Hepatic Involvement in Pediatric Patients with Paracoccidioidomycosis: A Clinical and Laboratory...
8
Hepatic Involvement in Pediatric Patients with Paracoccidioidomycosis: A Clinical and Laboratory Study Giselle de Melo Braga • Gabriel Hessel • Ricardo Mendes Pereira Received: 28 August 2012 / Accepted: 22 July 2013 / Published online: 6 August 2013 Ó Springer Science+Business Media Dordrecht 2013 Abstract The liver is one of the organs most affected by paracoccidioidomycosis, a systemic mycosis ende- mic in some Latin American countries. The majority of articles focused on adult populations and failed to describe any detailed experience of liver abnormalities in pediatric patients. Therefore, the aim of this study was to describe the frequency and characteristics of liver involvement in children with paracoccidioido- mycosis. This study comprised 102 patients less than 16 years of age (median 104.3 months) diagnosed with paracoccidioidomycosis from 1980 to 2010. Diagnosis was established by the identification of fungus. Forty- one patients had liver involvement. The main clinical features were generalized lymph node enlargement (39/41), weight loss (34/41) and fever 32/41). Approx- imately, one-third of the patients had jaundice. Patients with hepatic involvement were younger. A predomi- nant elevation of canalicular enzymes occurred. There was a statistically significant difference in albumin (p \ 0.001) and hemoglobin (p = 0.002) values between patients with and without liver involvement, and the lowest values were found in the former group. Cutoff levels of albumin ( \ 3.05 g/dL) and hemoglobin ( \ 9.2 g/dL) can be used to infer hepatic involvement. Hypoalbuminemia (median 2.4 g/dl) is more severe in patients with hepatic involvement and may indicate a worse liver function or complication of the disease (intestinal lymphangiectasia). Deaths (6) occurred only among patients with liver involvement. Particular clinical and laboratory characteristics are present in pediatric patients with hepatic involvement. Younger patients and those with severe hypoalbuminemia are more likely to present liver involvement by Paracoc- cidioides brasiliensis. Keywords Paracoccidioidomycosis Á Paracoccidioides brasiliensis Á Liver Á Pediatrics Á Children Á Serum albumin Introduction Paracoccidioidomycosis (PCM) is the eighth leading cause of death from chronic infectious and parasitic diseases with the highest mortality rate among systemic mycoses in Brazil [1]. It is a systemic mycosis caused by a thermally dimorphic fungus [2] that occurs only in Latin America. Brazil has the highest incidence of the disease [3, 4]. The etiological agent of PCM, Paracoccidioides brasiliensis (P. brasiliensis), is a cryptic species complex. It is composed of at least four different phylogenetic, potentially human pathogenic lineages (S1, PS2 and G. de Melo Braga (&) Center for Investigation in Pediatrics, UNICAMP School of Medicine, Campinas, Sa ˜o Paulo, Brazil e-mail: [email protected] G. Hessel Á R. M. Pereira Department of Pediatrics, UNICAMP School of Medicine, Sa ˜o Paulo, Brazil 123 Mycopathologia (2013) 176:279–286 DOI 10.1007/s11046-013-9682-8
-
Upload
ricardo-mendes -
Category
Documents
-
view
214 -
download
0
Transcript of Hepatic Involvement in Pediatric Patients with Paracoccidioidomycosis: A Clinical and Laboratory...

Hepatic Involvement in Pediatric Patientswith Paracoccidioidomycosis: A Clinicaland Laboratory Study
Giselle de Melo Braga • Gabriel Hessel •
Ricardo Mendes Pereira
Received: 28 August 2012 / Accepted: 22 July 2013 / Published online: 6 August 2013
� Springer Science+Business Media Dordrecht 2013
Abstract The liver is one of the organs most affected
by paracoccidioidomycosis, a systemic mycosis ende-
mic in some Latin American countries. The majority of
articles focused on adult populations and failed to
describe any detailed experience of liver abnormalities
in pediatric patients. Therefore, the aim of this study
was to describe the frequency and characteristics of
liver involvement in children with paracoccidioido-
mycosis. This study comprised 102 patients less than
16 years of age (median 104.3 months) diagnosed with
paracoccidioidomycosis from 1980 to 2010. Diagnosis
was established by the identification of fungus. Forty-
one patients had liver involvement. The main clinical
features were generalized lymph node enlargement
(39/41), weight loss (34/41) and fever 32/41). Approx-
imately, one-third of the patients had jaundice. Patients
with hepatic involvement were younger. A predomi-
nant elevation of canalicular enzymes occurred. There
was a statistically significant difference in albumin
(p \ 0.001) and hemoglobin (p = 0.002) values
between patients with and without liver involvement,
and the lowest values were found in the former group.
