Hemorrhage in late pregnancy - كلية الطب · 2019-08-10 · Antepartum hemorrhage •It is...
90
Hemorrhage in late pregnancy Presentation by Prativa Dhakal M.Sc. Nursing Maternal health nursing Batch 2011
Transcript of Hemorrhage in late pregnancy - كلية الطب · 2019-08-10 · Antepartum hemorrhage •It is...

Hemorrhage in late pregnancy
Presentation by
Prativa Dhakal
M.Sc. Nursing
Maternal health nursing
Batch 2011

Contents
• Antepartum Hemorrhage
• Causes of Antepartumhemorrhage
• Definition of Placenta Previa
• Incidence
• Etiology
• Pathological anatomy
• Types of placenta Previa
• Clinical Features
• Conformation of diagnosis
• Complications
• Prognosis
• Management
• Nursing Management
• Research Evidence
• References
12/13/2013 2

Antepartum hemorrhage
• It is defined as bleeding from or into the genital tract afterthe 28th week /22nd week of pregnancy but before thebirth of baby.
• Placenta previa
• Abruptio placenta
• Rupture of uterus
12/13/2013 3

Causes of Antepartum Hemorrhage
Presenting symptoms and
other symptoms and signs
typically present
Symptoms and signs sometimes present
Probable
diagnosis
Bleeding after 22nd weeks
gestation
Intermittent or constant
abdominal pain
Shock
Tense/tender uterus
Decreased/absent fetal movement
Fetal distress or absent fetal heart sounds
Abruptio placenta
Bleeding (intra abdominal
and/or vaginal)
Severe abdominal pain
(may decrease after
rupture)
Shock
Abdominal distention/free fluid
Abnormal uterine contour
tender abdomen
Easily palpable fetal parts
Absent fetal movements and fetal heart
sounds
Rapid maternal pulse
Ruptured uterus
12/13/2013 4

Causes of antepartum hemorrhage cont…
Presenting symptoms
and other symptoms and
signs typically present
Symptoms and signs sometimes present Probable
diagnosis
Bleeding after 22 weeks
gestation
Shock
Bleeding may be precipitated by
intercourse
Relaxed uterus
Fetal presentation not in pelvis/lower
Uterine pole feels empty
Normal fetal condition
Placental
previa
12/13/2013 5

Causes of antepartum hemorrhage
A.P.H.
12/13/2013 6
Placental bleeding (70%)
Placenta previa (35%) and Abruptio placenta (35%)
Unexplained (25%) Or Intermediate
Extra placental causes (5%)Local cervico-vaginal lesions:
Cervical polypCarcinoma cervixVaricose veinLocal trauma

Placenta previa
• When placenta is implanted partially or completely overthe lower uterine segment it is called placenta previa.
12/13/2013 7

Incidence of Placenta Previa
United States:
• 0.3-0.5% of all pregnancies.
• Risks increase 1.5- to 5-fold with a history of cesarean delivery.
• Meta analysis: Rate of placenta previa increases with a rate of1% after 1 cesarean delivery, 2.8% after 3 cesarean deliveries,and as high as 3.7% after 5 cesarean deliveries.
• Of all placenta previas, the frequency of complete placentaprevia ranges from 20-45%, partial placenta previa accountsfor approximately 30%, and marginal placenta previa accountsfor the remaining 25-50%.
12/13/2013 8

Etiology
• Dropping down theory
• Persistence of chorionic activity in the deciduacapsularis and its subsequent development intocapsular placenta
• Defective decidua
• Big surface area of the placenta
12/13/2013 9

Predisposing factors
• Multiparity
• Increased maternal age (> 35 years)
• History of previous caesarean section or any other scar inthe uterus (myomectomy or hysterotomy)
• Placental size and abnormality
• Smoking-causes placental hypertrophy or compensatecarbonmonoxide induced hypoxemia
12/13/2013 10

