Healthcare System Innovization through Digital Transformation
94
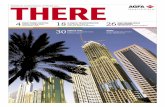
Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 1 Healthcare System Innovization through Digital Transformation First Edition, 2014 Sumit Chakraborty Digital Technology Portfolio DSS ERP Biomedical Technology BI KMS Registration Consulting Testing Discharge Billing & payment Surgery FI-CO, MM,HR SD, PLM Workflow management Project management Supply chain management Maintenance K-creation CoE K-storage Digital library K-sharing by cloud Perception Case based reasoning K-application Diagnosis Analytics Data warehousing Data mining Social Networking Data visualization Performance scorecard Image processing HCI Digital measuring instrumentation E-health cloud M-health Sensors
Transcript of Healthcare System Innovization through Digital Transformation

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 1
Healthcare System Innovizationthrough Digital Transformation
First Edition, 2014
Sumit Chakraborty
Digital TechnologyPortfolio
DSS ERP Biomedical Technology
BIKMS
Registration
Consulting
Testing
Discharge
Billing & payment
Surgery
FI-CO, MM,HR
SD, PLM
Workflow management
Project management
Supply chain management
Maintenance
K-creationCoE
K-storageDigital library
K-sharingby cloud
Perception
Case basedreasoning
K-applicationDiagnosis
Analytics
Data warehousing
Data mining
Social Networking
Data visualization
Performancescorecard
Imageprocessing
HCI
Digital measuring instrumentation
E-healthcloud
M-health
Sensors

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 2
ForewordThis e-book is written for various purposes : (1) an example of project for Management Information
Systems (MIS), Digital Transformation and Enterprise Solutions courses of academic programmes on
business administration (e.g. MBA, PGP, PGDM, PGDCM, PGDBM), information technology, computer
science and MCA; (2) consulting tool of business analysts in IT firms; (3) a reference for the healthcare
system administrators (e.g. CIO, CEO and CFO, ministry of healthcare) and (4) a reference of today’s
research on healthcare informatics and secure multi-party computation. The basic objectives of digital
transformation are to innovate and streamline business models, operational processes and experience of
the patients in healthcare service using information, communication and biomedical technology. This
work presents a healhcareflow mechanism; the intelligence of the mechanism is explored from the
perspectives of knowledge management through case based reasoning, decision making using analytics,
biomedical technology management, workflow control subject to time and resource constraints,
verification of fairness, correctness and privacy of patient data, multi-mode payment function,
cooperative communication protocol for collaborative information seeking, enterprise application
integration and life-science supply chain coordination. The service provider tries to improve the quality of
healthcare service at fair reasonable cost by integrating different enterprise applications through
systematic coordination of material, information and financial flows. This work also suggests the
information, communication and biomedical technology schema required for digital transformation in
terms of computational intelligence, communication, data, application and security schema. It is really
challenging to provide accessible, affordable and quality health care to the rural and urban population
globally.
For effective healthcare system innovization, digital technology management is not only the critical
success factor. There are other several factors. The healthcare consultants, specialists and work force
need a good human resource management model for proper talent acquisition and retention, research
and innovation, career growth planning, incentive, reward, recognition and retirement planning. The
healthcare service provider may have a flawed business model based on old legacy information
technology, malicious healthcare practice due to economic and financial pressure, mechanical HR policy
and bad resource allocation mechanism. The patients or service consumers may lose trust in health care
products and practice due to costly treatment procedure, complicated and fraudulent business rules and
vague computational intelligence. Fairness and correctness of computation and testing is a critical
concern in healthcare practice. Knowledge management is another critical success factor; case based
reasoning may be a good solution for information storage and retrieval.
Research Methodology : The present work has reviewed relevant literature and analyzed five
explorative cases on healthcare and healthcare information systems. The case study approach has been

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 3
selected to support analytical rather than statistical generalization. Case studies capture reality in
considerably greater detail and allow for the analysis of the problems of an adaptive enterprise. The
business processes of a complex multi-tier healthcare supply chain in USA has been analyzed and a group
of experienced healthcare system administrators have been interviewed. This work also explores the
basic properties of secure multi-party computation in healthcare from the perspectives of fairness,
correctness, privacy and rational information sharing.
Keywords: Healthcare information system, Digital Transformation, Computational intelligence, Cloud
computing schema, Artificial intelligence, Case based reasoning, Digital technology portfolio, Data
schema, Networking schema, Security schema, E-health, M-health, Information management schema.
E-book Structure : The present work is organized as follows. Chapter 1 defines the problem of today’s
healthcare service; shows industry analysis, critical success factors, healthcare chain and process flows. It
also presents the basic concept of digital transformation in the context of healthcare service model.
Chapter 2 presents the information technology schema. It explores the digital technology (DT) portfolio
of the healthcare service provider in the context of application schema. Chapter 3 highlights
computational intelligence and computing schema in terms of cloud computing, soft computing, artificial
intelligence, case based reasoning and perception. Chapter 4 and 5 present networking and data schema
respectively. Chapter 6 analyzes security schema. Chapter 7 discusses information management schema
and concludes the work.
Sumit Chakraborty
BEE (Jadavpur University), Fellow (MIS, IIM Calcutta)
Business Analytics Research Lab, India.
E-mail : [email protected]

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 4
ContentSL No. TopicPart I Digital System Schema1.1 Digital Transformation basic overview1.2 Healthcare industry analysis1.2.1 Business objectives1.2.2 Constraints1.2.3 Critical success factors1.3 Process flow analysis for healthcare chain1.4 Healthcareflow mechanism1.4.1 Mechanism’s intelligence analysis
Part II Digital Technology schema2.0 Application schema : Digital technology portfolio and application integration3.0 Computing schema and computational intelligence4.0 Data schema 5.0 Communication networking schema 6.0 Security schema
Part III Digital System Management Schema7.1 Organization structure for digital transformation7.2 Investment analytics for digital technology portfolio rationalization7.3 Strategic roadmap for digital transformation 7.4 Rural healthcare and conclusion
References

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 5
Chapter 1 : Introduction
1.1 What is digital transformation?
This is the case of a large healthcare chain. The healthcare service provider is a large organization having
complex structure. The Chief Information Officer (CIO) is planning to evaluate the scope of digital
transformation in the organization. He would like to discuss various aspects of digital transformation with
the top management. Digital transformation actually demands the fundamental rethinking and radical
redesign of different systems and processes for dramatic improvement of business performance,
quality of service and effective enterprise resource planning and capacity utilization through efficient
and intelligent application of modern information and communication technology and management skills.
It does not mean downsizing. Digital transformation is closely associated with an intelligent design of
information system schema, information technology schema and information management schema.
Today’s healthcare system must require an optimal portfolio of intelligent information and communication
systems and biomedical technology to satisfy various business objectives subject to a set of constraints.
These objectives may be improved quality of service (QoS); fast and correct transaction processing;
efficient management of resources; fast decision making in adaptive situation; improved accuracy in
decision making (e.g. intelligent scheduling, coordination); discovery of hidden intelligence from large
pool of data; supporting knowledge creation, storage, transfer and application in an enterprise;
supporting office automation and workflow control; effective asset management, cost control, revenue
management, strategic pricing and supply chain management and corporate social responsibilities. The
constraints may be time, cost, resources, skill, regulatory compliance, capacity, old and obsolete
technology, malicious and irrational business practice, policy paralysis and administrative failure. Digital
transformation does not mean downsizing; rather it can create new job opportunities through innovative
service offerings.
The basic objectives of digital transformation initiatives are to innovate and streamline business models,
operational processes and customer experience in healthcare service. They change how functions work,
redefine how functions interact and reshapes boundaries of the healthcare service provider. Today, the
healthcare service consumers need great digital experiences. They would like to interact with the
healthcare service providers anytime and anywhere. The healthcare service providers are expected to
build intelligent digital business models which can engage the service consumers digitally through online
and m-commerce mechanisms. A digital business model challenges the physical offline from the
perspectives of internal power, business process design and private data of the consumers. An efficient
digital business model is essential to connect a large or small organization to the service consumers
online. A digital business model has three components such as content (what is consumed), customer
experience (how is it packaged) and technology platform (how is it delivered). For instance, each

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 6
healthcare service provider should have a well-designed web site or portal which can give necessary and
correct information regarding the location, contact number, e-mail, address, transport facilities, service
and product offerings, consultants, approximate tariff or service charge, vision, organization structure,
rules and regulations to the local or national or international patients. The content is basically what is
consumed by the patients. It is applicable to all public and private hospitals, nursing homes and
healthcare clinics. The customer experience is associated with the website and the digitized business
processes such as e-mail acknowledgements, alert, payment processing options, shopping cart and
customer feedback. The platform consists of a set of digitized business process, data and infrastructure.
The platform has internal and external components. The internal platform components may be business
analytics, HR and finance modules; the external platforms include phones, communication networks,
tablets, laptops or computers that consumers use to interact with the healthcare service provider. It is
essential to create unique content with the help of healthcare consultants, experts and specialists for
improving and measuring customer’s experience. It is also required to develop a flexible global platform.
The healthcare service provider should monitor the performance of digital business model through the
feedback of the consumers about content, digital experience and platform.
Traditionally, digital transformation uses different types of technologies such as enterprise resource
planning, supply chain management and business intelligence solutions, analytics, mobile communication
system, social media and smart embedded devices to improve business performance, quality of service,
value propositions and internal processes. Additionally, the healthcare business model requires the
support of modern biomedical technology such as digital measuring instruments (e.g. blood pressure,
blood sugar, digital thermometer, digital stheoscope, digital x-ray), biosensors and human computer
interaction. The healthcare organizations often face common pressures from their customers, competitors
and workforce to take initiatives and show high commitment in digital transformation. But, it may occur
at different paces with different results. It explores new business opportunities and service offerings with
the support of biomedical, information and communication technologies. It must be driven by the top
management; it requires high commitment of top leaders, system and business analysts; strategic moves
of change management through monitoring a set of performance metrics. The top management may
create a new organization or reshape the boundaries of the organization by using strategic assets in new
ways. It is essential to manage people, processes and technology in a smart way.
The CIO has discussed with the top management of healthcare organization on critical steps and
strategies for digital transformation. For digital transformation, the top management of an organization
should see beyond the hype of new generation technology. An organization may often feel of getting
routine results from the investment in new technologies. The system and business analysts should try to
explore new ways of doing business and offering services to the service consumers by using digital
technology. They must understand the opportunities and threats of new technologies; they should assess
and mitigate the risks in time. An organization changes not only by using technology, but also by

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 7
improving its processes, business models and management skills. The top management should find
skilled, experienced and innovative technologists at a high level of decision making; those experts should
be capable of evaluating today’s digital technology platform correctly and convincing the leaders on the
risks and scope of technology appropriately. The top management should be able to take fast and correct
decisions in choosing right technology at right time. In other words, they should not adopt digital
technologies blindly; the project management team should run a pilot, test, get feedback from the
stakeholders and fine tune the new system. Such type of phased experimental approach can reduce the
chance of disaster or failure of new digital technologies. The project team requires a mix of experts on
different digital technologies. Digital transformation requires an open, transparent, fair and rational
corporate culture. It never stops; it is a continuous process. Despite the hype around disruptive
innovation of digital technologies, the healthcare service provider still has a long way to go in the journey
of digital transformation through enhanced customer experience, streamlined operations and processes
and creating new business models and service offerings. The CIO has asked the business analysts for a
detailed process flow analysis to study as-is system, find out the gap and design to-be system of the
healthcare service provider.
1.2 Healthcare Industry Analysis
The CIO has met with the chief of corporate strategy division in presence of the business and system
analysts and have discussed regarding the critical issues of today’s healthcare service industry such as
competition, value based service delivery model, competencies and the role of digital technology. Today’s
healthcare service sector faces several challenges such as increasing costs, poor quality of service in rural
and remote zone, unhealthy competitive environment, limited or non-existent measurements of costs
and outcomes and increasing demand. The outcome and critical observations of their meeting are as
follows:
The existing healthcare service may have a flawed business model based on old legacy information
technology, economics and financial pressure, mechanical HR policy and bad resource allocation
mechanism (e.g. health insurance scheme). The healthcare workforce may be forced to work under
excessive financial and economic pressure.
The healthcare workforce (e.g. consultants, nurses, surgeons, testing, maintenance, registration,
discharge and billing associates, system administrators, IT people) expect a good HR model for
proper talent acquisition and retention, research and innovation, career growth planning, incentives,
reward, recognition and retirement planning scheme. the quality of healthcare service may be
affected seriously if they are forced to work driven by economic and financial pressure, hard target of
revenue and profit, malicious business practice and evil wishes. The society should not accept narrow

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 8
and negative outlook, thoughts and policies created by the management scientists, statisticians,
economists, strategists and HR experts.
Fairness and correctness of computation and testing is a critical concern in healthcare
practice. Another important issue of secure multi-party computation is privacy of patient’s data. The
public may be losing trust in existing health insurance products and health care practice due to
dishonest and costly treatment procedure, complicated and fraudulent business rules and statistical
illusions.
Digital technology management is a critical success factor of healthcare service. Case based
reasoning can be a good solution for knowledge management.
Health security should cover each member of a society. Each member should have access to an
extensive set of healthcare services at fair, affordable and reasonable cost. Land is not a problem for
building smart healthcare infrastructure. The critical issues are efficient corporate governance free of
power play and politics, good medical practice and fair resource allocation mechanisms.
Advanced medical science evaluates quality of healthcare service through the outcomes achieved in
the treatment of illness. An increasing expectation of the service consumers and the change of
patient demographics due to aging population threaten to increase healthcare costs and restrict
timely access to patient care services. The aging and retiring skilled healthcare workforce affect
sustainability of the system. The system should utilize its resources and assets rationally and develop
and acquire new talents. Life is a precious asset of human society; it should be saved irrespective of
age, gender and social status.
The chief manager of corporate strategy is trying to convince the CIO about the basic concept of value
based healthcare service model. The basic objective of healthcare service model is to achieve high value
in terms of quality and access to different service offerings, outcome, cost, safety, convenience and
overall satisfaction index of the stakeholders associated with health chain. Outcomes are health results
for a patient’s condition over a healthcare cycle; costs are the total costs of care over the care cycle.
The CIO and the system analysts have informed the CIO that it is not a simple task to compute value in
terms of outcome achieved and cost of treatment for a healthcare system precisely. It is difficult to
quantify the outcome of healthcare service since it is a multi-dimensional parameter and depends on the
perception of the service consumers; it is possible to compute cost of healthcare service approximately
through financial and cost accounting system.
Value is the basic building block of performance improvement in healthcare service. A healthcare service
provider should focus on value, volume, efficiency and operational excellence through process re-
engineering simultaneously. Value is created across different tiers of healthcare chain spanning over a
specific set of services jointly satisfying the basic needs of a patient. The needs of the patients are
related to personal medical problems which may be addressed through proper coordination. For primary

