Ultrasound-Guided Biopsies in the Abdomen and...
24
Ultrasound-Guided Biopsies in the Abdomen and Pelvis Thomas C. Winter, MD, Fred T. Lee Jr, MD, and J. Louis Hinshaw, MD Abstract: Ultrasound-guided biopsies in the abdomen and pelvis are generally more effective, safer, faster, and cheaper than those performed under computed tomography guidance. This manuscript will discuss multiple aspects of sonographic biopsies performed between the diaphragm and the symphysis pubis. We begin with systems issues, patient preparation (including bleeding profile and anticoagulant use), pain management, and infection precautions. The procedure itself is then analyzed, including needle guidance, the role of the sonographer, image optimization, patient positioning, core- versus fine-needle aspiration, coaxial versus individual pass, needle technique, and postprocedure management. Issues specific to dif- ferent sites are then discussed: liver, spleen, pancreas, kidney, adrenal, bowel, retroperitoneum and mesentery, and the pelvis. We finish with a discussion of complications, future trends, and a brief summary. Key Words: ultrasound, biopsy, guidance, sonography (Ultrasound Quarterly 2008;24:45Y68) LEARNING OBJECTIVES 1. Identify patient selection and preparation. 2. Describe optimal biopsy technique. 3. List potential complications. T he advent of percutaneous image-guided biopsy has been a huge boon to patients, generally sparing them the morbidity of operative procedures for tissue characterization. Ultrasound guidance for these procedures is possible in most cases in the abdomen and pelvis and is often safer, quicker, and less expensive and has a higher diagnostic yield than other image guidance modalities. The goal of this article is to present techniques for ultrasound-guided biopsies in a variety of common and not-so-common scenarios in the abdomen and pelvis, potentially expanding the use of sonography in these situations and thereby bringing the benefits of ultrasound to more of our patients. HISTORY Although primacy is notoriously difficult to accurately assess, some of the earliest ultrasound-guided procedures were reported in 1972 by Goldberg and Pollack 1 with the demonstration of their dedicated aspiration transducer. 2 Com- puted tomography (CT) followed closely behind, with the first reported CT-guided biopsy performed by Alfidi et al 2 in 1975. 3 Ultrasound-guided needle placement grew steadily in the ensuing decades. The aptly entitled article of Dodd et al, 4 BSonography: The Undiscovered Jewel of Interventional Radiology,[ led to even more popularity for sonographically guided procedures. INDICATIONS The reasons for percutaneous biopsy are broad and expanding. These include the need for tissue characterization of an abdominal mass, confirmation of metastatic disease to direct therapy or counsel patients, confirmation of a specific tumor type for a clinical trial (a very large potential future application of percutaneous biopsy as cancer treatments become more specific for different tumors), evaluation for infection in a fluid collection, evaluation for parenchymal disease in native organs (typically the kidney and liver), and evaluation for transplant organ rejection. As abdominal radiologists, we appreciate the potential advantages of high- tech, noninvasive imaging; having said that, we definitely agree with one speaker who said Bthe most useful additional MR pulse sequence for lesion characterization is the 18-ga needle[! Another perspective was given by one of the memorable characters in Samuel Shem’s classic novel, BThe House of God,[ who stated Bthere is no body cavity that cannot be reached with a 14-gauge needle and a good strong arm.[ 5 What not to biopsy? All medical decision making is a risk-benefit analysis, so there are very few absolute contra- indications to biopsy. An excellent relationship and open communication with the referring physician are crucial to good radiological medical decision making; in addition, the radiologist needs to think like a clinician, know his or her patient’s medical history, and understand the clinical problem to be solved by the biopsy. For example, performing a biopsy of a highly suggestive hypervascular mass in a cirrhotic liver in the face of an elevated >-fetoprotein (AFP) is not necessary 6 Vthe very high likelihood of hepatocellular carcinoma (HCC) in this setting makes tissue confirmation not worth the small but nonzero risk of bleeding and/or seeding. In the past, percutaneous biopsy of renal masses was actively discouraged; recent improvements in pathological techniques, increasing evidence suggesting that the risk of tumor seeding is minimal, and new treatments for renal cell carcinoma (RCC), however, have led to a marked REVIEW ARTICLE CME ARTICLE Ultrasound Quarterly & Volume 24, Number 1, March 2008 45 Received for publication November 14, 2007; accepted January 2, 2008. Department of Radiology, Abdominal Imaging Section, University of Wisconsin Hospitals and Clinics, Madison, WI. Dr Winter has disclosed that he is on the speaker_s bureau of GE Ultrasound. Drs Lee and Hinshaw have disclosed that they have no financial interests in or relationships with any commercial companies pertaining to this educa- tional activity. All staff in a position to control the content of this CME activity have disclosed that they have no financial relationships with, or financial interests in, any commercial companies pertaining to this educational activity. Lippincott CME Institute, Inc. has identified and resolved all faculty and staff conflicts of interest regarding this educational activity. Reprints: Thomas C. Winter, MD, Department of Radiology, University of Wisconsin Medical School, E3/311 Clinical Science Center, 600 Highland Ave, Madison, WI 53792 (e-mail: [email protected]). Copyright * 2008 by Lippincott Williams & Wilkins Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
Transcript of Ultrasound-Guided Biopsies in the Abdomen and...
Ultrasound-Guided Biopsies in the Abdomen and PelvisThomas C. Winter, MD, Fred T. Lee Jr, MD, and J. Louis Hinshaw, MD
Abstract: Ultrasound-guided biopsies in the abdomen and pelvisare generally more effective, safer, faster, and cheaper than thoseperformed under computed tomography guidance. This manuscriptwill discuss multiple aspects of sonographic biopsies performedbetween the diaphragm and the symphysis pubis. We begin withsystems issues, patient preparation (including bleeding profile andanticoagulant use), pain management, and infection precautions. Theprocedure itself is then analyzed, including needle guidance, the roleof the sonographer, image optimization, patient positioning, core-versus fine-needle aspiration, coaxial versus individual pass, needletechnique, and postprocedure management. Issues specific to dif-ferent sites are then discussed: liver, spleen, pancreas, kidney, adrenal,bowel, retroperitoneum and mesentery, and the pelvis. We finish witha discussion of complications, future trends, and a brief summary.
Key Words: ultrasound, biopsy, guidance, sonography
(Ultrasound Quarterly 2008;24:45Y68)
LEARNING OBJECTIVES1. Identify patient selection and preparation.2. Describe optimal biopsy technique.3. List potential complications.
The advent of percutaneous image-guided biopsy has beena huge boon to patients, generally sparing them the
morbidity of operative procedures for tissue characterization.Ultrasound guidance for these procedures is possible in mostcases in the abdomen and pelvis and is often safer, quicker,and less expensive and has a higher diagnostic yield than otherimage guidance modalities. The goal of this article is topresent techniques for ultrasound-guided biopsies in a varietyof common and not-so-common scenarios in the abdomen andpelvis, potentially expanding the use of sonography in thesesituations and thereby bringing the benefits of ultrasound tomore of our patients.
HISTORYAlthough primacy is notoriously difficult to accurately
assess, some of the earliest ultrasound-guided procedureswere reported in 1972 by Goldberg and Pollack1 with thedemonstration of their dedicated aspiration transducer.2 Com-puted tomography (CT) followed closely behind, with thefirst reported CT-guided biopsy performed by Alfidi et al2 in1975.3 Ultrasound-guided needle placement grew steadily inthe ensuing decades. The aptly entitled article of Dodd et al,4
BSonography: The Undiscovered Jewel of InterventionalRadiology,[ led to even more popularity for sonographicallyguided procedures.
INDICATIONSThe reasons for percutaneous biopsy are broad and
expanding. These include the need for tissue characterizationof an abdominal mass, confirmation of metastatic disease todirect therapy or counsel patients, confirmation of a specifictumor type for a clinical trial (a very large potential futureapplication of percutaneous biopsy as cancer treatmentsbecome more specific for different tumors), evaluation forinfection in a fluid collection, evaluation for parenchymaldisease in native organs (typically the kidney and liver), andevaluation for transplant organ rejection. As abdominalradiologists, we appreciate the potential advantages of high-tech, noninvasive imaging; having said that, we definitelyagree with one speaker who said Bthe most useful additionalMR pulse sequence for lesion characterization is the 18-ganeedle[! Another perspective was given by one of thememorable characters in Samuel Shem’s classic novel, BTheHouse of God,[ who stated Bthere is no body cavity thatcannot be reached with a 14-gauge needle and a good strongarm.[5
What not to biopsy? All medical decision making is arisk-benefit analysis, so there are very few absolute contra-indications to biopsy. An excellent relationship and opencommunication with the referring physician are crucial togood radiological medical decision making; in addition, theradiologist needs to think like a clinician, know his or herpatient’s medical history, and understand the clinical problemto be solved by the biopsy.
For example, performing a biopsy of a highly suggestivehypervascular mass in a cirrhotic liver in the face of anelevated >-fetoprotein (AFP) is not necessary6Vthe very highlikelihood of hepatocellular carcinoma (HCC) in this settingmakes tissue confirmation not worth the small but nonzero riskof bleeding and/or seeding. In the past, percutaneous biopsy ofrenal masses was actively discouraged; recent improvementsin pathological techniques, increasing evidence suggestingthat the risk of tumor seeding is minimal, and new treatmentsfor renal cell carcinoma (RCC), however, have led to a marked
REVIEW ARTICLECME ARTICLE
Ultrasound Quarterly & Volume 24, Number 1, March 2008 45
Received for publication November 14, 2007; accepted January 2, 2008.Department of Radiology, Abdominal Imaging Section, University of
Wisconsin Hospitals and Clinics, Madison, WI.Dr Winter has disclosed that he is on the speaker_s bureau of GE Ultrasound.Drs Lee and Hinshaw have disclosed that they have no financial interests in or
relationships with any commercial companies pertaining to this educa-tional activity.
All staff in a position to control the content of this CME activity have disclosedthat they have no financial relationships with, or financial interests in, anycommercial companies pertaining to this educational activity.
Lippincott CME Institute, Inc. has identified and resolved all faculty and staffconflicts of interest regarding this educational activity.
Reprints: Thomas C. Winter, MD, Department of Radiology, University ofWisconsin Medical School, E3/311 Clinical Science Center, 600 HighlandAve, Madison, WI 53792 (e-mail: [email protected]).
Copyright * 2008 by Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

upsurge in renal biopsies (vide infra). Biopsy of a potentialovarian mass has also been frowned upon; however, whenthe consult is received from a subspecialist gynecologic-oncologist who has reviewed the entire clinical presentation,the biopsy may be in the patient’s best interest and can beeasily and safely performed. Similarly, splenic and bowelwall biopsies are beneficial and safe procedures in theappropriate setting.
CHOICE OF IMAGING MODALITYFOR GUIDANCE
This decision can essentially be simplified to a choicebetween ultrasound versus CT. Although magnetic resonanceimaging (MRI) guidance is possible and has some advantages,in practice the specialized expensive equipment requiredprecludes widespread use of this technology. Fluoroscopy iswidely available but rarely used in soft tissue biopsies of theabdomen and pelvis due to its inherent disadvantages in theseareas. The choice between CT and ultrasound is a multi-factorial decision that should be individualized on a case-by-case basis. In general, a radiologist should consult with thereferring physician and direct each case to the appropriateguidance modality; this direct physician-to-physician commu-nication optimizes patient care and minimizes the probabilityof poor outcomes.
In our abdominal imaging section, approximately 98%of the abdominal and pelvic biopsy procedures are performedusing ultrasound guidance. In 2006, 15% of our 16,000 totalannual ultrasound examinations (these statistics do not includebreast imaging) are procedures involving ultrasound guidancefor needle placement, whether they are simple thoracentesisand paracentesis, easy tissue sampling such as thyroid fine-needle aspiration (FNA), slightly more challenging solid organcore biopsy, or very difficult subcentimeter interaortocavallymph node sampling. In general, if the mass or target canbe seen with ultrasound, a biopsy will be performed underultrasound rather than CT.
Advantages of ultrasound include real-time imagingguidance (safety), speed of use, the ability to compress theabdomen and get closer to your target, lower cost of capitalequipment versus CT, rapid confirmation of complications(bleeding), higher success rates, portability, and lack ofradiation exposure to the patient and medical staff. Advantagesof CT include visualization of certain structures that can bedifficult to see with ultrasound (eg, adrenal, calcified masses,retroperitoneal structures, lung parenchymal lesions) and thecomfort of many radiologists with CT technology. Computedtomography fluoroscopy7 has increased the speed and proce-dure safety with which CT-guided biopsies can be performed,although the radiation exposure associated with this technol-ogy is not trivial.8,9
Several of the advantages listed above in sonography areself-evident (eg, real-time guidance and portability). Othershave been analyzed in a direct fashion. Kliewer et al,10 com-menting on the fact that cost minimization will be one ofthe principal determinants of success in the marketplace asthe economics of health care change in our country, foundthat CT guidance is 1.89 times more expensive than ultra-
sound guidance for percutaneous liver biopsy. In their deci-sion analysis, they justify usage of a 78% probability ofobtaining an adequate sample using CT guidance, versus ahigher 87% for sonographic guidance (although please notethat we are not aware of a randomized trial that actually directlycompares biopsy success rates between CT and ultrasound);in our opinion, the ease of real-time confirmation of needlepassage directly through the lesion with ultrasound is one of theprimary reasons that ultrasound may have a higher adequatesample rate. Although time spent on any procedure dependsheavily on patient selection and operator expertise, one studycomparing durations for ultrasound versus CT guidance forabdominal interventional procedures found an average roomtime of 77 minutes for ultrasound guidance versus 99 minutes(22 minutes longer) for the CT group.11 The advent of CTfluoroscopy has decreased the time necessary for a successfulprocedure when compared with helical CT; these improve-ments in needle placement times have been estimated atbetween 20%9 and 66%.12 However, in one phantom study,ultrasound with a needle guide still required less time than thatwith CT fluoroscopy. This publication also observed thatimprovements in needle placement time generally do not have asignificant effect on overall room time (eg, CT fluoroscopyversus conventional CT), and hence, the costs incurred. Theinherent ultrasound scan biopsy procedure itself is advanta-geous as physicians attempt to cope with the difficultiesbrought upon by the Bobesity epidemic[ in our society13;because of compression applied with the ultrasound probeupon the abdomen, the average distance from the skin surfaceto the lesion was reduced from an average of 8.8 cm with CT to4.5 cm with ultrasound,14 thereby facilitating tissue sampling.
SYSTEMS ISSUESWe have found the following 5 points to be very helpful
in developing a successful biopsy program. First, emphasize tothe sonographers the importance of their personally takingprofessional ownership of a successful biopsy service. Not allsonographers wish to embrace the responsibility inherent ininterventional procedures, but those who enjoy it and take itseriously add immeasurable value to the patient. Second, workclosely with pathologists and cytopathologists to ensure goodcommunication and useful consultation. Third, a dedicatednurse clinician who is available for patient preparation,moderate sedation, and clinician consultation is invaluable.Fourth, standardized paperworks (orders, notes, patienteducation, etc) make the day run smoother. Finally, follow-up is incredibly important for organizational learning. Foreverything except thoracentesis, paracentesis, and thyroidFNA, the patient is called the next day to check on theirwell-being. All procedures are kept in a quality assurancedatabase, and complications are tracked.
PATIENT PREPARATIONThere is an old carpenter’s axiom, Bmeasure twice and
cut once.[ This applies to image-guided biopsies as well, sinceproper planning is probably the single most important factor incourting success. Three quotes emphasize the value of properpreparation: Battention to the little details is the foundation of
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
46 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

excellence[ (Coach John Wooden); Ba pint of sweat will save agallon of blood[ (Gen George Patton); and Bwithoutexecution, vision is just another word for hallucination[15
(Mark Hurd, HP CEO).Preparation begins with open communication with the
referring physician, understanding the patient’s history, anddefining what clinical question is to be solved.
