Heavy chain deposition disease in kidney biopsies
18
Heavy chain deposition disease in kidney biopsies Alenka Vizjak, Jerica Mraz, Jelka Lindič, Dušan Ferluga Institute of Pathology, Faculty of Medicine University of Ljubljana, Slovenia Disclosures: no conflicts of interest
description
Heavy chain deposition disease in kidney biopsies. Alenka Vizjak , Jerica Mraz, Jelka Lindič, Dušan Ferluga Institute of Pathology, Faculty of Medicine University of Ljubljana , Slovenia Disclosures: no conflicts of interest. Heavy chain deposition disease (HCDD). - PowerPoint PPT Presentation
Transcript of Heavy chain deposition disease in kidney biopsies

Heavy chain deposition disease in kidney biopsies
Alenka Vizjak, Jerica Mraz, Jelka Lindič, Dušan Ferluga
Institute of Pathology, Faculty of Medicine University of Ljubljana, Slovenia
Disclosures: no conflicts of interest

Heavy chain deposition disease
(HCDD) • HCDD - a rare monoclonal immunoglobulin-
related disorder of not yet fully explored pathogenesis
• Characterized by production and systemic deposition of structurally abnormal immunoglobulin heavy chains, while light chains absent in the deposits
• First described by Aucouturier et al(N Engl J Med 1993; 329: 1389-93)

Monoclonal immunoglobulin deposits in the kidney
Amyloid deposits
Non-amyloid monoclonal immunoglobulin deposits
Amyloidosis LC
HC (very rare)
MIDD Randall-type
LCDD
LHCDD
HCDD
GN with monoclonal Igs dps mimicking IC-GN
Cryoglobulinemic-GN
Immunotactoid GP / fibrillary GN

Patients and methods
• 4 biopsy cases of HCDD (5 kidney biopsies; 1 autopsy), representing 0.09% prevalence among 5481 native kidney biopsies
• All 4 female patients, age range 62 – 79 yrs, mean age 73.0 yrs
• Standard light microscopy• Immunofluorescence microscopy
IgA, IgG, IgM, κ, λ, C3, C1q, fibrin/fibrinogen, albuminIgG1, IgG2, IgG3, IgG4, γCH1, γCH2, γCH3
• Electron microscopy

Clinical presentation / diagnosis in 4 patients with HCDD
Pts At kidney biopsy After kidney biopsy
PM - 1st CKD, prot, compl↓ no dysproteinemia
PM - 2nd CKD, NS, compl↓ no dysproteinemia
JA CKD, prot, compl↓ plasmocytoma
BŠ RPGN, NS, compl↓ plasmocytoma
RM CKD, nephr prot, compl norm
no dysproteinemia
CKD – chronic kidney disease, NS – nephrotic syndrome

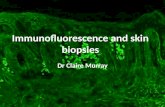
Immunofluorescence microscopy in 4 cases of HCDD
Pts IgG (γ)
IgGsubclass
γCH1 γCH2γCH3
κ / λ C3 C1q
PM - 1st 4+ n.d. n.d. n.d. 2+ / ± 2+ 4+
PM - 2nd 4+ IgG3 0 4+ 0 / 0 2+ 4+
JA 3+ IgG3 0 3+ 0 / 0 4+ 3+
BŠ 4+ IgG3 0 4+ 0 / 0 3+ 4+
RM 4+ IgG1 0 4+ 0 / 0 4+ 3+

Light and electron microscopy in 4 cases with HCDD
Light microscopy•Diffuse nodular glomerulosclerosis 4/4•Glomerular capillary aneurysms 4/4•Mesangial proliferation, 4/4with segm endo-, membranoprol pattern 3/4•Extracapillary crescents (few) 2/4
Electron microscopy•Punctate and powdery electron dense deposits 3/4

IgG (γ heavy chain) κ, λ light chains

IgG (γ heavy chain)

IgG1 IgG2

C3 C1q

γCH1 γCH2



SMA+CD31 CD68



Conclusions of our study
• Immunofluorescence examination of kidney biopsy, including testing for Igs heavy and light chains, as well as IgG subclasses, is crucial for the diagnosis of HCDD.
• Our study showed that HCDD is peculiar among MIDD because of uniform pattern of nodular glomerulosclerosis with pronounced capillary aneurysms and significant proliferation due to complement activation.
• Constant deletion of the gamma heavy chain CH1 domain and its significance in the pathogenesis of HCDD was confirmed.