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 9
and preventive care, value may be measured for specific patient groups with similar needs. It is created
over full care cycle through efficient supply chain coordination. The patients often require an integrated
unit accountable for total care of a complex medical problem. The patients can perceive value in terms of
sustainable recovery, need for ongoing interventions and reoccurrence of ailment. Value is created
through excellent delivery service, cost control, knowledge management, innovation, fair and correct
medical practices. A healthcare information system may track value of service through an innovative
patient’s feedback and performance scorecard.
Next, the chief manager of strategy has brought the issue of competition in the context of healthcare
service industry. The healthcare service providers are expected to compete based on cost and quality of
services. Such type of competition can result efficiency, effectiveness, operational excellence, reduction of
errors and disruptive innovation. They should be able to improve value in terms of quality of service and
cost. A provider should not only compete in local area but also in regional and national domain to
improve its business performance. They should develop differentiated services and facilities to create
unique value through use of digital technology, knowledge management, supply chain coordination. They
should develop competencies in medical diagnosis, prevention and treatment of specific diseases and
share correct data on the performance of their workforce, operational excellence and infrastructure
publicly through web services. They should get incentives for their specialized skill, operational
excellence, expertise, quality of service and efficiency. The providers should learn continuously and
innovate based on errors and feedback of the service consumers.
The chief manager of strategy has outlined the vision of a value based healthcare system, which should
be built upon a series of core principles. The service provider should clearly define the goal, organization
structure and the role of different stakeholders associated with the health chain. Each actor must
contribute to value. Even, the health plans or insurance providers can contribute rather than acting as
passive actors. The fundamental goal of the healthcare system is to provide timely access to care and
deliver good value for patients through cost control. The system needs an efficient healthcare delivery
model which is capable of controlling cost and improving value through various ways such as
recommending healthy living practice, accurate diagnosis, timely access to services and good
coordination among the workforce. The service should be organized around medical problems of the
patients over the full cycle of care through integrated practice units. The value is increased by the
experience, scale, skill and learning of the workforce through optimal breadth and depth of service
offerings. Many providers offer a broad range of services but the volume of care for any one service is
small. The provider may not be able to provide value for each service due to lack of proper facilities, skill
and knowledge. The provider should design its service lines strategically based on competencies. The
value should be appropriately measured and reported. The incentives should be aligned with value and
innovation should be rewarded.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 10
The business analysts are able to identify the problem, business objectives, constraints and critical
success factors of the healthcare service provider by analyzing vision, mission statement, corporate policy
and annual reports and also through industry analysis. The outcome is listed as follows :
1.2.1 Business objectives
Ensure high quality of service, work culture and administrative efficiency
Efficient time management and resource allocation for optimal capacity utilization
Fast and correct transaction processing for efficient enterprise resource planning and supply chain
management
Develop a highly skilled and innovative workforce through efficient knowledge management
Optimal fund allocation for digital technology portfolio rationalization
Revenue management through fair pricing, corporate social responsibilities and good medical practice
Intelligent HR policy in terms of talent acquisition, retention, incentives, training, career growth and
retirement planning
Building an innovative business model, mechanism and organization structure of the healthcare
service provider
Effective healthcare service model
o Prevention of illness : Early detection, right diagnosis, right treatment to right patient
o Rapid cycle time of diagnosis and treatment
o Treatment : Less invasive treatment methods, fewer complications, fewer mistakes and
repeats in treatment, faster recovery, more complete recovery, greater functionality and less
need for long term care, fewer recurrences and relapses
o Reduced need for visits, slower disease progression, less care induced illness
o Better health is less expensive than poor health
o Better health is the goal, not more treatment
1.2.2 Constraints
Resources (man, machine, material, method, money, land)
Digital technology infrastructure
Skill of experts for complex decision making
Timeline for digital transformation
High cost
Quality of service and
Process efficiency in supply chain coordination
Overcapacity in urban zone and shortage of capacity in rural zone
Large variation in quality across providers
No systematic measurement of outcomes and costs

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 11
Difference in QoS between public and private healthcare system
Many incremental reforms with limited impact
1.2.3 Critical Success Factors
Digital technology, an optimal mix of information, communication and biomedical technologies
Fairness, correctness and privacy in secure multi-party computation
Knowledge management
High commitment, cooperative work culture and skill of healthcare consultants and workforce
Supply chain coordination
Streamlined process flows and workflows subject to time and resource constraints
Disruptive innovation
Intelligent human resource management model
Free choice of health plans and providers, universal access to health insurance with a broad
range of services
Extensive network of capable providers
Scalability in excellent and compassionate rural care
The teams have come to a conclusion that the healthcare service provider must deploy an efficient
delivery service model which requires deep insights into the needs of the service consumers, process
flows, mechanisms, protocols and business rules. This innovation can be explored in terms of the
structure of interactions, service boundary, allocation of tasks and resource and delivery locations. The
service consumers and providers require a good coordination mechanism through information and
communication technology. The service provider should be able to optimize the breadth and depth of its
service offering based on competencies and facilities. The system should manage workflow control
subject to time and resource constraints. The outcome of patient care may be affected with the strategic
importance of location of healthcare facilities.
1.3 Process Flow Analysis
Healthcare Chain : The business analysts have shown the architecture of the health chain to the CIO.
Figure 1 shows the complex multi-tier architecture of a healthcare service model: patients (tier 1);
branded and non-branded hospitals, medical surgery centers and physicians (tier 2): healthcare service
providers (HCSP) having service centers and distribution centers (tier 3); distributors, wholesalers and
retailers (tier 4); suppliers, drug manufacturers and medical device manufacturers (tier 5) and carriers
(tier 6). Information and funds flow from tier1 - tier2 - tier3 - tier4 - tier5 - tier6 through the information
system and healthcare products and services flow in the reverse direction. The information is related to
healthcare products, services, providers and consumers. Healthcare supply chain is a network of
organizations that satisfies the demand of the service consumers for healthcare products and services.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 12
The basic objective is to improve the quality of service in patient care by integrating different business
units through systematic coordination of material, information and financial flows. The business and
system analysts intelligent mechanism for the above healthcare service model.
Figure 1: Healthcare Chain
Figure 2 : A typical process flow in a healthcare organization (through swim lane diagram)
Registrationassociate
Consultant
Testingassociate
Supply chain coordinator
Surgeon
Discharge associate
Dispute resolver
Billingassociate
Registration
Consulting
Testing
SCM & QC
Dispute resolution
PaymentBilling
Operation
Discharge
Collect payment in advance

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 13
The business analysts have done process flow analysis (Figure 2) and have found out many gaps in
existing healthcare operation and the use of information technology, particularly for rural healthcare
institutes. For example, the existing registration system use spreadsheets without verifying the identity
proof of the patients; the system does not generate any registration card and is not integrated with other
applications. There is no information system used for workflow control and appointment fixing for
consulting and surgery scheduling. The healthcare consultants write prescriptions manually based on
memory and experience without taking the help of any information system. There is no case based
reasoning system for proper knowledge management. The healthcare workforce do not use digital
measuring instruments. The as-is system does not support quality control initiatives of the drugs, medical
devices and healthcare products through any materials management and quality control modules. The
system does not support purchasing, goods receipt, inspection, acceptance or rejection of goods, vendor
control and invoice verification electronically. The testing lab faces various problems such as poor manual
documentation, lack of sufficient number of testing professionals, risk of mixing or swap of test results
and delay in delivery of test reports for emergence cases. The discharge certificate is prepared using
word pressing software; there are evidences of mistakes in event logs and the instructions of medical
administration and follow up are not clear. The data of patient’s help guide is not updated regularly; the
tariffs or service charges as mentioned in the bulletin board do not match with the data used in medical
bills. The payment processing system does not support credit card, e-banking and e-health insurance
facilities due to lack of proper application integration. The billing system does not provide break-up of
total bill amounts and tax computation; just shows summary. No online system is used for getting
patient’s feedback or providing patient’s help guide. In urban hospitals, the healthcare service provide
takes feedback of the patients through survey; but there is risk of incorrect feedback due to various
reasons such as wrong perception, misunderstanding of the tough questions used in the survey or lack of
knowledge or critical observations of the patients and their attendants and the timing of survey.
1. 4. Healthcareflow Mechanism
Digital transformation requires an efficient and intelligent mechanism. The business analysts of the
healthcare organization have developed an intelligent mechanism in terms of a set of agents, inputs,
outputs, strategic moves, protocol, revelation principle, payment function and information system
schema. It is the basic building block of healthcare business model. An efficient mechanism provides
different benefits such as improved customer service, accuracy, ease of processing, increased
productivity, quick access to information, greater geographical reach, better coordination, reduced
transaction costs, rational decision making and efficient knowledge management. But, it has several
constraints and challenges like high cost of computation and communication, information flow, privacy of

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 14
data, coordination, economic modeling, pricing strategy, payment, fairness and correctness of service
transactions and behavior of the service consumer and provider.
Agents: Service consumer or patient (C), Service providers (P): workflow (Pw), healthcare (Ph), testing
(Pt), financial service (Pf) and supply chain (Ps), maintenance (Pm), system (Psy) and human resources
(Phr);
Input : Data of C, P, healthcare products, services and pricing plan;
Strategic move: Knowledge management through case based reasoning; decision making using
analytics; biomedical technology management; workflow control subject to time and resource constraints;
verification of fairness, correctness and privacy of data; multi-mode payment function; cooperative
communication protocol; enterprise application integration, life-science supply chain coordination and
rational investment planning for IT portfolio optimization.
Protocol:
1. Registration : Pw call workflow management system → register C through a service contract on fair
healthcare and privacy policy; make a meeting plan for consultation and collects payment in advance. C
approaches P personally or with the help of family members, friends or security workforce.
2. Consulting: Ph call case based reasoning system → do health check-up and diagnosis; recommend
medication and testing.
3. Testing (optional) : Pw make a testing plan for C and sends it to Pt; Pt do testing; send test data to Ph;
Ph call analytics → make decision and recommendations.
4. Supply chain coordination: Ps call ERP-SCM system → do demand and distribution planning by CPFR,
inventory control, sourcing, order management, warehousing and shipping of medicines and medicare
products. C and P should verify the quality, performance and warranty of the biomedical devices while
sourcing the same from local or global vendors.
5. Surgical operations (optional) : Pw make operation plan; Ph perform operation on C. The process having
steps 2-5 may have single or multiple iterations depending on the complexity of the problem of C. C may
take the opinions of more than one healthcare specialists.
6. Receivables management: Pf call ERP system → generate invoice; process payment for C in single or
batch mode.
7. Dispute resolution: C verifies fairness and correctness of all transactions. C and P negotiate and settle
any medical, financial or privacy disputes mutually or with the intervention of a trusted third party.
8. Exit: Pw issues discharge certificate to C. C may exit from the system at any stage by submitting a
bond to Pw. Psy stores data of C in a secure data warehouse.
Revelation principle: Rational data sharing, fairness and correctness of computation, Privacy
preserving data mining through cryptographic and secure multi-party computation protocols, secure data
warehousing;

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 15
Payment function: The basic components of the payment function are discriminatory pricing scheme,
incentive, discount, penalty and multimode payment options comprising of free health check-up, health
insurance, corporate mediclaim policy, credit card, direct cash payment and bank loan; Phr process salary
of healthcare workforce.
Information system schema :
computational intelligence : workflow control for time scheduling and resource allocation; case based
reasoning: case retrieval and adaptation mechanism; analytics: data visualization and performance
scorecard; transaction processing for registration, testing, payment and discharge;
communication schema : web (e.g. e-mail, social networking), mobile communication (e.g. wireless
internet), netmeeting and videoconferencing system for virtual patient care and telemedicine;
data schema : data warehouse, data mining, relational database;
application schema : web enabled ERP, business intelligence system, knowledge management system;
Output: healthcareflow plans, transaction documents, business intelligence reports.
1.4.1 Mechanism’s intelligence analysis
In the above mechanism, the cost of communication depends on the interactions between the service
consumer and service provider; the number of negotiation rounds and the frequency of information
sharing among the trading agents associated with the supply chain. It depends on the complexity of
critical patient care and workflow control subject to time and resource constraints. It also depends on
cooperative communication among the healthcare specialists for collaborative information seeking and
knowledge management through videoconferencing and wireless or wired networks. The cost of
computation depends on the complexity of various algorithms associated with workflow control for time
scheduling and resource allocation; case based reasoning; analytics for data warehousing, data mining,
data visualization and performance scorecard and transaction processing for registration, testing,
payment, discharge and supply chain management. It also depends on the complexity of encryption and
decryption algorithm and signcryption to preserve the privacy of data. The cost of signcryption is
relatively less than the cost of signature-then-encryption approach.
An optimal mix of strategic moves provides adequate intelligence to the mechanism (HM) for
improved quality of service.
The mechanism requires a fundamental rethinking and radical redesign of healthcare practice and
infrastructure in terms of technology management, organization structure, operations, marketing,
financial and human resources management. The basic objective of the service provider is to improve the
quality of healthcare service at fair cost by adopting a set of intelligent rational strategic moves such as

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 16
case based reasoning, decision making using analytics, workflow control subject to time and resource
constraints, verification of fairness, correctness and privacy of data, multi-mode payment processing
system, cooperative communication protocol for collaborative information seeking, enterprise application
integration and life-science supply chain coordination. The healthcare service agents should use
intelligent information and communication technology schema for workflow control, transaction
processing, complex decision making, knowledge management and improved supply chain coordination.
The next theorems analyze these strategic moves in details. Additionally, the healthcare specialists should
be able to utilize the intelligence of modern biomedical engineering (e.g. bio-sensors, organ
transplantation), bio-inspired artificial intelligence (e.g. robotics in surgical operations), advanced testing
system (e.g. image processing, CT scanner, x-ray and homecare kits) and the innovations in life-science
industry (e.g. drug discovery) for critical patient care.
The mechanism (HM) adopts discriminatory pricing strategy, multi-mode payment options,
efficient ERP and application integration for fairness and correctness in revenue
management and cost control.
The healthcare service provider formulates a discriminatory pricing strategy for different types of service
offerings to ensure good quality of service at reasonable cost. The pricing strategy requires competitive
intelligence to ensure a sustainable business model. The mechanism must ensure fairness and
correctness of computation for the service consumer in testing and financial transactions processing
through the use of intelligent enterprise applications and honest and transparent work culture. A service
provider can optimize profit and revenue through malicious practice like unnecessary testing, operation,
ventilation, error in diagnosis, recommending costly drugs, lucrative incentive policy and incorrect
computation. The mechanism requires the support of efficient regulatory compliance policy and dispute
resolution protocol to resist malpractice and errors. Theorem 4 discusses these issues in details. It is
essential to declare brain death of the patients by the critical care expert, medical super, neurologist and
neurosurgeon before cardiopulmonary death. It saves the cost of unnecessary ventilation. It is also
possible to do transplantation of critical organs of a dying patient (e.g. heart, kidney, lungs, pancreas,
skin) to save the life of other patients. The revenue of the service provider can be optimized in various
fair ways such as regular preventive health check up, scalability, increased number of service offerings
(e.g. yoga, meditation, nutrition, childcare, men and women care, old people care, sports people care,
disabled and physically challenged people care, stress control), strategic pricing, efficient financial
accounting and cost control (e.g. cost of energy and utilities, rational use of communication schema,
intelligent architecture resulting optimal space utilization, reduced wastage of drugs, blood and medicare
products etc.). The primary healthcare centres, district, rural and state general hospitals should have
facilities of medical diagnosis and pathological tests (e.g. TC, DC, ESR, sugar, liver function test, USG, X-

