HEARING LOSS AND TINNITUS Charles Stewart. HEARING LOSS Hearing loss to many is an insignificant...
41
HEARING LOSS AND TINNITUS Charles Stewart
-
Upload
cori-gilmore -
Category
Documents
-
view
214 -
download
0
Transcript of HEARING LOSS AND TINNITUS Charles Stewart. HEARING LOSS Hearing loss to many is an insignificant...
HEARING LOSSAND
TINNITUS
Charles Stewart

HEARING LOSS
Hearing loss to many is an insignificant disability
Why is this?
It is invisible
usually painless
It is a hurt that does not show
To the profoundly deaf, they live in a world of silence, the emotional pain is devastating
HEARING LOSS
Hearing loss is important!
1 in 10 in the U.S. have some H.L.
1 in 100 has extreme difficulty with understanding speech
The cost to society is in the billions per year

WE NEED TO BE MORE AWARE, MORE SYMPOTHETIC, MORE
HELPFUL TO THOSE WITH HEARING LOSS

HEARING LOSS
Types of hearing loss:
Conductive hearing loss
Sensorineural hearing loss
Sensory (cochlea)
Neural (8th nerve)
Mixed hearing loss
Functional hearing loss: non-organic

HEARING LOSSAcoustics
Intensity of sound: loudness, measured in dB
Frequency of sound: Pitch, measured in Hz or cps
Pure tone: single frequency sound, as audiogram, rare in nature
Complex sound: more than one frequency; noise is a complex sound

HEARING LOSSAcoustics
Decibel scale (db): logarithmic scale, to measure intensity of sound; dB=log of a ratio of two sounds: reference sound & sound being described
Stimulus levels are stated with reference levels:
SPL: sound pressure level; .0002 dynes/cm2
HL: Hearing level; 0 dB HL on audiometer
SL: Sensation level
Hearing range: 10-20,000 cps; Intensity range 0-120

HEARING IMPAIRED: anyone with hearing loss
DEAF: anyone with profound SNHL
Categorizing hearing loss:
normal: 0-25 dB
mild H.L.: 26-45 dB
Mod.H.L.: 46-70 dB
Severe H.L.: 71-90 dB
Profound H.L.: >90 dB

PURE TONE AUDIOMETRY
Air conduction: actual hearing level: outer, middle, inner ear
Bone conduction: Potential hearing level, inner ear function
Conductive hearing loss: Difference between air & bone conduction threshold, the ABG
AUDIOGRAM
Screening audiogram should include:
l. Pure-tone evaluation: bone/ air threshold
2. Speech receptive threshold: (SRT)
3. Speech discrimination score (SDS)
THE MAJOR CAUSE OF SENSORINEURAL HEARING LOSS IS
NOISE EXPOSURE
The cause of the hearing loss is :
l. Acoustic trauma: single high intensity sound, causing a conductive &/or SNHL
2. Noise induced hearing loss: gradual loss from prolonged or repetitious noise exposure

EFFECTS OF NOISE EXPOSURE
Hair cell swelling (temporary threshold shift)
Hair cell destruction (permanent threshold shift)

CONTROL OF NOISE EXPOSURE
Environmental control:
reduce noise
Personal protection:
ear protection (ear plugs)
job rotation
job reassignment
test hearing periodically (annually)
TYPES OF HEARING LOSS THAT RAISE AN INDEX OF SUSPICION
Sudden hearing loss in healthy individuals
Gradual hearing loss
Fluctuating hearing loss
Pronounced buzzing or roaring tinnitus

What suggestive clues or symptoms does a person undergoing noise
induced hearing loss have?
Difficulty communicating at work
Head noise at work
Temporary loss of hearing