Pathological anatomy
Placenta:
• Placenta may be large and thin.
• Tongue shaped extension from the main placentalmass.
• Extensive areas of degeneration with infarction andcalcification may be evident.
• Morbidly adherent placenta due to poor deciduaformation in the lower segment.
12/13/2013 11

Pathological anatomy cont…
Umbilical cord:
• Cord may be attached to the margin or onto themembranes.
• Insertion of cord may be close to the internal os or thefetal vessels may run across the internal os invelamentous insertion giving rise to vasa previa
Lower uterine segment:
• Lower uterine segment and the cervix becomes softand more friable.
12/13/2013 12

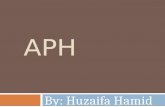
Types/degree of placenta previa
• Low-lying placenta (Type I)
• Marginal placenta previa (Type II)
• Partial or incomplete placenta previa (Type III )
• Total or central placenta previa (Type IV)
• Vasa previa
12/13/2013 13

12/13/2013 14

12/13/2013 15

Cause of bleeding
• As the placental growth slows down in later months and thelower segment progressively dilates, inelastic placenta issheared off the wall of lower segment.
• This leads to opening up of utero-placental vessels andleads to an episode of bleeding.
• As it is a physiological phenomena which leads to theseparation of placenta, the bleeding is said to be inevitable.
• The separation of the placenta may be provoked by traumaincluding vaginal examination, coital act, external version orduring high rupture of membranes.
12/13/2013 16

Clinical features
Symptoms:
• Painless, apparently causeless and recurrenthemorrhage
• Hemorrhage from the implantation site in the loweruterine segment may continue after placental delivery.
Signs:
• General condition and anemia are proportionate to the visible blood loss.
12/13/2013 17

Clinical features cont…
Abdominal examination
– Size of uterus is proportionate to POG.
– Uterus feels relaxed, soft and elastic.
– Persistence of malpresentation like breech or transverse orunstable lie is more frequent. There is also frequency oftwin pregnancy.
– Head is free floating in contrast to POG.
– FHS is usually present, unless there is major separation ofthe placenta with the patient in exsanguinated condition.
12/13/2013 18

Clinical features cont…
Vulval inspection
• Only inspection has to be done to note the amount,character of blood.
• Blood is bright red in colour.
Vaginal examination
• Must not be done outside the operation theater in thehospital.
12/13/2013 19

Confirmation of diagnosis
Localization of placenta
• Sonography: Transabdominal ultrasound (TAS)
• Transvaginal ultrasound (TVS)
• Transperineal ultrasound
• Colour Doppler flow study
Clinical
• By internal examination (Double setup examination)
• Direct visualization during caesarean section
• Examination of the placenta following vaginal delivery
12/13/2013 20

Complications
During pregnancy:
• APH with varyingdegrees of shock
• Malpresentation
• Premature labour
During Labour:
• Early rupture of membrane
• Cord prolapse
• Slow dilatation of cervix
• Intrapartum hemorrhage
• Increased incidence of operative interference
• PPH
• Retained placenta
12/13/2013 21
Maternal

Complications cont…
Puerperium
• Sepsis is increased due to
– Increased operativeinterference
– Placental site near tovagina and anemia
– Subinvolution
– Embolism
Fetal
• Low birth weight
• Asphyxia
• Intrauterine death
• Birth injuries
• Congenital malformation
12/13/2013 22

Prognosis
Maternal
• Substantial reduction of maternal deaths in placentaprevia throughout globe.
• Ultimate cause of death are hemorrhage and shock.
• Morbidity is raised due to hemorrhage and operativeinterference
Fetal
• Perinatal mortality ranges from 10-25%.
• The causes of death are prematurity, asphyxia andcongenital malformation.
12/13/2013 23

Prognosis cont…
• Maternal mortality rate ranges from 2-3%.
• Maternal mortality is 0.03% in the United States.
• Neonatal mortality associated with placenta previa is as high as 1.2%
12/13/2013 24