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 17
ray etc.) and distribution of common and essential drugs to the poor patients at fair and reasonable cost.
The payment processing system offers multiple options such as health insurance, corporate mediclaim
policy, credit card and direct cash payment. Such a flexible system requires effective enterprise
application integration among multiple organizations like healthcare service provider, vendors, insurance
companies and banks through an web enabled ERP system.
The revelation principle of the healthcareflow mechanism ensures security and privacy of
strategic data through secure data warehousing, privacy preserving data mining and basic
cryptographic tools like encryption, digital signature and signcryption.
The privacy of healthcare information is protected by various regulations that apply to healthcare plans
and electronic healthcare information in financial and administrative transactions. The healthcare
organizations are known as covered entities in the regulation. The regulation protects healthcare
information only if it is identifiable and created or received by a covered entity. The healthcare service
provider, health insurance provider and other healthcare professionals jointly maintain the privacy of
medical data of the service consumers or patients. The mechanism requires a trusted computing
environment. The primary objective of e-health is to increase the flow of healthcare products and
information so that the patients can get right treatment in time. The participation of healthcare
professionals and healthcare institutes in patient care should be nonrepudiable. A good e-patient care
system is essential for global healthcare outsourcing business model where no direct patient interaction is
involved. For example, there is shortage of medical experts for healthcare firm 1 at location A; the firm 1
uses an outsourcing business model. There are skilled medical experts in another healthcare firm 2 at
location B. The files of x-rays, CT scans, MRI and other test reports of the patients of firm 1 are uploaded
at the e-patient care system. The medical experts of firm 2 study the uploaded reports and perform the
diagnosis. The critical success factors of this practice are strict regulatory compliance, liability, privacy
and high quality medical practice, good outsourcing infrastructure, low cost base and proper utilization of
time zone difference. E-patient care is particularly useful for rural healthcare at remote locations. In this
patient care model, signcryption ensures confidentiality, message integrity and non-repudiation of
transmitted data. A real-time service oriented architecture can support critical patient care locally and
remotely through secure transmission of medical data stream. Here, data management is a critical issue
since the patients are attached with electronic sensors and life-support devices and these instruments
transmit real-time data to the service provider through authenticated communication channel. Access
control, security, privacy and trust are prominent issues of advanced patient care while the patient is
located at home or another medical facility.
The mechanism should ensure confidentiality, integrity and availability of data in real-time information
exchange among various tiers of healthcare supply chain. It is required to protect the confidential

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 18
information in storage and transmission. The information created and stored by the healthcare service
provider needs to be available to authorized entities in a timely manner. The confidentiality of data may
be affected by snooping i.e. unauthorized access or interception of data. The integrity of data can be
threatened by modification, masquerading, replaying and repudiation. Another critical issue is denial of
service which can threaten availability of data in time. The mechanism should protect the healthcare
information system from all these malicious attacks for better business continuity and improved customer
service. Privacy is required to maintain the competitiveness and reputation in e-healthcare and to avoid
the bias of trading agents. But, absolute privacy may result loss in e-transactions due to increased
transaction costs, lack of reputation, loss of coordination and relationship. Similarly, absolute anonymity
may cause serious flaws in regulatory compliance of the healthcare business.
The mechanism must address correct identification, authentication, authorization, privacy and audit for
each e-transaction. For any secure service, the system should ask the identity and authentication of one
or more agents involved in a communication. The agents of the same trust zone may skip authentication
but it is essential for all sensitive communication across different trust boundaries. After the identification
and authentication, a service should address the issue of authorization. The system should be configured
in such a way that an unauthorized agent cannot perform any task out of his scope. The system should
ask the credentials of the requester; validate the credentials and authorize the user to perform a specific
task. Each trading agent should be assigned an explicit set of access rights according to the assigned
role. Privacy is another important issue. A trading agent can view only the information according to his
authorized access rights. Finally, the system should audit each transaction, what has happened after the
execution of a specific service transaction. Secure communication is a critical issue of service oriented
computing model. The basic objective is to provide confidentiality, data integrity, authentication and non-
repudiation in the communication of sensitive data. Cryptography ensures privacy and secrecy of
sensitive data through encryption, digital signature and signcryption.
The mechanism should ensure confidentiality, integrity and availability of data in real-time information
exchange among various tiers of healthcare supply chain. It is required to protect the confidential
information in storage and transmission. The information created and stored by the healthcare service
provider needs to be available to authorized entities in a timely manner. The confidentiality of data may
be affected by snooping i.e. unauthorized access or interception of data. The integrity of data can be
threatened by modification, masquerading, replaying and repudiation. Another critical issue is denial of
service which can threaten availability of data in time. The mechanism should protect the healthcare
information system from all these malicious attacks for better business continuity and improved customer
service. Privacy is required to maintain the competitiveness and reputation in e-healthcare and to avoid
the bias of trading agents. But, absolute privacy may result loss in e-transactions due to increased
transaction costs, lack of reputation, loss of coordination and relationship. Similarly, absolute anonymity
may cause serious flaws in regulatory compliance of the healthcare business.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 19
The CIO and system analysts have been trying to fix the positioning strategy of the healthcare service
provider. The existing business model is acting as a beginner; the healthcare workforces are using e-mail,
internet and tradition softwares (e.g. word processors, spreadsheets). But, they lack experience with
emerging digital technologies. Now, the CIO has to decide whether the healthcare service provider should
adopt a conservative, fasionista or digrati approach. A conservative firm may struggle to adopt new
emerging digital technology though its management has a vision and effective structures to govern DT. A
fashionista firm is very aggressive in adopting new technologies, but may not have proper coordination
mechanisms or vision of DT. The CIO has selected Digirati approach which shares a clear vision of DT,
optimal investment in emerging digital technologies timely and managing the DT portfolio effectively to
gain the most value from digital transformation.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 20
Chapter 2 : Application Schema
An efficient healthcare information system integrates various enterprise applications while maintaining
individual autonomy and self-governance. The system should support confidentiality, message integrity,
non-repudiation, auditing and availability of service in time. The system should support sharing of data in
a collaborative business environment wherein a group of trading agents can exchange strategic business
information maintaining the privacy of critical data. Increased organizational agility is required for the
cooperation of adaptive enterprises. Information technology can improve the quality of service and
reduce cost in healthcare services. The demand for critical patient care is growing. But, many small rural
healthcare centers are facing problems to develop and maintain a costly IT infrastructure. This forces
those healthcare centers to search for innovative IT platform. E-health is a promising IT platform of
healthcare services.
The concept of e-health is promising; still there are lots of challenges. Many healthcare service providers
are reluctant to adopt or migrate to web enabled systems due to various reasons. One of the major
threats is security and privacy of data. Threat of Electronic Data Interchange [EDI] is another critical
issue. EDI is the electronic exchange of business information in a standard format among the trading
agents. Many healthcare service providers are still managing their business operations using EDI and FTP
protocols. They believe that EDI is a reliable robust system which can ensure the security and privacy of
data. But, EDI has several limitations. The major limitation is the investment in the initial set-up and the
high cost of implementation, customization and training. In healthcare business, the supply chain
network of a healthcare service provider grows periodically. New trading partners get added to the
existing supply chain architecture which become complex gradually. The cost of communication and
adoption of EDI technology is relatively high as compared to web enabled system.
This section presents a case of the application schema of a complex healthcare organization (P). The
healthcare service provider would like to maximize the business value from the investments in
information, communication and biomedical technologies. The provider has decided to manage digital
technology as a portfolio of assets similar to a financial portfolio; the primary objective is to improve the
performance of the portfolio by balancing risk and return. The chief information officer (CIO) of the
organization would like to align digital technology with the business strategy of the organization through
an effective IT portfolio management practice and an optimal mix of enterprise solutions or applications.
The top management has asked the CIO some fundamental questions:
What is the IT portfolio essential for the digital transformation of the healthcare organization (P)?
Does it require efficient enterprise application integration?
What are the inputs, outputs, process flow logic, protocol and mechanism essential for each
application?

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 21
How can the service provider use information and communication technology for effective and
intelligent decision making, transaction processing and knowledge management ?
How can the service provider use analytics and business intelligence system effectively for corporate
strategy formulation?
Does digital transformation require the intelligence of biomedical engineering from the perspective of
image processing, human computer interaction (HCI), and sensors for e-health and m-health service?
2.1 Digital Technology (DT) Portfolio Rationalization
Figure 3 : Digital Technology Portfolio for Healthcare System
Digital Transformation requires efficient enterprise application integration among DSS, ERP,
SCM, BI, WFMS and KMS and biomedical systems for improved quality of service,
coordination and resource utilization.
The CIO has consulted with the business analysts of the healthcare organization and they have jointly
designed an IT portfolio for the digital transformation of the complex business model of P (Figure). The
complexity of application schema depends on the architecture of healthcare chain, breadth and depth of
DT Portfolio
DSS ERP Biomedical BIKMS
Registration
Consulting
Testing
Discharge
Billing & payment
Surgery
FI-CO, MM,HR
SD, PLM
Workflow management
Project management
Supply chain management
Maintenance
K-creationCoE
K-storageDigital library
K-sharingby cloud
Perception
Case based reasoning
K-applicationdiagnosis
Analytics
Data warehousing
Data mining
Social Networking
Data visualization
Performancescorecard
Image processing
HCI
Digital measuring instrumentation
E-healthcloud
M-health
Sensors

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 22
service offering, scalability and the complexity of process flows. A simple healthcare service model may
require only a transaction processing system having patient registration, billing and payment processing
modules. But, the complex healthcare model P requires an optimal mix of decision support system (DSS),
enterprise resource planning (ERP), knowledge management system (KMS), business intelligence (BI)
and intelligent biomedical system. An web service oriented architecture can integrate multiple enterprise
applications properly to ensure improved coordination among different functional units of the healthcare
service provider. Efficient enterprise application integration is useful for payment processing, financial and
cost accounting, workflow control and supply chain coordination.
The CIO was analyzing each branch of the decision tree as shown in figure. A simple decision support
system should have workflow control, registration, consulting, testing, surgery scheduling, billing,
discharge and conference meeting modules. The business intelligence system should have data
warehousing, analytics, data visualization, data mining and performance measurement modules. The
healthcare specialists require intelligent test report analysis based on time series data, graphical
presentation and performance scorecard. The knowledge management system should support creation,
storage (e.g. digital library, CoE), sharing and application of knowledge through case based reasoning
and perception. Case based reasoning offers different types of benefits to a healthcare KMS. Knowledge
acquisition task becomes simple; the decision making agents can avoid repetiting mistakes made in the
past. They can reason incomplete or imprecise data; they can explore a new domain efficiently. They can
avoid repetition of all the steps that need to be taken to arrive at a solution. The recommender system
can learn over time as it encounters more situations and create more solutions. The case based
reasoning mechanism can be used in different ways to a broad range of domains. The CIO has also
considered some other important applications such as enterprise resource planning (ERP), supply chain
management (SCM), information security, videoconferencing, netmeeting, telemedicine and regulatory
compliance.
2.2. Healthcare Information System : Primary Modules
A decision support system (DSS) is an interactive, flexible and adaptable computer based information
system specially developed for supporting the solution of a non-structured, semi-structured or structured
problem for improved decision making. It uses data, provides easy user interface and can provide
decision maker’s own insights. In addition, a DSS may use interactive models and may include a
knowledge component. The business analysts have done process flow analysis and requirements
engineering of the healthcare information systems and have recommended a set of essential deliverables
of HIS to the CIO. The output of the basic modules of HIS include registration card, appointment slip and
medical prescription for consulting, surgery schedule, quality control certificate, test report, discharge

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 23
certificate, bill and payment, online feedback form and patient’s help guide. The analysts have outlined
the inputs to each module, outputs of HIS, process flow logic, protocol and complexities of each
deliverable or output. This exercise gives the basic overview of data and computing schema essential for
digital transformation. Sequential process flows are suitable for normal case, parallel process flows are
suitable for emergency cases. But, the system should check and complete each task correctly.
2.1 Registration Card
Agents: Registration associate (R), Healthcare service consumer (C);
Input : Name of patient, address, contact phone number, e-mail id, medical problems : symptoms,
medicine consumed (if any), case history, drug allergy;
Protocol :
1. The patient or the attendant of the patient fills registration form. R checks voter ID card/
passport / ration card / aadhar card/ PAN card for correct identification of the patient.
2. R enters the patient data into the system and generates registration card with registration
number and healthcareflow chart and allocate resources.
Output: Registration card [registration no., date of issue, patient’s name, age, gender, bar code,
consulting hours, address, logo]; patient’s flow chart [registration no., patient’s name, serial no., date,
process, signature]
2.2.1 Appointment Slip for Consulting
Agents : Appointment scheduler (A), Healthcare service consumer (C);
Input: Name of patient, Address, Contact phone number, E-mail id, Medical problem;
Protocol :
1. C submits registration card and medical documents to A.
2. A enters the patient’s data into the system; searches for empty slot as per availability of
consultant; fixes time and date through negotiation with patient, reserves slot and generates
appointment slip based on availability of consultant and First-In-First-Out (FIFO) queuing rule.
3. A manages exception rationally based on the critical and complex nature of a case and
emergency.
Output : Appointment slip [registration no., patient’s name, age, gender, appointment no. and date,
date of appointment, consultant, healthcare service: specialist and treatment, consulting charges,
location, remarks, issued by]
2.2.2 Prescription by Consultant
Agents : Healthcare consultant or Doctor (P), Healthcare service consumer (C);
Input : Registration card; Patient’s flow chart;

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 24
Protocol :
1. C produces registration card to P.
2. P checks case history and test reports of C; verifies health conditions of C; calls case based
reasoning system.
3. D generates prescription from HIS and gives to C.
Output : Prescription [ Registration no., name of patient, age, gender, location, consultant’s name, date
and time; Diagnosis : medical problem, case history, measurements : weight, blood pressure, body
temperature, pulse rate; medicine prescribed : serial no., medicine name, form, dose, frequency,
duration, quantity, from, to, remarks; special instructions: testing, surgical operations, next appointment
: consultant, location, time ]
2.2 Surgery Schedule
Agents: Scheduling associate of surgery scheduling center (S), Healthcare service consumer (C);
Input: Registration card, patient’s flow chart, consultant’s prescription;
Protocol :
1. C submits registration card and medical documents to S.
2. S enters the patient’s registration no. into HIS; searches for empty slot as per availability of
operation theater and surgeons.
3. S negotiates with C on technical and commercial issues of various options: technical specification
of medical device to be implanted, make, features, surgical operation procedure and tariff;
4. S fixes time and date of surgical operation through negotiation with patient, reserves slot and
generates surgery schedule based on availability of surgeons and First-In-First-Out (FIFO)
queuing rule. S manages exception rationally based on the critical and complex nature of a case
and emergency.
Output : Surgery schedule [ Report id, user id, date and time; registration no. of patient, patient’s name,
age, gender, surgery advised, organ, name of surgeon, list of pre-operative medical tests and charges,
advance to be deposited for surgical operation, admission date, surgery scheduled date and time,
reporting location / unit, anticipated duration of stay, pre-operative treatment : drugs, instructions of use,
remarks : emergency contact];
2.4.1 Quality Control Certificate
Agents: Healthcare service consumer or patient (C), healthcare service provider (P), Quality control
associate (Q), vendor or supplier (V);
Input : Registration ID of patient, Purchase order no. of medical device or drug;
Protocol :
1. C gets admitted to the hospital; the surgeon or doctor consults with C.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 25
2. P issues RFQ (request for quotation) to the vendors.
3. The vendors submit bids or quotations.
4. C and doctor jointly select the best bid subject to financial and quality constraints and C signs
device consent form.
5. P issues purchase order to V.
6. V supplies the medical devices or drugs with invoice. P makes goods receipt note (GRN) in the
system with reference to purchase order.
7. Q inspects the model, technical specification, manufacturing date, import history, valid warranty
period, test certificate, manual, programming performance and invoice in presence of the patient
or his attendant and accepts or rejects the device. The basic objective is to procure the best and
latest model.
8. If there is a three way match between purchase order, GRN and invoice; C gives payment to V
by cheque or credit card. The vendor issues receipt of cheque.
9. The device gets installed; the performance is monitored for a specific duration. If there is any
problem in device’s performance; V is recalled and the device get rejected and replaced through
issuing rejection memo. The packets of the devices or equipments should be collected by C for
future reference.
10. V gives final receipt to C and a copy to P.
Output : QC test certificate [Purchase order reference, Device : make, serial no., date of manufacturing,
warranty period; quantity, delivery date, GRN no., invoice no. and date]
The quality, performance and product life cycle management of biomedical devices and sensors is an
important issue in today’s healthcare service. The healthcare service provider and consumer should be
cautious of these issues while sourcing medical devices through local or global vendors. Quality control is
an important function to resist the flow of fake products in grey market of biomedical devices. The
patients may face the risk of buying old models of biomedical devices at high price. They may be
deprived of features and benefits of new models. It is basically a problem of product life-cyle
management. Many devices are imported from foreign countries a long time back; the selling agents
may try to clear old stock at high price. The quality control and invoice processing systems should verify
the make, date of manufacturing and warranty period carefully.
2.4.2 Medical Test Report
Agents : Healthcare service provider: Testing associate (T), Healthcare service consumer (C);
Input: Registration card, consultant’s prescriptions;
Protocol :