Patient Preparation: Bleeding ProfilePublished studies on bleed rates and bleeding profiles
are tenuous at best. Prothrombin time (PT) and partialthromboplastin time (PTT) are routinely ordered worldwidefor surgical patients, although studies consistently demonstratethe low diagnostic utility of this practice; preoperative PT andPTT values are poor predictors of abnormal bleeding aftersurgical procedures.16 Indices of coagulation in the peripheralblood have been shown to be unreliable indicators of therisk of bleeding after liver biopsy.17 The platelet count isreproducible but does not assess function, thereby providingincomplete and potentially misleading information.18 To quotefrom the seminal paper by Erban et al19 discussing theinappropriate use of the PT and PTT tests, BMany physiciansconsider tests like [these] to be inexpensive, Blittle-ticket[items that will protect them from the hazards of litigation.[ Forthe interested reader, Eckman et al18 provide an excellentreview regarding screening for bleeding risk. They concludedthat BIwithout synthetic liver dysfunction or a history of oralanticoagulant use, routine testing has no benefit in assessmentof bleeding risk.[Multiple studies have shown that obtaining agood history is the most important first step in determiningwhether testing is warranted.
However, partly because we have a large hepatology/liver transplant service and therefore perform invasiveprocedures on many patients with synthetic liver dysfunction,and partly because of the pervasive fear of litigation discussedabove (Bdefensive medicine[), we routinely obtain an inter-national normalized ratio (INR) and platelet count on all intra-abdominal biopsy patients. If the INR is less than 1.5 and theplatelet count is greater than 50,000/mL, we will performalmost any procedure. International normalized ratio of greaterthan 1.5 and/or platelet count of less than 50,000/mL promptsdiscussion of the biopsy with the referring physician.Depending on the location of the target, the type of needleto be used, and so on, a decision is madewhether to supplementthe patient with a transfusion of fresh frozen plasma (FFP)and/or platelets. This is particularly an issue in the biopsyof cirrhotic livers where both INR and platelets are typicallydepressed. We routinely perform diagnostic and therapeuticparacentesis in our population of cirrhotic patients with liverfailure if the INR is less than 2 without any infusion of FFP,but we always carefully look for and avoid the inferior epigas-tric arteries with Doppler before our paracentesis puncture.
What is the proper dose of FFP or platelets to give? Thecomplexity of blood product replacement requires clinicalconsultation for proper patient care. Rough guidelines aregiven here, but realize that the details of this process aregenerally beyond the scope of a radiologist’s practice. Therecommended platelet transfusion dose is 1 U/10 kg of bodyweight when using random-donor pooled platelets; this should
raise the platelet count by 40,000 to 50,000/mL, assumingnormal platelet survival. However, many acutely ill patientshave shortened platelet survival, patients with large spleens(eg, cirrhosis) will have lower platelet recovery, and patientswho have autoimmune thrombocytopenia or who are allo-immunized to donor platelets may be difficult or impossibleto correct. Proper dosing of FFP is also complex. Therecommended dose of FFP is 10 to 20 mL/kg, or 4 to 6 U in theaverage adult (the volume of a typical unit is 200Y250 mL).However, the dose of FFP needed to achieve a given targetgoes up dramatically as the target INR goes down. Table 3(BPredicted Fresh Frozen Plasma Transfusion Volume, Dose,and Expected Factor Improvement for Various Target INRValues[) of the 2006 article by Holland and Brooks20 showsthat if one starts with an INR of 6.0, it will take 1.5 L of FFP tobring the INR to 3; 2.5 L to bring the INR to 1.7; 3.5 L to bringthe INR to 1.5; and 4.5 L to bring the INR to 1.3. Bottom line,please consult liberally with your local hematology experts forissues in this area.
Patient Preparation: Anticoagulant UseThis is another area where the published literature pro-
vides no firm guidance. Many patients are now on long-termanticoagulation (heparin and its derivatives, or warfarin) orlong-term antiplatelet therapy (eg, aspirin, clopidogrel) or aretaking other medications that effect platelet function(eg, nonsteroidal anti-inflammatory agents). The risk of dis-continuing therapy (eg, thrombosis) must be weighed againstthe risk of an increased likelihood of a biopsy-induced bleed.
If the clinical service is comfortable discontinuingtherapy, remember that one must wait ~6 hours afterdiscontinuing heparin and 8 hours (overnight) after disconti-nuing low-molecular-weight heparin (LMWH), although onerecent trial states that one should consider giving the last doseof LMWH the morning of the day before surgery, rather thanour standard practice of giving the last dose the night beforesurgery; again, though, this change should be weighed againstthe risk of thromboembolism.21 Current recommendationssuggest waiting 5 to 7 days after discontinuing aspirin and 7 to10 days after stopping clopidogrel (Plavix) and ticlopidine(Ticlid).22 Nonsteroidal anti-inflammatory drugs (NSAIDs)are a large family, but they do not irreversibly affect plateletfunction the way that aspirin does; thus, our hematologistsstate that a 24-hour discontinuation before the procedure isgenerally sufficient. Warfarin’s duration of action varieswidely, depending on many factors (dose, liver function); ingeneral, we discontinue warfarin about a week ahead of timeand recheck an INR the morning of the procedure. In one trialof patients on long-term anticoagulation undergoing colono-scopic polypectomy for polyps of less than 1 cm, warfarin wasdiscontinued 36 hours before the procedure, and the averageINR on the day of the procedure was 2.3. No bleedingcomplications were identified with 41 polypectomies in 21patients.23 In all cases, reinstitution of medications after aprocedure should be individualized.22
For patients in whom even short-term discontinuation ofwarfarin therapy is felt to be too risky, our standard practice isto discontinue warfarin 5 to 7 days before the procedure andreplace with LMWH. The LMWH is then discontinued the
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 47
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

night before the procedure and restarted the night of theprocedure. Warfarin therapy is reinitiated on the next day. Asalways, close consultation with the referring service leads tooptimal patient management.
Should one ever perform an interventional procedure ina patient who has recently taken an aspirin or NSAID? There isno good evidence-based answer to this commonly occurringand vexing issue. In an informal survey of colleagues whoperform many ultrasound-guided procedures, some labora-tories hold firm to this rule and refuse procedures until therequisite time off the drug has passed, primarily over fear oflitigation in the setting of an adverse outcome rather than anytrue scientific sense that this is intrinsically dangerous. Othercolleagues share our opinion that this is too severe a practice,potentially leading to great patient inconvenience (eg, thepatient who lives 5 hours away and has taken 2 days off workfor a liver or thyroid biopsy, having failed to get the messagethat he should discontinue his daily baby aspirin 5 daysbefore). After a thorough discussion of the possible theoreticalincrease in risk with the patient and giving him or her theoption of rescheduling for a future date, we will typically goahead and perform the biopsy in this setting; conversely, in theretired patient who lives 10 minutes from our hospital and forwhom it is no true inconvenience to reschedule, we willusually delay the procedure until these drugs have beenstopped for an adequate period.
There are data to support performing low-risk biopsiesin patients on aspirin or NSAIDs. First, an editorialist statesthat maintaining patients who are at substantial risk forcardiovascular events on aspirin yields good results fortherapeutic endoscopic procedures.24 Second, many opensurgical procedures, especially vascular, are performed inpatients who are anticoagulated or on aspirin due to afavorable risk-benefit ratio. Third, a UK expert writing onguidelines for liver biopsy states that BIeven though theingestion of aspirin and other NSAIDs in the week prior toinvasive intervention is a recognised contraindication byseveral authoritiesIthere are, to our knowledge, however, noconvincing data to support this as a contraindication topercutaneous liver biopsy.[25 Fourth, a review of the issue oflow-dose baby aspirin in patients undergoing ultrasound-guided transrectal biopsies of the prostate identifies 2 studiesthat found no increased risk of hemorrhage in the groups onaspirin.26 Finally, a Radiological Society of North Americapresentation in 2005 looked specifically at the risk ofsignificant hemorrhage resulting from image-guided corebiopsy in patients taking aspirin.27 In this study of 6073biopsies, the authors concluded that Bthere is an elevated riskof significant bleeding complications in those patients takingaspirin at the time of percutaneous biopsy. However, this riskis small and should not preclude biopsy in most cases.[ Infact, although not statistically significant, in their subset ofpatients undergoing liver biopsy, the hemorrhage rate inpatients taking aspirin was approximately half that of thosenot taking it (0.46% vs 0.93%). In summary, as in all ofmedicine, optimal care results from treating each patient as anindividual and fully discussing the pros and cons of anypotential course of action so that the patient may make aninformed choice.
Pain ManagementAdequate pain control is not only a moral imperative,
but it has high political priority as well. Pain managementguidelines implemented by the Joint Commission on Accred-itation of Healthcare Organizations in 2001 mandate regularassessment of pain and the establishment of policies andprocedures that support the appropriate use of pain medica-tion.28 A comfortable patient makes an abdominal biopsy amuch easier procedure all the way around! Pain managementcan be simplified into the BGolden Rule[; how would you likeyourself or your mom to be treated? There are 3 componentsto adequate pain relief: psychosocial, local anesthesia, andmoderate sedation.
PsychosocialIt has been shown again and again that obvious care,
concern, and warmth from the medical team result indecreased patient anxiety and perceived pain. Follow commonsense tactics such as making sure that the patient is at acomfortable temperature, that there are no bright lights in thepatient’s eyes, and so on. Think about how you prepare thepatient. For needles that can be test fired before use (readthe package insert; some of the older devices recommendagainst testing), there is a world of difference between facingthe patient with the needle fully visible, close to his face,and stating, Byou will hear a bang from the gun as I fire it,[versus turning your back to the patient and blocking view ofthe needle and calmly stating, Byou will hear a click from thespring in the biopsy device as I test it.[ Consider your wordchoice and the subsequent mental state you engender as youinject the lidocaine. Our orientation packet for the residentsincludes a superb article entitled, BCan Words Hurt? Patient-Provider Interactions During Invasive Procedures.[29 Usingwords similar to Ba bee sting[ or Ba sharp jab[ before instillinglocal anesthesia may engender more perceived pain thanneutral statements such as Byou’ll feel cool tingling with thespreading of the numbness.[ Although we do not practiceovert hypnosis routinely, there is a body of work on themedical utility of hypnosis in minor (and occasionally major)invasive procedures; if interested, peruse the Web site of theAmerican Society for Clinical Hypnosis (http://www.asch.net/genpubinfo.htm).
Local AnesthesiaWe use 1% lidocaine buffered with 8.4% sodium
bicarbonate in a 9:1 ratio. Although somewhat controversial,the buffering is generally reported to decrease the Bstinging[sensation of the lidocaine injection.30 On a practical note, therate of injection is often the most important factor for makingthe injection more tolerableVslow is good. When performinglocal anesthesia, start with a subdermal injection of 2 to 3 mLof lidocaine using a 30-gauge needle (note how small this is,rather than the typically provided 22- or 25-gauge diameters),followed by deeper anesthesia with a 22-gauge spinal needle(through the biopsy guide, if you are using one). Thistechnique ensures a cylinder of anesthesia along the path of thebiopsy and gives a Bpreview[ of the biopsy trajectory; thelatter is useful if there are ribs or other structures to be avoided
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
48 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

along the way. Make sure that all air has been purged from thesyringe and needle as air can cause obscuration of the needleor target (Fig. 1)! Be sure to place several milliliters oflidocaine directly on the peritoneal surface and at the liver (orother organ) capsule. Do not puncture the liver or othervisceral organ because anesthetizing the liver parenchyma willnot decrease the pain of the procedure and may increase therate of bleeding. Use lidocaine liberally. We routinely give10 mL, and there is no risk of lidocaine toxicity in giving20 mL as necessary. More specifically, the maximumpercutaneous dose of lidocaine without epinephrine in healthyadults is 4 mg/kg, up to 300 mg. Because there is 10 mglidocaine/mL in a 1% solution, this represents a maximumdose of 20 to 30 mL for most patients. Busy physicians takenote: lidocaine requires time to diffuse through the tissues, soallow a few minutes before biopsy after local anestheticadministration to minimize discomfort.
Moderate SedationThe third tool for pain management is moderate sedation
(previously referred to as Bconscious sedation[). If the patientis treated appropriately, and copious local anesthetic isproperly administered, moderate sedation is usually notnecessary for routine liver biopsies; however, if a nurse isreadily available, if the biopsy looks to be particularly difficult,or if the patient is particularly anxious, we will certainly useintravenous medications, typically fentanyl (Sublimaze) andmidazolam (Versed). We almost never use moderate sedationfor thyroid biopsies, superficial lymph node biopsies,thoracenteses, or paracenteses. Conversely, transvaginalbiopsies may be quite painful, so moderate sedation is almostalways used here.
If moderate sedation is used, make sure that it is donesafely. Most hospitals now require special credentialing andprivileging to perform sedation, and many also require consentfor the sedation as well as the procedure itself. Themedications should be administered in small aliquots,typically 50 Kg of fentanyl and 1 mg of midazolam, althoughin elderly, very sick, or small patients, we will often halve
these doses. Always monitor oxygen saturation, pulse, andblood pressure throughout the procedure and afterward in thededicated recovery area. Oxygen, suction, and airwaymanagement equipment should be readily available. Althoughalmost never needed if fentanyl and/or midazolam areappropriately administered, reversal agents (naloxone andflumazenil) should be easily accessible. Keep your advancedcardiac life support skills current.
Infection PrecautionsTo drape or not to drape? We always drape the probe for
guided biopsies (for thoracenteses and paracenteses, weusually mark the spot and do not use the transducer duringneedle placement). I am not aware of any literature thatdocuments that this extra step decreases the risk of infection.In fact, several very experienced centers of excellence (MayoClinic, Italian groups) do not sterilely drape the probe unlessthe patient is known to have HIV infection and instead simplycleanse and disinfect the transducer before and after eachbiopsy; they have had no known issues with this protocol. Thedisadvantages to draping include time, cost, and potentialdegradation of image quality (although the latter is moretheoretical than real in our opinion). If chemical disinfectionis used (eg, alcohol, povidone-iodine [Betadine]), ensure thatthe substance used is compatible with the transducer surfaceand manufacturer’s recommendations.
Skin PreparationWe now use chlorhexidine 2%/isopropyl alcohol 70%
(Chloraprep) rather than povidone-iodine 10% (Betadine).Both are adequate, but the former has better antimicrobial ac-tivity, does not stain or itch, and works quicker. Read the pack-age insert for application instructions, and take care to applywith a back-and-forth action for a full 30 seconds, and then letair dryVdo not blot or wipe. Only 1 application is required.
Needle SafetyBe careful! There is a veritable alphabet of pathogens to
be wary of. In addition to HIV, there are a variety of hepatitis
FIGURE 1. Inadvertently injected air obscuring the target. A, White arrow on CT denotes a soft tissue mass that was laterbiopsy proven to represent peritoneal carcinomatosis from rectal cancer. The high-density structure just anterior to the noduleis a hepatic arterial infusion pump. B, Arrow denotes nodule on ultrasound. C, Although the lidocaine syringe was flushed of air,the dead space in the numbing needle after the stylet was removed contained enough gas to seriously degrade the ultrasoundimage. Note how the nodule is now barely visualized behind the shadow caused by the injected air.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 49
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
strains which currently run from hepatitis A through G. Themost important of these are hepatitis B virus, for which avaccine is available (make sure to check your antibody re-sponse to ensure you are adequately immunized), and hepatitisC virus, for which no vaccine is available. Despite all of ourprecautions, we average about 1 needlestick in our laboratoryevery year. Protect yourself, the sonographer you work with,and the cytopathologist you are passing the needle to.