Prevention
• Adequate antenatal care to improve the health status ofwomen and correction of anemia
• Antenatal diagnosis of low lying placenta at 20 weeks withroutine ultrasound needs repeat ultrasound examinationat 34 weeks to confirm diagnosis.
• Significance of warning hemorrhage should not beignored
• Family planning and limitation of births reduce theincidence.
12/13/2013 25

Management
At home:
• The patient is immediately put in bed.
• To assess the blood loss
• Inspection of clothing soaked with blood
• To note the pulse, blood pressure and degree of anemia
• Quick but gentle abdominal examination to mark height ofuterus, to auscultate the FHS and to note any tenderness onthe uterus.
• Vaginal examination must not be done.
12/13/2013 26

Treatment
1. Immediate attention: Quickly assess
• Amount of blood loss: General condition, pallor, pulse rate andblood pressure.
• Blood samples: Cross matching, group and hemoglobin.
• An infusion of normal saline is started and blood transfusion
• Gentle abdominal palpation: Uterine tenderness and auscultationto note the fetal heart rate.
• Inspection of vulva to note the presence of any active bleeding.
Confirmation of diagnosis: History, physical examination and
sonographic examination.
12/13/2013 27

Treatment cont…
2. Formulation of line of treatment
• Depends upon the duration of pregnancy, fetal and maternal status and extent of the hemorrhage.
a. Expectant treatment
• Vital prerequisites: Availability of blood for transfusion, facilities for caesarean section
• Selection of cases:
– Mother is in good health status (Hemoglobin ≥ 10 gm%, hematocrit > 30%),
– Duration of pregnancy is <37 weeks,
– Active vaginal bleeding is absent,
– Fetal well being is assured.
12/13/2013 28

Treatment cont…
Conduct of expectant treatment:
• Bed rest with bathroom facilities
• Investigations: Hemoglobin estimation, blood grouping and urine for protein
• Periodic inspection of the vulval pads and fetal surveillance with USG at interval of 2-3 weeks
• Supplementary hematinics if the patient is anemic.
• When patient is allowed out of bed a gentle speculum examination is made to exclude local cervical and vaginal lesions for bleeding.
12/13/2013 29

Treatment cont…
Termination of the expectant treatment: Expectant treatment iscarried upto 37 weeks of pregnancy.
• Premature termination may have to be done in conditions, such as
– Recurrence of brisk hemorrhage and which is continuing
– The fetus is dead
– The fetus is found congenitally malformed on investigation
• Steriod therapy: If the duration of pregnancy is less than 34 weeks.
12/13/2013 30

Treatment cont…
Active interference:
• Bleeding occurs at or after 37 weeks of pregnancy.
• Patient is in labour
• Patient is in exsanguinated state on admission
• Bleeding is continuing and of moderate degree
• Baby is dead of known to be congenitally deformed.
12/13/2013 31

Definitive treatment
1. Vaginal examination in operation theatre followed by low ruptureof membranes or Caesarean section.
2. Caesarean section without internal examination
1. Vaginal examination: Double setup examination should be done in
operation theatre keeping everything ready for caesarean section.
• Contraindications of vaginal examination are:
– Patient is in exsanguinated state
– Major degree of placenta previa
– Associated complicating factors: Malpresentation, elderlyprimigravida, history of previous caesarean section, contractedpelvis etc.
12/13/2013 32

Definitive treatment cont…
a. Low rupture of membrane: Done in lesser degree of placentaprevia (Type I and Type II anterior).
b. Caesarean section: The indication are:
– Severe degree of placenta
– Lesser degree of placenta previa where amniotomy fails to stopbleeding or fetal distress appears.
– Complicating factors associated with lesser degrees of placentaprevia where vaginal delivery is unsafe.
– Caesarean section without internal examination
12/13/2013 33

Nursing Assessment
• Determine the amount and type of bleeding; also, review anyhistory of bleeding throughout this pregnancy.
• Inquire as to the presence or absence of pain in associationwith the bleeding.
• Record maternal and fetal vital signs.
• Palpate for the presence of uterine contractions.
• Evaluate laboratory data on hemoglobin and hematocritstatus.
• Assess fetal status with continuous fetal monitoring.
12/13/2013 34

