. Kishimoto, and
P. C. Heinrich. 1988. Recombinant human interleukin-6 (IL-6/BSF-2/HSF) reg-
ulates the synthesis of acute phase proteins in human hepatocytes. FEBS Lett. 232:347–350.
4. Streetz, K. L., T. W€ustefeld, C. Klein, K. J. Kallen, F. Tronche, U. A. Betz,
G. Sch€utz, M. P. Manns, W. M€uller, and C. Trautwein. 2003. Lack of gp130
expression in hepatocytes promotes liver injury. Gastroenterology 125: 532–543.5. Guillen, M. I., M. J. Gomez-Lechon, T. Nakamura, and J. V. Castell. 1996. The
hepatocyte growth factor regulates the synthesis of acute-phase proteins in human
hepatocytes: divergent effect on interleukin-6-stimulated genes. Hepatology 23:1345–1352.
6. Lukowski, S. W., R. J. Fish, J. Martin-Levilain, C. Gonelle-Gispert, L. H. B€uhler,P. Maechler, E. T. Dermitzakis, and M. Neerman-Arbez. 2015. Integrated analysisof mRNA and miRNA expression in response to interleukin-6 in hepatocytes.Genomics 106: 107–115.
7. Xu, M. J., D. Feng, H. Wu, H. Wang, Y. Chan, J. Kolls, N. Borregaard, B. Porse,T. Berger, T. W. Mak, et al. 2015. Liver is the major source of elevated serumlipocalin-2 levels after bacterial infection or partial hepatectomy: a critical role forIL-6/STAT3. Hepatology 61: 692–702.
8. Norris, C. A., M. He, L. I. Kang, M. Q. Ding, J. E. Radder, M. M. Haynes,Y. Yang, S. Paranjpe, W. C. Bowen, A. Orr, et al. 2014. Synthesis of IL-6 by he-patocytes is a normal response to common hepatic stimuli. PLoS One 9: e96053.
9. Broughan, T. A., G. F. Jin, and J. Papaconstantinou. 1996. Early gene response tohepatic ischemia reperfusion. J. Surg. Res. 63: 98–104.
10. Tiberio, L., G. A. Tiberio, L. Bardella, E. Cervi, K. Cerea, M. Dreano, G. Garotta,A. Fra, N. Montani, A. Ferrari-Bravo, et al. 2006. Mechanisms of interleukin-6protection against ischemia-reperfusion injury in rat liver. Cytokine 34: 131–142.
11. Kusashio, K., H. Shimizu, F. Kimura, H. Yoshidome, M. Ohtsuka, A. Kato,H. Yoshitomi, K. Furukawa, T. Fukada, and M. Miyazaki. 2009. Effect of excessiveacute-phase response on liver regeneration after partial hepatectomy in rats. Hep-atogastroenterology 56: 824–828.
12. Grande, M., G. F. Tucci, O. Adorisio, A. Barini, F. Rulli, A. Neri, F. Franchi, andA. M. Farinon. 2002. Systemic acute-phase response after laparoscopic and opencholecystectomy. Surg. Endosc. 16: 313–316.
13. Bauza, G., G. Miller, N. Kaseje, N. A. Wigner, Z. Wang, L. C. Gerstenfeld, andP. A. Burke. 2011. The effects of injury magnitude on the kinetics of the acute phaseresponse. J. Trauma 70: 948–953.
14. Seki, E., and D. A. Brenner. 2008. Toll-like receptors and adaptor molecules in liverdisease: update. Hepatology 48: 322–335.
15. Vodovotz, Y., S. Liu, C. McCloskey, R. Shapiro, A. Green, and T. R. Billiar. 2001.The hepatocyte as a microbial product-responsive cell. J. Endotoxin Res. 7: 365–373.
16. Galloway, E., T. Shin, N. Huber, T. Eismann, S. Kuboki, R. Schuster, J. Blanchard,H. R. Wong, and A. B. Lentsch. 2008. Activation of hepatocytes by extracellularheat shock protein 72. Am. J. Physiol. Cell Physiol. 295: C514–C520.
17. Matsumura, T., A. Ito, T. Takii, H. Hayashi, and K. Onozaki. 2000. Endotoxinand cytokine regulation of toll-like receptor (TLR) 2 and TLR4 gene expression inmurine liver and hepatocytes. J. Interferon Cytokine Res. 20: 915–921.