OTHER BIOPSY ISSUES
GuidanceMechanical biopsy guide versus freehand. Both systems
work well if the operator is comfortable with the technique.Freehand technique offers the possibility of better needlevisualization (more specular reflection if angles are chosenappropriately) but generally requires more skill and experi-ence. In one study, a phantom model of lesions in the humanliver with simulated overlying ribs was used to comparefreehand and probe-guided techniques31; the authors con-cluded that there was a time benefit to the use of probe guides
but that this benefit was greatest for inexperienced operators.In our laboratory, most deep abdominal biopsies areperformed using a biopsy guide, whereas superficial biopsies(eg, thyroid, breast, groin) are performed freehand. Remem-ber, though, that a guide is just a guide, not a guarantee,particularly with thin needles, cirrhotic (hard) livers, and/orany firm overlying structures (eg, ribs) that may deflect theneedle (Fig. 2). If consistent deviation to one side is observed,one can adjust the projected trajectory outside the lesion tocompensate for the amount of deviation (similar to compen-sating for wind or elevation issues through the site of a rifle)(Fig. 3).
Role of the SonographerSome laboratories have the radiologist guide the pro-
cedure while the needle is placed; this requires more manualdexterity but allows more direct control of needle placement.However, in our laboratory, the sonographers scan and guidebiopsy procedures for several reasons: they are usually the besttechnical scanners; the large number (~2400/yr) of needleguidance procedures done by ultrasound in our laboratory
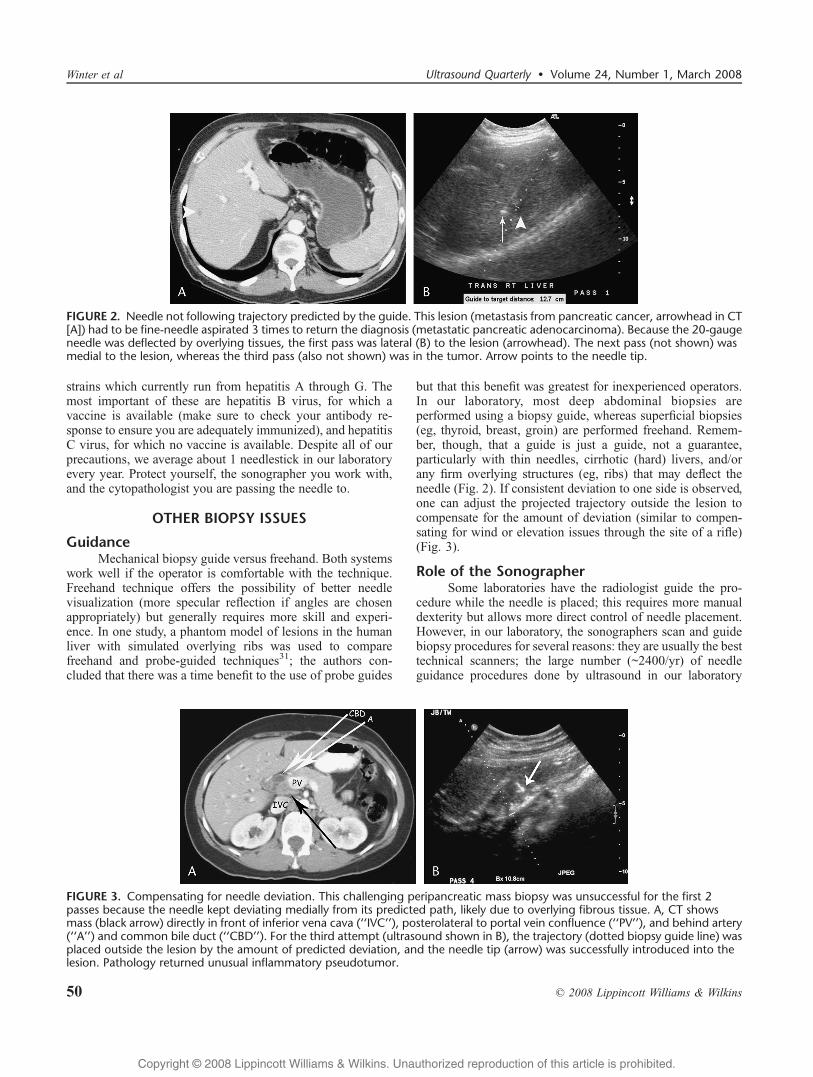
FIGURE 3. Compensating for needle deviation. This challenging peripancreatic mass biopsy was unsuccessful for the first 2passes because the needle kept deviating medially from its predicted path, likely due to overlying fibrous tissue. A, CT showsmass (black arrow) directly in front of inferior vena cava (‘‘IVC’’), posterolateral to portal vein confluence (‘‘PV’’), and behind artery(‘‘A’’) and common bile duct (‘‘CBD’’). For the third attempt (ultrasound shown in B), the trajectory (dotted biopsy guide line) wasplaced outside the lesion by the amount of predicted deviation, and the needle tip (arrow) was successfully introduced into thelesion. Pathology returned unusual inflammatory pseudotumor.
FIGURE 2. Needle not following trajectory predicted by the guide. This lesion (metastasis from pancreatic cancer, arrowhead in CT[A]) had to be fine-needle aspirated 3 times to return the diagnosis (metastatic pancreatic adenocarcinoma). Because the 20-gaugeneedle was deflected by overlying tissues, the first pass was lateral (B) to the lesion (arrowhead). The next pass (not shown) wasmedial to the lesion, whereas the third pass (also not shown) was in the tumor. Arrow points to the needle tip.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
50 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
contributes to a high level of expertise and experience by thesonographers in the face of a constantly changing group ofresidents and fellows, thereby enabling us to deliver moreuniform quality; the division of labor enables all participantsto concentrate on a single task (sonographers on the probeand guidance, and sonologists on passing the needle andmanaging the specimen); and the fact that the most difficultand challenging biopsies require abdominal compression,awkward transducer angulation, and/or prolonged targeting,which can be nearly impossible to perform by a single operator.
Image OptimizationThis is perhaps one of the most important aspects of any
nontrivial biopsy. First, choose the correct transducer. Toquote Prof Faye Laing, Bin ultrasound, always start high, thengo low.[ That is, attempt to use the highest possible frequencytransducer. Many superficial liver lesions, especially those inthe left hepatic lobe, can be imaged with high-frequency lineartransducers (the Bsmall parts[ probes); the better depiction ofthe target inherent with these transducers makes biopsieseasier and enables one to reliably hit smaller masses (Fig. 4).If the lesion cannot be seen with a high-frequency lineartransducer, try a lower-frequency linear (Bvascular[ probe) orhigh-frequency curved linear array. If those do not work, moveto a low-frequency curved linear probe, and only if all of thesefail, use the small footprint sector/vector/phaser probe. These
latter probes are often necessary for deep lesions that areaccessed between ribs, but should not generally be your firstchoice. Second, optimize your gray-scale image. Zoom in, putyour focal zones at the area of interest, and try harmonics;we have found that compound imaging technology greatlyimproves needle visualization.
Seeing the NeedleAfter the gray-scale image has been optimized, what can
one do to help visualize the needle? Obviously, the moreperpendicular the sound beam is to the needle, the stronger thereflection will be. Move the inner stylet in and out withoutactually moving the outer needle; this saves tissue trauma andoften is all that is needed to find the needle. Rotating theneedle often allows optimization of the specular ultrasoundreflection from asymmetric needle tips. If these maneuversfail, then judiciously moving the needle back and forth is oftenuseful. Echogenic needle coatings are not a cure-all, but do aidin needle detection32 with very little additional cost. Someauthors have described using color Doppler to locate a movingneedle tip, but in our experience, the artifact associated withthis generally limits its usefulness.
Patient PositioningMany practitioners inadvertently assume that biopsy
should be performed with the patient in supine position,
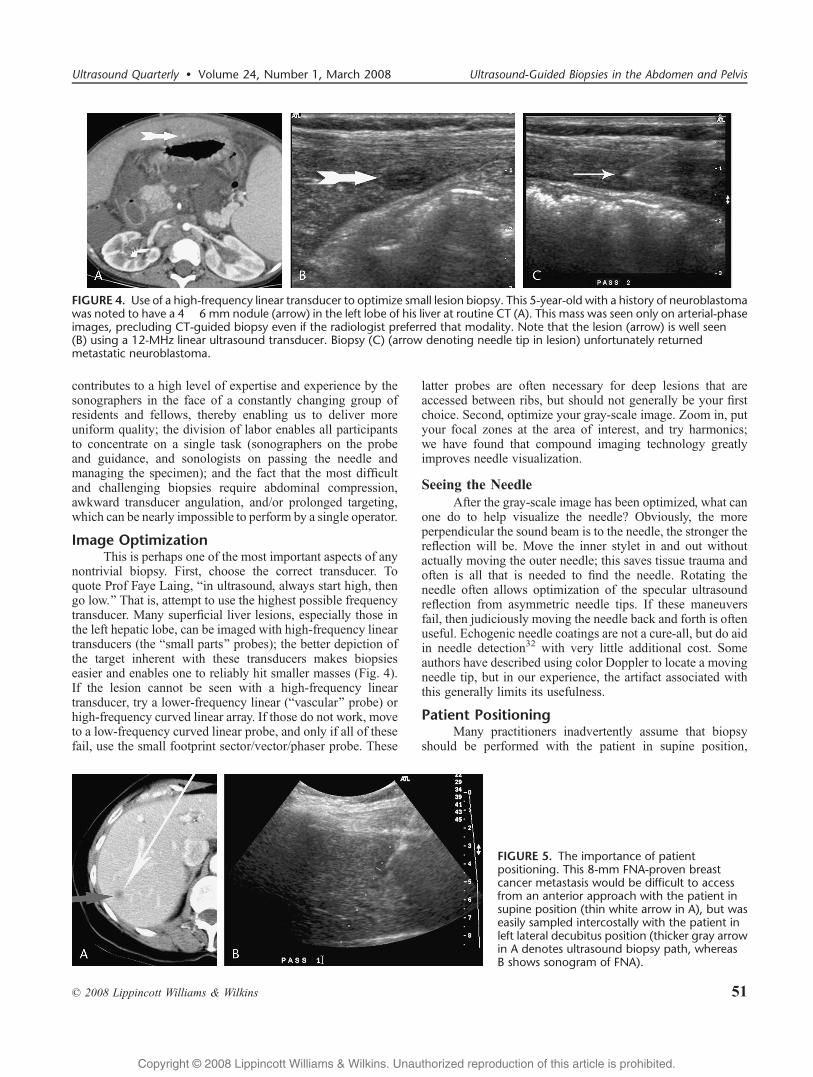
FIGURE 5. The importance of patientpositioning. This 8-mm FNA-proven breastcancer metastasis would be difficult to accessfrom an anterior approach with the patient insupine position (thin white arrow in A), but waseasily sampled intercostally with the patient inleft lateral decubitus position (thicker gray arrowin A denotes ultrasound biopsy path, whereasB shows sonogram of FNA).
FIGURE 4. Use of a high-frequency linear transducer to optimize small lesion biopsy. This 5-year-old with a history of neuroblastomawas noted to have a 4 � 6 mm nodule (arrow) in the left lobe of his liver at routine CT (A). This mass was seen only on arterial-phaseimages, precluding CT-guided biopsy even if the radiologist preferred that modality. Note that the lesion (arrow) is well seen(B) using a 12-MHz linear ultrasound transducer. Biopsy (C) (arrow denoting needle tip in lesion) unfortunately returnedmetastatic neuroblastoma.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 51
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

similar to the positioning used for most CT scans. Althoughthis often works well for left lobe liver and pancreatic biopsies,other targets are often more optimally accessed with thepatient in oblique, decubitus, or even prone positions (Fig. 5).Spend time scanning and preparing ahead of time with this inmind, and potentially difficult procedures can often be easilyconverted to very manageable ones.
Core Versus FNAThe choice between cytology (FNA) and pathology
(core) is multifactorial and is often based on institutionalaccess and expertise. If cytology service is not available duringthe procedure to assess the adequacy of a specimen, a corebiopsy is often the best choice. The smaller needles possiblewith cytology (20- to 25-gauge) are associated with aprocedure that is likely safer as well as more comfortable forthe patient. In general, cytological aspiration should beconsidered in patients with a known malignancy and a highpretest probability that the area on which a biopsy will beperformed is a metastasis; hypervascular lesions; massessurrounded by certain structures (ie, bowel, blood vessels)where trauma needs to be minimized; and epithelial tumors(adenocarcinomas and squamous cell carcinomas). Althoughthere is a great variety of opinion on this matter,33 our cytologyteam believes that better FNA samples are obtained with thesmallest possible needle (eg, 25-gauge for a thyroid FNA) andno suction, just vigorous back-and-forth motion to pack theneedle with cells. Larger needles and syringe suction givefewer diagnostically adequate samples due to dilution withblood products14 and are reserved for the rare scirrhous lesionthat fails to shed cells with the smallest gauge needle.Interestingly, and perhaps somewhat counterintuitively, thereare very little data suggesting that appropriate use of an18-gauge needle is any more dangerous than using a smallerFNA needle.34
Biopsies are usually more appropriately performedusing automated cutting needles in cases other than thosejust listed, particularly lymphoma, RCC, and hepatoma.Although both work well, we generally prefer the newercylindrical full-bore cutting needles to the older side-notchneedles, because one obtains significantly more tissue per corefor analysis than the former for a given puncture diameter(Fig. 6). If a small bowel loop needs to be traversed to get tothe mass, try to use no larger than a 20-gauge needle. Corebiopsy specimens can be assessed for adequacy by either
Btouch-prep[ (the cytology team rolls the core on a glassslide and performs cytological analysis on the shed cells)or, often with high accuracy, by simple visual inspection(Fig. 7). Interpretation of cytology specimens is not onlyoperator dependent but also inappropriate for some tumortypes, and thus, the decision to obtain cytological orpathological specimen in a given patient should be individ-ualized on a case-by-case basis; consult with your cliniciansand pathology experts regarding the clinical question thatneeds to be answered and the best method for getting tothat answer.
Coaxial Versus Multiple Separate PassesShould one place a larger bore introducer needle and
sample (either FNA or core biopsy) multiple times throughthis, or should one serially perform multiple separate passeswith a smaller bore needle? As with many of theBcontroversies[ regarding technique in the biopsy arena,there is a paucity of hard, evidence-based data regarding thisquestion. Our general preference and practice is to performmultiple separate passes with a smaller bore needle. Anexception is made when the initial needle placement is verychallenging; in these cases, we will place an introducer andsample coaxially through it.
FIGURE 7. Core biopsy of HCC specimen on Telfa pad showsdark cirrhotic liver (mahogany color in real life) at either endand pale white tumor tissue (arrows) in the center.
FIGURE 6. Traditional side-notch core needle (A), newer cylindrical full-bore core needle (B), and differences in pathologicalspecimen area (C).
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
52 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

One article suggested that the strategy of multipleseparate needle passes might have a higher successful yieldrate because slightly different areas of the target (due to theinevitable slight differences in needle positioning inherentwith this technique) are sampled, thereby avoiding repeatedlysampling a necrotic or nondiagnostic area.35 Anothertheoretical advantage to this technique is that if samples areperformed during suspended respiration (as we always do),one does not shear or tear the capsule (liver, kidney, pleura,peritoneum) but rather makes focal discrete punctures thatmay have less tendency to bleed. Disadvantages to thisstrategy include multiple holes in the covering capsule (asopposed to just 1 hole with coaxial technique) and the fact that,for very difficult and challenging biopsies, one has tosuccessfully navigate the needle to the lesion multiple times.
The coaxial technique makes it easy to obtain multiplesamples once the introducer needle is placed. There isgenerally only 1 hole in the capsule. Normal tissue is relativelyprotected from the trauma of multiple needle passages.Disadvantages of the coaxial technique include potentialshearing of the capsule (because the introducer is generally leftin during quiet respiration between samples), a larger puncturehole in the capsule, and repetitive sampling of the same area. Apostulated but unproven advantage is less chance for trackseeding because the needle that samples the tumor iswithdrawn through the inside of the introducer needle. Theissue of the true risk of track seeding is very controversial, but
1 article that evaluated the use of a 17-gauge introducer withan 18-gauge biopsy needle in 128 patients with proven HCCfound a 0% incidence of track seeding with a mean follow-upof 410 days36; however, 8 (6.25%) of these patients also had anepisode of bleeding within 24 hours of biopsy that requiredhospital admission, fluid resuscitation, and/or transfusion.This 6.25% bleed rate is significantly higher than the 0% to1.4% rates published in several other series, and it is possiblethat this increased risk is related to the coaxial technique.
