Hemolytic Anemia and Sickle Cell Disease - ez-med.org fileHemolytic Anemia Introduction Etiology...
33
Hemolytic Anemia and Sickle Cell Disease Dr. Wael Maher MD; PhD A.Professor of Pathology SRC, KU, FOMSCU
Transcript of Hemolytic Anemia and Sickle Cell Disease - ez-med.org fileHemolytic Anemia Introduction Etiology...

Hemolytic Anemia and Sickle Cell Disease
Dr. Wael Maher MD; PhD
A.Professor of Pathology
SRC, KU, FOMSCU

Hemolytic Anemia
Introduction Etiology
Corpuscular and Extra-corpuscular
Classification
Intra and Extra Vascular
Features
SSD

Introduction
• Blood composition: Plasma, blood cells
• Bone marrow: Red, Yellow
• Hematopoiesis:
• Pluripotent stem cell
• Unipotent stem cell
• Precursor cell
• Mature cell
• Properties of stem cell: PROLIFERATION, MATURATION
Introduction
• Erythropoiesis:• Pluripotent stem cell
• BFU-E, CFU-E
• Proerythroblast
• Erythroblast: Basophilic, Polychromatic, Orthochromatic
• Reticulocyte
• Eryhtrocyte
• Factors• Normal stem cells of BM
• Normal architecture of BM
• Regulatory hormones: Epo, Androgen, thyroxin, Cortisol, ACTH
• Nutritional elements: Ptns., Fe, Folic acid, Vit.B12, Vit.C

Normal Hematological values
1- RBCs• Hemoglobin concentration (Hb conc.)
• Red cell count
• Color index = Hb concentration / Red cell count=1
• Hematocrit/Packed cell volume (PCV)
• Red cell indices:
• MCV= PCV/Red cell count
• MCH=Hb conc./Red cell count
• MCHC=Hb conc./PCV
• Red cell distribution width (anisocytosis)
• Red cell diameter: Micro-Macro-Aniso
• Red cell morphology
• Reticulocytic count (Activity of BM)• +++ in Anemia due to destruction, MEGALOBLASTIC anemia under treatment, Recovery from BM supp.
• --- in Anemia due to --- RBCs production
Normochromic anemia
Hypochromic anemia
Anemia with increased color index
Anemia with increased MCH
Hyperchromic anemia
Normocytic anemia
Microcytic anemia
Macrocytic anemia
2- WBCs• TLC
• Differential count
3- Platelet count
Normal Hematological values
AnemiaGeneral
• Definition
• Pathophysiology:
• +++Oxygen delivery to tissue
• +++Plasma volume
• +++CO
• Redistribution of blood
• +++Epo
• Classification
• Etiological
• Morphological

AnemiaGeneral
• Etiological classification
• Decrease production
• Decrease proliferation (Hypoproliferative)
# BM stem cells # BM architecture Organ failure Chronic disease
• Decrease maturation (Dyshematopoietic)
Hypochromic Megaloblastic Myelodysplastic
• Increase destruction
Hemolytic Acute post-Hemorrhagic
• Dilutional
• Morphological
• Hypochromic microcytic Anemia: Fe #, Thaless
• Normochromic normocytic Anemia: Hemolytic, Hgic
• Macrocytic Anemia: Megaloblastic