Cutoff levels of albumin (\3.05 g/dL) and hemoglobin
(\9.2 g/dL) can be used to infer hepatic involvement.
Hypoalbuminemia (median 2.4 g/dl) is more severe in
patients with hepatic involvement and may indicate a
worse liver function or complication of the disease
(intestinal lymphangiectasia). Deaths (6) occurred
only among patients with liver involvement. Particular
clinical and laboratory characteristics are present in
pediatric patients with hepatic involvement. Younger
patients and those with severe hypoalbuminemia are
more likely to present liver involvement by Paracoc-
cidioides brasiliensis.
Keywords Paracoccidioidomycosis �Paracoccidioides brasiliensis � Liver � Pediatrics �Children � Serum albumin
Introduction
Paracoccidioidomycosis (PCM) is the eighth leading
cause of death from chronic infectious and parasitic
diseases with the highest mortality rate among
systemic mycoses in Brazil [1]. It is a systemic
mycosis caused by a thermally dimorphic fungus [2]
that occurs only in Latin America. Brazil has the
highest incidence of the disease [3, 4]. The etiological
agent of PCM, Paracoccidioides brasiliensis
(P. brasiliensis), is a cryptic species complex. It is
composed of at least four different phylogenetic,
potentially human pathogenic lineages (S1, PS2 and
G. de Melo Braga (&)
Center for Investigation in Pediatrics, UNICAMP School
of Medicine, Campinas, Sao Paulo, Brazil
e-mail: [email protected]
G. Hessel � R. M. Pereira
Department of Pediatrics, UNICAMP School
of Medicine, Sao Paulo, Brazil
123
Mycopathologia (2013) 176:279–286
DOI 10.1007/s11046-013-9682-8

PS3, from the P. brasiliensis complex, and Paracoc-
cidioides lutzii—P. lutzii) [5–8]. S1 is the most widely
distributed species occurring in Brazil, Argentina,
Paraguay, Uruguay, Peru and Venezuela. PS2 occurs
in Venezuela and Brazil. PS3 is restricted to Colombia
and P. lutzii, occurs predominantly in the west central
region of Brazil [7, 8]. The PCM disease has two types
of manifestations: acute (juvenile) and chronic (adult).
The former accounts for less than 10 % of cases [2, 9,
10], affecting predominantly children and adolescents.
It can also affect individuals up to 35 years of age.
Gender distribution is similar, but there may be a slight
male predominance among young adults [10].
Involvement of the abdominal organs is most
frequent in children and young adults. The most
exuberant lesions are found in a form called lymph-
abdominal disease [4]. Autopsy studies have shown
that the liver is one of the organs most affected by
paracoccidioidomycosis [11–15].
Although liver involvement is more common in
children and young adults [10, 15–19], there is no
detailed study of liver involvement in the pediatric
population. Furthermore, PCM is not a disease of
compulsory notification, making the acquisition and
access to clinical and epidemiological data more
difficult. The present study aimed to describe clinical
and laboratory features of hepatic involvement by
paracoccidioidomycosis in pediatric patients.
Materials and Methods
This study comprised all patients under the age of
16 years diagnosed with PCM, managed at the UNI-
CAMP Teaching Hospital from January 1980 to
September 2007 (retrospective/96 patients) and new
cases from October 1, 2007 to April 31, 2010
(prospective/6 patients). Inclusion criterion consisted
of the diagnosis of paracoccidioidomycosis, estab-
lished by the detection of fungus in pathological
examination (lymph node, liver, bone, skin or bone
marrow) or cultures of pulmonary secretions or lymph
node fistulization. Exclusion criterion consisted of
cases associated with other diseases leading to liver
involvement or immunodeficiency, namely acquired
immunodeficiency syndrome caused by HIV. Cases of
HIV-related immunodeficiency were not included to
evaluate the clinical and laboratory features attribut-
able only to P. brasiliensis and not to the underlying
disease. We based the definition of hepatic involve-
ment on laboratory criteria because few patients
underwent liver biopsy (the gold standard for identi-
fication of liver involvement). Furthermore, the indi-
cation of liver biopsy occurred in a small number of
patients.
Hepatic involvement was defined as increased
levels of one or more liver enzymes (AST—aspartate
aminotransferase, ALT—alanine aminotransferase,
AF—alkaline phosphatase or GGT—gamma-glutam-
yltransferase). Elevation of alkaline phosphatase was
considered only if associated with an increased level
of any of the other three enzymes, due to the
possibility of bone involvement.