Needle TechniqueIn choosing a needle path, consider the intervening
structures (ie, attempt to avoid vasculature and bowel,although small bowel can generally be traversed safely witha 20- to 22-gauge needle), and usually select the shortest pathfrom skin to lesion. The needle should be advanced duringsuspended respiration with a firm, continuous motion tominimize pain and to keep the needle on target. Also, theneedle tip is usually much easier to see when it is in motion.Slow and tenuous needle passes tend to deflect rather thanpuncture structures (like the liver capsule), decrease the abilityto see the needle tip, and increase patient pain, especially whentraversing the peritoneum or visceral structures sensitive tostretching; thus, a brisk puncture is optimal when passingthrough these coverings.
Is biopsy through ascites safe? In a word, yes. Older,anecdotal teachings stated that biopsy through surrounding
FIGURE 8. Hepatic biopsy through ascitesis safe (see text). Needles (arrows = tip) areshown passing through ascites (‘‘A’’) intohepatic metastases from ovarian cancer(A, first patient) and endometrialcarcinosarcoma (B, different patient).
FIGURE 9. The ‘‘Don’t Look Afterwards’’ school. Gray-scale (A), color Doppler (B), and pulsed Doppler (C, black-and-whitereproduction of original color image) images of a jet of blood (arrow) flowing into surrounding ascites following renal transplant(‘‘RTX’’) biopsy. Images 15 minutes later (not shown) show a small amount of blood, but the patient did fine and was asymptomaticthe entire time.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 53
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

fluid was a (relative) contraindication, presumably becausethere would be no tissue tamponade of the puncture site.However, several studies have shown that, at least in the caseof the liver, the presence of ascites does not alter complicationrates37,38 (Fig. 8).
PostprocedureImaging
There is no consensus as to whether one should imageafter a biopsy to assess for potential complications. The Bno[group feels that the patient should simply be assessedclinically (Btreat the patient, not the lab test[ school ofthought), that most bleeds are small and resolve sponta-neously, and that imaging of these asymptomatic hemorrhagesleads to unnecessary excitement and overtreatment (Fig. 9).Others state that postprocedure imaging is useful in predictinghigh-risk groups for more careful follow-up. For example, arecent article by Kim et al39 showed that a negative Dopplerbiopsy track immediately after biopsy had a 100% negativepredictive value for postprocedural hemorrhage, whereasDoppler detectable flow in the track and again at 5 minuteslater had a positive predictive value of 75% for postbiopsybleeding (Fig. 10).
MonitoringFollowing an intra-abdominal biopsy, we observe the
patient for ~4 hours in a dedicated recovery area with frequent
vital sign monitoring; this is a Joint Commission on Accredi-tation of Healthcare Organizations requirement if moderatesedation has been administered. We do not obtain routinepostprocedure hematocrit/hemoglobin levels if the patient isasymptomatic. The patient must be awake, alert, and able tohold down fluids before discharge. The patient should have aride home from the hospital, appropriate instructions aboutwhat to do if questions or complications arise, and know theprotocol for contacting his or her physician to discuss thebiopsy results. Good communication and patient teaching helpprevent unfortunate outcomes such as the patient who had aliver biopsy, returned to his home 2 hours away, had mild pain,and went to the local emergency room where the on-call sur-geon heard the words Bliver biopsy today[ and then performedunnecessary exploratory celiotomy for a small bleed that easilycould have been managed conservatively.
SPECIFIC SITES
LiverThe liver is likely the most commonly percutaneously
biopsied solid abdominal organ. Liver biopsies can be dividedinto Bmedical[ biopsies, acquiring tissue from a random sitein the hepatic parenchyma to assess for diffuse disease (eg,staging hepatitis C damage, assessing cirrhosis, or gradingrejection after transplant), versus Bsurgical[ biopsies, target-ing a specific suspicious lesion in the liver. The former hasoften been (and still often is) performed Bblindly[ with just
FIGURE 11. Biopsy complication. Severe painafter a nonradiology-performed ‘‘blind’’ liverbiopsy (no image guidance was used)prompted a postprocedure CT. Scout view (A)denotes a large mass in the right abdomen(black arrows), shown to be a large hematoma(white arrows) on axial imaging (B). Thepatient required several blood transfusionsbut recovered.
FIGURE 10. An example of the Doppler ‘‘patent track’’ sign immediately after liver biopsy (see text). A, Note blood flow withintrack (arrow) extending to the liver capsule (arrowheads). This flow was absent at 5 minutes (B, black-and-white reproduction oforiginal color image), and the patient remained asymptomatic. Unfortunately, multiple lesions visible in both images representmetastatic pancreatic adenocarcinoma.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
54 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
palpatory guidance, but intuition and data suggest thatsonographic guidance leads to a safer procedure (Fig. 11).Left lobe access for ultrasound-guided medical liver biopsy isperhaps minimally easier and safer and is therefore our firstchoice, but we will readily move to the right lobe if access isbetter. A subcostal approach during suspended inspiration isdefinitely preferred, but we often use an intercostal approachas necessary. Needle insertion below the 12th rib posteriorlyor the 10th rib laterally should avoid pleural transgression40;however, we have not experienced a pneumothorax from atranspleural needle passage as long as we punctured below theaerated lung (which can easily be seen on ultrasound). Wetypically find that a single, 18-gauge, 3.3-cm-long core using afull-bore-type needle (vide supra) provides sufficient tissue,but work closely with your clinicians and pathology depart-ments to determine the specimen volume required.
Surgical (targeted lesion) biopsies by definition limit theoptions available for approach to the lesion. Close attention todetail and careful application of the principles already coveredwill maximize success; many of the principles discussedabove were written based specifically on experience with liver
biopsies. However, several other relatively unique issuesapply to the liver and not as much to other deep abdominal orpelvic biopsies.
Intercostal biopsies, often necessary for high domelesions, run the risk of traversing the pleural space (asexpected, the risk is higher at 10 to 11 than it is at 11 to 12).Pneumothorax, however, is extremely unusual if sonographicguidance is used to identify and consciously avoid aeratedlung parenchyma (Fig. 12).
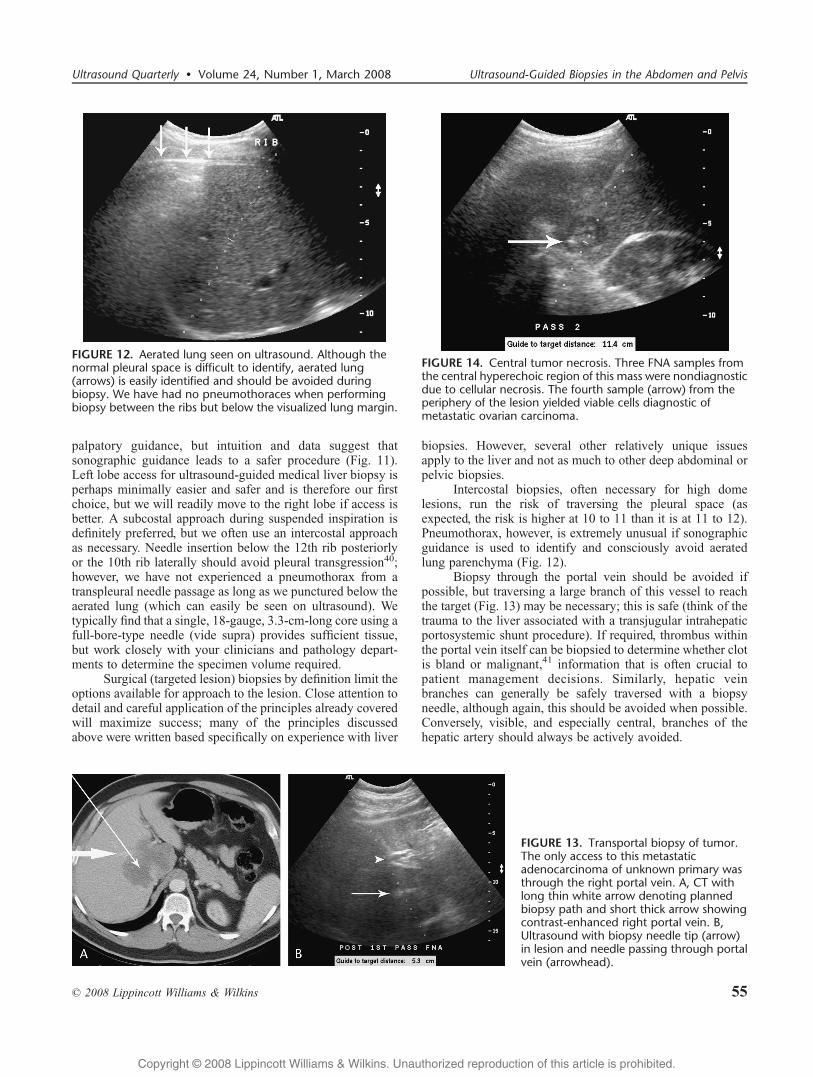
Biopsy through the portal vein should be avoided ifpossible, but traversing a large branch of this vessel to reachthe target (Fig. 13) may be necessary; this is safe (think of thetrauma to the liver associated with a transjugular intrahepaticportosystemic shunt procedure). If required, thrombus withinthe portal vein itself can be biopsied to determine whether clotis bland or malignant,41 information that is often crucial topatient management decisions. Similarly, hepatic veinbranches can generally be safely traversed with a biopsyneedle, although again, this should be avoided when possible.Conversely, visible, and especially central, branches of thehepatic artery should always be actively avoided.
FIGURE 13. Transportal biopsy of tumor.The only access to this metastaticadenocarcinoma of unknown primary wasthrough the right portal vein. A, CT withlong thin white arrow denoting plannedbiopsy path and short thick arrow showingcontrast-enhanced right portal vein. B,Ultrasound with biopsy needle tip (arrow)in lesion and needle passing through portalvein (arrowhead).
FIGURE 14. Central tumor necrosis. Three FNA samples fromthe central hyperechoic region of this mass were nondiagnosticdue to cellular necrosis. The fourth sample (arrow) from theperiphery of the lesion yielded viable cells diagnostic ofmetastatic ovarian carcinoma.
FIGURE 12. Aerated lung seen on ultrasound. Although thenormal pleural space is difficult to identify, aerated lung(arrows) is easily identified and should be avoided duringbiopsy. We have had no pneumothoraces when performingbiopsy between the ribs but below the visualized lung margin.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 55
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

Should hemangiomas be biopsied? We have performedcore biopsies and FNAs on many hemangiomas withoutincident in our careers. Although there is no reason to sample aclassic-appearing hemangioma in a low-risk patient42; manypatients have atypical-appearing hemangiomas or high-riskhistories, leading to a very reasonable desire from the clinicalservice for definitive tissue assessment. Given that heman-gioma incidence in the adult population has been reported inup to 20%,43 it is inevitable that biopsy will be performed onthese lesions, and there is no convincing evidence to suggestthat it is unsafe to do so.
If multiple samples from the center of a lesion arenondiagnostic, this may be due to central tumor necrosis; toobviate this problem, sample the rim of the lesion where moreviable cells may be present (Fig. 14).
Whenever possible, attempt to perform biopsy on alesion through a cuff or rim of normal overlying liver.Although there are no good data to support this recommenda-tion, and although wewill perform biopsy directly into a lesionif no access is possible through normal liver, it makes sensethat an overlying layer of normal hepatic parenchyma (Fig. 15)may decrease postbiopsy bleeding and possibly tumor seedingas well.
Should potential hepatomas be biopsied? If necessary,yes, although this is controversial. Hepatomas may have ahigher risk of bleeding (Fig. 16) and/or seeding (Fig. 17) than
other pathologies. Therefore, intersociety guidelines havebeen proposed44 that state that clinical and noninvasiveimaging data may be used in certain circumstances to reliablymake this diagnosis without biopsy. For example, a lesion ofgreater than 2 cm that has arterial-phase hypervascularityon CT or MRI, combined with a serum AFP of more than400 ng/mL, does not need tissue diagnosis. In equivocalcases, though, it is reasonable to biopsy a potential HCC fortissue characterization.
SpleenTo quote from a 1999 Duke article,45 Bthe reluctance to
perform splenic needle aspiration comes from the unfounded(italics added) perception that this procedure is a dangerousone with a high risk for hemorrhageI.[ The belief thatsplenic sampling is unsafe is not backed by data; for example,Soderstrom46 reported more than 1000 splenic FNAs thatwere performed without complications. Although, as with allinvasive procedures, complications may occur,47 splenicbiopsy complication rates are well within the limits associatedwith biopsy of other abdominal organs.45 A biopsy can besafely performed on the spleen under sonographic guid-ance,48,49 even in children.50
A 2007 study of 43 splenic biopsies showed that18-gauge needles had a higher diagnostic rate comparedwith 21-gauge needles, with no increased incidence of
FIGURE 15. This peripheral carcinoid metastasis(CT [A] and ultrasound [B]) was successfullysampled through a thin wedge of overlyingnormal liver (arrow). Note also the use of a lineartransducer for improved biopsy visualization.
FIGURE 16. Ruptured hepatoma (HCC). A, CT showing HCC (arrow) before biopsy. B, Large perihepatic intraperitoneal hematoma(arrowheads) following FNA with 25-gauge needle (L indicates liver). C, Gross specimen after surgery showing rupturedhepatoma (arrow) in cirrhotic liver.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
56 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
complications, and thus recommended the use of 18-gaugecutting needles for ultrasound-guided splenic lesion biopsy.51
Although this conclusion has been reached by other authorsas well, close communication with the clinical team andpathology department provides optimal patient care; we maystart with core biopsy for suspected lymphoma (Figs. 18 and19) but will otherwise often start with FNA and then move tocore only if necessary.
PancreasA biopsy can be safely performed on the pancreas under
sonographic guidance.52,53 Biopsy for suspected adenocarci-noma is usually only performed when the lesion is thought tobe unresectable; if there is any chance for surgical extirpation,the patient typically goes straight to the operating room,thereby bypassing the potential minimal risks and problemsinherent in any type of image-guided biopsy. Percutaneousbiopsy often necessitates a transgastric approach (Fig. 20);either FNA or core technique can be used. We generally startwith FNA, but given the scirrhous nature of most adenocarci-nomas, insufficient tissue is not infrequently obtained; there-fore, in those cases, we escalate to core biopsy.