Nursing Diagnoses
• Ineffective Tissue Perfusion, Placental, related toexcessive bleeding causing fetal compromise
• Deficient Fluid Volume related to excessive bleeding
• Risk for Infection related to excessive blood loss and openvessels near cervix
• Anxiety related to excessive bleeding, procedures, andpossible maternal-fetal complications
12/13/2013 35

12/13/2013 36

Definition
• It is one form of antepartum hemorrhage where bleedingoccurs due to premature separation of normally situatedplacenta.
12/13/2013 37

Pathology• Initiated by hemorrhage into the decidua basalis.
• The decidua then splits, leaving a thin layer adhered to themyometrium.
• Consequently, the process in its earliest stages consists of thedevelopment of a decidual hematoma that leads toseparation, compression, and ultimate destruction of theplacenta adjacent to it.
• Inflammation—infection—may be a contributor to causalpathways.
12/13/2013 38

Pathology cont…
• Early stage: May be no clinical symptoms, and separationis discovered upon examination of the freshly deliveredplacenta.
– There is a circumscribed depression on the placenta's maternalsurface.
– Usually measures a few centimeters in diameter and is coveredby dark, clotted blood.
• In some instances, a decidual spiral artery ruptures tocause a retroplacental hematoma, which as it expands,disrupts more vessels to separate more placenta.
12/13/2013 39

Pathology cont…
• The area of separation rapidly becomes more extensiveand reaches the margin of the placenta.
• Because the uterus is still distended by the products ofconception, it is unable to contract sufficiently tocompress the torn vessels that supply the placental site.
• The escaping blood may dissect the membranes from theuterine wall and eventually appear externally or may becompletely retained within the uterus.
12/13/2013 40

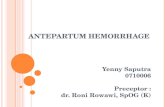
Varieties of abruptio placenta
• Concealed Hemorrhage
• Revealed
• Mixed
12/13/2013 41

12/13/2013 42

12/13/2013 43
Concealed Revealed Mixed

Risk factors
• Increased age, poor socioeconomic condition and parity
• Preeclampsia
• Chronic hypertension
• Preterm ruptured membranes
• Folic acid deficiency
• Short cord
• Multifetal gestation
• Low birth weight
• Hydramnios
• Cigarette smoking
• Thrombophilias
• Cocaine use
• Prior abruption
• Uterine leiomyoma
12/13/2013 44

Abruptio placenta cont…
Couvelaire uterus
• Widespread extravasation of blood into the uterinemusculature and beneath the uterine serosa.
• Such effusions of blood are also occasionally seenbeneath the tubal serosa, between the leaves of thebroad ligaments, in the substance of the ovaries, and freein the peritoneal cavity.
• Incidence is unknown, can be demonstrated only atlaparotomy.
12/13/2013 45

Abruptio placenta cont…
• These myometrial hemorrhages seldom interfere withmyometrial contraction to cause atony, and they are notan indication for hysterectomy.
12/13/2013 46

Abruptio placenta cont…
Changes in other organs
• Liver: fibrin knots in the hepatic sinusoids
• Kidney: Acute cortical necrosis or acute tubular necrosis
• Shock proteinuria: is due to renal anoxia which usuallydisappears two days after delivery.
12/13/2013 47

Abruptio placenta cont…
Blood coagulopathy:
• It is due to excess consumption of plasma fibrinogen dueto DIC and retroplacental bleeding.
• There is overt hypofibrinogenemia (<150mg/dl) andelevated levels of fibrin degradation products and Ddimer.
12/13/2013 48

Clinical classification
Depending upon the degree of placental abruption and its
clinical effects, the cases are graded as follows:
• Grade 0: Clinical feature may be absent.
• Grade 1: External bleeding is slight. Uterus is irritable;tenderness may or may not be present. Shock is absent.FHS is good.
12/13/2013 49