Enzyme level was considered elevated when
patient values were above the reference value used
by the Clinical Pathology laboratory of the Unicamp
Clinics Hospital at the time of blood sample collec-
tion. Hypoalbuminemia was defined as serum albumin
lower than 3.2 g/dL and hypergammaglobulinemia as
gamma globulin level higher than 2.1 g/dL.
We used the Gomez criteria to assess nutritional
status [20]:
• Normal Weight: Weight = 90–110 % of median
weight for chronological age
• Mild Malnutrition (grade I): Weight \90 % of
median weight for chronological age
• Moderate Malnutrition (grade II): Weight \75 %
of median weight for chronological age
• Severe Malnutrition (grade III): Weight \60 % of
median weight for chronological age
Concerning clinical and laboratory data at the time
of admission, this was a descriptive, analytical and
cross-sectional study. Follow-up data were also
obtained regarding clinical course and laboratory
tests. Registration of medical charts allowed for data
collection.
Logistic regression analysis with univariate and
stepwise multiple regression models for variable
criteria selection was used to analyze risk factors for
hepatic involvement. The receiver operating charac-
teristic curve (ROC curve) was used to obtain cutoff
values for baseline laboratory measurements to dif-
ferentiate between the presence and absence of liver
involvement. We used analysis of variance (ANOVA)
for repeated measures to compare numerical variables
related to laboratory tests between the two groups and
among the three sampling time periods (T0 at hospital
280 Mycopathologia (2013) 176:279–286
123

admission, T1 at 1 month of treatment and T6 at
6 months of treatment), followed by post hoc Turkey’s
multiple comparison to compare two groups at any
given time, and the contrast profile test to analyze
clinical course at the three time periods in each group.
The variables were transformed into ranks in the
absence of normal distribution. We used the Statistical
Package for Social Sciences (SPSS) for Windows
Institute Inc, 1989–1999, Chicago, IL, USA.), version
10.0.7, for database registration and preparation of
charts and graphs. The computer program Statistical
Analysis System (SAS) for Windows (Institute Inc,
2002–2003, Cary, NC, USA), version 9.1.3, was used
for statistical analysis. The significance level for
statistical tests was 5 % (p \ 0.05), and the confidence
interval was 95 % (when the confidence interval
contains the value one, the result is not statisti-
cally significant). The project was approved by
the Research Ethics Committee, under SISNEP
(CAAE-0493.0.146.000-07).
Results
From 1980 to 2010, 102 patients under age 16 were
diagnosed with paracoccidioidomycosis and received
follow-up care. Of these patients, 41 (40.1 %) had
liver involvement.
The main complaint was generalized lymph node
enlargement (25/41), followed by fever (6/41),
abdominal pain (3/41), increased abdominal size (2/
41), jaundice (2/41), asthenia (1/41), osteoarticular
pain (1/41) and diarrhea (1/41). Major clinical man-
ifestations were as follows: generalized lymphade-
nopathy (39/41 patients), weight loss (34/41) and fever
(32/41). Hepatomegaly was detected by physical
examination in 28/41 patients. The other clinical
manifestations observed were as follows: asthenia (26/
41), splenomegaly (24/41), pallor (23/41), anorexia
(19/41), skin and mucosal lesions (11/41), osteoartic-
ular symptoms (6/41), cough (3/41), edema (3/41),
lymph node fistulization (2/41) and localized lym-
phadenopathy (1/41). Approximately, one-third of the
patients (12/41) had jaundice. The only case of
bleeding disorder in this case series occurred in
patients with hepatic compromise. Ascites was infre-
quent (3/41). All patients with liver involvement had
an impaired lymphatic system (41/41). The spleen was
the second most affected organ (32/41). Other organs
or systems involved were as follows: the mucocuta-
neous tissue (13/41), osteoarticular tissue (11/41),
bone marrow (6/41), lungs (4/41), kidneys (2/41),
adrenals (1/41), tonsils (1/41), epiglottis (1/41), myo-
cardial infarction (1/41), pancreas (1/41) and testis (1/41).
Abdominal ultrasonography was performed in 34
patients: 27/34 had hepatomegaly, 23/34 had spleno-
megaly, 29/34 had adenopathy and one patient had a
normal examination. Eight patients with abdominal
adenopathy had jaundice, without bile duct dilatation.
Two deaths were recorded in patients with abdominal
adenopathy, and jaundice was associated in one of
these cases.
We present the frequency of altered levels of AST,
ALT, FALC, BD, albumin and gamma globulin in
patients with paracoccidioidomycosis and liver
involvement (Table 1).
Trimethoprim–sulfamethoxazole was the main drug
used for treatment, in both study groups, with or without
hepatic involvement. In the former group, a single-drug
treatment with trimethoprim–sulfamethoxazole was
given to 26/41 patients. An association with amphoter-
icin B, ketoconazole or itraconazole was required in
13/41 cases. The remaining patients (n = 2/41) received
a single-drug treatment with amphotericin B. Multiple-
drug treatment was more frequent in patients with liver
involvement (p\0.001).