Although I am not aware of good evidence to supportthe recommendation that normal tissue should always beavoided to minimize the risk of biopsy-provoked pancreati-tis,54 this seems like a reasonable tenet and can usually beeasily implemented. Seeding after biopsy is generally not aclinical problem given the dismal prognosis of patients withthis disease, but animal studies suggest that 100 to 10,000cells may be deposited along the track with just one pass55;potential improvements in chemotherapy in the future maymake this consideration more important as patients survivelonger. A recent trend includes a movement toward endo-scopic ultrasound (EUS)Yguided FNA of pancreatic adeno-carcinoma, away from image-guided percutaneous sampling,
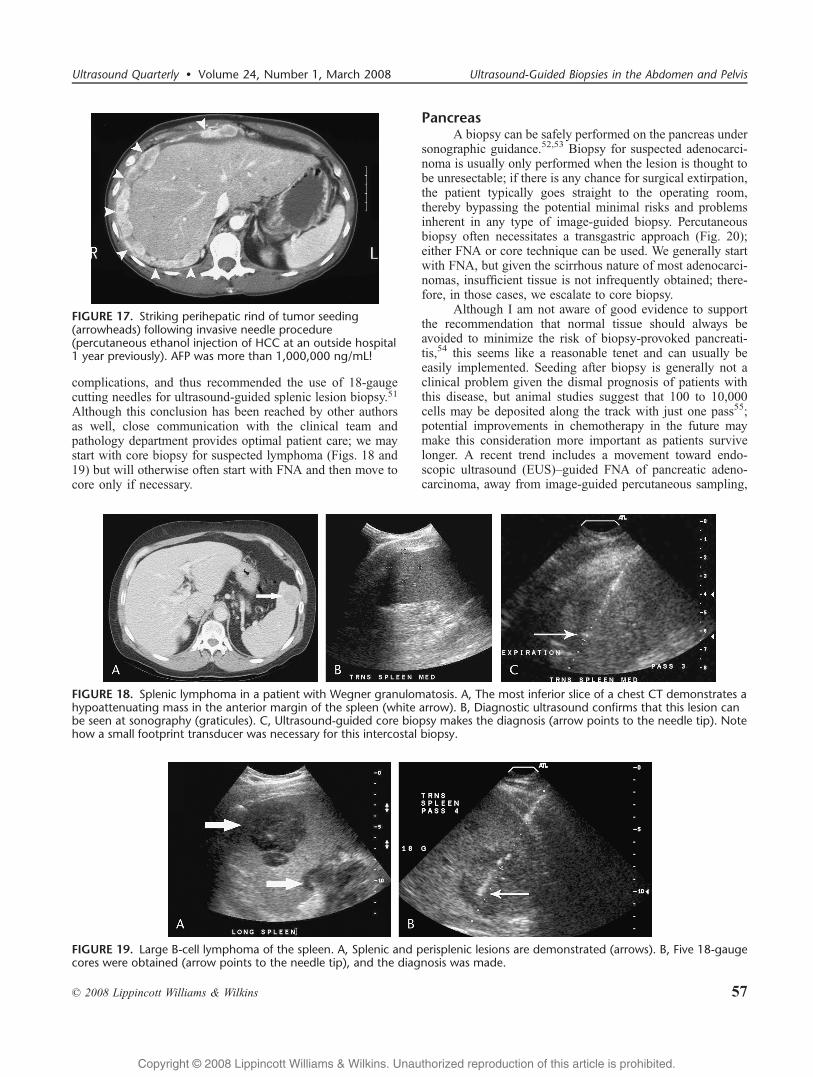
FIGURE 17. Striking perihepatic rind of tumor seeding(arrowheads) following invasive needle procedure(percutaneous ethanol injection of HCC at an outside hospital1 year previously). AFP was more than 1,000,000 ng/mL!
FIGURE 18. Splenic lymphoma in a patient with Wegner granulomatosis. A, The most inferior slice of a chest CT demonstrates ahypoattenuating mass in the anterior margin of the spleen (white arrow). B, Diagnostic ultrasound confirms that this lesion canbe seen at sonography (graticules). C, Ultrasound-guided core biopsy makes the diagnosis (arrow points to the needle tip). Notehow a small footprint transducer was necessary for this intercostal biopsy.
FIGURE 19. Large B-cell lymphoma of the spleen. A, Splenic and perisplenic lesions are demonstrated (arrows). B, Five 18-gaugecores were obtained (arrow points to the needle tip), and the diagnosis was made.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 57
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
with possible benefits including decreased seeding,56 lessrisk of pancreatitis, and an overall safer procedure.55,57
However, EUS is a specialty procedure with limitedpenetration in private practice and does not allow for reason-able size core biopsies.
Other pancreatic masses besides adenocarcinoma (eg,various solid or cystic primaries and potential metastases to thepancreas) can easily be sampled. In addition, pancreatic glandbiopsy of transplants (Fig. 21) is often performed to assessfor rejection in those who have received a pancreas transplantfor diabetes. Postbiopsy pancreatitis in this setting is arare event; at our institution, there was only 1 significantcomplication of pancreatitis in 180 pancreas transplantbiopsies (oral communication with transplant surgeon JonOrdorico, August 07, 2007).
KidneyTissue sampling of the kidney has classically been
discouraged due to concerns over poor histological accuracyand the fear of tumor seeding. However, a series of recentarticles58Y63 discusses the growing utility of this technique ashistology techniques have improved; in addition, the risk ofseeding, although real, is very small.62,64 Given the rapidgrowth of percutaneous ablation techniques for smallRCCs,65,66 preprocedural lesion biopsies are becoming verycommon. Other indications for mass biopsy include possiblelymphoma (Fig. 22) and distinguishing an RCC from a renal
metastasis in the face of widespread tumor of another type(Fig. 23). Another common indication for ultrasound-guidedrenal biopsy is assessing for rejection in renal transplants;17,249 renal transplants were performed in the year 2005 inthe United States alone.67 Figure 24 provides an unusualexample of a focal mass biopsy in a renal transplant. Althoughmany people prefer core biopsy, there is some literature thatFNA seems to perform as well (or better) for most of thecommon lesions,62 but as with all cytology techniques,accuracy depends heavily on local expertise in this specializedarea. There is debate about whether coaxial technique is usefulin preventing tumor seeding; we feel that there are noconvincing data that the use of an introducer needle helpsdecrease seeding and therefore only use coaxial techniquewhen we feel its use is warranted for other reasons.
AdrenalAlthough the number of benign adrenal adenomas on
which biopsy was performed has decreased with theintroduction of dedicated adrenal CT and MRI for adrenalmass characterization,68 percutaneous imaging-guided biopsyis still requested for tissue confirmation when these studies areinconclusive, and it is important for clinical management.Metastases to the adrenal gland (most from primary lungcancer) are the most commonly identified adrenal mass atbiopsy. Although some consider biopsy of potential adrenalcortical carcinomas (ACCs) relatively contraindicated due to
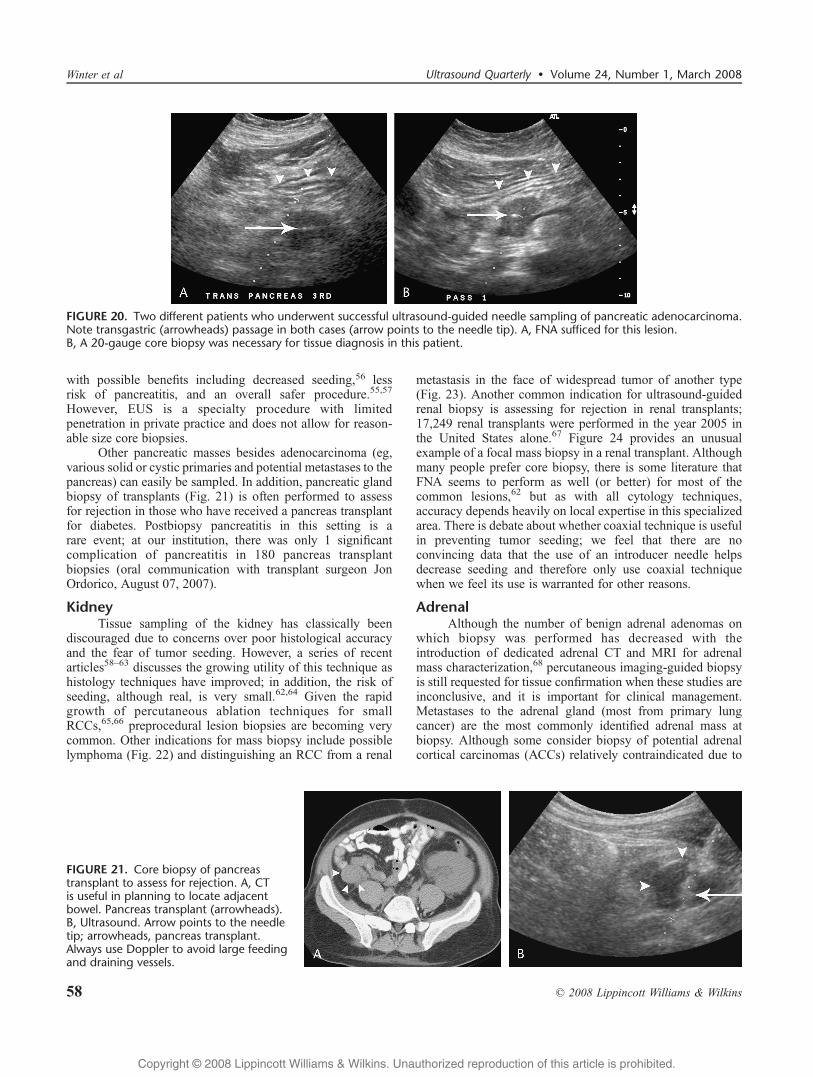
FIGURE 20. Two different patients who underwent successful ultrasound-guided needle sampling of pancreatic adenocarcinoma.Note transgastric (arrowheads) passage in both cases (arrow points to the needle tip). A, FNA sufficed for this lesion.B, A 20-gauge core biopsy was necessary for tissue diagnosis in this patient.
FIGURE 21. Core biopsy of pancreastransplant to assess for rejection. A, CTis useful in planning to locate adjacentbowel. Pancreas transplant (arrowheads).B, Ultrasound. Arrow points to the needletip; arrowheads, pancreas transplant.Always use Doppler to avoid large feedingand draining vessels.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
58 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

the risk of seeding and difficulties in pathological differentia-tion between ACC and degenerated adenomas,69 we willoccasionally perform this procedure in the correct clinicalsituation. Functioning tumors of the adrenal gland, such aspheochromocytomas, do not require biopsy; one should striveto avoid performing pheochromocytoma biopsy due to the riskof hemodynamic instability.
Some radiologists prefer CT guidance for adrenalbiopsies, particularly on the right side where a CT-guidedparaspinal approach obviates a transhepatic path, thus
avoiding the superficial and deep liver capsule. However, ifwe are able to visualize the mass sonographically, biopsy isoften performed under ultrasound guidance for the many otherreasons listed above. Right-sided lesions are typicallyapproached transhepatically (Fig. 25), whereas left-sidedlesions may be targeted through a left lower intercostal spacewith the patient in a right lateral decubitus position.Ultrasound-guided FNA of the adrenals has been shown tobe as safe and accurate as CT-guided FNA in patients withlung cancer.70
FIGURE 23. Melanoma metastasis. Lesion (arrow) notedon CT (A) could have been transitional cell carcinoma,but ultrasound-guided biopsy (B) in this patient with ahistory of melanoma confirmed the diagnosis. Arrowin B denotes needle tip.
FIGURE 24. Posttransplant lymphoproliferative disorder in a renal transplant. CT (A) performed to rule out appendicitis in thispatient status-post hepatic and renal transplants more than 5 years ago noted a new solid mass (arrow) in the kidney transplant(‘‘RTX’’), confirmed by ultrasound (B). Although tissue sampling could have been performed with a lower frequency curved lineartransducer, note how use of a high-frequency, 17-MHz straight linear probe makes this core biopsy trivially easy (C).
FIGURE 22. Oncocytic RCC (arrow). The patienthad a history of lymphoma, so the oncology servicedesired a biopsy of this renal mass. CT (A) andultrasound (B). Arrow in B denotes needle tip.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 59
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
BowelTwo issues pertain to biopsy and the bowel: is it safe to
pass through the gastrointestinal (GI) tract en route to a target,and when can biopsy be used for lesions intrinsic to the bowel?
The answer to the first question is yes.71 We routinelypass needles through the stomach (Fig. 20) and small bowel(Fig. 26) to reach the target lesion in certain situations. InBrandt’s 1993 study on percutaneous biopsy of the pancreas,there were 66 documented needle passes through the GI tract(41 gastric, 18 small bowel, and 7 colonic, all of the latter witha 21-gauge needle) without any related complications.72 Thestomach has a muscular thick wall that renders it relativelyforgiving to puncture; a rabbit study suggested that 18-gaugetransgastric Tru-Cut cores can be used without fear ofbleeding, leakage, or peritonitis.73 Fine-needle aspirationtraversal of the small bowel is generally considered safe inimmunocompetent patients.74 Passage through the colon is themost problematic area. Although several articles report noproblem with this approach,72,75 with one group stating Btherisk of peritonitis associated with colonic transgression withan 18- or 20-gauge core needle biopsy appears to besmallI,[71 we generally try to avoid this approach, especiallywith large-gauge needles.76 If a transcolonic approach isconsidered, a cleansing bowel prep may be prudent.
In a study on ultrasound-guided biopsy of small lymphnodes in the abdomen and pelvis, the authors state, BWe made
no particular attempt to avoid transgression of interveningsmall bowel or colon; in fact, with compression, it is usuallyimpossible to differentiate bowel from mesenteric or omentalfatty tissue.[14 None of their patients received antibiotics orhad complications related to bowel perforation, but they didsuggest that prophylactic antibiotics may be indicated in thosepatients in whom passage through the colon is anticipated. Asexpected, complications with transenteric passage have beenreported, including peritonitis34 and infection of an adjacentfluid collection.77
Although there is much contradictory and/or incompletedata on this topic, our approach can be roughly summarized asfollows: avoid bowel if easily possible; if bowel must betransgressed, use the smallest feasible needle diameter; FNAand large core (18-gauge) sampling through the stomach arevery safe; FNA and, if necessary, 20-gauge core samplingthrough small bowel are reasonable; avoid colon if at allpossible, and if necessary to pass through colon, try to staywith FNA.
Many reports demonstrate the utility of FNA forintrinsic lesions of the alimentary canal.78 Fine-needleaspiration is particularly useful in patients whose lesionscannot be reached by endoscopy, or who are poor candidatesfor endoscopy.79 Percutaneous core biopsy of bowel wallmasses is also safe71,80Y82 and allows a definitive diagnosis tobe made (Figs. 27 and 28)83 in difficult cases when other
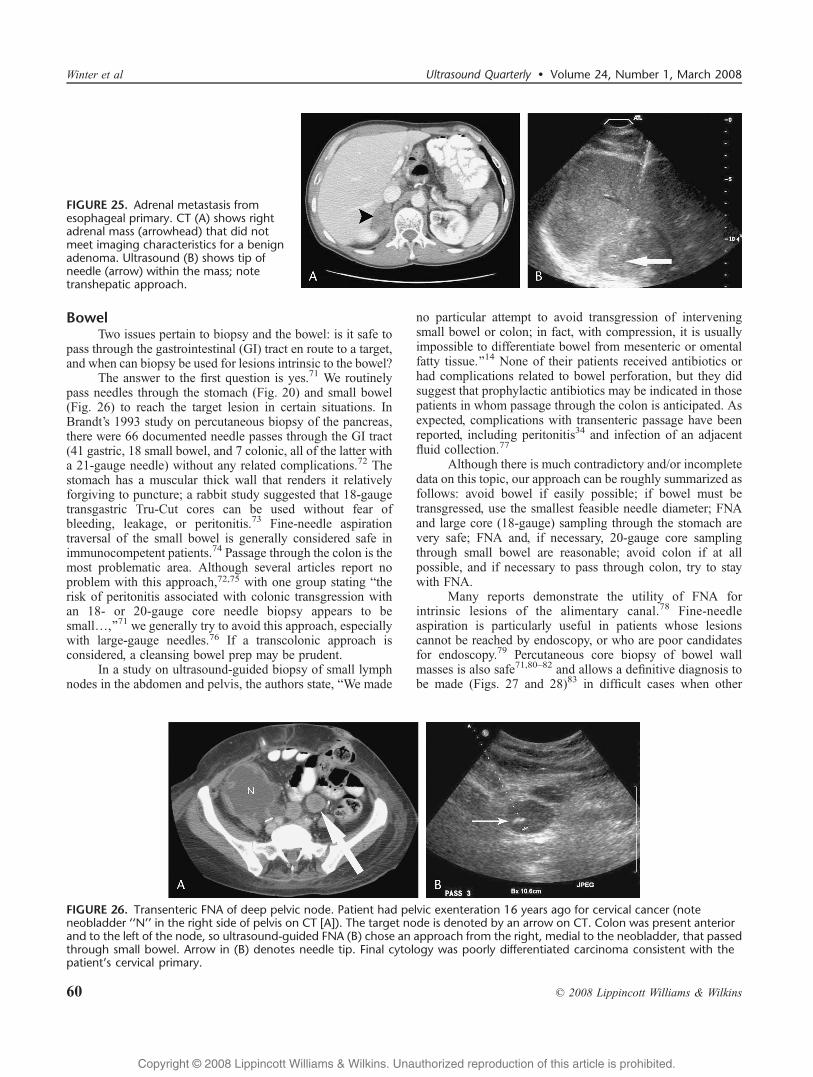
FIGURE 25. Adrenal metastasis fromesophageal primary. CT (A) shows rightadrenal mass (arrowhead) that did notmeet imaging characteristics for a benignadenoma. Ultrasound (B) shows tip ofneedle (arrow) within the mass; notetranshepatic approach.