Clinical classification cont…
• Grade 2: External bleeding is mild to moderate. Uterinetenderness is always present. Shock is absent. Fetaldistress or even fetal death occurs.
• Grade 3: Bleeding is moderate to severe or may beconcealed. Uterine tenderness is marked. Shock ispronounced. Fetal death is the rule. Associatedcoagulation defect or anuria is present.
12/13/2013 50

Clinical features
Depends upon
• Degree of separation of placenta
• Speed at which separation occurs and
• Amount of blood concealed inside the uterine cavity.
12/13/2013 51

The clinical features of the revealed and mixed variety are given below:
Revealed Mixed
Symptoms: Abdominal discomfort or pain
followed by vaginal bleeding
Active intense pain abdomen
followed by slight vaginal bleeding.
The pain becomes continuous.
Character of
bleeding
Continuous dark colour (slight to
moderate)
Continuous dark colour (usually
slight) or blood stained serous
discharge.
General
condition
Proportionate to visible blood
loss, shock is usually absent
Shock is pronounced which is out
of proportion with the visible
blood loss.
Pallor Related with visible blood loss Pallor is usually severe and out of
proportion to visible blood loss.
12/13/2013 52

The clinical features of the revealed and mixed variety are given below:
Revealed Mixed
Features of
preeclampsia
May be absent Frequent association either
preexisting or appear.
Uterine height Proportionate to POG Disproportionately enlarged and
globular.
Uterine feel Normal feel with localized
tenderness, contractions frequent
and local amplitude
Uterus is tense, tender and rigid
Fetal parts Can be identified easily Difficult to make out
FHS Usually present Usually absent
Urine output Normal Usually diminished
12/13/2013 53

The clinical features of the revealed and mixed variety are given below:
Revealed Mixed
Laboratory
Blood Hb%
Low value proportionate
to blood loss
Markedly lower, out of proportion to
blood loss
Coagulation
profile
Usually unchanged Variable changes :
Clotting time increased (>6 min)
Fibrinogen level low (<150mg/dl)
Platelet count low
Increased PTT
Increased FDP and D dimer
Urine for protein May be absent Usually present
Confusion in
diagnosis
With placenta previa. With acute obstetrical gynecological
surgical complication
12/13/2013 54

Abruptio placenta cont…
Sheehan Syndrome
• Severe intrapartum or early postpartum hemorrhage rarely isfollowed by pituitary failure.
• Characterized by failure of lactation, amenorrhea, breast atrophy,loss of pubic and axillary hair, hypothyroidism, and adrenal corticalinsufficiency.
• Exact pathogenesis is not well understood but such endocrineabnormalities develop infrequently in women who hemorrhageseverely.
• Varying degrees of anterior pituitary necrosis and impairedsecretion of one or more trophic hormones (in some cases)
• Diagnosis: MRI
12/13/2013 55

Distinguishing features of placenta previa and abruptio placenta
12/13/2013 56
Placenta previa Abruptio placenta
Clinical features
Nature of bleeding
Character of
bleeding
General condition
and anemia
Features of pre-
eclampsia
Painless, apparently
causeless and recurrent
Bleeding is always revealed
Bright red
Proportionate to visible blood
loss
Not relevant
Painful, often attributed to
preeclampsia or trauma
and continuous
Revealed, concealed or
usually mixed
Dark coloured
Out of proportion to the
visible blood loss in concealed
or mixed variety
Present in one-third cases

Distinguishing features contd…
Placenta previa Abruptio placenta
Abd. examination
Height of uterus
Feel of uterus
Malpresentation
FHS
Proportionate height
Soft and relaxed
Malpresentation is common.
The head is high floating
Usually present
May be disproportionately
enlarged in concealed type
May be tense, tender and rigid
Head may be engaged
Usually absent specially in
concealed type
Placentography Placenta in lower segment Placenta in upper segment
Vaginal examination Placenta is felt on lower
segment
Placenta is not felt on lower
segment. Blood clots should not
be confused with placenta.
12/13/2013 57