We compared the clinical and laboratory charac-
teristics of patients with and without liver involvement
in Table 2.
Regarding the period from clinical progression to
death, univariate logistic regression analysis was
associated with liver involvement (OR = 22.52; CI
1.23–411.75) and albumin level at the time of
Table 1 Frequency of abnormal values of AST, ALT, FALC,
BD, albumin and gamma globulin in patients with paracoc-
cidioidomycosis and liver involvement
N %
Increased AST 12/33 36.4
Increased ALT 13/33 39.4
Increased FALC 25/33 75.7
Increased GGT 19/24 79.2
Increased BD 10/14 71.4
Hypoalbuminemia 36/39 92.3
Hypergammaglobulinemia 27/30 90.0
Mycopathologia (2013) 176:279–286 281
123

admission (OR = 0.154; CI 0.027–0.881). Multivar-
iate logistic regression analysis showed an association
with liver involvement; there was a 19.6-fold increase
in the risk of death. This analysis should be viewed
carefully because of the limited number of deaths in
this case series.
On univariate logistic regression analysis of liver
involvement, the variables malnutrition (p = 0.005),
age (p = 0.008), albumin (p \ 0.001) and hemoglobin
(p = 0.003) at baseline were statistically significant.
The results of multivariate logistic regression
analysis showed that baseline albumin levels, age
and malnutrition were associated with liver involve-
ment. Each 1-g/dL increase in baseline albumin levels
decreased the risk of liver involvement by 77.9 % or
each 1-g/dL decrease in baseline albumin levels
increased the risk of liver involvement by 4.5 times
(OR = 0.22; CI 0.085–0.571). Each 1-year increase in
age decreased the risk of liver involvement by 29.5 %
or any 1-year decrease in age increased the risk of liver
involvement by 41.8 % (OR = 0.75, CI 0.556–0.895).
Malnourished patients have a 5.5-fold higher risk of
liver involvement (OR = 5.51, CI 1.36–22.39).
It was possible to establish cutoff levels to deter-
mine the values of albumin, hemoglobin and lympho-
cyte with the highest probability of liver involvement
(albumin B3.05 g/dL, hemoglobin B9.2 g/dL and
lymphocytes B2,508/mm3).
The sensitivity of albumin for the diagnosis of
hepatic involvement is 82.1 %. The sensitivity of
Table 2 Comparison of clinical and laboratory variables between patients suffering from paracoccidioidomycosis, with and without
liver involvement, at time of admission
N Without liver
involvement
N With liver
involvement
p
Age (years) 61 9.5 ± 3.0 41 7.8 ± 2.5 0.009
Male gender 61 54 % 41 68.3 % 0.152
Time from onset of symptoms to diagnosis (days) 61 84.4 ± 82.3 41 82.9 ± 77.7 0.82
Malnutrition 59 52.5 % 41 80.5 % 0.008
Weight loss 61 60.6 % 41 82.9 % 0.029
Adynamia 61 36.0 % 41 63.4 % 0.012
Anorexia 61 18.6 % 41 46.3 % 0.0043
Pallor 61 11.5 % 41 56.1 % \0.001
Splenomegaly 61 3.3 % 41 58.5 % \0.001
Trimethoprim–sulfamethoxazole as single treatment 61 91.8 % 41 63.4 % \0.001
Deaths 61 0 41 6 0.002
Abdominal adenopathy 49 69.5 % 39 85 % 0.04
Hemoglobin g/dL 61 10.05 ± 1,9 41 8.8 ± 1.8 0.002
Leukocyte count/mm3 61 14194.4 ± 9378.9 41 14600 ± 8876.8 0.64
Lymphocyte count/mm3 61 2976.1 ± 1456.1 41 2399.5 ± 1764 0.003
Platelet count/mm3 60 405150 ± 178617 41 321951.2 ± 185441 0.023
Eosinophil count/mm3 61 2652 ± 4680 41 2427.5 ± 3256.6 0.78
Alpha-1 globulin g/dL 50 0.37 ± 0.11 30 0.45 ± 0.12 0.001
Alpha-2 globulin g/dL 49 0.96 ± 0.23 30 0.97 ± 0.29 0.91
Beta globulin g/dL 49 0.88 ± 0.21 30 0.79 ± 0.29 0.07
Albumin g/dL 61 3.1 ± 0.71 39 2.5 ± 0.6 \0.001
Gamma globulin g/dL 49 3.1 ± 1.12 30 3.4 ± 1.2 0.57
AST (U/L) 23 17.52 ± 10.34 33 47.6 ± 45.9 0.009
ALT (U/L) 23 14.83 ± 10.16 33 47.5 ± 53.8 0.003
AF (U/L) 19 440.74 ± 279.62 33 1119.7 ± 1168.3 0.019
GGT (U/L) 13 32.77 ± 36.32 24 262.9 ± 229.4 \0.001
BD (mg/dL) 5 0.14 14 2.9 ± 5.4 0.006
282 Mycopathologia (2013) 176:279–286
123

hemoglobin is 65.9 %, and lymphocytes have a
sensitivity of 70.7 %. The specificity for these vari-
ables is 59, 68.9 and 57.4 %, respectively. If albumin
is lower than 3.05 g/dL and hemoglobin is lower than
9.2 g/dL, the sensitivity for hepatic involvement is
61.54 % and specificity is 77.05 % (p \ 0.001).