FIGURE 26. Transenteric FNA of deep pelvic node. Patient had pelvic exenteration 16 years ago for cervical cancer (noteneobladder ‘‘N’’ in the right side of pelvis on CT [A]). The target node is denoted by an arrow on CT. Colon was present anteriorand to the left of the node, so ultrasound-guided FNA (B) chose an approach from the right, medial to the neobladder, that passedthrough small bowel. Arrow in (B) denotes needle tip. Final cytology was poorly differentiated carcinoma consistent with thepatient’s cervical primary.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
60 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
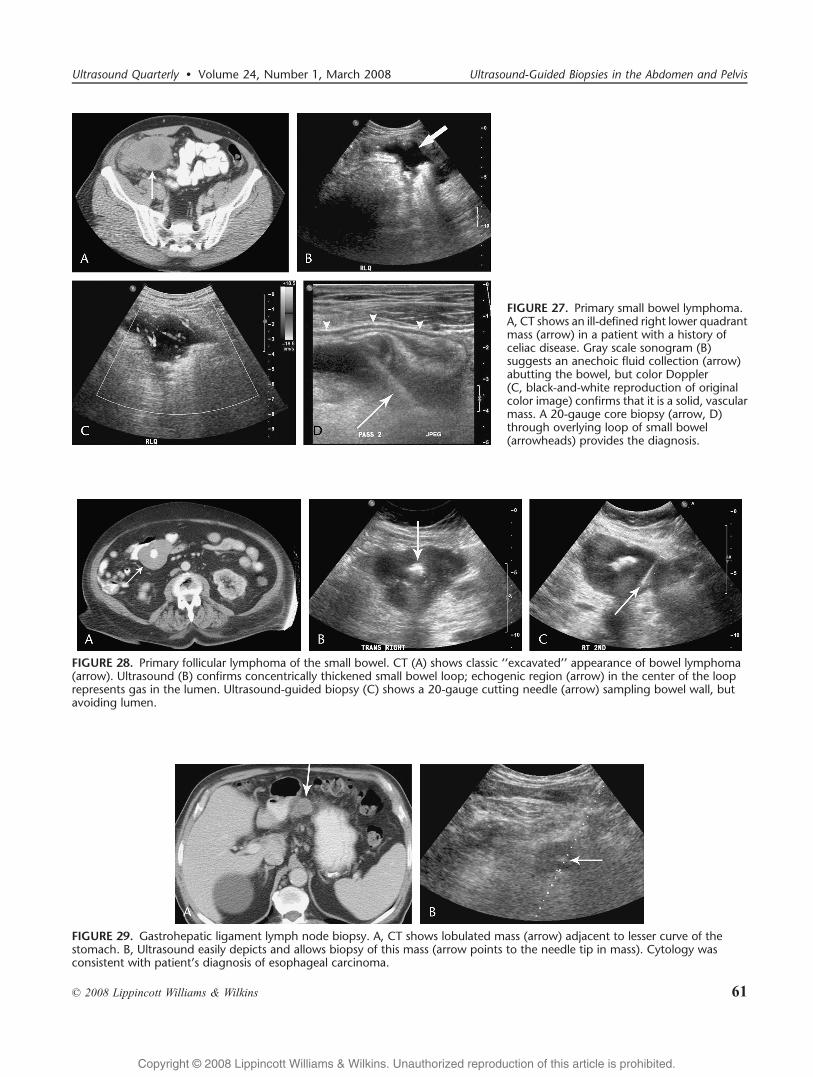
FIGURE 28. Primary follicular lymphoma of the small bowel. CT (A) shows classic ‘‘excavated’’ appearance of bowel lymphoma(arrow). Ultrasound (B) confirms concentrically thickened small bowel loop; echogenic region (arrow) in the center of the looprepresents gas in the lumen. Ultrasound-guided biopsy (C) shows a 20-gauge cutting needle (arrow) sampling bowel wall, butavoiding lumen.
FIGURE 29. Gastrohepatic ligament lymph node biopsy. A, CT shows lobulated mass (arrow) adjacent to lesser curve of thestomach. B, Ultrasound easily depicts and allows biopsy of this mass (arrow points to the needle tip in mass). Cytology wasconsistent with patient’s diagnosis of esophageal carcinoma.
FIGURE 27. Primary small bowel lymphoma.A, CT shows an ill-defined right lower quadrantmass (arrow) in a patient with a history ofceliac disease. Gray scale sonogram (B)suggests an anechoic fluid collection (arrow)abutting the bowel, but color Doppler(C, black-and-white reproduction of originalcolor image) confirms that it is a solid, vascularmass. A 20-gauge core biopsy (arrow, D)through overlying loop of small bowel(arrowheads) provides the diagnosis.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 61
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
approaches (eg, EUS) cannot or have not provided an adequatetissue sample. The series by Farmer et al84 successfully used18-gauge cutting needles in 12 patients with suspected tumorsof the GI tract. Although not driven by hard data, we postulatethat avoiding the bowel lumen, when possible, during bowelwall biopsy may reduce the risk of bowel perforation.
Peritoneal and RetroperitonealUltrasound should be the method of choice for tissue
sampling of most of these masses. In the past, manyradiologists assumed that nonsolid organ masses could onlybe seen and biopsied under CT; we now know that, particularlyif armed with a good-quality diagnostic CT or MRI ahead oftime, most mesenteric and retroperitoneal masses can be foundand sampled at sonography.85
In a study on performing biopsy on small lymph nodesof the abdomen, pelvis, and retroperitoneum, Fisher et al14
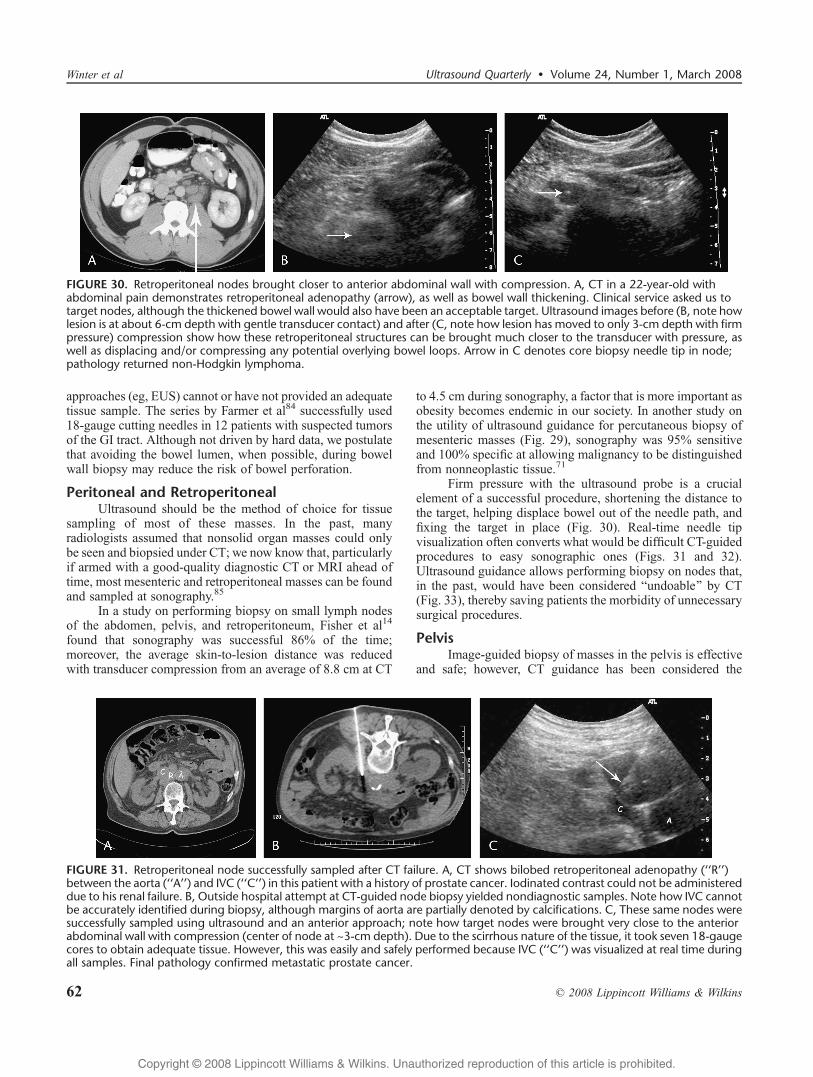
found that sonography was successful 86% of the time;moreover, the average skin-to-lesion distance was reducedwith transducer compression from an average of 8.8 cm at CT
to 4.5 cm during sonography, a factor that is more important asobesity becomes endemic in our society. In another study onthe utility of ultrasound guidance for percutaneous biopsy ofmesenteric masses (Fig. 29), sonography was 95% sensitiveand 100% specific at allowing malignancy to be distinguishedfrom nonneoplastic tissue.71
Firm pressure with the ultrasound probe is a crucialelement of a successful procedure, shortening the distance tothe target, helping displace bowel out of the needle path, andfixing the target in place (Fig. 30). Real-time needle tipvisualization often converts what would be difficult CT-guidedprocedures to easy sonographic ones (Figs. 31 and 32).Ultrasound guidance allows performing biopsy on nodes that,in the past, would have been considered Bundoable[ by CT(Fig. 33), thereby saving patients the morbidity of unnecessarysurgical procedures.
PelvisImage-guided biopsy of masses in the pelvis is effective
and safe; however, CT guidance has been considered the
FIGURE 30. Retroperitoneal nodes brought closer to anterior abdominal wall with compression. A, CT in a 22-year-old withabdominal pain demonstrates retroperitoneal adenopathy (arrow), as well as bowel wall thickening. Clinical service asked us totarget nodes, although the thickened bowel wall would also have been an acceptable target. Ultrasound images before (B, note howlesion is at about 6-cm depth with gentle transducer contact) and after (C, note how lesion has moved to only 3-cm depth with firmpressure) compression show how these retroperitoneal structures can be brought much closer to the transducer with pressure, aswell as displacing and/or compressing any potential overlying bowel loops. Arrow in C denotes core biopsy needle tip in node;pathology returned non-Hodgkin lymphoma.
FIGURE 31. Retroperitoneal node successfully sampled after CT failure. A, CT shows bilobed retroperitoneal adenopathy (‘‘R’’)between the aorta (‘‘A’’) and IVC (‘‘C’’) in this patient with a history of prostate cancer. Iodinated contrast could not be administereddue to his renal failure. B, Outside hospital attempt at CT-guided node biopsy yielded nondiagnostic samples. Note how IVC cannotbe accurately identified during biopsy, although margins of aorta are partially denoted by calcifications. C, These same nodes weresuccessfully sampled using ultrasound and an anterior approach; note how target nodes were brought very close to the anteriorabdominal wall with compression (center of node at ~3-cm depth). Due to the scirrhous nature of the tissue, it took seven 18-gaugecores to obtain adequate tissue. However, this was easily and safely performed because IVC (‘‘C’’) was visualized at real time duringall samples. Final pathology confirmed metastatic prostate cancer.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
62 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

method of choice in the past. Recent work has shown thattechnological improvements in sonography, as well as greaterconfidence and experience with ultrasound guidance, allow allof the previously described advantages (speed, lack ofradiation, cost, real-time visualization, etc) of sonographicimaging to be brought to bear on pelvic lesions. A 2007 studyby Yarram et al86 concluded that the accuracy and sensitivityof ultrasound-guided core biopsies of pelvic masses werehigher than those for CT-guided biopsies.
Percutaneous biopsy may be easily performed on largepelvic masses using the techniques already described (Fig. 34).Ultrasound guidance (using the biopsy guide on the endo-vaginal or endorectal probe) is particularly suited, however,for deep pelvic masses that are not safely amenable to per-cutaneous approaches, because transvaginal (Fig. 35) or endo-rectal access often allows easy tissue sampling. Although mostof the biopsies already discussed may be performed with justlocal anesthesia, passage of a needle through the muscular
FIGURE 34. Large omental metastasis. Thepatient had ‘‘low-grade’’ cervical cancer onPap smear. Subsequent MRI (A) revealed alarge mass (arrow) anterior to the uterus(‘‘U’’), with differential including leiomyoma.Simple percutaneous 18-gauge core pelvicbiopsy (B) was performed (arrow points tothe needle tip). Unfortunately, the finaldiagnosis was stage IVB squamous cellcarcinoma of the cervix.
FIGURE 33. ‘‘Impossible’’ retroperitoneal node successfully biopsied.A,CT in this patientwithpancreatic carcinoma (‘‘C’’) andCourvoisiergallbladder (‘‘GB’’) shows target node (arrow denoting both node and path needle will take) between aorta (‘‘A’’) and cava (‘‘IVC’’), andbehind superior mesenteric artery and superior mesenteric vein. B, Doppler ultrasound (oriented similarly to CT in A) shows path (dottedbiopsy guide line) FNA needle took to reach node (red arrow); unfortunately, cytology revealed node positive disease.
FIGURE 32. Retroperitoneal (interaortocaval) adenopathy successfully sampled from an anterior approach. A, CT shows nodal mass(arrow) between IVC (not well seen due to compression by mass) and aorta (‘‘A’’). B, (Black-and-white reproduction of original colorimage) Ultrasound confirms mass (arrow) compressing IVC posteriorly. C, Ultrasound shows 20-gauge FNA needle tip (arrow)within the mass. Cytology was consistent with the patient’s known cervical cancer.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 63
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
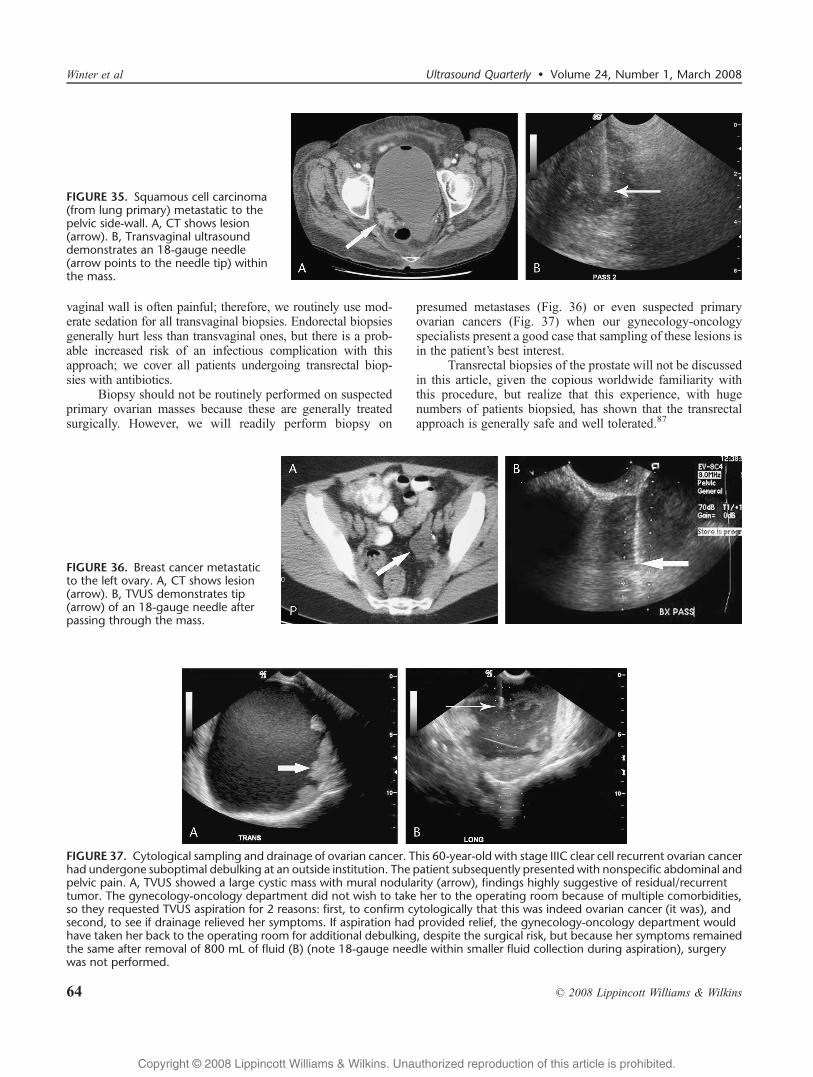
vaginal wall is often painful; therefore, we routinely use mod-erate sedation for all transvaginal biopsies. Endorectal biopsiesgenerally hurt less than transvaginal ones, but there is a prob-able increased risk of an infectious complication with thisapproach; we cover all patients undergoing transrectal biop-sies with antibiotics.