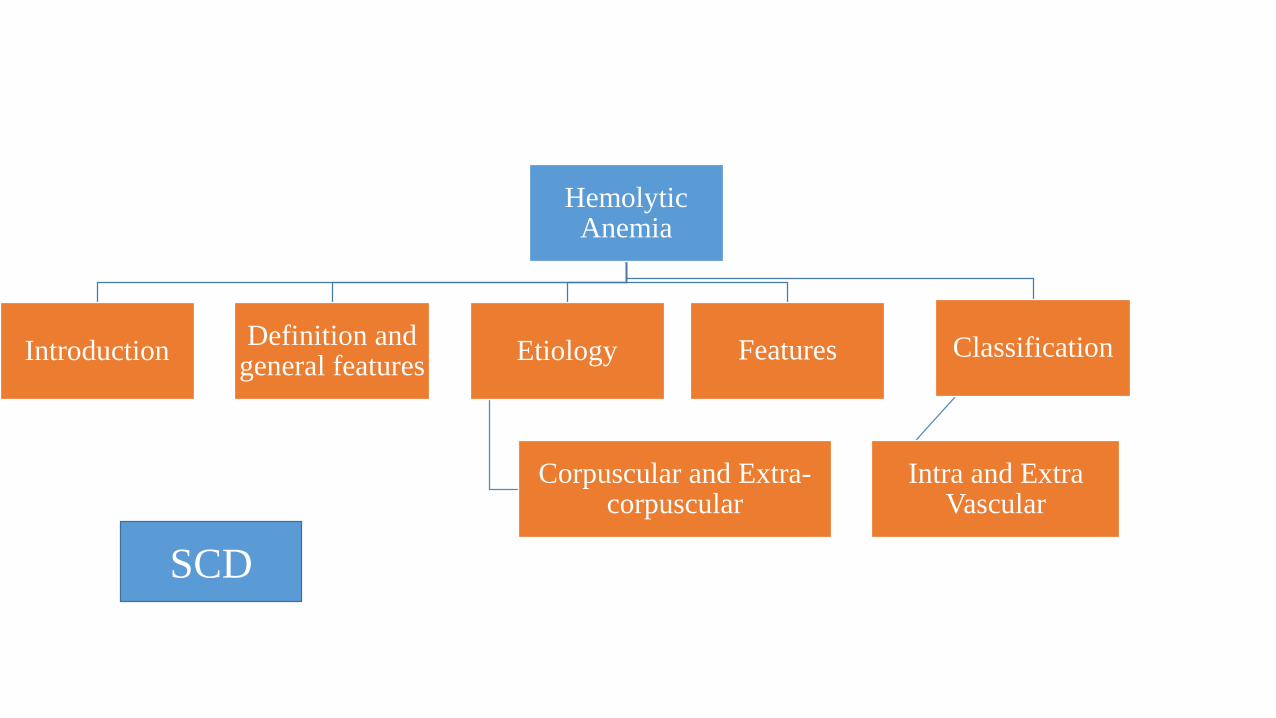
Hemolytic Anemia
IntroductionDefinition and
general featuresEtiology
Corpuscular and Extra-corpuscular
Classification
Intra and Extra Vascular
Features
SCD

Hemolytic Anemia
• Definition
• Anemia due to shortened red cell life span (normal = 120 days); that is, premature destruction of red cells
• Hemolytic anemias share the following features:
• --- life span below the normal 120 days
• +++ Epo levels and a compensatory increase in erythropoiesis
• Accumulation of Hb degradation products

Hemolytic Anemia
IntroductionDefinition and
general featuresEtiology
Corpuscular and Extra-corpuscular
Classification
Intra and Extra Vascular
Features
SCD

Hemolytic AnemiaEtiology
• Corpuscular:• Membrane defects: HS, PNH• Hemoglobin defect ( Hemoglobinopathies)
• Thalessemia (Defect in chain synthesis)• Others (Defect in aa sequence in chain)
Sickle cell anemia (HbS) HbC, HbD, HbE
• Enzyme defect• G6PD deficiency
• Extracorpuscular: • Immune hemolytic anemia
• Alloimmune: Incompatible blood transfusion, Hemolytic disease of the newborn• Autoimmune hemolytic anemia
• Hypersplenism• Infection: ( eg, Malaria, Clostridium welchii)• Traumatic: DIC, March hemoglobinuria, Artificial and Calcific valves• Chemicals: Snake venom, Copper

Hemolytic Anemia
IntroductionDefinition and
general featuresEtiology
Corpuscular and Extra-corpuscular
Classification
Intra and Extra Vascular
Features
SCD

Hemolytic AnemiaManifestations
• Anemia
• Increased numbers of normoblasts in the marrow
• Increased Reticulocytic count
• Increased serum LDH
• Hepatosplenomegaly
• Hemolytic Jaundice
• Pigment stones and Obstructive Jaundice

HemeUnconjugatedIndirect
CholeConjugatedDirect

Hemolytic Anemia• Crisis:
• Hemolytic crisis
• RES hyperplasia( e.g. with infection)
• Aggravation of anemia and Jaundice:
• Fever, Rigors, Abdominal and bone pains
• Marked pallor, Deepening of jaundice and Dark urine
• Marked increased Reticulocytic count
• Aplastic crisis
• Viral infection ( Parvovirus B19)
• Aggravation of anemia without deepening of Jaundice
• Decreased reticulocytic count
• Megaloblastic crisis: Aggravation of anemia due to relative folate deficiency
• Sequestrational crisis: Aggravation of anemia due to pooling of RBCs in spleen.
• Painful veno-occlusive crisis: Sickle cell anemia
• Other features:
Iron Overload : Thalessemia Iron deficiency: PNH
Skin pigmentation and leg ulcers: Sickle Cell Anemia..
Hemolytic AnemiaManifestations
• Intravascular Hemolysis
• Hemoglobinemia
• Hemoglobinuria
• Hemosiderinuria
• Reduced serum Haptoglobin
• Reduced serum Hemopexin
• Methemalbuminemia and Methemoglobinurea
• Anemia and Jaundice