We compared the laboratory measurements of
interest between groups with and without liver
involvement and among the three sampling time
periods (T0, T1 and T6). Only the data from patients
who had test samples in all three time periods were
computed.
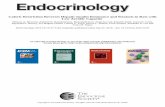
The results were shown in Fig. 1. Briefly, hemo-
globin levels were significantly lower in patients with
liver involvement at all times. Hemoglobin had a trend
toward normalization in both groups, which is statis-
tically demonstrated at the time of admission. In
patients with liver involvement, this trend was signif-
icant for albumin and gamma globulin only at a later
time, after T1. Regarding leukocyte and eosinophil
counts, the downward trend can only be statistically
demonstrated in the group without liver involvement.
Concerning lymphocyte count, clinical course occurs
in opposite directions: a decline in the group without
liver involvement and a rise in patients with liver
involvement.
Discussion
Paracoccidioidomycosis was highly endemic in the
area where our patients acquired the disease [21, 31].
S1 and PS2 lineages of P. brasiliensis were isolated
from these areas [5, 6, 8]. Two major pediatric case
series originated in the state of Sao Paulo: the present
study and a study by Bellissimo-Rodrigues [21]. Only
few studies to date explore the clinical characteristics
of paracoccidioidomycosis in the pediatric population.
None of the previous pediatric case series [22–29],
acute/subacute cases [30] or those including all age
groups [15, 30–32] of paracoccidioidomycosis had a
larger number of pediatric patients than the two above-
mentioned case series.
Description of the frequency of hepatic involve-
ment in our study based on laboratory criteria is
relevant, in view of the size of this pediatric case
series. Furthermore, PCM is not a disease of compul-
sory notification in Brazil, hindering the acquisition of
clinical and epidemiological data.
The most common main complaint in our study was
lymphadenopathy, followed by fever and abdominal
pain. The same complaints were also observed by
other authors investigating PCM, PCM in children and
acute/subacute PCM [22, 24, 27, 28, 30]. The most
frequent clinical manifestations of this study are also
identified by other studies on paracoccidioidomycosis
in children and acute/subacute PCM: lymphadenopa-
thy, weight loss and fever [22, 24, 26–28, 30].
Abdominal ultrasonographic findings are similar to
other studies on acute PCM. Barbosa [22] and Ferreira
[30] described lymphadenopathy, hepatosplenomeg-
aly and one case of bile duct dilatation [22, 30]. A
frequent association between abdominal adenopathy
and hepatic involvement (p = 0.04) was expected.
Contamination in the liver with P. brasiliensis may
occur by lymphatic–hematogenous dissemination
from other tissues, particularly abdominal or by
contiguous invasion [4]. Although 8/12 icteric patients
had abdominal adenopathy, it is likely that lymph node
compression of major bile ducts was not the predom-
inant cause, since there was no report of bile duct
dilatation. Mechanisms responsible for jaundice in
PCM may be extrahepatic biliary tract obstruction
(choledocus infiltration by granulomas, extrinsic
compression by abdominal lymph nodes or choledo-
cus retraction due to fibrosis) or granulomatous
hepatitis. [15, 16]. Histopathological examination of
the liver shows a predominantly portal granulomatous
process, and interlobar bile duct compression with
cholestasis may be present in the periphery [4, 33].
Statistical differences were found in some clinical
variables evaluated in a comparison between patients
with and without liver involvement. Liver involve-
ment occurred in younger patients. The clinical
presentation was shown to be more exuberant in
patients with liver involvement, with a high percent-
age of malnourished individuals and increased rate of
complaints such as weight loss, malaise, anorexia and
pallor. However, this was not associated with a shorter
period between onset of complaints and diagnosis. A
common complaint of pallor can be correlated with a
lower mean hemoglobin level in patients with hepatic
involvement. A study showed that malnutrition is an
important factor contributing to death by paracoccid-
ioidomycosis [34].