Biopsy should not be routinely performed on suspectedprimary ovarian masses because these are generally treatedsurgically. However, we will readily perform biopsy on
presumed metastases (Fig. 36) or even suspected primaryovarian cancers (Fig. 37) when our gynecology-oncologyspecialists present a good case that sampling of these lesions isin the patient’s best interest.
Transrectal biopsies of the prostate will not be discussedin this article, given the copious worldwide familiarity withthis procedure, but realize that this experience, with hugenumbers of patients biopsied, has shown that the transrectalapproach is generally safe and well tolerated.87
FIGURE 37. Cytological sampling and drainage of ovarian cancer. This 60-year-old with stage IIIC clear cell recurrent ovarian cancerhad undergone suboptimal debulking at an outside institution. The patient subsequently presented with nonspecific abdominal andpelvic pain. A, TVUS showed a large cystic mass with mural nodularity (arrow), findings highly suggestive of residual/recurrenttumor. The gynecology-oncology department did not wish to take her to the operating room because of multiple comorbidities,so they requested TVUS aspiration for 2 reasons: first, to confirm cytologically that this was indeed ovarian cancer (it was), andsecond, to see if drainage relieved her symptoms. If aspiration had provided relief, the gynecology-oncology department wouldhave taken her back to the operating room for additional debulking, despite the surgical risk, but because her symptoms remainedthe same after removal of 800 mL of fluid (B) (note 18-gauge needle within smaller fluid collection during aspiration), surgerywas not performed.
FIGURE 36. Breast cancer metastaticto the left ovary. A, CT shows lesion(arrow). B, TVUS demonstrates tip(arrow) of an 18-gauge needle afterpassing through the mass.
FIGURE 35. Squamous cell carcinoma(from lung primary) metastatic to thepelvic side-wall. A, CT shows lesion(arrow). B, Transvaginal ultrasounddemonstrates an 18-gauge needle(arrow points to the needle tip) withinthe mass.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
64 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
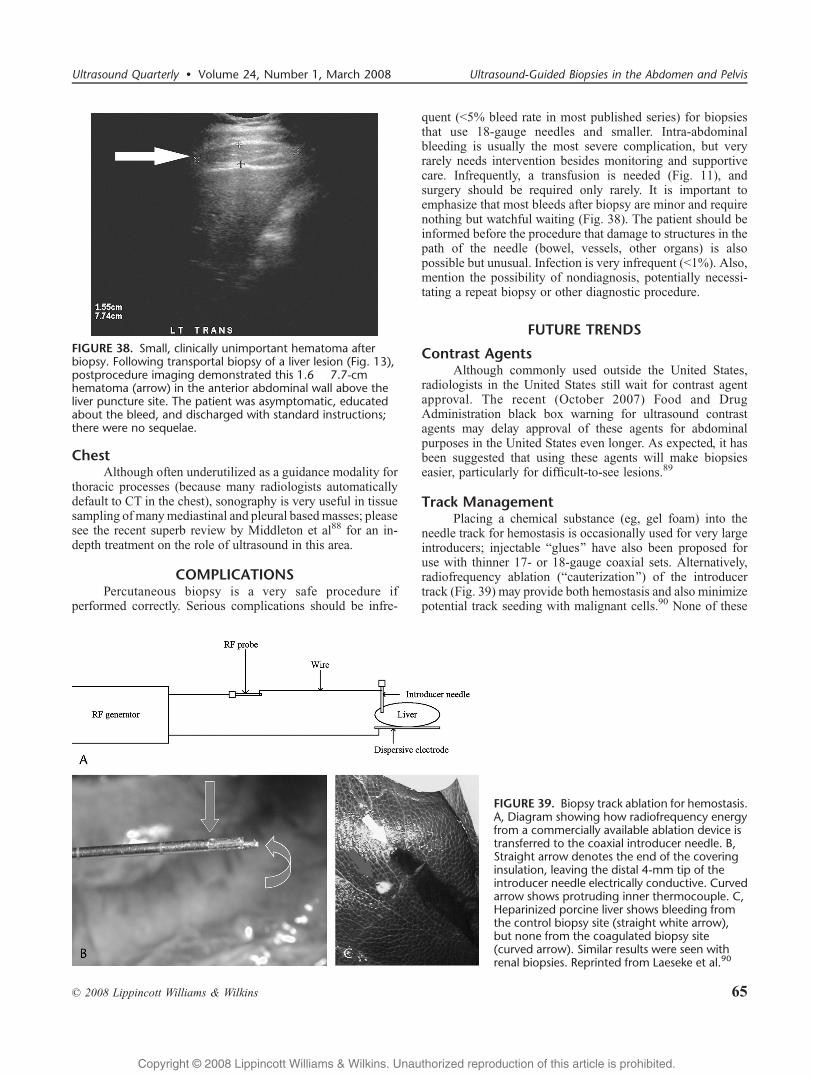
ChestAlthough often underutilized as a guidance modality for
thoracic processes (because many radiologists automaticallydefault to CT in the chest), sonography is very useful in tissuesampling ofmanymediastinal and pleural basedmasses; pleasesee the recent superb review by Middleton et al88 for an in-depth treatment on the role of ultrasound in this area.
COMPLICATIONSPercutaneous biopsy is a very safe procedure if
performed correctly. Serious complications should be infre-
quent (G5% bleed rate in most published series) for biopsiesthat use 18-gauge needles and smaller. Intra-abdominalbleeding is usually the most severe complication, but veryrarely needs intervention besides monitoring and supportivecare. Infrequently, a transfusion is needed (Fig. 11), andsurgery should be required only rarely. It is important toemphasize that most bleeds after biopsy are minor and requirenothing but watchful waiting (Fig. 38). The patient should beinformed before the procedure that damage to structures in thepath of the needle (bowel, vessels, other organs) is alsopossible but unusual. Infection is very infrequent (G1%). Also,mention the possibility of nondiagnosis, potentially necessi-tating a repeat biopsy or other diagnostic procedure.
FUTURE TRENDS
Contrast AgentsAlthough commonly used outside the United States,
radiologists in the United States still wait for contrast agentapproval. The recent (October 2007) Food and DrugAdministration black box warning for ultrasound contrastagents may delay approval of these agents for abdominalpurposes in the United States even longer. As expected, it hasbeen suggested that using these agents will make biopsieseasier, particularly for difficult-to-see lesions.89
Track ManagementPlacing a chemical substance (eg, gel foam) into the
needle track for hemostasis is occasionally used for very largeintroducers; injectable Bglues[ have also been proposed foruse with thinner 17- or 18-gauge coaxial sets. Alternatively,radiofrequency ablation (Bcauterization[) of the introducertrack (Fig. 39) may provide both hemostasis and also minimizepotential track seeding with malignant cells.90 None of these
FIGURE 39. Biopsy track ablation for hemostasis.A, Diagram showing how radiofrequency energyfrom a commercially available ablation device istransferred to the coaxial introducer needle. B,Straight arrow denotes the end of the coveringinsulation, leaving the distal 4-mm tip of theintroducer needle electrically conductive. Curvedarrow shows protruding inner thermocouple. C,Heparinized porcine liver shows bleeding fromthe control biopsy site (straight white arrow),but none from the coagulated biopsy site(curved arrow). Similar results were seen withrenal biopsies. Reprinted from Laeseke et al.90
FIGURE 38. Small, clinically unimportant hematoma afterbiopsy. Following transportal biopsy of a liver lesion (Fig. 13),postprocedure imaging demonstrated this 1.6 � 7.7-cmhematoma (arrow) in the anterior abdominal wall above theliver puncture site. The patient was asymptomatic, educatedabout the bleed, and discharged with standard instructions;there were no sequelae.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 65
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.
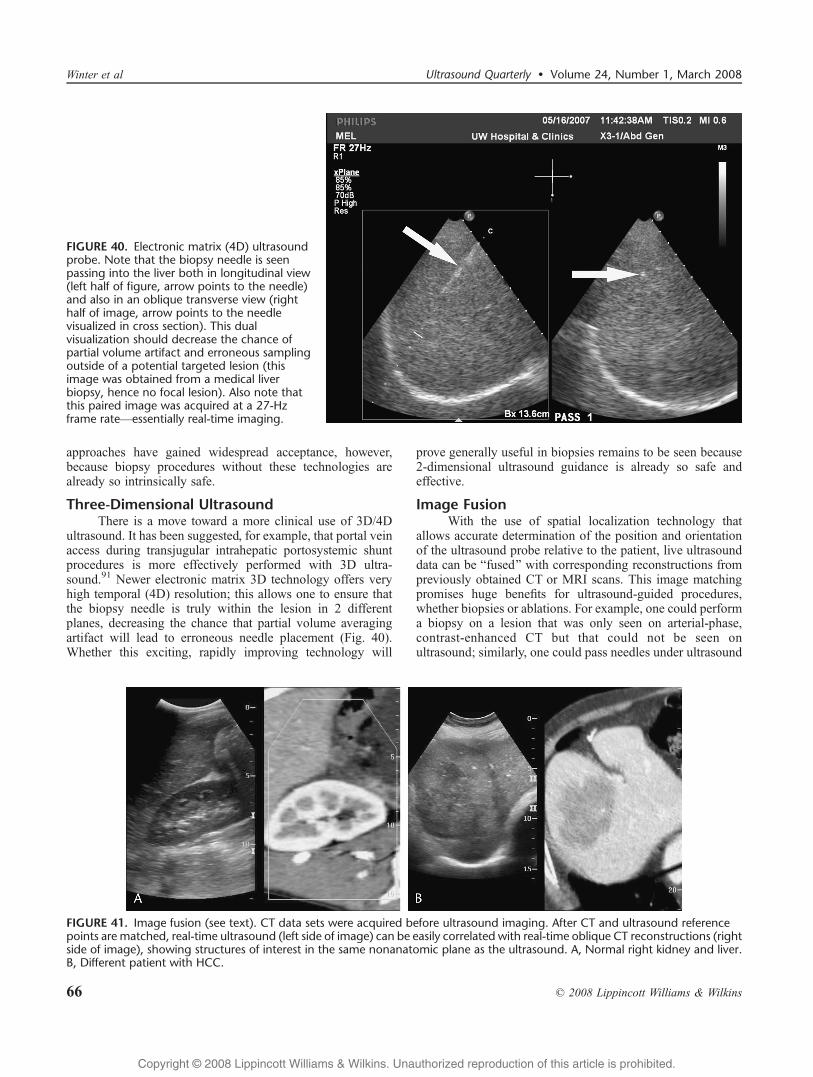
approaches have gained widespread acceptance, however,because biopsy procedures without these technologies arealready so intrinsically safe.
Three-Dimensional UltrasoundThere is a move toward a more clinical use of 3D/4D
ultrasound. It has been suggested, for example, that portal veinaccess during transjugular intrahepatic portosystemic shuntprocedures is more effectively performed with 3D ultra-sound.91 Newer electronic matrix 3D technology offers veryhigh temporal (4D) resolution; this allows one to ensure thatthe biopsy needle is truly within the lesion in 2 differentplanes, decreasing the chance that partial volume averagingartifact will lead to erroneous needle placement (Fig. 40).Whether this exciting, rapidly improving technology will
prove generally useful in biopsies remains to be seen because2-dimensional ultrasound guidance is already so safe andeffective.
Image FusionWith the use of spatial localization technology that
allows accurate determination of the position and orientationof the ultrasound probe relative to the patient, live ultrasounddata can be Bfused[ with corresponding reconstructions frompreviously obtained CT or MRI scans. This image matchingpromises huge benefits for ultrasound-guided procedures,whether biopsies or ablations. For example, one could performa biopsy on a lesion that was only seen on arterial-phase,contrast-enhanced CT but that could not be seen onultrasound; similarly, one could pass needles under ultrasound
FIGURE 41. Image fusion (see text). CT data sets were acquired before ultrasound imaging. After CT and ultrasound referencepoints are matched, real-time ultrasound (left side of image) can be easily correlated with real-time oblique CT reconstructions (rightside of image), showing structures of interest in the same nonanatomic plane as the ultrasound. A, Normal right kidney and liver.B, Different patient with HCC.
FIGURE 40. Electronic matrix (4D) ultrasoundprobe. Note that the biopsy needle is seenpassing into the liver both in longitudinal view(left half of figure, arrow points to the needle)and also in an oblique transverse view (righthalf of image, arrow points to the needlevisualized in cross section). This dualvisualization should decrease the chance ofpartial volume artifact and erroneous samplingoutside of a potential targeted lesion (thisimage was obtained from a medical liverbiopsy, hence no focal lesion). Also note thatthis paired image was acquired at a 27-Hzframe rateVessentially real-time imaging.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
66 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

guidance with confident knowledge of structures that are to beavoided (like bowel) that may be difficult to see at sonography(Fig. 41).
SUMMARYWe have reviewed many aspects regarding the use of
sonography to guide biopsies in the abdomen and pelvis.Simply put, ultrasound is generally cheaper, faster, safer, andmore effective than CT in most instances in this anatomicalregion. Keep ultrasound in mind for all biopsies, includingthose Bimpossible[ retroperitoneal nodes on CT. Our motto is:BIf you can see it by ultrasound, you can hit it![
REFERENCES1. Goldberg BB, Pollack HM. Ultrasonic aspiration transducer. Radiology.
1972;102:187Y189.2. Hopper KD. Percutaneous, radiographically guided biopsy: a history.
Radiology. 1995;196:329Y333.3. Alfidi RJ, Haaga J, Meaney TF, et al. Computed tomography of the thorax
and abdomen; a preliminary report. Radiology. 1975;117:257Y264.4. Dodd GD 3rd, Esola CC, Memel DS, et al. Sonography: the
undiscovered jewel of interventional radiology. Radiographics. 1996;16:1271Y1288.
5. Shem S. The House of God: The Classic Novel of Life and Death in anAmerican Hospital Dell. New York, NY: Dell Publishing; 2003:416.
6. Stigliano R, Burroughs AK. Should we biopsy each liver mass suspiciousfor HCC before liver transplantation?VNo, please don’t. J Hepatol.2005;43:563Y568.
7. Daly B, Templeton PA. Real-time CT fluoroscopy: evolution of aninterventional tool. Radiology. 1999;211:309Y315.
8. Paulson EK, Sheafor DH, Enterline DS, et al. CT fluoroscopyYguidedinterventional procedures: techniques and radiation dose to radiologists.Radiology. 2001;220:161Y167.
9. Silverman SG, Tuncali K, Adams DF, et al. CT fluoroscopy-guidedabdominal interventions: techniques, results, and radiation exposure.Radiology. 1999;212:673Y681.
10. Kliewer MA, Sheafor DH, Paulson EK, et al. Percutaneous liver biopsy: acost-benefit analysis comparing sonographic and CT guidance. AJR Am JRoentgenol. 1999;173:1199Y1202.
11. Sheafor DH, Paulson EK, Simmons CM, et al. Abdominal percutaneousinterventional procedures: comparison of CT and US guidance.Radiology. 1998;207:705Y710.
12. Sheafor DH, Paulson EK, Kliewer MA, et al. Comparison of sonographicand CT guidance techniques: does CT fluoroscopy decrease proceduretime? AJR Am J Roentgenol. 2000;174:939Y942.