Hemolytic AnemiaManifestations
• Extravascular hemolysis
• Hemolytic Jaundice
• RES hyperplasia (work-related hyperplasia marked by splenomegaly)
• Hemoglobinemia and hemoglobinuria are not observed
Hemolytic Anemia
IntroductionDefinition and
general featuresEtiology
Corpuscular and Extra-corpuscular
Classification
Intra and Extra Vascular
Features
SCD

Hemoglobinopathies
• Hb is formed of:
• Haem: Fe +prtotporphyrin
• Globin: 4 polypeptide chains
• Normally, Hb in adult is of 3 types:
• HB A: 2 alpha (141 aa), 2 beta (146 aa) (4 alpha genes on chrom.16, 2 beta genes on chrom. 11)
• Hb A2: 2 alpha, 2 delta (2 delta genes on chromosome 11)
• Hb F: 2 alpha, 2 gamma (4 gamma genes on chromosome 11)
• Hemoglobinopathies are abnormalities in the structure of globin molecule giving rise to abnormal types of Hb.
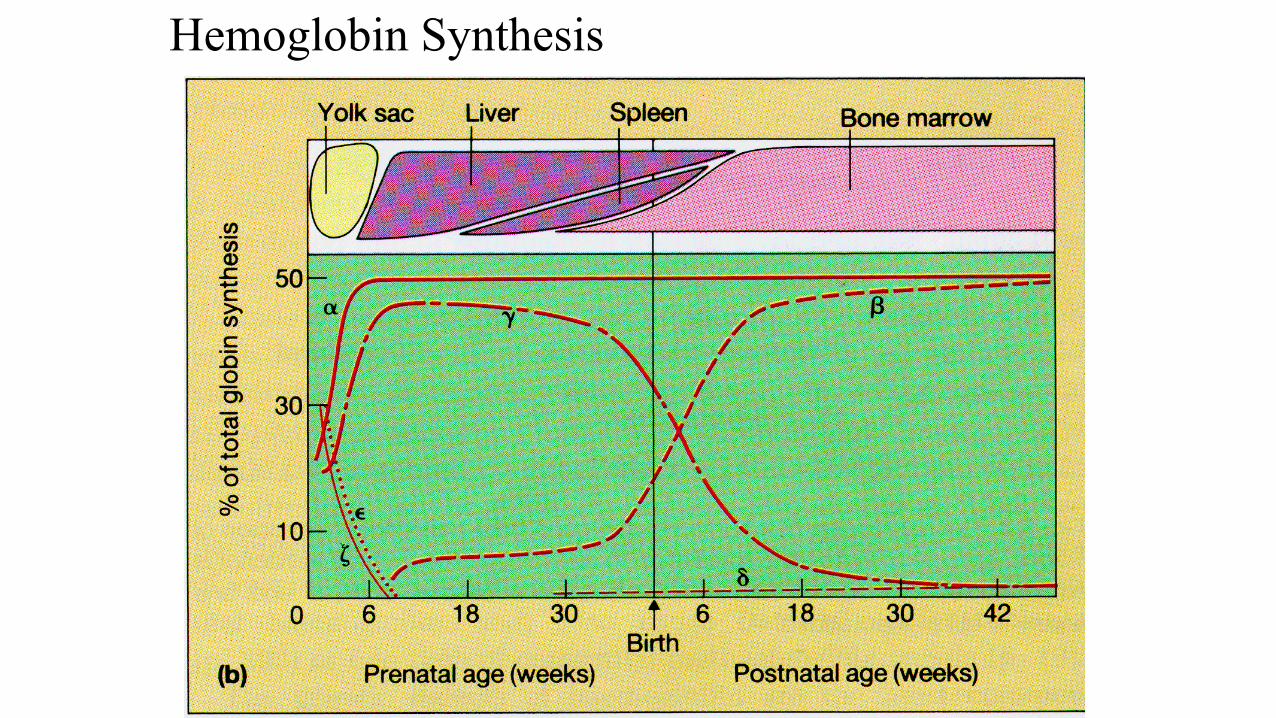
Hemoglobin Synthesis