Hepatomegaly is described in paracoccidioidomy-
cosis, ranging in frequency from 41.6 to 71.1 % in
both studies restricted to children/adolescents and also
Mycopathologia (2013) 176:279–286 283
123

studies evaluating the acute/subacute form of the
disease [16, 22, 24, 26, 28, 30]. The frequency of
hepatic involvement in this study is in agreement with
necropsy studies that are not restricted to the pediatric
population, whose proportion of liver injury ranges
from 21 to 56.7 % [4, 35].
Different results between groups at each time - T0, T1 and T6 (p= 0.002)
Different results over the period in both groups - T0≠T1, T0≠T6 (p=0.001)
T0 T1 T60
1
2
3
4
5
6Without liver involvement.With liver involvement.
Time
T0 T1 T61
2
3
4
5
Without liver involvementWith liver involvement.
Alb
umin
Time
T0 T1 T6
-2000
0
2000
4000
6000
8000
10000
Without liver involvement.With liver involvement.
Eos
inop
hils
Time
T0 T60
1000
2000
3000
4000
5000
6000
Without liver involvementWith liver involvement
Time
T0 T1 T60
5000
10000
15000
20000
25000
30000Without liver involvement.With liver involvement
Leuk
ocyt
es
Time
T0 T1 T66789
1011121314
Without liver involvement.With liver involvement
Hem
oglo
bin
Time
Lym
phoc
ytes
Gam
ma-
glob
ulin
Different results between groups at T6 and different results over the period in group without liver involvement ( ≠ ≠ and in group with liver involvement ≠ (p<0.001)
Different results between groups at T1 and T6 (p= 0.002)
Different results over the period only in group without liver involvement - T0≠T1, T0≠T6 (p<0.001)
Different results over the period only in group without liver involvement (T0≠T1, T0≠T6, T1≠T6); (p<0.001)
Different results over the period in group without liver involvement (T0≠T1, T0≠T6, T1≠T6); and in group with liver involvement ( ≠
≠ ). (p<0.001)
Different results between groups at T1 and T6 (p= 0.002)
Different results over the period in group without liver involvement (T0 ≠T1, T0≠T6, T1≠T6); and in group with liver involvement (T1≠T6). (p<0.001)
Fig. 1 Comparison and follow-up of hemoglobin, albumin and gamma globulin and leukocyte, lymphocyte and eosinophil counts in
patients with and without liver involvement at T0, T1 and T6
284 Mycopathologia (2013) 176:279–286
123

Similar to the study results found by other authors,
our study showed anemia, eosinophilia, hypoalbumi-
nemia and hypergammaglobulinemia [22, 27, 30, 35,
36]. Factors associated with anemia in PCM may be a
direct action of P. brasiliensis on the bone marrow,
malnutrition, loss of nutrients by intestinal involve-
ment and myelotoxicity related to amphotericin B use.
Some authors assume that the frequent association
between PCM and intestinal parasitic disease may
contribute to anemia [30]. A higher percentage of
malnourished patients with hepatic involvement,
showing statistical difference, may be related to more
severe anemia in this group. Other factors can explain
anemia in chronic liver disease, such as folate
deficiency, hypersplenism, hemodilution, hemolysis
and bleeding esophageal varices [37].
There was a predominant increase in canalicular
enzymes in patients with hepatic involvement. Similar
to other studies, aminotransferase elevations are milder
and less frequent. Increased levels of aminotransferases
may be due to the damaging effect of bile retention or
the direct action of the fungus or its products and
granuloma on the hepatocyte [30, 35, 36].
Lower albumin values in patients with hepatic
involvement did not arise simply because of the
presence of P. brasiliensis in those individuals.
Hypoalbuminemia may be indicative of liver dys-
function. Another possible cause and aggravating
factor of hypoalbuminemia is intestinal lymphangiec-
tasia as a complication of the disease [38].
A higher proportion of multiple-drug treatment in
patients with liver involvement may indicate greater
disease severity in these cases. Furthermore, all six
deaths occurred in patients with hepatic involvement.
Cutoff levels for simple laboratory tests such as
hemoglobin, albumin and lymphocyte count can help
in the diagnosis of hepatic involvement, even without
the performance of invasive tests (such as liver
biopsy). Young patients can receive proper clinical
care, since hepatic involvement is associated with a
greater risk of severe disease and a worse prognosis
(either by impairment of liver functions or as a marker
of disseminated disease).