18. Carrera-Silva, E. A., N. Guinazu, A. Pellegrini, R. C. Cano, A. Arocena, M. P. Aoki,and S. Gea. 2010. Importance of TLR2 on hepatic immune and non-immune cellsto attenuate the strong inflammatory liver response during Trypanosoma cruzi acuteinfection. PLoS Negl. Trop. Dis. 4: e863.
19. Petrasek, J., A. Dolganiuc, T. Csak, E. A. Kurt-Jones, and G. Szabo. 2011. Type Iinterferons protect from Toll-like receptor 9-associated liver injury and regulate IL-1receptor antagonist in mice. Gastroenterology 140: 697–708.e4.
20. Foy, E., K. Li, R. Sumpter, Jr., Y. M. Loo, C. L. Johnson, C. Wang, P. M. Fish,M. Yoneyama, T. Fujita, S. M. Lemon, and M. Gale, Jr. 2005. Control of antiviraldefenses through hepatitis C virus disruption of retinoic acid-inducible gene-I sig-naling. Proc. Natl. Acad. Sci. USA 102: 2986–2991.
21. Ferreon, J. C., A. C. Ferreon, K. Li, and S. M. Lemon. 2005. Molecular deter-minants of TRIF proteolysis mediated by the hepatitis C virus NS3/4A protease. J.Biol. Chem. 280: 20483–20492.
22. Brownell, J., J. Wagoner, E. S. Lovelace, D. Thirstrup, I. Mohar, W. Smith,S. Giugliano, K. Li, I. N. Crispe, H. R. Rosen, and S. J. Polyak. 2013. Independent,parallel pathways to CXCL10 induction in HCV-infected hepatocytes. J. Hepatol.59: 701–708.
23. Liu, Y., J. Li, J. Chen, Y. Li, W. Wang, X. Du, W. Song, W. Zhang, L. Lin, andZ. Yuan. 2015. Hepatitis B virus polymerase disrupts K63-linked ubiquitination ofSTING to block innate cytosolic DNA-sensing pathways. J. Virol. 89: 2287–2300.
24. Guo, F., Y. Han, X. Zhao, J. Wang, F. Liu, C. Xu, L. Wei, J. D. Jiang, T. M. Block,J. T. Guo, and J. Chang. 2015. STING agonists induce an innate antiviral immuneresponse against hepatitis B virus. Antimicrob. Agents Chemother. 59: 1273–1281.
25. Hritz, I., P. Mandrekar, A. Velayudham, D. Catalano, A. Dolganiuc, K. Kodys,E. Kurt-Jones, and G. Szabo. 2008. The critical role of toll-like receptor (TLR) 4 inalcoholic liver disease is independent of the common TLR adapter MyD88. Hep-atology 48: 1224–1231.
26. Petrasek, J., A. Iracheta-Vellve, T. Csak, A. Satishchandran, K. Kodys, E. A. Kurt-Jones, K. A. Fitzgerald, and G. Szabo. 2013. STING-IRF3 pathway links endo-plasmic reticulum stress with hepatocyte apoptosis in early alcoholic liver disease.Proc. Natl. Acad. Sci. USA 110: 16544–16549.
27. Roychowdhury, S., M. R. McMullen, S. G. Pisano, X. Liu, and L. E. Nagy. 2013.Absence of receptor interacting protein kinase 3 prevents ethanol-induced liverinjury. Hepatology 57: 1773–1783.
28. Takemoto, K., E. Hatano, K. Iwaisako, M. Takeiri, N. Noma, S. Ohmae,K. Toriguchi, K. Tanabe, H. Tanaka, S. Seo, et al. 2014. Necrostatin-1 protectsagainst reactive oxygen species (ROS)-induced hepatotoxicity in acetaminophen-induced acute liver failure. FEBS Open Bio 4: 777–787.
29. Imaeda, A. B., A. Watanabe, M. A. Sohail, S. Mahmood, M. Mohamadnejad,F. S. Sutterwala, R. A. Flavell, and W. Z. Mehal. 2009. Acetaminophen-inducedhepatotoxicity in mice is dependent on Tlr9 and the Nalp3 inflammasome. J. Clin.Invest. 119: 305–314.