a
a
a
a a
a
b g d
b dg
HbA HbF HbA2
98% ~1% <3.5%
Hemoglobins in normal adults

Sickle cell anemia
• Hereditary disorder…Abnormality in structure of beta chain of globin…..Abnormal Hb…HbS• Point mutation in beta globin chain: HYDROPHILIC aa Glutamine is substituted with
HYDROPHOBIC aa VALIINE at 6th position
• Sickle cell RBCs live only 10-20 days
• Homozygous (Sickle cell anemia= βS/βS) and Heterozygous (Sickle cell trait= βS/β)
• On exposure to hypoxia, HbS :• Polymerization…. +++ K+ efflux… +++ cell density/dehydration….Sickle shaped
• ---Deformability…+++ Rigidity….Destruction
• Vascular occlusion ( may be due to abnormal interactions between sickle cells and the vascular endothelium or the coagulation system)
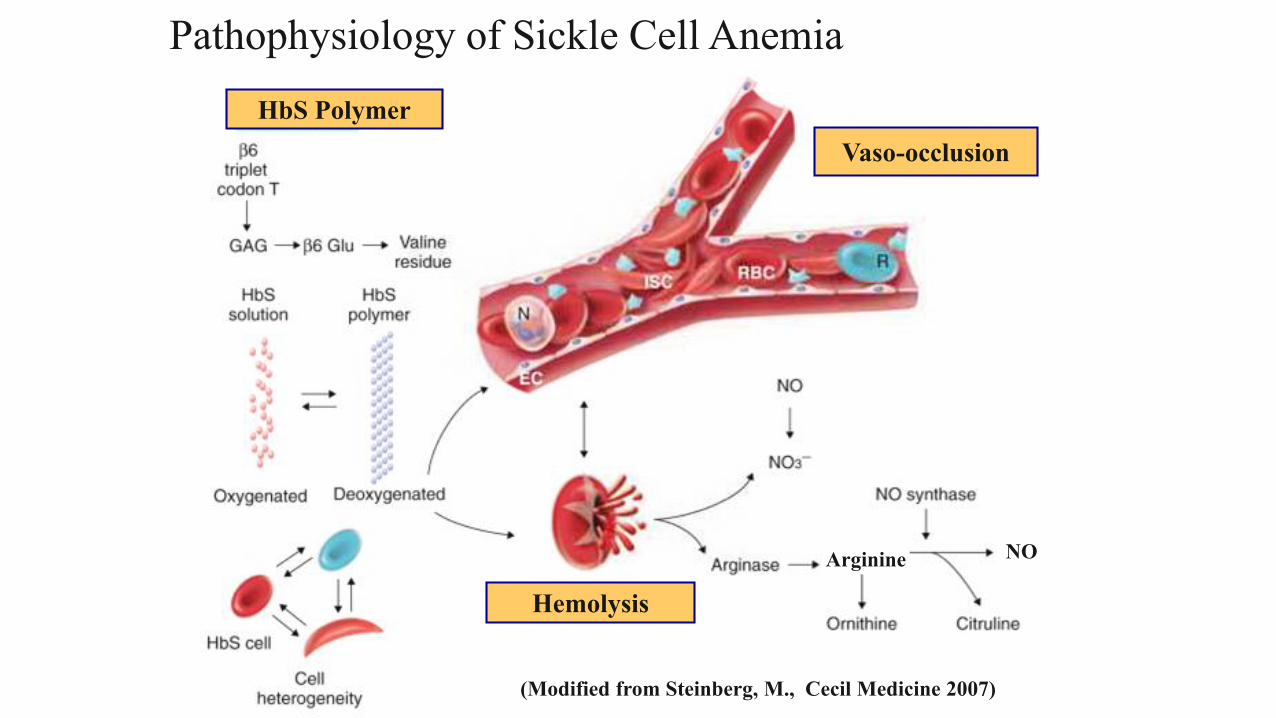
Pathophysiology of Sickle Cell Anemia
(Modified from Steinberg, M., Cecil Medicine 2007)
HbS Polymer
Vaso-occlusion
Hemolysis
Arginine NO