WHAT IS NEW FOR THE TREATMENT OF HEARING LOSS?
BAHA
COCHLEAR IMPLANTS
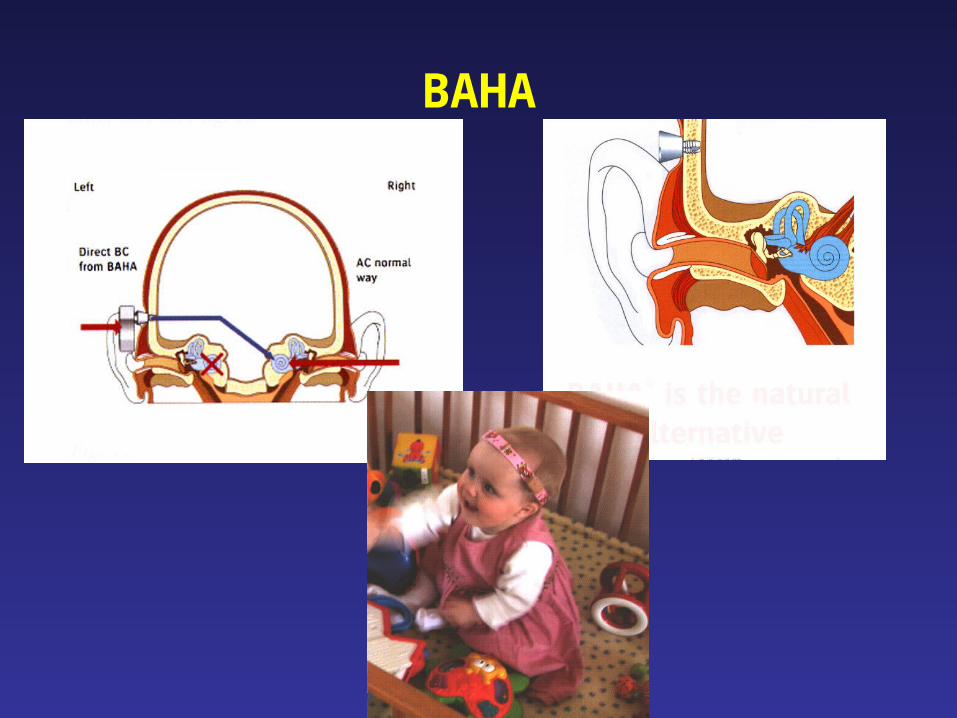
BAHA

COCHLEAR IMPLANTS

COCHLEAR IMPLANTS

COCHLEAR IMPLANTS
TINNITUS
Definition: perception of noise in the absence of acoustic stimulus
phantom auditory perception
Incidence: 40 million Americans have it
75% are not bothered by it
25% it interferes with their daily life
TINNITUSDIFFERENTIAL DIAGNOSIS
Two types:
1. Objective tinnitus -others hear it too
2. Subjective tinnitus -patient only hears it

OBJECTIVE TINNITUS
l. Patulous eustachian tube:
2.Muscular:
1. Stapedius spasm: myoclonus of the stapedius causes contractions of the TM seen with impedance bridge or otoscope
2. Palatal myoclonus: myoclonus of the palate
3. TMJ: 28% of those with TMJ syndrome have tinnitus

TINNITUSOBJECTIVE
3.Vascular AV shunts: Glomus tympanicum/jugulare tumour
Pulsating tinnitus, hearing loss
Bluish mass behind ear drum
Arteriovenous malformation: Dxn. with MRI, MRA, Angiogram; Tmt. Embolization
Arterial bruits:
Aberrant carotid artery
Persistent stapedial arteryVenous hum:
HBP; Hyper/hypothyroidism; high jugular bulb
TINNITUSTESTS
Audiogram, tympanogram: ENG & posturography not usually necessary
Lumbar puncture: after CT, those with papillodema
BAER, ECOG:
MRI, MRA, CT
Blood tests: ANA,B12,FTA,ESR,SMA-24 Glucose,TSH,antimicrosomal antibodies
TINNITUSTREATMENT
Tinnitus may be eliminated if a specific cause is found:
l. Tumors: glomus, AN,
2. Infections, wax
3. Meniere’s disease:
4. TMJ disorder
5. Otosclerosis
6. Vascular malformations
7. Medications

TINNITUSTREATMENT
Medications:
NSAIDS (motrin, naproxen, relafen, etc)
ASA & other salicylates
Lasix & other “loop” diuretics
“mycin” antibiotics such as vancomycin( rarely macrolides as azithromycin)
Quinine
Chemotherapy drugs as cis-platin
Rarely, SSRI antidepressants as Paxil

SUBJECTIVE TINNITUS
l. Otologic:
Noise induced hearing loss
Presbycusis
Otitis media with effusion
Otosclerosis
Meniere’s disease
Cerumen
Foreign body against tympanic membrane

SUBJECTIVE TINNITUS
2.Drugs:
ASA
NSAIDS
Aminoglycosides
Antidepressants
Heavy metal
3. Metabolic
Vitamin A/B deficiency
Hyperlipidemia

SUBJECTIVE TINNITUS
4. Neurologic:Head trauma
MS
Meningitis
Acoustic neuroma
Temporal lobe tumour
5. PsychologicAnxiety
Depression
TINNITUS & HEARING LOSSCOMMON QUESTIONS
90% of those with tinnitus have some hearing loss. Noise exposure is the most common cause of hearing loss & of tinnitus
Is ringing in my ear normal?
Is it possible for others to hear my tinnitus?
Can I “Toughen Up” My Ears?
How can I tell if Noise is Dangerous?
How is sound measured, and how does Frequency of sound and Intensity of sound affect hearing
loss?
What is a Decibel?