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 26
1. C shows registration card and consultant’s prescription or surgery schedule to T. T generates
testing bill; collects payment from C and gives receipt; collects test sample of C.
2. T enters test results into HIS.
3. C shows receipt to T; T gives test reports to C.
Output : Test report [ Report id, report date, request no., location, Referred by, package, specimen,
date and time of collection, result date, Test : type, test parameters, results, unit, biological reference
interval, method of testing, remarks / opinion / conclusion from test results, verified by, authorized by]
2.3 Discharge Certificate
Agents : Discharge associate (D), Healthcare service consumer (C);
Input : Registration card; Patient’s flow chart;
Protocol : C produces registration card to D. D generates discharge certificate and gives to C.
Output : Discharge certificate [ Registration no., name of patient, age, gender, location, user, date and
time; discharge summary : medical problem, reason for admission, date of surgery, operative procedure;
details of hospital stay : event during hospitalization, medication administered during hospitalization,
investigation, condition at discharge, date of discharge; Advice on discharge : serial no., medicine, form,
dose, frequency, duration, quantity, from, to, remarks; special instruction, next appointment : consultant,
location, time]
2.4 Bill and Payment Receipt
Agents: Healthcare billing associate (B), Healthcare service consumer (C);
Input : Registration card; patient’s flow chart; discharge certificate;
Protocol :
1. C produces registration card, patient’s flow chart and discharge certificate to B.
2. B generates medical bill or invoice.
3. D checks the correctness of computation and pays through cash or credit card or demand draft.
4. B generates receipt and gives to C.
Output : Discharge bill [ Patient details : registration no., name of patient, age, gender; Billing: bill no.,
service tax registration no., admission date, discharge date, location, user, date and time, serial no.,
service description, tariff, total bill amount, advance paid, patient’s due or refund; digital signature or
stamp; consolidated bill break up details : anesthesia charges, bed / stay / ambulatory service charges,
drug, non-medical items, OT store items, others, surgery charges, theatre charges]

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 27
2.5 Online Feedback Form
Agents : Patient care associate (P), Healthcare service consumer (C);
Input: Feedback form [Business functions, units, performance metrics, rating scale, questionnaires,
suggestions, patient’s information: registration no., name, phone no., e-mail id];
Protocol :
1. The patient or the attendant of the patient fills data in feedback form based on perception.
2. The system accepts data and generates feedback number.
Output : Feedback acceptance confirmation with feedback number
Critical success factors: open feedback; rational, logical and analytical thinking; understanding of the
patient on performance metrics and questions.
2.6 Patient’s Help Guide
Agents : Healthcare helpdesk associate (H), Healthcare service consumer (C);
Input : Registration card; Consulting doctor’s prescription, Patient’s flow chart;
Protocol : C produces registration card to H. H provides patient help guide, general instruction chart and
medical problem information sheet to C.
Output : Patient help guide [Location of facilities, contact phone number, e-mail, rules, service offerings,
list of consultants, tariff or service charges, patient’s rights and responsibilities]; Patient information guide
[ Medical problem, biological information, causes of problems, symptoms, treatment procedure, general
patient queries, post treatment problems]
3. Enterprise Resource Planning (ERP)
Agents : Healthcare service provider (P);
Input: Master data schema - human resource, material, healthcare service, vendor and service
consumer or patient, business rules, organization structure;
Protocol :
1. Deploy an optimal mix of ERP and SCM system modules through scope analysis, business process
re-engineering, selection of appropriate hardware, networking schema and package, master data
configuration, customization of applications, data migration and testing, training, system
monitoring and performance optimization.
2. Call ERP system : FI-CO, MM, HR, maintenance, project management and SD (optional);
3. Call SCM system :
a. Planning : demand, inventory, distribution, capacity;
b. Collaboration : sourcing, CPFR;

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 28
c. Execution: warehousing, transportation, order management and reverse logistics;
Output : Transaction processing, intelligent reports for decision making.
The business analysts have also done the requirements engineering of enterprise resource planning and
supply chain management system. The CIO would like to present these requirements to the top
management to streamline various business processes associated with the healthcare supply chain. A
supply chain is a network of organizations that satisfies the demand of ultimate customers by producing
values in the form of products and services. Supply chain management (SCM) is a novel management
paradigm; the basic objective is to improve the competitiveness of the supply chain and to fulfill ultimate
customer demands by integrating a network of organizational units through systematic coordination of
material, information and financial flows. A supply chain includes all the stages involved directly or
indirectly in a business process such as suppliers, manufacturers, distributors, retailers, healthcare service
providers and patients. Each stage performs different processes and interacts with other stages of the
supply chain; there is a flow of material, information and funds between different stages. The ultimate
objective is to maximize the value, which is measured in terms of the difference between revenue
generated from the customer and. the overall cost across the supply chain. Enterprise Resource Planning
(ERP) is a cross-functional enterprise backbone that integrates and automates many internal business
processes and information systems within the sales and distribution, production, logistics, accounting and
human resource functions of an enterprise. These have evolved considerably over fifty years as a result
of continuous improvements in business management and the development of information and
communication technologies. ERP system tries to integrate and synchronize isolated functions into
streamlined business processes. The healthcare service provider may get different types of benefits in
terms of streamlined business processes, best practices, flexible, configurable organizational structure
can be implemented in modules, global capabilities, multi-currency support and local language support.
The critical issues are consulting and implementation skill of ERP and SCM systems and version
upgradation problems.
The ERP system of healthcare service provider should have material management (MM), finance and cost
control (FICO), human resource (HR) management, maintenance and project management modules.
FICO module should be used for financial accounting, cost control, revenue management, tax
computation, budget planning and investment management for various projects. MM module should be
used for e-procurement, tendering, purchasing, inventory control, materials requirement planning (MRP),
contract negotiation, vendor selection, spend analysis, vendor rating, receiving and inspection of
healthcare products for warehousing, quality control and invoice processing. Sales and distribution (SD)
module may be used for distribution planning, order management, pricing and receivables management.
Another important module is project management which can be used for project planning, resource

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 29
allocation and monitoring functions. Maintenance module may be used for periodic and preventive
maintenance scheduling, service contracts management and spare parts management related to the
maintenance of information and communication system, biomedical instruments, civil, mechanical and
electrical infrastructure.
Web enabled ERP HR module can be effectively used for human resource management through HR
master data schema for various functions such as human resource planning (e.g. job design, organization
structure modeling), HR strategy and policy formulation (e.g. pay package, incentive, allowance, reward
like performance based bonus, provident fund and pension), efficient talent acquisition (e.g. interview
scheduling, selection, testing and recruitment), talent retention (e.g. career growth planning), HR
development (e.g. training, research and innovation), personal administration (e.g. time management,
leave management, salary processing, performance management, promotion and reward distribution,
360 degree feedback, retirement planning), outsourcing (e.g. contracts negotiation with service
providers) and employee relationship management (e.g. trade unions, negotiation, corporate culture and
communication).
An extended ERP system may be used for supply chain management (SCM). The SCM system may have
planning, collaboration and execution modules. The SCM planning module may be used for demand
planning, inventory control, distribution and capacity planning. The collaboration module may be used for
strategic sourcing and CPFR. Collaborative planning, forecasting and replenishment (CPFR) is a strategic
tool for comprehensive value chain management of a healthcare organization. This is an initiative among
all the stakeholders of the healthcare supply chain in order to improve their relationship through jointly
managed planning, process and shared information using web service. The ultimate goal is to improve a
firm’s position in the competitive market and the optimization of its own value chain in terms of optimal
inventory, improved sales, higher precision of forecast, reduced cost and improved reaction time to
customer demands. The execution module may be used for warehousing, transportation management,
reverse logistics or returns management and product life-cycle management.
2.3 Knowledge Management System (KMS)
Agents : Healthcare service provider (P);
Input : cases, globally best healthcare practice: diagnosis, surgery, drugs;
System: data warehouse, web enabled collaboration platform, intranet, extranet, e-mail, knowledge
based system (e.g. expert system), groupware, videoconferencing, medical bulletin board;
KM Mechanism:
1. Knowledge creation through socialization, externalization, internalization and combination;

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 30
2. Knowledge storage in organization memory (e.g. case base, digital library, e-books, e-papers, e-
journals, e- magazines and e-technical reports);
3. Knowledge sharing or transfer through meeting, seminar, workshop, conference and training
programs;
4. Knowledge application to support innovaton, research and development and new problem
solving;
5. Case based reasoning
6. Perception
Output : digital library, centre of excellence (CoE), case base, innovation model (K-A-B-C-D-E-T-F).
Digital transformation ensures creation, storage, transfer and application of knowledge
effectively in a healthcare organization.
The innovation cells of healthcare organization have met with the CIO, CEO, CFO and business analysts
and have analyzed various critical issues of knowledge management. They have discussed about the
need of a medical digital library which should store structural data (e.g. patient lab results and
demographic studies), multimedia data (e.g. MRI images) and free-text documents (e.g. patient reports,
medical literature, teaching files and news articles). The digital library requires efficient information
retrieval algorithms and data processing techniques to support quality decision making from a large pool
of data and to help overcoming human cognitive constraints. Medical data are often available in free text
form and the doctors require scenario specific retrieval. For example, a doctor would like to get the
output of two specific queries: (1) diagnosis scenario: diagnosis of pancreatic cancer from patient reports
and (2) treatment scenario: treatment of pancreatic cancer from the collection of medical literature.
Specific complex queries may not be processed by traditional information retrieval systems due to various
reasons such lack of indexing for representing synonyms, phrase and similar concepts in free text,
ranking the similarity of the content within the document with the query term and a method to resolve
the mismatch of the term in the query with that in the document. Medical information knowledge and
healthcare data grow at explosive rates. The basic objective of the knowledge management system is to
provide correct information from the data warehouse or case base for intelligent decision making and
improved quality of patient care.
The research, development and innovation cell have discussed on different aspects of knowledge
management and the role of information and communication technology in KM with the business analysts
and CIO. They have jointly explored knowledge management mechanisms and the related information
sytem. They feel that a knowledge management cell should be formed and it should be responsible for
defining knowledge, reengineering of KM processes and design of KMS architecture. Knowledge and
knowledge management are complex and multi-faceted abstract concepts, justified true belief. Data is

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 31
raw numbers and facts, information is processed data and knowledge is personalized authenticated
information related to facts, procedures, concepts, interpretations, ideas, observations and judgments.
Knowledge management cell focuses on exposing the workforce to potentially useful information and
facilitating assimilation of information. KMS applies information and communication technology for
knowledge management. Knowledge is considered as a significant organizational resource; the objective
of KMS is to support creation, transfer and application of knowledge in the healthcare organization. This
knowledge is embedded in and carried through multiple entities including organization culture and
identity, routines, policies, systems, documents and workforce. According to the knowledge-based view
of a firm, these knowledge assets can produce long-term sustainable competitive advantages of the
healthcare service provider.
Organizational knowledge creation involves developing new content or replacing existing content within
the knowledge base of healthcare service provider. Knowledge is created, shared, amplified, enlarged
and justified in organizational settings through social and collaborative process and individual’s cognitive
process. Knowledge may be tacit and explicit. Tacit knowledge is rooted in actions, experience, mental
models (mental map, belief, paradigm) and individual belief on cause-effect relationships. Technical tacit
knowledge is the know-how applicable to specific task such as surgery skill. The explicit dimension of
knowledge is articulated and generalized knowledge such as knowledge of medicine and healthcare
practice.
In a healthcare organization, knowledge creation can occur through socialization, externalization,
internalization and combination. Socialization is the process that transfers tacit knowledge in one person
to that in another person. It is experiential, active and knowledge extracted from internal and external
environment of the organization. Socialization is primarily a process between individuals. Externalization
is the process for making tacit knowledge explicit. One case is the articulation of one’s own tacit
knowledge like ideas or images in words, metaphors, and analogies. A second case is eliciting and
translating the tacit knowledge of others. Dialogue is an important means for both. During such face-to-
face communication people share beliefs and learn how to better articulate their thinking, though
instantaneous feedback and the simultaneous exchange of ideas. Externalization is a process among
individuals within a group. Once knowledge is explicit, it can be transferred as explicit knowledge through
a process called combination by using information and communication technology. Combination allows
knowledge transfer among groups across organizations. Internalization is the process of understanding
and absorbing explicit knowledge into tacit knowledge held by the individual. Knowledge in the tacit form
is actionable by the owner. Internalization is largely experiential in order to actualize concepts and
methods, either through the actual doing or through simulations. The internalization process transfers
organization and group explicit knowledge to the individual.
Knowledge management of healthcare service provider involves various patterns of knowledge
manipulation activities such as acquire, selection, internalize and use. Acquiring knowledge is the

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 32
identification of knowledge in the organization’s environment so that it can be internalized and used
within an organization. Knowledge selection is the activity of identifying needed knowledge within
existing knowledge resources and providing it in an appropriate representation to an activity that need it.
In a pull system, knowledge selection is triggered by a request received from a knowledge seeker. In a
push system, knowledge selection is triggered by prespecified automatic alert criteria without explicit
request from knowledge seeker. Selection involves identify, capture, organize and transfer of knowledge
through proper channels. In push based system, identification of appropriate knowledge is more active
than in pull based system. Triggering from knowledge seeker activates identification function, which
involves locating the knowledge resource, accessing knowledge quality, valuing parameters for selecting
knowledge and filtering. Capturing involves retrieval of knowledge from identified knowledge sources or
coordinated collection of knowledge from multiple resources. Once knowledge has been captured, it may
be necessary or useful to organize it prior to transfer to the knowledge seeker. Organizing captured
knowledge involves interpreting, refining, assembling, transforming and rearranging. Transfer includes
channel identification, choice of the most reliable channel, scheduling and sending. Thus, captured
knowledge is transferred to one or more knowledge seekers. Internalizing alters organizational
knowledge sources based on acquired, selected or generalized knowledge. It receives knowledge flows
from these activities and produce knowledge flows that impacts organization state of knowledge. Using
knowledge is the activity of applying existing knowledge and / or producing an externalization of
knowledge.
Organization memory system is a significant part of an organization’s knowledge resides in the minds of
the workforce. However, in the current organizational environment where downsizing, reengineering,
restructuring and high rates of organizational turnover are common, enterprises are beginning to find
that it is easy to loose a vital element of their intellectual property i.e. corporate knowledge. While
organization create knowledge and learn, they also forget. In other words, organizations are beginning to
recognise that they can suffer a failure of their collective corporate memory. Unsurprisingly, one solution
that is put forward to this problem is that of an organizational memory system. The storage, organisation
and retrieval of organizational knowledge is known as organizational memory. An organizational memory
system enables the integration of dispersed and unstructured organizational knowledge by enhancing its
access, dissemination and reuse among an organization’s members and information systems. From the
view of information technology, organizational memory means a comprehensive computer system, which
captures a company’s accumulated know-how, business activities, the related core competencies, and
other forms of knowledge assets and makes them available to enhance the efficiency of knowledge
intensive work processes. Thus, knowledge from the past experience and events influence present
organizational activities. Organisational memory includes knowledge residing in various component forms
including written documentation, structured information stored in electronic databases, codified human
knowledge stored in expert system, documented organizational procedures and processes and tacit