13. Uppot RN, Sahani DV, Hahn PF, et al. Impact of obesity on medicalimaging and image-guided intervention. AJR Am J Roentgenol. 2007;188:433Y440.
14. Fisher AJ, Paulson EK, Sheafor DH, et al. Small lymph nodes of theabdomen, pelvis, and retroperitoneum: usefulness of sonographicallyguided biopsy. Radiology. 1997;205:185Y190.
15. CNNMoney.com. BMark Hurd takes his first swing at HP[. Available athttp://money.cnn.com/magazines/fortune/fortune_archive/2005/08/08/8267666/index.htm. Accessed February 12, 2008.
16. Auble TE, Taylor DM, Hsu EB, et al. Evaluation of guidelines forordering prothrombin and partial thromboplastin times. Acad Emerg Med.2002;9:567Y574.
17. Ewe K. Bleeding after liver biopsy does not correlate with indices ofperipheral coagulation. Dig Dis Sci. 1981;26:388Y393.
18. Eckman MH, Erban JK, Singh SK, et al. Screening for the risk forbleeding or thrombosis. Ann Intern Med. 2003;138:W15YW24.
19. Erban SB, Kinman JL, Schwartz JS. Routine use of the prothrombin andpartial thromboplastin times. JAMA. 1989;262:2428Y2432.
20. Holland LL, Brooks JP. Toward rational fresh frozen plasma transfusion:the effect of plasma transfusion on coagulation test results. Am J ClinPathol. 2006;126:133Y139.
21. O’Donnell MJ, Kearon C, Johnson J, et al. Brief communication:preoperative anticoagulant activity after bridging low-molecular-weight
heparin for temporary interruption of warfarin. Ann Intern Med. 2007;146:184Y187.
22. Zuckerman MJ, Hirota WK, Adler DG, et al. ASGE guideline: themanagement of low-molecular-weight heparin and nonaspirin antiplateletagents for endoscopic procedures. Gastrointest Endosc. 2005;61:189Y194.
23. Friedland S, Soetikno R. Colonoscopy with polypectomy inanticoagulated patients. Gastrointest Endosc. 2006;64:98Y100.
24. Rex D. Managing anticoagulated patients who are referred for endoscopy.J Watch Gastroenterol. 2005.
25. Grant A, Neuberger J. Guidelines on the use of liver biopsy in clinicalpractice. British Society of Gastroenterology. Gut. 1999;45(suppl 4):IV1YIV11.
26. Sadeghi-Nejad H, Simmons M, Dakwar G, et al. Controversies intransrectal ultrasonography and prostate biopsy. Ultrasound Q. 2006;22:169Y175.
27. Smith R, Atwell T, Callstrom M, et al. Incidence of significant bleedingcomplications following image-guided biopsy in patients taking aspirin.Radiology. 2005;SSE03YSSE04.
28. Partners Against Pain. In 2007. JCAHO Standards. Available at:http://www.partnersagainstpain.com/index-hs.aspx?sid=22.Accessed February 12, 2008.
29. Lang EV, Hatsiopoulou O, Koch T, et al. Can words hurt? Patient-providerinteractions during invasive procedures. Pain. 2005;114:303Y309.
30. Xia Y, Chen E, Tibbits DL, et al. Comparison of effects of lidocainehydrochloride, buffered lidocaine, diphenhydramine, and normal salineafter intradermal injection. J Clin Anesth. 2002;14:339Y343.
31. Phal PM, Brooks DM, Wolfe R. Sonographically guided biopsy of focallesions: a comparison of freehand and probe-guided techniques using aphantom. AJR Am J Roentgenol. 2005;184:1652Y1656.
32. Bergin D, Pappas JN, Hwang JJ, et al. Echogenic polymer coating: doesit improve needle visualization in sonographically guided biopsy?AJR Am J Roentgenol. 2002;178:1188Y1190.
33. Tublin ME, Martin JA, Rollin LJ, et al. Ultrasound-guided fine-needleaspiration versus fine-needle capillary sampling biopsy of thyroidnodules: does technique matter? J Ultrasound Med. 2007;26:1697Y1701.
34. Berger H, Permanetter W, Steiner W, et al. Fine-needle and incisionalbiopsy technics in the percutaneous puncture of abdominalspace-occupying lesions [in German]. Radiologe. 1988;28:265Y268.
35. Sheiman RG, Fey C, McNicholas M, et al. Possible causes of inconclusiveresults on CT-guided thoracic and abdominal core biopsies. AJR Am JRoentgenol. 1998;170:1603Y1607.
36. Maturen KE, Nghiem HV, Marrero JA, et al. Lack of tumor seeding ofhepatocellular carcinoma after percutaneous needle biopsy using coaxialcutting needle technique. AJR Am J Roentgenol. 2006;187:1184Y1187.
37. Little AF, Ferris JV, Dodd GD 3rd, et al. Image-guided percutaneoushepatic biopsy: effect of ascites on the complication rate. Radiology.1996;199:79Y83.
38. Murphy FB, Barefield KP, Steinberg HV, et al. CT- or sonography-guidedbiopsy of the liver in the presence of ascites: frequency of complications.AJR Am J Roentgenol. 1988;151:485Y486.
39. Kim KW, KimMJ, Kim HC, et al. Value of Bpatent track[ sign on Dopplersonography after percutaneous liver biopsy in detection of postbiopsybleeding: a prospective study in 352 patients. AJR Am J Roentgenol.2007;189:109Y116.
40. Quinn SF, vanSonnenberg E, Casola G, et al. Interventional radiology inthe spleen. Radiology. 1986;161:289Y291.
41. Dodd GD 3rd, Carr BI. Percutaneous biopsy of portal vein thrombus: anew staging technique for hepatocellular carcinoma. AJR Am JRoentgenol. 1993;161:229Y233.
42. Leifer DM, Middleton WD, Teefey SA, et al. Follow-up of patients at lowrisk for hepatic malignancy with a characteristic hemangioma at US.Radiology. 2000;214:167Y172.
43. Karhunen PJ. Benign hepatic tumours and tumour like conditions in men.J Clin Pathol. 1986;39:183Y188.
44. Bruix J, Sherman M, Llovet JM, et al. Clinical management ofhepatocellular carcinoma. Conclusions of the Barcelona-2000 EASLconference. European Association for the Study of the Liver. J Hepatol.2001;35:421Y430.
45. Keogan MT, Freed KS, Paulson EK, et al. Imaging-guided percutaneousbiopsy of focal splenic lesions: update on safety and effectiveness. AJRAm J Roentgenol. 1999;172:933Y937.
Ultrasound Quarterly & Volume 24, Number 1, March 2008 Ultrasound-Guided Biopsies in the Abdomen and Pelvis
* 2008 Lippincott Williams & Wilkins 67
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.

46. Soderstrom N. How to use cytodiagnostic spleen puncture. Acta MedScand. 1976;199:1Y5.
47. O’Malley ME, Wood BJ, Boland GW, et al. Percutaneous imaging-guidedbiopsy of the spleen. AJR Am J Roentgenol. 1999;172:661Y665.
48. Lopez JI, Del Cura JL, De Larrinoa AF, et al. Role of ultrasound-guidedcore biopsy in the evaluation of spleen pathology. APMIS. 2006;114:492Y499.
49. Civardi G, Vallisa D, Berte R, et al. Ultrasound-guided fine needle biopsyof the spleen: high clinical efficacy and low risk in a multicenter Italianstudy. Am J Hematol. 2001;67:93Y99.
50. Muraca S, Chait PG, Connolly BL, et al. US-guided core biopsy of thespleen in children. Radiology. 2001;218:200Y206.
51. Liang P, Gao Y, Wang Y, et al. US-guided percutaneous needle biopsy ofthe spleen using 18-gauge versus 21-gauge needles. J Clin Ultrasound.2007;35(9):477Y482.
52. Di Stasi M, Lencioni R, Solmi L, et al. Ultrasound-guided fine needlebiopsy of pancreatic masses: results of a multicenter study. Am JGastroenterol. 1998;93:1329Y1333.
53. Paulsen SD, Nghiem HV, Negussie E, et al. Evaluation of imaging-guidedcore biopsy of pancreatic masses. AJR Am J Roentgenol. 2006;187:769Y772.
54. Mueller PR, Miketic LM, Simeone JF, et al. Severe acute pancreatitis afterpercutaneous biopsy of the pancreas. AJR Am J Roentgenol. 1988;151:493Y494.
55. Goldin SB, Bradner MW, Zervos EE, et al. Assessment of pancreaticneoplasms: review of biopsy techniques. J Gastrointest Surg. 2007;11:783Y790.
56. Micames C, Jowell PS, White R, et al. Lower frequency of peritonealcarcinomatosis in patients with pancreatic cancer diagnosed byEUS-guided FNA vs. percutaneous FNA. Gastrointest Endosc. 2003;58:690Y695.
57. Eloubeidi MA, Varadarajulu S, Desai S, et al. A prospective evaluationof an algorithm incorporating routine preoperative endoscopicultrasound-guided fine needle aspiration in suspected pancreatic cancer.J Gastrointest Surg. 2007;11:813Y819.
58. Caoili EM, Bude RO, Higgins EJ, et al. Evaluation of sonographicallyguided percutaneous core biopsy of renal masses. AJR Am J Roentgenol.2002;179:373Y378.
59. Rybicki FJ, Shu KM, Cibas ES, et al. Percutaneous biopsy of renalmasses: sensitivity and negative predictive value stratified by clinicalsetting and size of masses. AJR Am J Roentgenol. 2003;180:1281Y1287.
60. Silverman SG, Gan YU, Mortele KJ, et al. Renal masses in the adultpatient: the role of percutaneous biopsy. Radiology. 2006;240:6Y22.
61. Beland MD, Mayo-Smith WW, Dupuy DE, et al. Diagnostic yield of 58consecutive imaging-guided biopsies of solid renal masses: should webiopsy all that are indeterminate? AJR Am J Roentgenol. 2007;188:792Y797.
62. Heilbrun ME, Zagoria RJ, Garvin AJ, et al. CT-guided biopsy for thediagnosis of renal tumors before treatment with percutaneous ablation.AJR Am J Roentgenol. 2007;188:1500Y1505.
63. Maturen KE, Nghiem HV, Caoili EM, et al. Renal mass core biopsy:accuracy and impact on clinical management. AJR Am J Roentgenol.2007;188:563Y570.
64. Wolf JS Jr. Evaluation and management of solid and cystic renal masses.J Urol. 1998;159:1120Y1133.
65. Atwell TD, Farrell MA, CallstromMR, et al. Percutaneous cryoablation of40 solid renal tumors with US guidance and CT monitoring: initialexperience. Radiology. 2007;243:276Y283.
66. Zagoria RJ, Traver MA,Werle DM, et al. Oncologic efficacy of CT-guidedpercutaneous radiofrequency ablation of renal cell carcinomas. AJR Am JRoentgenol. 2007;189:429Y436.
67. US Renal Data System. USRDS 2007 Annual Data Report: Atlas ofChronic Kidney Disease and End-stage Renal Disease in the UnitedStates. Bethesda, MD: National Institutes of Health, National Institute ofDiabetes and Digestive and Kidney Diseases; 2007.
68. Paulsen SD, Nghiem HV, Korobkin M, et al. Changing role ofimaging-guided percutaneous biopsy of adrenal masses: evaluation of50 adrenal biopsies. AJR Am J Roentgenol. 2004;182:1033Y1037.
69. Korobkin M, Francis IR, Kloos RT, et al. The incidental adrenal mass.Radiol Clin North Am. 1996;34:1037Y1054.
70. Kocijancic K, Kocijancic I, Guna F. Role of sonographically guidedfine-needle aspiration biopsy of adrenal masses in patients with lungcancer. J Clin Ultrasound. 2004;32:12Y16.
71. Ho LM, Thomas J, Fine SA, et al. Usefulness of sonographic guidanceduring percutaneous biopsy of mesenteric masses. AJR Am J Roentgenol.2003;180:1563Y1566.
72. Brandt KR, Charboneau JW, Stephens DH, et al. CT- and US-guidedbiopsy of the pancreas. Radiology. 1993;187:99Y104.
73. Akan H, Ozen N, Incesu L, et al. Are percutaneous transgastric biopsiesusing 14-, 16- and 18-G Tru-Cut needles safe? An experimental study inthe rabbit. Australas Radiol. 1998;42:99Y101.
74. Gupta S, Nguyen HL, Morello FA Jr, et al. Various approaches forCT-guided percutaneous biopsy of deep pelvic lesions: anatomic andtechnical considerations. Radiographics. 2004;24:175Y189.
75. Gianfelice D, Lepanto L, Perreault P, et al. Value of CT fluoroscopyfor percutaneous biopsy procedures. J Vasc Interv Radiol. 2000;11:879Y884.
76. Mueller PR. Pancreatic biopsy: striving for excellence. Radiology.1993;187:15Y16.
77. Martino CR, Haaga JR, Bryan PJ. Secondary infection of anendometrioma following fine-needle aspiration. Radiology. 1984;151:53Y54.
78. Heriot AG, Kumar D, Thomas V, et al. Ultrasonographically-guidedfine-needle aspiration cytology in the diagnosis of colonic lesions. Br JSurg. 1998;85:1713Y1715.
79. Carson BW, Brown JA, Cooperberg PL. Ultrasonographically guidedpercutaneous biopsy of gastric, small bowel, and colonic abnormalities:efficacy and safety. J Ultrasound Med. 1998;17:739Y742.
80. Kim SH, Han JK, Lee KH, et al. Experimentally induced small-boweltumor in rabbits: US-guided percutaneous 18-gauge core biopsy.Radiology. 2004;231:150Y155.
81. Tudor GR, Rodgers PM, West KP. Bowel lesions: percutaneousUS-guided 18-gauge needle biopsyVpreliminary experience. Radiology.1999;212:594Y597.
82. Marco-Domenech SF, Gil-Sanchez S, Fernandez-Garcia P, et al.Sonographically guided percutaneous biopsy of gastrointestinal tractlesions. AJR Am J Roentgenol. 2001;176:147Y151.
83. Ghai S, Pattison J, Ghai S, et al. Primary gastrointestinal lymphoma:spectrum of imaging findings with pathologic correlation. Radiographics.2007;27:1371Y1388.
84. Farmer KD, Harries SR, Fox BM, et al. Core biopsy of the bowel wall:efficacy and safety in the clinical setting. AJR Am J Roentgenol. 2000;175:1627Y1630.
85. Gottlieb RH, Tan R, Widjaja J, et al. Extravisceral masses in the peritonealcavity: sonographically guided biopsies in 52 patients. AJR Am JRoentgenol. 1998;171:697Y701.
86. Yarram SG, Nghiem HV, Higgins E, et al. Evaluation of imaging-guidedcore biopsy of pelvic masses. AJR Am J Roentgenol. 2007;188:1208Y1211.
87. Rifkin M. Biopsy Techniques in BUltrasound of the Prostate[. 2nd ed.Philadelphia, PA: Lippincott-Raven; 1997:237Y262.
88. Middleton WD, Teefey SA, Dahiya N. Ultrasound-guided chest biopsies.Ultrasound Q. 2006;22:241Y252.
89. Meuwly JY, Schnyder P, Gudinchet F, et al. Pulse-inversion harmonicimaging improves lesion conspicuity during US-guided biopsy. J VascInterv Radiol. 2003;14:335Y341.
90. Laeseke PF, Winter TC 3rd, Davis CL, et al. Postbiopsy bleeding in aporcine model: reduction with radio-frequency ablationVpreliminaryresults. Radiology. 2003;227:493Y499.
91. Rose SC, Pretorius DH, et al. Adjunctive 3D US for achieving portal veinaccess during transjugular intrahepatic portosystemic shunt procedures.J Vasc Interv Radiol. 2000;11:611Y621.
Winter et al Ultrasound Quarterly & Volume 24, Number 1, March 2008
68 * 2008 Lippincott Williams & Wilkins
Copyright @ 2008 Lippincott Williams & Wilkins. Unauthorized reproduction of this article is prohibited.