As observed in other studies not limited to pediatric
patients, hepatic involvement associated with jaundice
may lead to a worse prognosis [15, 16]. The initial
follow-up of pediatric patients with paracoccidioido-
mycosis and liver involvement should be frequent
(weekly) because clinical and laboratory presentations
are more severe with an increased risk of death.
References
1. Coutinho ZF, Silva D, Lazera M, Petri V, Oliveira RM,
Sabroza PC, Wanke B. Paracoccidioidomycosis mortality in
Brazil (1980–1995). Cad Saude Publica. 2002;18:1441–54.
2. Moreira APV. Paracoccidioidomicose: historico, etiologia,
epidemiologia, patogenese, formas clınicas, diagnostico labo-
ratorial e antıgenos. Bol Epidemiol Paul. 2008;51:11–24.
3. Brummer E, Castaneda E, Restrepo A. Paracoccidioido-
mycosis: an update. Clin Microbiol Rev. 1993;6:89–117.
4. Del-Negro G, Lacaz CS, Fiorillo AM, editors. Paracoccid-
ioidomicose (Blastomicose sul-americana). Sarvier-Edusp:
Sao Paulo; 1982.
5. Matute DR, McEween JG, Montes BA, San-Blas G, Bagagli
E, Rauscher JT, Restrepo A, Morais F, Nino-Vega G, Taylor
JW. Cryptic speciation and recombination in the fungus
Paracoccidioides brasiliensis as revealed by gene geneal-
ogies. Mol Biol Evol. 2006;23:65–73.
6. Carrero LL, Nino-Vega G, Teixeira MM, Carvalho MJ,
Soares CM, Pereira M, Jesuino RS, McEwen JG, Mendoza
L, Taylor JW, Felipe MS, San-Blas G. New Paracoccidi-
oides brasiliensis isolate reveals unexpected genomic var-
iability in this human pathogen. Fungal Genet Biol.
2008;45:605–12.
7. Teixeira MM, Theodoro RC, Carvalho MJ, Fernandes L,
Paes HC, Hahn RC, Mendoza L, Bagagli E, San-Blas G,
Felipe MS. Phylogenetic analysis reveals a high level of
speciation in the Paracoccidioides genus. Mol Phylogenet
Evol. 2009;52:273–83.
8. Theodoro RC, Teixeira Mde M, Felipe MS, Paduan Kdos S,
Ribolla PM, San-Blas G, Bagagli E. Genus paracoccidioi-
des: species recognition and biogeographic aspects. PLoS
One. 2012;. doi:10.1371/journal.pone.0037694.
9. Franco M, Montenegro MR, Mendes RP, Marques SA,
Dillon ML, Mota NGS. Paracoccidioidomycosis: a recently
proposed classification of its clinical forms. Rev Soc Bras
Med Trop. 1987;20:129–32.
10. Shikanai-Yasuda MA, Telles Filho FQ, Mendes RP,
Colombo AL, Moretti ML. Guidelines in paracoccidioido-
mycosis. Rev Soc Bras Med Trop. 2006;39:297–310.
11. Pinto HB. La paracoccidiodosis brasiliensis como en-
fermedad sistemica. Comentarios a la casuistica venezol-
ana. Mycopathologia. 1961;15:90–114.
12. Pena CE. Deep mycotic infections in Colombia. A clini-
copathologic study of 162 cases. Am J Clin Path. 1967;
47:505–20.
13. Raphael A, Campana AO, Waimann J. Coma hepatico na bla-
stomicose sul-americana. Rev Ass Med Bras. 1964;10:151–4.
14. Teixeira F, Gayotto LC, Brito T. Morphological patterns of
the liver in South American blastomycosis. Histopathology.
1978;2:231–7.
15. Boccalandro I, Albuquerque FJM. Icterıcia e comprometi-
mento hepatico na blastomicose sul-americana. A proposito
de 10 casos. Rev Paul Med. 1960;56:350–66.
Mycopathologia (2013) 176:279–286 285
123

16. Daher RR, Vasconcelos WMP, Cardoso VM. Fıgado e a
blastomicose sul-americana. J Bras Med. 1973;25:83–90.
17. Marques SA. Paracoccidioimycosis: epidemiological, clin-
ical and treatment up-date. An Bras Dermatol. 2003;78:
135–50.
18. Campos MV, Penna GO, Castro CN, Moraes MA, Ferreira
MS, Santos JB. Paracoccidioidomycosis at Brasilias uni-
versity hospital. Rev Soc Bras Med Trop. 2008;41:169–72.
19. Paniago AM, Aguiar JI, Aguiar ES, da Cunha RV, Pereira
GR, Londero AT, Wanke B. Paracoccidioidomycosis: a
clinical and epidemiological study of 422 cases observed in
Mato Grosso do Sul. Rev Soc Bras Med Trop. 2003;
36:455–9.