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 33
knowledge acquired by individuals and network of individuals. Organizational memory has both positive
and negative effects. The positive effects include standardization of business process, organizational
change management and reuse of resources avoiding waste of time and cost. The negative effects
include organizational memory may cause decision making bias, lack of innovation and creativity. It may
lead to stable consistent organizational culture which may be resistant to change.
Knowledge transfer occurs at various levels: transfer of knowledge between individuals, transfer of
knowledge from individuals to explicit sources, transfer of knowledge from individuals to groups, transfer
of knowledge between or across groups and transfer of knowledge from a group to the whole
organization. The effectiveness of knowledge transfer depends on type of knowledge, perception and
motivation of sources and receivers and the quality of transmission channel. Knowledge transfer channels
can be classified into four categories. Informal transfer channels are unscheduled meeting or gossip
during break or informal seminar may be very effective for knowledge transfer in small firms. Formal
transfer channels are seminars, corporate training programmes which ensure greater distribution of
knowledge but may affect creativity and innovativeness, Personal transfer channels are job rotation
among various groups/departments/divisions, apprenticeships and Impersonal transfer channels are
knowledge management repositories.
Source of competitive advantages resides in the application of knowledge rather than in the knowledge
itself. There are three primary mechanisms for the integration of knowledge to create organizational
capability. Directives are the set of rules, standards or instructions derived through tacit knowledge of
experts in a healthcare organization. Directives should be communicated to non-specialists for improving
their productivity. Organizational routine refers to interaction protocols and process standards that allow
individuals to apply their specialized knowledge without sharing the same to others. Self-contained task
teams are formed to solve problems ignoring directives and organization routines. Knowledge discovery is
a process that attempts to identify and interpret patterns in information that are important to perform
some task. Knowledge discovery system adds value to information by making it more accessible,
tractable and usable. The information is more accessible because improved search engines allow
knowledge discovery systems to collect pertinent information from rapidly growing databases. The
information is more tractable as the information can be displayed at the right time in a workflow or in
higher density using data visualization techniques. The information is more usable as discovered rules or
constraints can be more tightly integrated into collaborative network system.
A KMS can possess six types of knowledge in a healthcare organization: descriptive, procedural,
reasoning, linguistic, presentation and assimilative. A KMS can manage i.e. acquire, store, process and
eliminate any and all of these six types of knowledge. Descriptive knowledge or data is information about
past, present, future and hypothetical states of relevance to a decision making situation - it is concerned
with knowing what. Procedural knowledge is knowing how and specifies step-by-step procedures for
accomplishing tasks. Reasoning knowledge specifies what conclusions are valid under what

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 34
circumstances: knowing why. Presentation knowledge facilitates communication from one entity to
another. Linguistic knowledge helps in interpreting communication received. Assimilative knowledge helps
maintain a knowledge base. Knowledge based DSS can be classified into four categories: Symbiotic DSS
(SDSS), Expert DSS (EDSS), Holistic DSS (HDSS) and Adaptive DSS (ADSS).
2.4 Business Intelligence (BI) System
Agents : Analysts, Healthcare service provider (P);
Problem : Intelligent decision making in complex and rapidly changing business environment;
Business objectives: organize, automate, monitor and analyze different business processes, metrics
and systems to improve overall corporate performance; discovery of hidden intelligence from large pool
of data;
BI system components: data warehouse, data mining, web mining, performance scorecard, analytics,
data visualization techniques;
Input: Transactional data associated with registration, consulting, testing, surgery, discharge, billing and
payment processing, supply chain management, project management, maintenance;
Strategic moves:
1. Strategize : Where does P want to go?
2. Plan : How does P get there?
3. Monitor: What is P doing to achieve specific business objectives subject to different constraints?
4. Act and adjust : What does P need to do differently?
5. Call balance scorecard or six sigma or dash board or business activity monitoring; use analytics in
medical testing through intelligent data visualization techniques.
6. Competencies : data governance, analytical tools and skills and data oriented culture;
Algorithm:
1. Identify a set of functions and critical performance metrics or parameters for each function.
Define a or a set of simple questions related to each performance metric with weight.
2. Select a simple rating scale for each performance metric: [e.g. 1-5; Excellent (5), Good(4),
neither good nor bad (3), Fair (2), Poor (1)]
3. Identify a group of innovative, skilled, knowledgeable and experienced raters; the raters should
observe the systems and give rating to various performance parameters independently and
freely through a true, unbiased feedback system. Compute aggregate score.
4. The raters should analyze as-is system, find out gap and design to-be systems through logical
suggestions and recommendations.
Output: Performance scorecard, alert, dash board, knowledge discovery from data, test reports;

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 35
The CIO scheduled an workshop to explore the scope of business intelligence system and analytics for
digital transformation of the healthcare organization. The business analysts, system administrator, CEO,
CFO and the analytics consultants were invited to the workshop. The CIO fixed a set of critical agenda for
the discussion in the workshop. Why should the healthcare service provider use analytics? What are the
areas of focus? What are the competencies and capabilities essential for analytics? What are the risks,
complexities, challenges and best practices?
Descriptive, predictive and prescriptive analytics perform intelligent data analysis through applied
statistics, data mining algorithms and quantitative models for intelligent decision making, planning,
strategy formulation, performance measurement and learning. The healthcare service provider should use
analytics as a strategic tool instead of a supporting one for digital transformation. In an uncertain and
competitive business environment, the healthcare service provider can use analytics for various business
functions such as human resource management, strategic management, customer relationship
management, supply chain optimization, streamlining operations, pricing, financial forecasting, risk
management and budget allocation. The provider may adopt binning as an advanced analytic technique
that analyzes the response of all patients to a set of direct questions related to specific domains.
Responses are then categorized into bias and corrective actions are taken to improve the quality of
service.
The digital transformation requires key competencies such as data governance, analytical tools and skills
and data oriented corporate culture for improving competitiveness and business performance of the
healthcare service provider. Data governance requires capabilities in terms of correct data model and
standardized data management practice. Analytical tools and skills require the appointment of
knowledgable and innovative data analysts, selection of good BI software package, efficient ETL
algorithms, analytical modeling tools and intelligent data visualization techniques. Data driven culture
requires the support of top management, high commitment and innovation in leadership; it considers
analytics as an important asset. The service provider can select any of the two alternative options.
Analytics may be used for specific performance metrics for a specialized path. Along the collaborative
path, analytics is used to achieve the business objectives of the enterprise through an information
platform which enables insights to be developed and shared across different business units. The
participants of the workshop have concluded that the healthcare service provider requires right focus,
proper resource allocation, right people, sophisticated technology and right culture as sources of
competitive strength.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 36
2.5 Biomedical System
Digital transformation requires the intelligence of biomedical engineering, bio-sensors, bio-
inspired artificial intelligence and human computer interaction for improved QoS in patient
care.
The CIO has decided that the healthcare information system of P should be integrated with bio-medical
system appropriately through sensors, robotics, human computer interaction, mobile communication
system and internet. An effective digital transformation enables the service provider to offer different
innovative patient care services through medical imaging systems, digital radiography, computed
tomography, nuclear medicine, computer-integrated interventional medicine, ultrasonic imaging,
magnetic resonance imaging, diffuse optical imaging, image compression, medical image retrieval,
parametric imaging, brain magnetic resonance imaging, molecular imaging, data processing and analysis
by electronic medical record (EMR), image registration, biological computing, picture archiving, medical
imaging informatics, digital library, integrated multimedia patient record systems, computer-aided
diagnosis and clinical decision support system.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 37
Chapter 3: Computing Schema & Computational
Intelligence Digital transformation of healthcare system demands the computational intelligence of distributed
computing (e.g. cloud computing, service oriented computing), secure multi-party computation (e.g.
fairness, correctness and privacy), embedded computing and artificial intelligence (e.g. robotics, case
based reasoning, computational theory of perception and soft computing) for intelligent decision making,
fast and correct transaction processing, knowledge management, enterprise resource planning, supply
chain management, complex surgical operations and medical diagnosis. This section explores the
computational intelligence through a set of algorithms, protocols, mechanisms, heuristics and quantitative
models. These are closely associated with data, networking, application and security schema of
healthcare information system. Computational intelligence are essential for data processing and
structuring, pattern recognition, knowledge representation, knowledge processing, learning, knowledge
aggregation, knowledge discovery, reasoning, decision making, predictive actions, adaptation and
evolution, behavior patterns generation, expert advising, planning, and proactive reasoning in medical
science and healthcare domain. The computational intelligence is a critical issue in healthcare domain due
to several factors such as complexity of data structure, reasoning methods, domain specific and
interdisciplinary knowledge, wide verities of diseases and medical treatment procedures, increasing
population and old aged people.
3.1 Distributed computing
Distributed computing considers the scenario where a number of distinct, yet connected computing
agents wish to execute a joint computation. The objective is to enable these agents to carry out such
distributed computing tasks privately. The advancement of computer network technologies, multi-agent
system and cryptography has improved the efficiency of distributed computing significantly. There exist a
set of standards (e.g. HIPAA, EDI, HL-7, DICOM, IEEE 11073, ICD-9 and CPT) related to health
information systems and the electronic exchange of private transactional data among the stakeholder of
the health chain such as patients and service providers. The standards allow the exchange of complete,
timely and correct data among different tiers of the chain in an effective and efficient way through a fully
integrated information and communication technology infrastructure. This section explores the scope of
cloud computing and service oriented computing for healthcare service.
The CIO has called the system administrator, system analysts and a cloud computing service provider to
discuss some critical issues such as why the healthcare industry should adopt cloud computing
technology, what are the expected benefits and how to compete more effectively. The healthcare

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 38
industry is facing different problems such as cost reduction associated with information and
communication technology infrastructure, maintenance and operations; fast and correct transaction
processing and data sharing for patient care, supply chain coordination and regulatory compliance. Many
healthcare organizations find it harder to stay in compliance with regulations by using old legacy
technology. Large organizations would like to consolidate their IT infrastructure which is spread across
multiple geographic regions. Small firms are trying to use information and communication technology at
fair price. Another important issue is security and privacy of critical patient data which should be stored in
encrypted form in the data warehouse. The service provider often faces the problems of availability and
continuity of service against natural disaster, communication link failure and shortage of power.
3.2 Cloud Computing Schema
With the significant advancement of information and communication technology, computing is perceived
to be used as the next utility after water, electricity, gas and telecommunication. The concept can be
extended to cloud computing and grid computing for a market oriented grid. Utility computing is
associated with a parallel and distributed system that enables the sharing, selection and aggregation of
geographically distributed autonomous computational resources dynamically at runtime depending on
their availability, capability, performance, cost and quality through web service. The computational
resources include different types of sophisticated software applications such as data mining, scientific
computing and image processing, data, CPU or processing power, servers, storage devices, scanners,
UPS and network interfaces which can be shared through web service. The objective of utility computing
is to provide computing power and storage capacity that can be used and reallocated for any application
and billed on a pay-per-use basis. Utility computing consists of a virtualized pool of information systems
and other IT resources that can be continually reallocated to meet changing business and service needs
of the consumers. These resources can be located anywhere and managed internally or externally. The
service provider tracks the usage of computational resources of the consumers and makes invoice based
on predefined price setting and usage data. An efficient resource management system coordinates and
monitors the complex operation.
Utility computing supports virtualization. Cloud computing is basically a distributed computing where
dynamically scalable and virtualized resources are provided as a service over the internet to achieve cost
saving, easy scalability and high availability. The services offered through cloud computing usually include
Software-as-a-Service (SaaS), Infrastructure-as-a-service (IaaS), Platform-as-a-service (PaaS), data-
Storage-as-a-Service (dSaaS) and database-as-a-service (DaaS). SaaS allows users to run applications
remotely from the cloud. IaaS provides a set of computing resources as a service which includes
virtualized computers with guaranteed processing power and reserved bandwidth for storage and
Internet access. PaaS includes operating systems and required services for particular applications along

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 39
with data security, backup and recovery, application hosting and scalable architecture. dSaaS provides
data storage, data warehousing and data mining facilities. This is a cost effective, innovative IT
infrastructure from which the consumers are able to access desired computational resources and from
anywhere in the world on demand.
The key technologies that enable cloud computing are virtualization, web service, service oriented
architecture, service flows and work flows. The trading in cloud computing depends on several
technological issues such as high availability of service, business continuity, data lock-in, security and
privacy of data, efficient data transfer, performance predictability, scalable storage, efficient bugs
management in large distributed system, adaptive scaling of operation, innovative software licensing and
reputation mechanisms. Strategic pricing considers all these QoS factors to define optimal price setting
for cloud computing. In fact, an intelligent, innovative competitive pricing mechanism and secured high
QoS can make cloud computing an attractive IT business model as compared to traditional corporate
computing model based on direct IT investment. Nowadays, pay-for-use or pay-as-you-go licensing are
becoming popular in cloud computing market. Thus, the computing world is rapidly transforming towards
developing information systems to be consumed as a service. Various service providers have started to
build scalable data centers at various locations for hosting cloud computing.
The key players of the market of cloud computing are a set of service providers, service consumers and
resource brokers. There are several challenges of trading in cloud computing : fair resource allocation
protocols, optimal task scheduling, tendering, contract net protocols, auction, market clearing and
negotiation mechanisms and pricing algorithms. The major threats are reduced contract duration,
uncertainty, risk and variable duration of a portfolio of contracts, reduced switching costs and customer
lock-in, uncertain customer demand, short life-cycle and high sunk cost. Cloud computing may require
high development cost for instrumentation, provisioning and monitoring and start up costs in the face of
uncertain demand. The cloud service provider shows the following computing schema to the CIO, system
administrator and system analysts to explore the scope of cloud computing.
Cloud Computing Schema:
Agents: Cloud computing service provider (Pcc), cloud computing service consumer i.e. healthcare
service provider (Ph);
Application domain: electronic medical records [EMR], office productivity, health information
exchange, physician collaboration solutions, clinical information systems, medical interfaces;
Input: Demand plan of Ph, Service plans of Pcc ;
Mechanism: Ph and Pcc negotiate and select an optimal mix of public or private or hybrid cloud
computing services.
SaaS (Software-as-a-Service)
dSaaS (Data storage-as-a-Service)
DaaS (Database-as-a-Service)