Genetic and Laboratory Features of Sickle Hemoglobinopathies


Sickle cell anemia• Clinical features
• Common in blacks• Sickle cell trait: Asymptomatic. Partial protection from malaria• Features of hemolytic anemia• Attacks ppt. by temperature changes, stress, dehydration and high altitude• Painful veno-occlusive crisis: Attacks of severe pain in back, abdomen and extremities.• Splenic sequestration crisis• Acute chest syndrome
• At least two: chest pain, fever, pulmonary infiltrate, respiratory symptoms, or hypoxemia.• Second-most common complication• Accounts for 25% of deaths in patients with SCD.
• Vascular occlusion:• Splenic infarction
• Renal infarction
• Bone infarction: Avascular necrosis of femur head.
• Pulmonary vascular occlusion and cor pulmonale
• Cerebral vascular occlusion
• Retinal detachment
• Priapism and impotence
• Leg ulcers
• Increased susceptibility to infections especially• Pneumococcal infections
• Salmonella and St.aureus osteomyelitis
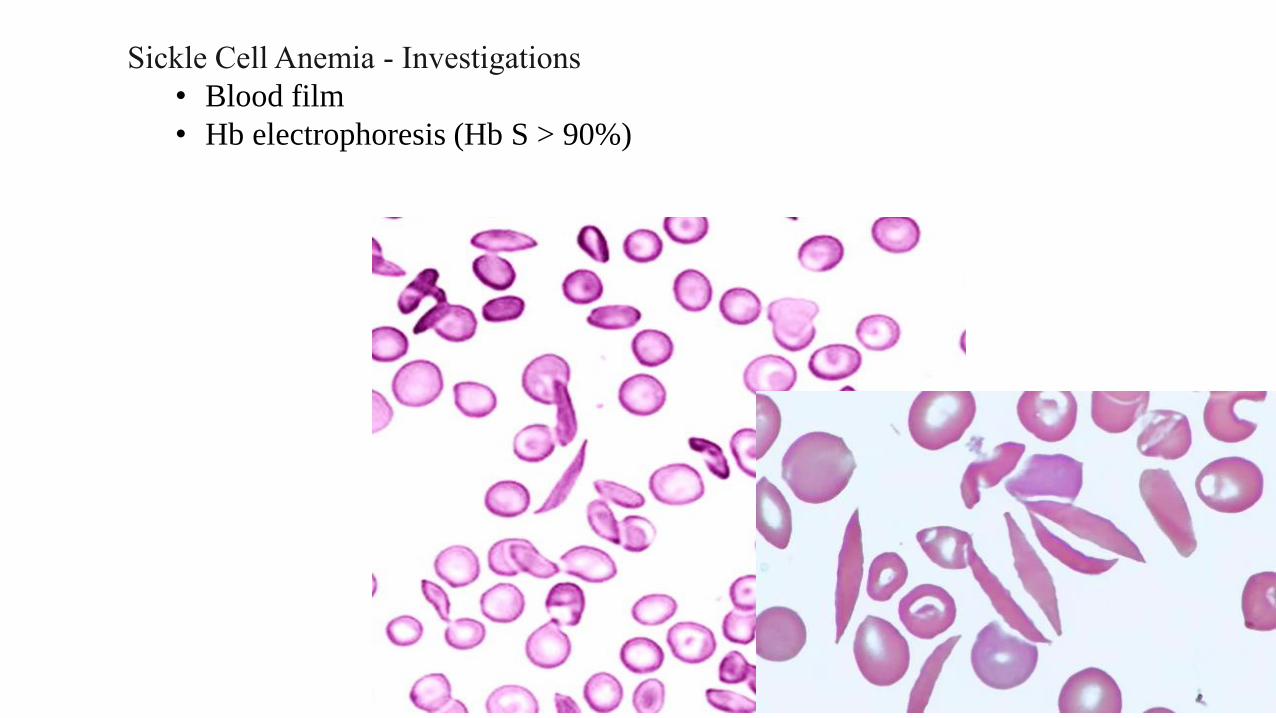
Sickle Cell Anemia - Investigations
• Blood film
• Hb electrophoresis (Hb S > 90%)

Sickle Cell Anemia - treatment
• Opiates and hydration for painful crises
• Pneumococcal vaccination
• Retinal surveillance
• Transfusion for serious manifestations (eg stroke); exchange transfusion
• Hydroxyurea
• Stem cell transplant

Hemolytic Anemia
IntroductionDefinition and
general featuresEtiology
Corpuscular and Extra-corpuscular
Classification
Intra and Extra Vascular
Features
SCD