30. Li, S., R. Sun, Y. Chen, H. Wei, and Z. Tian. 2015. TLR2 limits development ofhepatocellular carcinoma by reducing IL18-mediated immunosuppression. CancerRes. 75: 986–995.
31. Lin, K. J., T. M. Lin, C. H. Wang, H. C. Liu, Y. L. Lin, and H. L. Eng. 2013.Down-regulation of Toll-like receptor 7 expression in hepatitis-virus-related humanhepatocellular carcinoma. Hum. Pathol. 44: 534–541.
20 BRIEF REVIEWS: HEPATOCYTE IMMUNOLOGY
by guest on February 2, 2019http://w
ww
.jimm
unol.org/D
ownloaded from

32. John, B., and I. N. Crispe. 2005. TLR-4 regulates CD8+ T cell trapping in the liver.J. Immunol. 175: 1643–1650.
33. Cani, P. D., S. Possemiers, T. Van de Wiele, Y. Guiot, A. Everard, O. Rottier,L. Geurts, D. Naslain, A. Neyrinck, D. M. Lambert, et al. 2009. Changes in gutmicrobiota control inflammation in obese mice through a mechanism involvingGLP-2-driven improvement of gut permeability. Gut 58: 1091–1103.
34. Lin, R., L. Zhou, J. Zhang, and B. Wang. 2015. Abnormal intestinal permeabilityand microbiota in patients with autoimmune hepatitis. Int. J. Clin. Exp. Pathol. 8:5153–5160.
35. Chou, H. H., W. H. Chien, L. L. Wu, C. H. Cheng, C. H. Chung, J. H. Horng,Y. H. Ni, H. T. Tseng, D. Wu, X. Lu, et al. 2015. Age-related immune clearance ofhepatitis B virus infection requires the establishment of gut microbiota. Proc. Natl.Acad. Sci. USA 112: 2175–2180.
36. Seki, E., and B. Schnabl. 2012. Role of innate immunity and the microbiota in liverfibrosis: crosstalk between the liver and gut. J. Physiol. 590: 447–458.
37. Fox, J. G., Y. Feng, E. J. Theve, A. R. Raczynski, J. L. Fiala, A. L. Doernte,M. Williams, J. L. McFaline, J. M. Essigmann, D. B. Schauer, et al. 2010. Gutmicrobes define liver cancer risk in mice exposed to chemical and viral transgenichepatocarcinogens. Gut 59: 88–97.
38. Wu, J., X. J. Zhang, K. Q. Shi, Y. P. Chen, Y. F. Ren, Y. J. Song, G. Li, Y. F. Xue,Y. X. Fang, Z. J. Deng, et al. 2014. Hepatitis B surface antigen inhibits MICA andMICB expression via induction of cellular miRNAs in hepatocellular carcinomacells. Carcinogenesis 35: 155–163.
39. Yanagisawa, K., S. Yue, H. J. van der Vliet, R. Wang, N. Alatrakchi, L. Golden-Mason, D. Schuppan, M. J. Koziel, H. R. Rosen, and M. A. Exley. 2013. Ex vivoanalysis of resident hepatic pro-inflammatory CD1d-reactive T cells and hepatocytesurface CD1d expression in hepatitis C. J. Viral Hepat. 20: 556–565.
40. Ishikawa, S., K. Ikejima, H. Yamagata, T. Aoyama, K. Kon, K. Arai, K. Takeda, andS. Watanabe. 2011. CD1d-restricted natural killer T cells contribute to hepaticinflammation and fibrogenesis in mice. J. Hepatol. 54: 1195–1204.
41. Sander, L. E., S. D. Sackett, U. Dierssen, N. Beraza, R. P. Linke, M. M€uller,J. M. Blander, F. Tacke, and C. Trautwein. 2010. Hepatic acute-phase proteinscontrol innate immune responses during infection by promoting myeloid-derivedsuppressor cell function. J. Exp. Med. 207: 1453–1464.