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 40
IaaS (Infrastructure-as-a-Service) and HaaS (Hardware-as-a-Service)
PaaS (Platform-as-a-Service)
CaaS (Communication-as-a-Service)
Revelation principle : Ph and Pcc jointly preserve the privacy of data and cloud computing system.
Payment function: Pcc pays Ph based on negotiated pricing plan and service consumed for a specific
period i.e. pay-as-you-go scheme.
Output : Cloud computing service plan, pricing plan.
The healthcare service provider (Ph) can use cloud based electronic medical records (EMR) solutions. The
primary benefits are reduced implementation time, lower initial costs instead of significant IT investments
on in-house technology evaluation and testing, partnership of compliance, better scalability and cost
control. Ph can also use cloud based secure office collaboration platform, electronic mail, file, spread
sheets and document sharing solutions, unified communication services including telephone, e-mail,
instant messaging, audio and video conferencing and miscellaneous cutting edge technologies to improve
productivity in healthcare operations. Different stakeholders of the healthcare chain can share critical and
strategic information through Health Information Exchange (HIE). Physician Collaboration Solutions
(PCS), m-health and e-health enable virtual patient care and telemedicines system for rural healthcare.
Cloud based clinical information systems may be used for efficient and fast workflow control,
appointment and surgery scheduling, testing, retrieval of patient’s information, procurement of drugs and
medical devices, billing and payment processing. Both small and large healthcare organizations are able
to use cutting edge technologies at reduced investment on information and communication technology.
The cloud computing schema can support the transition from the design of large scale medical
instrumentation to smart micro system technologies in the form of intelligent Hardware-as-a-Service
(HaaS), the transition from large telecommunication infrastructures to mobile data transfer in the form of
Infrastructure-as-a-Service (IaaS), the transition from isolated islands of medical data towards integrated
end-to-end cloud solutions in the form of Software-as-a-Service (SaaS) and the transition from intrusive
and expensive testing to harmless indirect health monitoring through novel devices in the form of user
Interface-as-a-Service (UIaaS). The patients or healthcare service consumers can receive innovative
healthcare services such as mobile electrocardiogram (ECG) recording, portable defibrillators, digital
stethoscopes and emerging medical peripheries based on multimodal data fusion through cloud
compatible novel medical interfaces.
Ph can adopt either cloud computing schema or go for direct IT investment. Cloud computing is a unique,
cost effective, differentiated business model. It makes the healthcare service provider agile and flexible to
the basic needs. Pay-for-what-happens is a flexible IT pricing strategy; Ph can pay per user per month on
any application as a service. It should not throw anything away; rather it should build on existing IT
assets and choose a hybrid model of on-premises and off-premises resources. There are different options

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 41
of cloud computing such as public, private and hybrid cloud. The computing resources are dynamically
provisioned over web via web applications or web services from an off-site third party service provider in
public cloud computing. In case of private cloud computing, private networks are used to provide full
control over data, security and quality of service by a cloud service provider or a company’s own IT
division. A hybrid cloud environment combines private and public cloud models.
dSaaS / DaaS : The basic objective of DaaS is to avoid the complexity and cost of running a database
with improved availability, performance, price and flexibility. It gives the access to various types business
intelligence solutions (through web) which include distributed database, data warehousing, data mining,
business and web analytics, data visualization and business performance measurement applications. The
pricing of dSaaS is based on the cost of hardware (e.g. data warehouse, servers), the cost of software
(e.g. business intelligence solutions) and system administration cost (e.g. data centre administration,
data base security, backup, recovery and maintenance). A consumer can lease a data storage space
where it is required to measure different system parameters such as stored data (GB/month) and number
of processed queries (per 10k requests / month) to compute the price of dSaaS / DaaS. The provider can
offer quantity discount in case of group buying of storage space. The prices of DaaS / dSaaS are also
determined by various QoS parameters such as connection speed, data store delete time, data store read
time, deployment latency (i.e. the amount of latency between when an application is posted and ready to
use) and lag time (how slow the system is).
The pricing of dSaaS is also governed by the security and privacy of data and the related system
architecture. A complex system architecture enhances the cost of computation and communication
among the agents and also the cost of energy. There may be different types of system architecture
possible in cloud computing. In a simple setting, the service consumer encrypts its data and stores in the
data storage server of the service provider. Whenever required, the consumer gets access its data
through proper access control schema and decrypts the data. In a slightly complex setting; the service
consumer stores its encrypted data in the server of the service provider and wants to share data with a
client. In this case, the service provider uses a data processor, data verifier and tocken generator for
dSaaS service. The service consumer perform data indexing with the support of the data processor,
encrypts the data and sends to the cloud server. The client requests the service consumer for a specific
query on stored data. The consumer sends a credential and tocken to the client. The client sends the
tocken to the service provider. The provider finds the appropriate encrypted data with the help of the
tocken and returns the same to the client. The client and the consumer jointly check the integrity of data
using verification mechanism. So, the costs of computation and communication are different in simple
and complex cloud computing settings. The pricing of dSaaS should consider these issues intelligently.
Some applications (e.g. education sector) require low level of privacy of data. Some applications (e.g.
financial service, healthcare etc.) need high level of security and privacy in data outsourcing and this

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 42
involves high cost of computation and communication from the perspectives of statistical disclosure
control, private data analysis, privacy preserving data mining, intelligent access control and query
processing on encrypted data. The service provider should define a discriminatory pricing mechanism for
dSaaS: high level of security and privacy of data demands high price and low level of security asks low
price.
The price of dSaaS is a function of miscellaneous cost elements of a data center. A data centre or data
bank is the collection of servers where the applications and data are stored. Data center consists of a set
of servers and network architecture. The servers store the data from different organizations and network
architecture facilitates the services to use, store, and update the data of the servers. The cost of
administration of data centre includes several factors: initial development cost, operating cost,
maintenance cost and cost associated with disaster recovery plan. The development cost includes the
cost that requires making master plan, building infrastructure, buying hardware and software, making
database and security schema. Operating cost includes the cost of energy, cooling system, system
administrators, software license and network cost. Maintenance cost is the cost of maintaining the system
which includes upgradation of hardware and software. One of the most challenging issues of data center
management is the resource allocation strategy: how it is possible to cater the demand of the service
consumers using minimum number of servers. It has an impact on the size, complexity and cost of data
center. The data centre administrator can follow dedicated or shared server allocation strategy.
The price of dSaaS is also a function of energy consumption of cloud computing system in a data center.
There are many open challenges of energy efficient design of computing systems and green IT covering
the hardware, operating system, virtualization and data center levels [22]. The basic objective of the
cloud computing system design has been shifted to power and energy efficiency to improve the profit of
the service provider. Energy consumption is not only determined by hardware efficiency, but it is also
dependent on the resource management system deployed on the infrastructure and the efficiency of
applications running in the system. Solar power electronics is an interesting option of green IT. Higher
power consumption results not only high energy cost but also increases the cost of cooling system and
power delivery infrastructure including UPS and power distribution units / panels. The consolidation of IT
infrastructure should be done intelligently to reduce both energy consumption and performance
degradation through improved power management. Energy consumption can be reduced by increasing
the resource utilization and use of energy efficient cloud computing system.
Software-as-a-Service (SaaS) : SaaS is an application hosted on a remote server and accessed
through web; it can be business service or customer oriented service. The basic objective is to reduce
software licensing cost and improve productivity by using sophisticated applications. The pricing strategy
of SaaS is based on pay-as-you-go basis; not dependent on number of licensing period and licensing
users as in case of direct software procurement. The service provider can configure the number of

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 43
required features of a software as per the demand of a service consumer and price SaaS service charge
accordingly based on basic, medium and mega package configuration. Another concept is software plus
service where an enterprise uses a locally hosted software application and additionally uses SaaS through
cloud for a specific type of application. Using the existing software paradigm, the consumer purchases a
software package and license by paying a one-time fee. The software then becomes the property of the
consumer. Support and updates are provided by the vendor under the terms of the license agreement.
This can be costly if the user is installing a new application on hundreds or thousands of computers.
SaaS, on the other hand, has no licensing. Rather than buying the application, the consumer pay for it
through the use of a subscription based on number of concurrent users and only pay for what is used.
The computation of subscription fee can be stochastic pricing or simple cost based pricing. The price of
SaaS depends on the specific business model of the service provider. Suppose, a service provider
develops in-house software products. Another service provider buys COTS from third-party vendor based
on number of licensed users and licensing period and provides SaaS to the consumers. There may be
restriction of number of concurrent users and different subscription rate of SaaS in second case.
This pricing strategy should also consider cost of upgrading software application; the provider may offer
incentive for upgrading applications. In case of security software pricing, there may be different
alternative strategies to manage network security: (i) consumer self-patching where no external
incentives are provided for patching or purchasing, (ii) mandatory patching, (ii) patching rebate and (iv)
usage tax. For proprietary software, when the software security risk and the patching costs are high, a
patching rebate dominates the other strategies. When the patching cost or the security risk is low, self-
patching is the best option.
Stochastic risk based pricing mechanism considers several risk factors and optimizes the expected net
present value of revenue subject to maximum acceptable risk of the provider. In this case, the service
provider does not give much focus on cost accounting model or profit margin but tests the price
sensitivity of the customers experimentally or through trial and error method. The provider does not have
any precise perception about the demand of the new software products. But, it follows dynamic risk
based pricing based on assessed risks and competitive intelligence. For in-house software development,
software cost is a function of efforts on feasibility study, requirement analysis, system design, program
design, coding, testing and modification following waterfall / v-process / spiral / proto-typing /
incremental delivery model. The service provider estimates effort for a specific SDLC model and then
selects an optimal profit margin.
Infrastructure-as-a-Service (IaaS) : A cloud computing infrastructure consists of different types of
elements: clients (e.g. mobile, PDA, laptop, thin and thick), the data center and distributed servers. Thin
clients are less costly than thick clients. A growing trend in the cloud computing is virtualization of
servers. In a virtualized environment, applications run on a server and are displayed on the client. The

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 44
server can be local or on the other side of the cloud. Software can be installed allowing multiple instances
of virtual servers which run on a physical server. Full virtualization is a technique in which a complete
installation of one machine is run on another. It allows the running of different and unique operating
systems. Hardware-as-a-Service (HaaS) simply offers the hardware required by a consumer. Cloud
computing is a business model of delivering IT resources and applications as services accessible remotely
over the Internet rather than locally. IaaS supports remote access of computer infrastructure as a
service.
Cloud computing supports elastically scaling computation to match time varying demand. But, the
uncertainty of variable loads necessitate the use of margins i.e. the servers that must be kept active to
absorb unpredictable potential load surges which can be a significant fraction of overall cost. The
provider should not adopt a fixed margin strategy; the margin should be load dependent. The margin
required at low loads may be higher than the margin required at high loads. Secondly, the tolerance i.e.
the fraction of time when the response time target may be violated need not be uniform across all load
levels. It is really challenging to achieve optimal margin cost while guarantying desired response time for
IaaS.
The pricing strategy of IaaS is based on the cost of servers, storage space, network equipment and
system software like operating systems and database systems. The price of IaaS is basically a
subscription fee for a specific timeline. Now the question is how to compute this subscription fee. The
rate should be fixed based on the cost of hardware and software, target revenue and profit margin. The
service provider may adopt a profit maximizing pricing strategy or revenue maximizing pricing strategy
within reasonable, stable target profit margin. The profit margin is a dynamic variable; it should be set
intelligently according to competitive intelligence and quality of service. The quality of service is
measured in terms of computing time. For small firm or individual service consumer, the provider can set
a fixed price per unit time; there may be SLA but there is no scope of negotiation of price. Large PSU can
negotiate with the service provider to set a rational price for fixed timeline.
Incentive compatibility plays a significant role in IaaS pricing, it is important to analyze the significance of
incentives for network infrastructure investment under different pricing strategies: congestion based
negative externality pricing and the flat rate pricing]. A lack of proper infrastructure investment incentive
may lead to an environment where network growth may not keep pace with the service requirements. It
is really complex to compute maximum capacity that IaaS provider will be willing to invest under different
pricing schemes. Optimal capacity of IaaS is determined by different factors: per unit cost of capacity of
network resources, average value of the user’s requests, average value of the user’s tolerance for delay
and the level of exogenous demand for the services on the network. It is hard to determine whether time
based pricing is more profitable than flat rate pricing. IaaS consumers always try to identify whether
average stream of the net benefits realized under congestion based pricing is higher than the average net
benefits under flat rate pricing. IaaS provider may adopt different types of pricing strategies at different

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 45
points of time but the service consumers may control their demand of IaaS service adaptively to avoid
the increase in cost.
Platform-as-a-Service (PaaS) : PaaS supplies all the resources required to build applications and
services completely from the web without any download or installation of any software in the clients. The
price of PaaS can be negotiated for a specific project. There can be different types of project
environments such as application-delivery-only-environment (e.g. security and on demand scalability),
standalone environment and add-on-developmental-environment (e.g. subscriptions of add-on SaaS
application are bought). The price of system software can be charged as a subscription fee based on
number of concurrent users and usage period. The pricing of PaaS is also governed by the complexity of
platform services which may include application design, development, testing, deployment, hosting,
geographically dispersed team collaboration, web service integration, database integration, security,
scalability, storage, state management and versioning. The developers, project managers, and testers
can access the development and testing softwares of the service provider through web; but, lack of
interoperability and portability may be a critical issue in PaaS. The price of PaaS is determined by the
complexity of interoperability between the systems of the service provider and service consumer.
Communication-as-a-service (CaaS) : For CaaS, the a service provider can adopt service or traffic
pricing strategy and can offer several options to the consumers for voice calls, text messages, multi-
media messages, mobile internet and smart phone applications. For CaaS, the service provider may adopt
fixed up to pricing : a fixed fee p, a free call time allowance of n units and over limit rate r i.e. charge p
for usage upto n units and bill r for usage over n units. In case of traffic pricing, the service provider
simply prices the traffic consumed and each consumer has the right to allocate the purchased traffic
among various types of services according to individual preferences. The provider designs only a single
price schedule to price the traffic consumption; each plan in the schedule provides a certain level of
traffic usage for a specific price setting. Traffic pricing is a specific case of quasi bundling. Bundling of
services may increase the profit of the service provider when the service consumers have different
valuations for individual goods but similar valuations for a bundle of services. Though the service provider
chooses the bundle composition, each consumer chooses individual traffic allocation in case of traffic
pricing.
The consumer of cloud computing service can reduce IT maintenance cost significantly and can always
use the latest software applications with the cloud without worrying about upgrades and patches. It can
reduce the training cost using the skill, product knowledge and experience of the cloud service providers.
It can build a real-time enterprise model with the help of an enterprise ready cloud computing
infrastructure through a well-defined SLA and 24/7 support. The service consumer uses resources more