Management
• Depending on gestational age and status of mother and fetus.
• With a fetus of viable age, and if vaginal delivery is notimminent, then emergency cesarean delivery is chosen.
• Resuscitation and acute management, with massive externalbleeding, intensive resuscitation with blood plus crystalloidand prompt delivery to control hemorrhage are lifesaving forthe mother and hopefully, for the fetus.
• If the diagnosis is uncertain and the fetus is alive but withoutevidence of compromise, then close observation can bepracticed in facilities capable of immediate intervention.
12/13/2013 58

Prevention
• Prevention, early diagnosis and effective therapy ofpreeclampsia and other hypertensive disorders of pregnancy.
• Needle puncture during amniocentesis should be underultrasound guidance.
• Avoidance of trauma specially forceful external cephalicversion under anesthesia
• To avoid sudden decompression of the uterus
• To avoid supine hypotension
• Routine administration of folic acid from early pregnancy.
12/13/2013 59

In the hospital
1. Revealed type: assessment is to be done as regards:
– Amount of blood loss
– Maturity of fetus
– Whether the patient is in labour or not
Preliminaries
• Blood for Hemoglobin and hematocrit estimation, coagulationprofile, ABO and Rh grouping and urine for detection ofprotein.
• RL solution drip started with wide bore cannula andarrangement for blood transfusion.
• Close monitoring of maternal and fetal condition.
12/13/2013 60

Management cont…
Patient is in labour
• Labour is accelerated by low rupture of membranes.
• Oxytocin drip is started to accelerate labour.
The patient is not in labour:
• Pregnancy 37 weeks or more: induction of labour is to bedone by low rupture of membrane with or withoutoxytocin.
12/13/2013 61

Management cont…
• Pregnancy less than 37 weeks:
– Bleeding moderate to severe and continuing—lowrupture of membrane, administration of oxytocin drip
– Bleeding slight or has stopped—the patient is put onconservative management, close observation of themother and careful monitoring is essential.
12/13/2013 62

Management cont…
2. Mixed or concealed type
Principles of management of concealed type are:
• To correct hypovolemia and to restore blood loss. Normalsaline or hemaccel infusion is started
• To bring about effective uterine contraction and terminationof the abruption process.
• To observe blood coagulation profiles at two hourly interval.
• Close monitoring of maternal and fetal condition ismaintained.
12/13/2013 63

Management cont…
• Vaginal delivery
• Caesarean section:
– Early: Unfavourable cervix where speedy vaginal delivery is notpossible and there is good prospect of fetal survival.
– Late: If inspite of amniotomy and oxytocin, the progress oflabour is delayed (6-8 hours) and instead, the general conditiongradually deteriorates with appearance of complicating factorslike oliguria or falling fibrinogen level or there is evidence offetal distress.
12/13/2013 64

Nursing Diagnoses
• Ineffective Tissue Perfusion: Placental related to excessivebleeding, hypotension, and decreased cardiac output,causing fetal compromise
• Deficient Fluid Volume related to excessive bleeding
• Fear related to excessive bleeding, procedures, andunknown outcome
12/13/2013 65

12/13/2013 66

Rupture of uterus
• Dissolution in the continuity of uterine wall any timebeyond 28 weeks of pregnancy is called rupture of uterus.
• Injury to the wall of uterus in early months of pregnancyis called perforation either instrumental or perforatinghydatidiform mole.
12/13/2013 67

Classification of rupture uterus
Uterine rupture typically is classified as either:
• Complete
• Incomplete
12/13/2013 68

Causes1. Spontaneous
2. Scar rupture
3. Iatrogenic
12/13/2013 69

Causes cont…
Spontaneous
1. During pregnancy: previous dilatation and curettage operation orMRP, grand multiparity, congenital malformation of the uterus ofbicornuate variety, in couvelaire uterus.
• Usually complete, involves the upper segment and usually occurs inlater months of pregnancy.
2. During labour:
• Obstructive rupture: involves lower segment and usually extendsthrough one lateral side of the uterus to the upper segment.
• Non-obstructive rupture: Grand multiparae , rupture usually occursin early labour, usually involves fundal area and is complete.
12/13/2013 70