42. Yen, B. L., M. L. Yen, P. J. Hsu, K. J. Liu, C. J. Wang, C. H. Bai, and H. K. Sytwu.2013. Multipotent human mesenchymal stromal cells mediate expansion ofmyeloid-derived suppressor cells via hepatocyte growth factor/c-met and STAT3.Stem Cell Rep. 1: 139–151.
43. Warren, A., D. G. Le Couteur, R. Fraser, D. G. Bowen, G. W. McCaughan, andP. Bertolino. 2006. T lymphocytes interact with hepatocytes through fenestrationsin murine liver sinusoidal endothelial cells. Hepatology 44: 1182–1190.
44. Qian, S., Z. Wang, Y. Lee, Y. Chiang, C. Bonham, J. Fung, and L. Lu. 2001.Hepatocyte-induced apoptosis of activated T cells, a mechanism of liver transplanttolerance, is related to the expression of ICAM-1 and hepatic lectin. Transplant.Proc. 33: 226.
45. Ebrahimkhani, M. R., I. Mohar, and I. N. Crispe. 2011. Cross-presentation ofantigen by diverse subsets of murine liver cells. Hepatology 54: 1379–1387.
46. Bertolino, P., M. C. Trescol-Biemont, J. Thomas, B. Fazekas de St Groth,M. Pihlgren, J. Marvel, and C. Rabourdin-Combe. 1999. Death by neglect asa deletional mechanism of peripheral tolerance. Int. Immunol. 11: 1225–1238.
47. Benseler, V., A. Warren, M. Vo, L. E. Holz, S. S. Tay, D. G. Le Couteur, E. Breen,A. C. Allison, N. van Rooijen, C. McGuffog, et al. 2011. Hepatocyte entry leads todegradation of autoreactive CD8 T cells. Proc. Natl. Acad. Sci. USA 108: 16735–16740.
48. Radziewicz, H., C. C. Ibegbu, M. L. Fernandez, K. A. Workowski, K. Obideen,M. Wehbi, H. L. Hanson, J. P. Steinberg, D. Masopust, E. J. Wherry, et al. 2007.Liver-infiltrating lymphocytes in chronic human hepatitis C virus infection displayan exhausted phenotype with high levels of PD-1 and low levels of CD127 ex-pression. J. Virol. 81: 2545–2553.
49. Spahn, J., R. H. Pierce, and I. N. Crispe. 2011. Ineffective CD8(+) T-cell immunityto adeno-associated virus can result in prolonged liver injury and fibrogenesis. Am. J.Pathol. 179: 2370–2381.
50. Tay, S. S., Y. C. Wong, D. M. McDonald, N. A. Wood, B. Roediger, F. Sierro,C. Mcguffog, I. E. Alexander, G. A. Bishop, J. R. Gamble, et al. 2014. Antigenexpression level threshold tunes the fate of CD8 T cells during primary hepaticimmune responses. Proc. Natl. Acad. Sci. USA 111: E2540–E2549.
51. Ando, K., L. G. Guidotti, S. Wirth, T. Ishikawa, G. Missale, T. Moriyama,R. D. Schreiber, H. J. Schlicht, S. N. Huang, and F. V. Chisari. 1994. Class I-restricted cytotoxic T lymphocytes are directly cytopathic for their target cells invivo. J. Immunol. 152: 3245–3253.
52. Smith, C. M., N. S. Wilson, J. Waithman, J. A. Villadangos, F. R. Carbone,W. R. Heath, and G. T. Belz. 2004. Cognate CD4(+) T cell licensing of dendriticcells in CD8(+) T cell immunity. Nat. Immunol. 5: 1143–1148.
53. Crispe, I. N. 2014. APC licensing and CD4+ T cell help in liver-stage malaria.Front. Microbiol. 5: 617.
54. Dini, L., F. Autuori, A. Lentini, S. Oliverio, and M. Piacentini. 1992. The clearanceof apoptotic cells in the liver is mediated by the asialoglycoprotein receptor. FEBSLett. 296: 174–178.
55. Wuensch, S. A., J. Spahn, and I. N. Crispe. 2010. Direct, help-independentpriming of CD8+ T cells by adeno-associated virus-transduced hepatocytes. Hepa-tology 52: 1068–1077.
The Journal of Immunology 21
by guest on February 2, 2019http://w
ww
.jimm
unol.org/D
ownloaded from