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 46
effectively; a service consumer can identify areas that can be moved to the cloud and quickly free up
skilled IT staff on high value initiatives. It can lower operating costs in terms of IT infrastructure,
maintenance and operational costs. It can stay secure and store sensitive data on a global network of
sophisticated data centers. Further, it can develop IT solutions faster with the support of the service
provider’s platform and interoperability support of third party solutions.
Cloud computing is particularly a desirable option for small to medium sized business wherein in-house
development and operations of IT applications may be time consuming and expensive. Small or medium
sized enterprises are best served by cloud computing within small IT budget. Large enterprises may
select cloud computing as a suitable option when they want to experiment with new information
technologies without high initial investment. It helps improve productivity by providing new machines and
instant access to new resources and software; it builds an adaptive enterprise model in a changing
business environment. The overall business competitiveness can be strengthened by reducing the time of
deployment and enhancing the ability to adapt to changing market conditions. The new paradigm of
cloud computing provides different types of benefits but there are still a number of challenges such as
performance for intensive transaction and data oriented applications, security and privacy, control over IT
platform, bandwidth costs and reliability of service.
3.3 Artificial intelligence
Soft computing is a consortium of methodologies including fuzzy sets, neural networks, genetic
algorithms and rough sets that works synergistically and provides flexible information processing
capability for handling ambiguous situations in healthcare domain. The basic objective is to exploit the
tolerance for imprecision, uncertainty, approximate reasoning, and partial truth in tractable, robust and
low-cost solutions. This technique is widely used for data mining and KDD applications. Fuzzy sets deal
with uncertainty. Neural networks and rough sets are used for classification, prediction, clustering and
rule generation. Genetic algorithms (GAs) are used for optimization and search processes. The other
approaches are case based reasoning, perception and decision trees. Fuzzy sets are suitable for handling
incomplete and noisy data and pattern, mixed information, human interaction and can generate
approximate solutions faster. Neural networks are nonparametric, robust and exhibit good learning and
generalization capabilities for intelligent data processing. Genetic algorithms provide efficient search
algorithms to select a model from mixed data based on preference criterion/objective function. Rough
sets are suitable for handling different types of uncertainty in data.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 47
Figure 4 : Computing schema for soft computing
3.3.1 Case based reasoning
The CIO, system analysts and business analysts have been exploring the computing schema of
knowledge management system based on artificial intelligence. A significant part of an organization’s
knowledge resides in its memory. While a healthcare organization creates knowledge and learns, it also
forgets. It can suffer a failure of collective corporate memory. The storage, organization and retrieval of
knowledge is known as organizational memory. In healthcare management, this knowledge can be
classified as declarative, procedural, causal, conditional and relational - what drug is appropriate for an
illness, how the drug works, why the drug works, when the drug works and how a drug interacts with
other drugs. An organizational memory system enables the integration of dispersed and unstructured
knowledge by enhancing its access, dissemination and reuse among the authorized entities.
Organizational memory is a comprehensive information system that captures accumulated know-how,
business activities, core competencies and other assets and makes them available to enhance the
efficiency of knowledge intensive business processes in healthcare management. Knowledge from the
past cases, experience and events can influence present activities and solution methodologies. Case
based reasoning can be the basic building block of healthcare knowledge management system. It
standardizes a set of processes, methods and best practices and saves time and cost in knowledge
management. But, it may cause decision making bias and may affect innovation and creativity.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 48
Case based reasoning (CBR) is a methodology for solving problems by utilizing previous experience. It
involves retaining a memory of previous healthcare problems and their solutions and solving new
problems by referencing the past cases. A healthcare expert presents a new query case to the
recommender system. The recommender system searches its memory of past cases stored in case base
and attempts to find a case that has the same problem specification of the current case. If the system
does not find an identical case in its case base, it will attempt to find the case or cases that match most
closely to the current query case. There are two different types of search such as similarity search and
neighborhood search. In case of similarity search, the solution of the retrieved case is directly used for
the current problem. The system adapts the retrieved cases if the retrieved case is not identical to the
current case. In a complex search, the system requires the access of multiple case bases which are
located at various locations. This collaborative information seeking requires a web service enabled
platform for complex search.
Case based reasoning mechanism
Agents : Healthcare consultant (Ph);
Input: New case or query (q) regarding a patient;
Protocol:
Retrieve the most similar cases (c1,…,ck) k nearest neighbors w.r.t. q from the case base;
Adapt the proposed solutions to a solution s(q) compute s(q) by combining the solutions sj of the
cases cj. sj is weighted as per the differences between cj and q;
Learn after applying s(q) to q in reality Store the new solution in the case base for solving q’.
Evaluate performance : Rejection ratio = no. of unanswered queries / total no. of queries.
Output: Recommended solution;
CBR is selected for the proposed healthcare recommender system due to various reasons. The healthcare
domain has an underlying model, the process is not random and the factors leading to the success or
failure of a solution can be captured in a structured way. Cases recur in healthcare domain though there
may be exceptions and novel cases. Healthcare solutions can be improved through case retrieval and
case adaptation. Relevant healthcare cases are available at different healthcare institutes; it is possible to
obtain right data. Case retrieval is the process of finding within the case base those cases that are the
closest to the current case. There must be criteria that determine how a case is evaluated to be
appropriate for retrieval and a mechanism to control how the case base is searched. Most often, an
entire case is searched. But, partial search is also possible if no full case exists.
Case retrieval mechanism

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 49
Agents: Decision-making agents (DMAs), mediator (M);
Input : Query case (q);
Output: Retrieved cases s(q);
1. DMAs define the query case and inform the same to M. M requests DMAs to specify their preferential
parameters.
2. DMAs negotiate with each other and define aspiration point (pa), reservation point (pr), indifference
threshold (ith), strong preference threshold (st), weak preference threshold (wt) and veto threshold
(vt). DMAs communicate this to M.
3. Repeat until DMAs are satisfied with a solution or concludes that no compromise point exists for the
query case.
3.1 M retrieves a set of cases from the case base: the most similar case to the query case and its
characteristics neighbors. M sends the search results to DMAs.
3.2 If the retrieved cases are acceptable to DMAs, the search process stops.
Otherwise DMAs refine their preferential parameters; go to step 3.1.
A case is a record of a previous experience or problem in terms of problem definition, patient’s
symptoms, drugs, solution methodology, test results and recommendations. A case base also stores
global best practices, standards, valid drugs, price and contacts of specialists. Data is stored based on
domain knowledge and objectives of the reasoning system. The cases should be stored in a structured
way to facilitate the retrieval of appropriate case when queried. It can be a flat or hierarchical structure.
Case indexing assign indices to the cases for retrieval and comparisons. There are different approaches of
case retrieval. In case of nearest neighbor search, the case retrieved is chosen when the weighted sum
of the features that match the query case is greater than the other cases in the case base. A case that
matches the query case on n number of features is retrieved rather than a case which matches on k
number of features where k < n; different features may be assigned with different weights. Inductive
approach is driven by a reduced search space and requires reduced search time. This results reduced
search time for the queries. Knowledge based approaches select an optimal set of features of case by
using domain knowledge. The complexity of case retrieval depends on multiple factors: (a) number of
cases to be searched, (b) domain knowledge, (c) estimation of the weights for different features and (d)
case indexing strategy.
The mediator agent searches for a set of cases similar to the query case on the basis of the specifications
of the query case and the preferential parameters as defined by the decision making agents. Aspiration
point is the value of an attribute which is desirable or satisfactory to the DMAs. Reservation point is the
value of an attribute that the DMAs like to avoid. DMAs inform the mediator agent regarding various
preference thresholds in order to compare alternative cases. There is an interval of preference wherein it
is not possible for the DMAs to distinguish between different alternatives due to imprecision and

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 50
uncertainty of measurements of various attributes. This is indifference threshold. Strong preference
threshold is defined as minimal change of any attribute that makes the new alternative case strictly
preferred with respect to a set of attributes. There exists an intermediate region between indifference
and strong preference threshold where the decision-making agent hesitates to compare alternatives. It is
weak preference threshold. Veto threshold indicates what is the minimal change of any attribute that
makes the new alternative unacceptable regardless of the value of other attributes. The mediator tries to
explore the most similar case with respect to the query case and also a set of cases within the
neighborhood of the most similar case. The neighborhood is defined by a set of cases that are not worse
than the middle point. These cases indicate to what extent the values of particular attributes can be
possible with respect to the most similar case.
Case adaptation is the process of translating the retrieved solution appropriate for the current problem; it
adds intelligence to the recommendation process. There are various approaches of case adaptation. The
retrieved case can be directly used as a solution to the current problem without any modification.
Otherwise, the retrieved solution should be modified according to the current problem. The steps or
processes of the previous solution can be reused or modified. The solution of the current case can be
derived by combining knowledge of multiple retrieved cases. Case adaptation is a complex decision
making task, it considers multiple factors: how close is the retrieved case to the query case? How many
parameters are different between the retrieved and the query case? DMAs can apply common sense or a
set of rules or heuristics for case adaptation.
Case adaptation mechanism
input: Retrieved case(s), Query case;
output: Recommended solution;
1. Cosense : DMAs view the complete information path, unified chronological ordering of all the events
of the search process and try to make sense of the search results.
1.1 DMAs view the sense making trajectories of other agents. A DMA may hand-off the sense making
task to an expert if it is difficult to understand the search results.
1.2 DMAs share relevant information and negotiate to reach an agreement.
1.3 DMAs verify whether the solution of the retrieved case can be applied to the current case
directly.
1.4 DMAs analyze the gaps between the query case and the retrieved case(s) and sense the need of
appropriate modifications by assessing risks, threats and opportunities of the current problem.
2. DMAs decide how to respond to the change and finally recommend the solution of the current case
rationally.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 51
Making sense of the information found during an investigational web search is a complex task of case
based reasoning. Sense making is to find meaning in a situation, it is the cognitive act of understanding
information. The system should support collaborative information search by providing several rich and
interactive views of the search activities of a group. One of the problems facing HCI research today is the
design of computer interfaces to enable sense making of the processed information. Sense making is not
only important for individuals, but also for groups to achieve shared goals. Traditional sense making tools
focus on data mining, provide better information representation, visualization and organization of search
results. But, it is also required to support the collaboration and communication that occurs among the
investigators when they make sense of information together.
Figure 5: Healthcare recommender system
Soft computing tools like artificial neural network (ANN) and memory based reasoning can be used as the
computational components of the proposed healthcare recommender system (Figure 5). In this scheme,
prediction query manager (PQM) receives new query request and consults with ANN and MBR
concurrently. When both predictors agree in prediction value, PQM normally returns the predicted value.
When the predictions of ANN and MBR are significantly different, PQM reports failure and asks for the
opinion of human experts. ANN is trained with the given data set or cases stored in the case base. The
feature weights are calculated. When a new query comes in, k nearest neighbors are retrieved from the
case base based on the feature weight sets. The prediction value of ANN is utilized in conjunction with
the prediction of MBR system. ANN predicts on the basis of trained data and test data. MBR predicts the
Training algorithm
Best practices
Case retrieval
Initial training data
Predicted value k-most similar
casesFeatureweights
Online learning
Case maintenance
Old Cases
Healthcare Case Base
Knowledge creation
Artificial neuralnetwork
Memory based reasoning
Case adaptation
New query
New cases
Healthcare expert
Prediction manager

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 52
solution based on k-nearest neighbor cases. This provides extended information for the query with most
similar cases in the case base.
K-Nearest-Neighbors (KNN) Algorithm
Input : Training objects :D; Test object: Z (a vector of attribute values);
L : Set of classes to label the objects; output: cz L where cz is the class of z;
Algorithm:
for each object y D do
compute d(z,y), the distance between y and z;
end
select ND, k closest training objects for z;
cz = argmax v L ∑yN I(v = class (cy));
where I(.) is an indicator function that returns the value 1 if its argument is true and 0 otherwise.
d(x,y) = √nk=1 (xk – yk)
2 i.e. eucledian distance;
d(x,y) = √nk=1 |(xk – yk)| i.e. manhattan distance;
xk, yk are the attributes of x and y respectively; wi = 1/ d(y,z)2;
distance weighted voting : cz = argmax v L ∑yN wi . I (v =class (cy));
KNN algorithm computes the distance or similarity between z and all the training objects to determine
nearest neighbor list for given training set D and test object z which is a vector of attribute values and
has an unknown class label. The algorithm then assigns a class to z by taking the class of majority of
neighboring objects. The storage complexity of KNN algorithm is o(n) where n is the training objects. The
time complexity is also o(n) since the distance needs to be computed between the target and each
training object. There are several key elements of this approach : (a) set of labeled training objects to be
used for evaluating a test object’s class; (b) a distance of similarity metric to compute the closeness of
objects; (c) the value of k, number of nearest neighbors and (d) the method of distance measurement.
KNN is a specific case of instance based learning such as CBR. It is particularly suited for multimodal
classes as well as applications in which an object can have many class labels. The performance of KNN
algorithm depends on the choice of k, an estimate of the best value for k that can be obtained by cross
validation. If k is very small, the results can be sensitive to the noise points. If k is too large, then the
neighborhood may include too many points from the classes.
Another approach is the approach of combining class labels. The simplest method is to take a majority
vote. This can be a problem if the nearest neighbors vary widely in their distance and the closer
neighbors, more reliably indicate the class of the objects. Another approach is to weight each object’s
vote by its distance wi = 1/ d(y,z)2 ; distance weighted voting : cz = argmax wi x I (v = class (cy). The

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 53
choice of distance measure is another important issue. It can be Eucledian or Manhattan distance
measure. Building the classification model is cheap but classifying unknown objects relatively expensive
since it requires the computation of k nearest neighbors of the objects to be labeled.
3.3.2 Perception
Human agents can perform different types of physical and mental tasks without any measurements and
any computations. In healthcare domain, a doctor can understand the medical problems of the patients
and recognize symptoms, similarities and dissimilarities through the perception of time, distance, force,
direction, shape, color, odor, taste, number, possibilities, likelihood, truth and other different types of
attributes of physical and mental objects. Perception is the basic building block of approximate reasoning.
Recognition and perception are closely associated. Recognition is a sequence of decisions, decision are
made based on information and the information is a mix of measurements and perceptions.
Measurements are crisp (e.g. Body weight is 60 kg.) while perceptions are fuzzy (e.g. body weight is
normal). Perception may be converted into measurements but such conversions may be
counterproductive, unrealistic and infeasible. Alternatively, perceptions are converted into propositions
expressed in natural languages such as a patient is very weak. Perceptions are intrinsically imprecise and
f-granular i.e. both fuzzy and granular. The boundaries of perceived classes are unsharp and the values
of the attributes are granulated. A granule is a clump of elements of a class that are drawn together by
similarity, proximity, indistinguishability or functionality. The perception of blood pressure of a patient
may be expressed as very high, high, medium, low and very low. F-granularity of perceptions reflects
the finite ability of sensory organs and the brain to resolve detail and store information. Information can
be singular (temperature: 980 C), c-granular (temperature: 960 - 990C) and f-granular (temperature:
normal). The computational theory of perception (CTP) deals with perception based system and function
modeling, time series analysis, probability and statistical analysis treating perceptions as a collection of
different linguistic if-then rules. CTP uses natural languages systematically to express patterns, classes,
perceptions and recognitions for data mining and knowledge discovery from data. CTP computes and
reasons with perception based information replacing traditional predicate logic and probability theory. In
CTP, a proposition p is an answer to a question and it represented as a generalized constraint. The
descriptors of perceptions are translated into generalized constraint language (GCL) and precisiated
natural language (PNL). Goal directed constraint propagation answers a given query. In fact, a doctor can
use both complex perception based fuzzy information and simple measurement based crisp information
for intelligent decision making in patient care.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 54
Figure 6 : Decision making in healthcare
Robots are increasingly used for complex surgical operations such as brains, eyes, hearts and hip
replacements. Intelligent robotic walkers and toys are used for elderly and handicapped people. Robots
are equipped with sensors for perceiving their environment and effectors with which they can assert
physical forces on their environment. Perception is the process by which robots map sensor
measurements into internal representations of the environment. Perception is a complex process as the
sensors are noisy and the environment is partially observable, unpredictable and dynamic. Robots have e
problems of state estimation or filtering. Good internal representations imply that robots have sufficient
information to make good decisions, they are structured and updated efficiently and they are natural.
Machine learning plays an important role in robot perception.
The mechanism (HM) uses the intelligence of workflow management system for efficient
time management, exception handling and resource assignment during registration,
consulting, testing and surgical operations.
The healthcare service provider should use a workflow management system to improve quality of service,
operational efficiency and to ensure the safety of the service consumers through proper resource
allocation, capacity utilization, meeting scheduling and exception management. The system requires
proper integration among process definition, workflow engine, rules engine and healthcare information
system through exchange of data, events and actions [35]. Generally, sequential and parallel control
flows are used for simple time scheduling. Process optimization, high throughput and efficiency are
essential to improve revenue and reduce the cost of the service provider. The workflow management
system should plan the schedule of the specialists of a healthcare chain for attending national and
international medical conferences, workshops and seminars logically so that the service consumers get
proper treatment and consulting service in time.
Case based reasoning
AnalyticsPerception
Decision Making
Experiment
DSS, GDSS, KMS, Expert system