Causes cont…
Scar rupture
• Incidence of lower uterine segment scar rupture is about 1-2%,Classical: 5-10 times higher.
• During pregnancy: Classical or hysterotomy scar is likely to give wayduring later months of pregnancy. Lower segment scar rarelyruptures during pregnancy.
• During labour: The classical or hysterotomy scar is more vulnerable to rupture during labour.
12/13/2013 71

Causes cont…
Iatrogenic or traumatic:
During pregnancy:
– Injudicious administration of oxytocin
– Use of prostaglandins for induction of abortion or labour.
– Forcible external version specially under general anesthesia
– Fall or blow on the abdomen
During labour:
– Internal podalic version, Destructive operation
– Manual removal of placenta
– Application of forceps or breech extraction through incompletely dilated cervix
– Injudicious administration of oxytocin for augmentation of labour.
12/13/2013 72

Dehiscence and scar rupture
Dehiscence:
– Disruption of part of scar and not the entire length
– Fetal membranes remain intact and
– Bleeding is almost nil or minimal
Rupture includes:
– Disruption of the entire length of scar
– Rupture of membranes with varying amount of bleeding from the margins or from its extension.
12/13/2013 73

Diagnosis
During pregnancy
1. Scar rupture
Classical or hysterotomy
• Dull abdominal pain all over the area with slight vaginal bleeding.
• Tenderness on uterine palpation.
• FHS may be irregular or absent.
• Sooner or later the rupture becomes complete.
12/13/2013 74

Diagnosis cont…
2. Spontaneous rupture in uninjured uterus:
• Confined to the high parous women.
• Acute onset but sometimes insidious.
• Acute type: Patient has acute pain abdomen with faintingattacks and may collapse.
• Presence of features of shock, acute tenderness onabdominal examination, palpation of superficial fetalparts, if the rupture is complete and absence of FHS.
12/13/2013 75

Diagnosis cont…
3. Rupture following fall, blow or external version or use ofoxytocics:
• History of such accident followed by acute pain abdomenand slight vaginal bleeding.
• Rapid pulse and tender uterus, confirmation is done bylaparotomy.
12/13/2013 76

Diagnosis cont…
During labour
1. Scar rupture:
• Classical or hysterotomy scar rupture: Features are same asthose occur during pregnancy. The onset is usually acute.
• Lower segment scar rupture (silent rupture): The onset isinsidious, no classical feature of lower segment scar rupture,confirmation is by laparotomy.
2. Spontaneous or obstructive rupture: Has distinct premonitoryphase prior to rupture.
12/13/2013 77

Diagnosis of spontaneous obstructive rupture cont…
Premonitory phase:
• Multipara in labour with features of obstruction.
• Pain becomes severe in an attempt to overcome theobstruction and come to quick intervals.
• Gradually the pains become continuous and mainlyconfined to the suprapubic region.
• Patient is exhausted and dehydrated.
12/13/2013 78

Diagnosis of spontaneous obstructive rupture cont…
• Pulse rate and temperature rise.
• Distended tender lower segment.
• Bandl’s ring may be visible
• Fetal distress or FHS absent.
• Presenting part is found jammed in the pelvis and thevagina becomes dry and oedematous.
12/13/2013 79

Phase of rupture in spontaneous obstructive rupture
• Sense of something giving way at height of uterinecontraction.
• Constant pain is changed to dull aching pain with cessation ofuterine contraction.
• Features of exhaustion and shock.
• Abdominal examination: Superficial fetal parts, absence ofFHS, absence of uterine contour and two separate swellings,one contracted uterus and the other fetal ovoid.
• Vaginal examination: Recession of presenting part and varyingdegrees of bleeding.
12/13/2013 80