20. Gomez F. Desnutricion. Bol Med Hosp Infant Mex.
1946;3:543–51.
21. Bellissimo-Rodrigues F, Machado AA, Martinez R. Para-
coccidioidomycosis epidemiological features of a 1,000-
cases series from a hyperendemic area on the southeast of
Brazil. Am J Trop Med Hyg. 2011;85:546–50.
22. Barbosa GL. Paracoccidioidomicose na crianca. Rev Pat
Trop. 1992;21:269–383.
23. Castro RM, Del Negro G. Particularidades clınicas da
paracoccidioidomicose na crianca. Rev Hosp Clin Fac Med
Sao Paulo. 1976;31:194–8.
24. Fonseca ERS, Pardal PPO, Severo LC. Paracoccidioidom-
icose em criancas em Belem do Para. Rev Soc Bras Med
Trop. 1999;32:31–3.
25. Pereira RM, Bucaretchi F, Barison Ede M, Hessel G, Tre-
soldi AT. Paracoccidioidomycosis in children: clinical
presentation, follow-up and outcome. Rev Inst Med Trop
Sao Paulo. 2004;46:127–31.
26. Londero AT, Goncalves AJR, Cruz MLS, Rozembaum R,
Cunha RQ, Machado ES, Viera ARM, Carvalho FG, Braga
MP, Azevedo ECL, Wanke B, Cruz MFF, Menezes JA.
Paracoccidioidomicose disseminada ‘‘infanto-juvenil’’ em
adolescentes. Relato de quatro casos e revisao da literatura.
Arq Bras Med. 1987;61:5–12.
27. Londero AT, Goncalves AJR, Terra GMF, Nogueira SA.
Paracoccidiodomycosis in Brazilian children. A critical
review (1911-1994). Arq Bras Med. 1996;70:197–203.
28. Nogueira MGS, Andrade GMQ, Tonelli E. Clinical evolu-
tion of paracoccidioidomycosis in 38 children and teenag-
ers. Mycopathologia. 2006;161:73–81.
29. Terra GMF, Rios-Goncalves AJ, Londero AT, Braga MP,
Ouricuri AL, Mesquita CC, Marino JCA, Ervilha LM,
Vieira ARM, Deker-Macher S, Duarte DMA. Paracoccidi-
oidomicose em criancas. Apresentacao de casos. Arq Bras
Med. 1991;65:8–15.
30. Ferreira MS. Contribuicao para o estudo clınico-laboratorial
e terapeutico da formacao juvenil da paracoccidioidomi-
cose. Rev Pat Trop. 1993;22:267–406.
31. Blotta MH, Mamoni RL, Oliveira SJ, Nouer SA, Papai-
ordanou PM, Goveia A, Camargo ZP. Endemic regions of
paracoccidioidomycosis in Brazil: a clinical and epidemi-
ologic study of 584 cases in the southeast region. Am J Trop
Med Hyg. 1999;61:390–4.
32. Valle ACP. Tratamento da paracoccidioidomicose: estudo
retrospectivo de 500 casos Analise clınica, laboratorial e
epidemiologica. An Bras Derm. 1992;67:251–4.
33. Brito T, Castro RM, Shiroma M. Biopsia hepatica na bla-
stomicose sul-americana. Rev Inst Med Trop Sao Paulo.
1968;10:188–91.
34. Santo AH. Tendencia da mortalidade relacionada a para-coccidioidomicose, Estado de Sao Paulo, Brasil, 1985 a
2005: estudo usando causas multiplas de morte. Rev Panam
Salud Publica. 2008;23:313–23.
35. Hildebrand TM, Rosario Filho NA, Telles Filho FQ, Costa
O, Miasaki N, Miyaki M. Paracoccidioidomicose na cri-
anca: aspectos clınicos-laboratoriais em 25 casos. J Ped.
1987;63:92–6.
36. Nogueira MGS, Andrade GMQ, Tonelli E, Diniz SN, Goes
AM, Cisalpino PS. Aspectos laboratoriais evolutivos de
criancas em tratamento da paracoccidioidomicose. Rev Soc
Bras Med Trop. 2006;39:478–83.
37. Gonzalez-Casas R, Jones EA, Moreno-Otero R. Spectrum
of anemia associated with chronic liver disease. World J
Gastroenterol. 2009;15:4653–8.
38. Troncon LE, Martinez R, Meneghelli UG, De Oliveira RB,
Iazigi N. Protein-losing enteropathy in paracoccidioidomyco-
sis. Rev Hosp Clin Fac Med Sao Paulo. 1981;36:172–8.
286 Mycopathologia (2013) 176:279–286
123