NOISE EXPOSURE &HEARING LOSS
How does noise cause hearing loss? Is it permanent?
What is loud?0 dB faintest sound heard by human ear
30 Whisper, quiet library
40 Refrigerator hum
50 Rainfall
60 Normal conversation, typewriter, sewing machine, truck traffic
70 Washing machine
85 average traffic
95 MRI
100 Blow dryer, subway train,chainsaw, snowmobile
115 Sandblasting, rock concert, auto horn, screaming child
130 Jack hammer, jet engine plane
140 Shotgun blast, airbag deployment, firecracker, pain is experienced in unprotected ears

TINNITUS & HEARING LOSS
Why has hearing loss increased significantly in young people? Loud rock music along with the use of earphones with portable radios
Can noise affect more than my hearing?
Tinnitus commonly occurs after noise exposure, and may be permanent
Who should wear hearing protectors?
What are the laws for on the job?

TINNITUS &HEARING LOSS
OSHA (Occupational Safety & Health Administration) Guidelines
What is permissible Noise Level Exposure?
Hours per day Sound level
8 90 dB
4 95 dB
2 100 dB
1 105 dB
.5 110 dB
85 dB or higher more than 8 hrs. requires hearing conservation programs to protect workers.

TINNITUS & HEARING LOSS
What does OSHA recommend for Hearing Conservation?
l. Hearing protection devices:
2. Education: Sound less than 80 dB is unlikely to cause
hearing loss.
Over 85 dB a One time exposure or continuous noise may cause temporary threshold shift, usually disappears in 16- 48 hrs. after exposure.
3. Noise exposure for unprotected ear is 115 dB for 15 min/day (rock concert 115-120 dB)
4. Noise above 140 dB is not permitted unprotected
TINNITUS & HEARING LOSSHEARING CONSERVATION TIPS
Be conscious of environmental noise: 3 foot rule
Wear earplugs at the movies, ask the manager to turn the volume down
Wear earplugs at amusement parks, concerts
Wear earplugs or earmuffs using power lawn mower, vacuum, power tools
Read labels on appliances, toys that generate sounds
TINNITUS & HEARING LOSSHow effective are hearing protectors?
Earplugs & earmuffs: are about equally effective, reduce noise 15-30 dB. Earplugs are better for low frequency sounds, earmuffs for high frequency sounds
Combined use of earplugs & earmuffs: adds 10-15 dB more protection, should be used if noise is above 105 dB
Can I get protection stuffing my ears with cotton?
Cotton reduces noise by 7dB
Common problems of Hearing Protectors: ½ of workers, get ½ the needed protection because they are not worn continuously & are poorly fit. 7 hrs. of protection is only 9 dB of protection
How do I know I’m getting protection? Your own voice is louder & deeper

TINNITUS & HEARING LOSS
Can I understand other people & hear machinery well enough with hearing protectors? They enhance speech discrimination in very
noisy places. Those with SNHL may have reduced ability to understand normal conversation. Workers adjust to the lower level of noise of machinery & still can detect problems.
How can I tell if my hearing is already damaged?
People seem to mumble, difficulty understanding, need people to repeat frequently, & tinnitus is present
Hearing loss is painless, invisible & comes on slowly
Only sure way to tell is by a hearing test

TINNITUS TREATMENT
As of 4/2002 the National Library of Medicine’s search engine revealed 3900 research articles on tinnitus since
1966
What do you do if you have tinnitus & no specific cause?
l. Avoid noise exposure
2. Avoid stimulants, coffee, tea, coke, nicotine
3. Decrease salt intake (hydrops)
4. Avoid fatique, get adequate rest, daily exercise
5. Avoid ototoxic drugs, as ASA, non-steroidals, quinine preparations
6. Balanced diet, normal amts. Of fruits & vegetables

TINNITUSTREATMENT
Miscellaneus approaches:
l. Hearing aids:
2. Maskers
3. Psychological help:
4. Self help
5. TRT (Tinnitus Retraining Therapy):
TINNITUSTREATMENT
Non-drug treatments: dubious
l. Acupuncture:
2. Electrical stimulation:
3. Electromagnetic stimulation
4. Magnetic stimulation:
5. Ultrasound
6. Surgery