Diagnosis cont…
3. Spontaneous non-obstructive rupture:
• Rare and confined to high parous women.
• Height of uterine contraction is suddenly seized with anagonizing bursting pain followed by a relief with cessationof contractions.
• Presence of shock, evidences of internal hemorrhage,tenderness over the uterus and varying amount of vaginalbleeding.
12/13/2013 81

Diagnosis cont…
4. Rupture following manipulative or instrumental delivery
• Sudden deterioration of general condition of patient withvarying amount of vaginal bleeding following manipulativedelivery
• Exploration of uterus to feel the rent confirms the diagnosis.
• Shortening of cord immediately following a difficult vaginaldelivery
• Placenta being extruded out into abdominal cavity, throughthe rent in the uterus.
12/13/2013 82

Prevention
• At risk mothers likely to rupture should have mandatoryhospital delivery. There are
– Contracted pelvis
– Previous history of caesarean section, hysterotomy ormyomectomy
– Uncorrected transverse lie
– Multiparity with pendulous abdomen
– Grand multiparity
– Known case of hydrocephalous
• General anesthesia should not be used to give undue force inexternal version
12/13/2013 83

Prevention cont…
• Undue delay in the progress of labour in a multipara withprevious uneventful delivery should be viewed with concernand cause should be sought for.
• Judicious selection of cases with previous history of caesareansection for vaginal delivery.
• Judicious selection of cases and careful watch are mandatoryduring oxytocin infusion either for induction or acceleration oflabour.
12/13/2013 84

Prevention cont…
• Internal podalic version in singleton fetus should never bedone in obstructed labour.
• Attempted forceps delivery or breech extraction throughincompletely dilated cervix should be avoided.
• Destructive vaginal operations should be performed by skilledpersonnel.
• Manual removal in morbid adherent placenta should be doneby senior person.
12/13/2013 85

Treatment
Resuscitation and laparotomy
• Depending upon the state of clinical condition, eitherresuscitation is to be done followed by laparotomy or in acuteconditions, resuscitation and laparotomy are to be donesimultaneously.
• Any of the following procedures may be adopted followinglaparotomy
– Hysterectomy
– Repair
– Repair and sterilization
12/13/2013 86

Nursing Assessment
• Continuously evaluate maternal vital signs; especially note anincrease in the rate and depth of respirations, an increase inpulse, or a drop in BP indicating status change.
• Observe for signs and symptoms of impending rupture (ie, lackof cervical dilatation, tetanic uterine contractions,restlessness, anxiety, severe abdominal pain, fetal bradycardia,or late or variable decelerations of the FHR).
• Assess fetal status by continuous monitoring.
• Speak with family, and evaluate their understanding of thesituation.
12/13/2013 87

Nursing Diagnoses
• Deficient Fluid Volume related to active fluid loss from hemorrhage
• Ineffective Tissue Perfusion, Maternal Vital Organ and Fetal, related to hypovolemia
• Fear related to surgical outcome for fetus and mother
12/13/2013 88

References 1. Fraser DM, Cooper MA. Myles Textbook for Midwives. 15th edition.
Philadelphia: Churchill livingstone elsevier; 2009
2. Dutta DC. Textbook of obstetrics. 6th edition. Calcutta: New central bookagency;2004
3. Pillitteri A. Maternal and child health nursing. Care of the childbearing andchildrearing family. Sixth edition. Philadelphia: Lippincott Williams & Wilkins;2010.
4. Cunningham, Leveno, Bloom. William’s obstetrics. 23rd edition. United states ofAmerica: Mcgraw Hill companies; 2010.
5. Placenta Previa. Internet [Updated on 5th June 2012, Cited on 21st October2013] Available form: http://emedicine.medscape.com/article/262063-overview
6. Nettina SM, Mills EJ. Lippincott manual of nursing practice. 8th edition.Baltimore: Lippincott Williams and Wilkins; 2006
12/13/2013 89