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 55
The mechanism (HM) uses the intelligence of web enabled ERP system for improved
coordination and integration among various healthcare units.
The mechanism uses an web enabled enterprise resource planning system for fast and correct
transaction processing, financial management and supply chain coordination among various tiers of the
healthcare chain. A typical ERP system should be used for sales and distribution, materials management,
finance and cost control and human resource management. The ERP system should be integrated with
workflow management, supply chain management and business intelligence systems for a complex and
large healthcare organization. The supply chain management system should be used for collaborative
planning, forecasting and replenishments, order management, distribution and demand planning,
inventory control, warehousing and shipping functions. The BI system should have data warehousing,
analytics, data visualization, data mining and performance measurement modules for strategic decision
making. The enterprise applications of multiple tiers of the healthcare supply chain are integrated
through internet.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 56
Chapter 4: Data Schema
4.1 Business Intelligence Systems
The healthcare workforce can use novel, rich and interactive Business Intelligence
applications through efficient data warehousing and data acquisition techniques, cloud data
services and next generation mobile devices for intelligent data analysis, query and
transactions processing.
The healthcare information system requires a well-defined master data schema and configuration setting
for fast and correct computation and intelligent query processing. The primary elements of data schema
are an efficient data extraction and noise filtering algorithm, a secure data warehouse and a set of data
mining algorithms. Raw data is extracted from heterogeneous sources; the extracted data is filtered and
stored in a secure data warehouse. The data mining algorithms are applied on the stored filtered data
and new knowledge is discovered and applied for intelligent decision making.
The healthcare service provider (Pf and Ps in healthcareflow mechanism) evaluate the performance of the
trading agents associated with the supply chain periodically based on historical trading data stored in a
secure data warehouse; this evaluation is important for efficient financial and cost accounting, sourcing
and risk management. Pf compute the credit rating of the service consumers and also performs spend
analysis; Ps compute the vendor rating of the vendors on the basis of quality of products and delivery
performance. Ps inform the vendor rating to the vendors periodically; efficient vendors are rewarded and
the inefficient agents get alert or blacklisted as per regulatory compliance policy. The data schema should
support various transactions maintaining confidentiality, message integrity and nonrepudiation through
credential based access control mechanism. Auditing is required to check fairness and correctness of
computation and to validate security policies on periodic basis. Data plays a strategic role in healthcare
information system and its protection against unauthorized disclosure (secrecy) and improper
modifications (integrity), while ensuring its availability to legitimate users (no denial of service) is also
very important.
The CIO, system administrator and system analysts have jointly decided that the healthcare service
workforce should use BI applications through sophisticated data analysis techniques on strategic data
assets for better and faster decision making and innovative service offerings to the patients. From market
surveys and negotiation with the vendors, they have observed that the cost of data acquisition and data
storage has declined with the launch of parallel data architecture and sophisticated analytic tools. Today,
the top management requires short time lag between data acquisition and decision making.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 57
4.2 Performance Scorecard
The healthcare service provider should deploy an online performance scorecard system for
the evaluation of quality of service based on correct feedback of the patients.
The business analysts have designed a performance scorecard for online implementation. A patient and
his / her attendant should enter name, registration number, age, gender, date, contact phone number
and e-mail id into the online feedback form before going through a set of questions and giving rating
based on perception, observations and practical experience. He / she should indicate the reason of
selection of the healthcare service provider. The performance scorecard is designed based on a simple
data structure : serial number, business function, performance metrics, rating scale and suggestions /
remarks. The rating scale has five options : excellent or very satisfactory (rating score: 5), very good or
satisfactory (rating score : 4), good i.e. neither satisfactory nor dissatisfactory (rating score : 3), average
or dissatisfactory (rating score : 2) and poor or very dissatisfactory (rating score :1). The basic objectives
of the performance scorecard are to ensure fairness and correctness in computation, evaluate the
performance of the healthcare consultants and workforce and improve quality of service. The objectives
of the feedback systems should be communicated clearly to the patients and their attendants. The
patients give rating for each business function and performance metric after the discharge and they are
assumed to give true and honest feedback and suggestions in a trusted computing environment for the
improvement of the healthcare system, quality of service and operational excellence. The performance
scorecard computes the aggregate score based on the rating selected by the patients during a specific
period. The patient’s relationship management associates should be able to interact with the patients in
time for any clarification. The service provider should also keep the option of manual feedback form for
the patients not knowing computers and information technology.
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Registration Speed / waiting time 2. Identity proof check3. Data entry accuracy4. Design of registration card5. Cooperation and attitude6. Clarity of information7. Quality of workflow
managementTable 1: Performance scorecard for registration

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 58
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Consulting Correctness of appointment2. Design of appointment slip3. Accuracy of data4. Flexibility5. Exception management 6. Quality and clarity of
treatment7. Punctuality and availability8. Waiting time 9. Care, concern and
attentiveness10. Use of IS ( e.g. CBR)
Table 2: Performance scorecard for consulting
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Testing Explanation of consent form2. Waiting time 3. Skill of testing4. Quality of measuring
instruments5. Correctness of test results6. Payment processing
Table 3: Performance scorecard for testing
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Surgery Waiting time2. Pre-surgery testing3. Surgery schedule4. Correctness of data( e.g. tariff)5. Operation theatre environment6. Conduct of OT personnel7. Quality of nursing8. Skill of surgeons9. Clarity of post operative
instructions10. Promptness in transfer from OT
to ward or waiting room11. Overall coordination
Table 4: Performance scorecard for surgery
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Supply chain coordination
Scope of negotiation
2. Clarity of information given for procurement
3. Purchasing4. Receiving5. Inspection 6. Payment processing7. Quality control certificate 8. warranty verification9. Quality of medical devices
Table 5: Performance scorecard for supply chain management

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 59
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Discharge Clarity of instructions and guidance during discharge
2. Medical diagnosis3. Correctness of data in
discharge summary4. Drug prescription and
administration5. Pain management 6. Promptness in attending calls
Table 6: Performance scorecard for discharge
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Billing Correctness in computation2. Fairness in computation3. Flexibility in payment mode4. Admission and settlement of
bills5. Skill 6. Attitude of workforce7. Speed / waiting time
Table 7: Performance scorecard for billing
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Follow up Correctness of schedule2. Patientflow control3. Care, concern & attentiveness4. Punctuality5. Clarity of instructions6. Coordination
Table 8: Performance scorecard for follow up
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Nursing care Attending calls and promptness 2. Behavior, attitude, care and
concerns 3. Communication and clarity of
instructions4. Pre operative nursing care5. Post operative nursing care6. Medicare administration7. Diet chart
Table 9: Performance scorecard for nursing care
SL No.
Business Function
Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Maintenance Electrical system2. Mechanical system3. Civil infrastructure4. Measuring instruments5. Information system6. Communication system7. Quality of house keeping

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 60
services : Hygiene and courtsey 8. Cleaning of rooms / ward9. Cleaning of toilets
Table 10: Performance scorecard for maintenance
SL No.
Infrastructure Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Infrastructure Ward2. Operation theatre3. Canteen4. Signage 5. Parking facilities6. Outdoor7. Emergency
Table 11: Performance scorecard for infrastructure
SL No.
Criteria Performance Metrics
Excellent Very good
Good Average Poor Suggestions & remarks
1. Overall impression
Quality of service
2. Healthcare cost3. Healthcare outcome 4. Value
Recommend others : yes / no
Table 12: Overall impression
4.3 Data Visualization
Intelligent data visualization techniques are extensively used for image processing
applications and graphical presentation of test results of the patients. The healthcare
consultants require the support of these techniques for correct medical diagnosis and
subsequent treatment and surgical operations.
Medical imaging ensures fairness and correctness in medical diagnosis. Intelligent pattern recognition or
data mining algorithms are generally used for digital radiography, computed Tomography, Nuclear
medicine, ultrasonic imaging, magnetic resonance imaging and diffuse optical imaging. Biosignals are
used for Electroencephalography and Electrocardiograms. The fairness and correctness of computation
for medical testing depends on the efficiency of machine learning and data mining algorithms. The
pattern recognition algorithms are based on computed tomography, multi-element and multidimensional
phased arrays in ultrasound, combined positron emission tomography (PET) for CT scanners and rapid
parallel imaging for MRI. For example, planar X-ray imaging techniques are used for orthopedic, kidney
stones, lungs and gastrointestinal problems. Nuclear imaging techniques image the spatial distribution of
radioactive materials injected into the body to detect abnormal tissue distribution for cancer. Ultrasonic
imaging use ultrasound technology and Doppler measurements. MRI is a non-ionizing technique with
excellent soft tissue contrast and high spatial resolution used for brain disease, spinal disorders,
angiography, cardiac assessment, and musculoskeletal damage. The other common techniques are
Diffuse Optical imaging, parametric imaging and biosignals based EEG and ECG for the treatment of

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 61
cardiac and cancer problems. Biomedical data processing and analytics are extensively used for medical
diagnosis through image enhancement, segmentation, feature extraction and interpretation.
The advances in digital biomedical imaging technologies enable visualization of the structure, function
and pathology of human body effectively. These images can be acquired in multiple dimensions and with
multiple modalities through magnetic resonance imaging (MRI) and positron emission tomography
coupled with computed tomography (PET/CT). A major challenge now is to put the large amount of
imaging data in a readily usable and viewable format for interpretation. The healthcare service provider
should also consider the progress in three-dimensional visualization of biomedical data. It is the ability to
interact and navigate the image data in a realistic 3D volumetric display. These volumetric displays are
typically constructed from 2D slice images that are acquired in a regular pattern and make up a
volumetric grid. 3D visualization techniques are extensively used for image processing applications, image
guided surgery, radiotherapy and computer aided diagnosis. It is possible to perform real-time interactive
visualization of multidimensional data using low cost hardware instead of high end workstations.
Intelligent data visualization techniques are increasingly used for innovative biomedical data
interpretation in computer integrated surgery, virtual biopsy, motion activity visualization, radiotherapy,
parametric medical imaging, computer aided design and modeling of bones, muscles, cartilage,
ligaments, and tendons. Parametric imaging requires modeling and parameter estimation for certain
metabolic, pharmacokinetic, endocrine and various biochemical systems and visualization of anatomical
structures.
The healthcare consultants and medical test lab professionals have a meeting with the CIO and system
analysts. They have informed the need of intelligent data visualization techniques for correct
interpretation of test results. The system needs high accuracy of machine learning and pattern
recognition algorithms for correct image processing. For critical cases, they need the graphical
presentation of test data (e.g. blood, urine, pressure) for time series analysis. The system analysts have
also met the chief financial officer (CFO) and supply chain manager. They need intelligent analytics and
multi-dimensional data visualization techniques for analysis of revenue, cost, demand, inventory, resource
capacity, supplier’s performance, spend, quality and HR performance. These analyses are important for
financial, supply chain and human resource management, process mining, patient care and formulation of
corporate strategy and policy.
4.4 Data Warehouse & Data Mining
Business Intelligence applications requires the support of efficient data warehousing (DW)
architecture, Extract-Transform-Load (ETL) tools, Complex Event Processing (CEP) engines
and efficient data mining algorithms.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 62
Figure 7: Data schema with data warehouse and data mining for KDD
The healthcare information system gets various types of data from registration, consulting, testing,
surgery, supply chain management, billing and discharge modules. The BI applications require
integration, cleaning and standardization of data against inconsistencies, incompleteness and noise. The
filtered data is loaded into a data warehouse (DW) server for simple and complex multidimensional SQL
query processing, data mining and case based reasoning. Intelligent relational database management
systems (RDBMS) can be used for storing and querying DW data. The system administrator is facing a
big data challenge - how to use low cost data warehouse to support large volume of data. Additionally,
the data schema requires online analytic processing (OLAP) servers for filtering, aggregation, drill-down
and pivoting of data, reporting servers to generate intelligent reports for financial analysis and supply
chain management, enterprise search engines, data mining engines, text analytic engines and web
analytics.
Decision support queries use index structures in RDBMS for filtering, join, and aggregation; materialized
views for summary of data; partitioning to divide tables and indexes into smaller manageable units and
hash and range partitioning for database maintenance. Data compression can reduce data load and the
cost of the query; results lower storage and backup costs; supports intelligent query processing on
compressed data and increases network bandwidth. Data compression is important in biomedical imaging
applications due to digital biomedical imaging systems (e.g. digital x-ray), improvement of image
resolution and online sharing of information through networks. A basic data compression system has an
encoding and a decoding component. The encoder performs compression and the decoder does
decompression. The objective of any data compression system is to reduce the size of signal data while
maintaining information integrity or a certain degree of it. Digitized medical images require storage
space and bandwidth for transportation over communication networks. Data compression is useful for

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 63
reduced storage and transmission requirements. The critical issue of medical images compression is
information integrity. Information loss should be avoided when possible. Data compression may be lossy
or lossless. Lossless compression is desirable since it maintains information integrity. Competitive
compression strategies employ predictive coding and context based coding prior to entropy coding to
enhance compression performance.
Intelligent query processing can provide multidimensional view of data; OLAP supports filtering,
aggregation, pivoting, rollup and drill down on multi-dimensional view of data. OLAP servers use
multidimensional storage engine (MOLAP) or relational DBMS engine (ROLAP) or hybrid engine (HOLAP).
MOLAP computes large data cubes to speed up query processing. In ROLAP, the multidimensional model
and its operations are mapped into relations and SQL queries. Relational database servers are the
backend of large data warehouses; they support processing of complex SQL queries from very large
databases by query optimization. The query optimizer selects a complex query and compiles that into an
execution plan. Parallel processing supports query processing over large databases for selection,
projection, join and aggregation operations. BI applications search over different types of data through
an integrated model. The search engine crawls each data source and stores the data into a central
content index for fast querying. ETL tools take care of data quality issues for correct reporting, ad hoc
queries, and predictive analysis.
Cloud data services can support hardware provisioning and server consolidation based on virtualization
and pay-as-you-go model. But, data-storage-as-a-service faces various challenges such as security and
privacy of data, access control, performance and scaling of complex query processing and intelligent
reporting. The system administrator has considered the issues of data partitioning, data compression,
query optimization, data cube, multidimensional data model, parallel processing enterprise search
engines, ETL algorithms and private cloud services for effective data warehousing at affordable cost.
Data mining algorithms are provided through statistical software packages (e.g. SAS, SPSS, MATLAB,
Microsoft Excel minor, Microstrategy) or in-database-analytics solutions for various functions such as
classification, prediction, clustering, regression, time series forecasting and association rule mining. But,
the main problem is the high cost of data mining software packages. The CIO have asked the business
analysts to explore the scope of data mining in healthcare business, select a specific set of data mining
algorithms and also to do the cost benefit analysis. He has also discussed the issue with the purchasing
manager for the procurement of costly machines such as CT scanner. For example, support vector
machine can be used as optimal margin classifier in image processing.
4.5 Electronic Medical Records (EMR)
Electronic Medical Records (EMR) is expressed by various terms such as Personal Health Record (PHR),
EMR and Electronic Patient Record (EPR). PHR contains a patient’s medical history in a digital format.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 64
EMR is the documentation for a patient with all services provided within a healthcare service provider.
EMR should take care of system quality (accessibility, usability), information quality (readability,
accuracy) and decision support (data analysis). The data structure of EMR is complex and diverse
including demographic and historical data. Demographic data give the details of patient’s name, date of
birth, unique MRN or patient identification number (PID), address and contact details, attendants identity
proof and the details of referring doctors. The historic data provide the details of medical records like
current clinical diagnosis, medical history, medications, allergies, examination findings, treatment plan,
investigations, complications, nursing observations, treatment plans and notes of specialists. EMR
provides benefits in terms of access control, searching, information retrieval, secure storage and safe
transmission of patient data. But, the critical issues are quantity and complexity of data, use of standard
medical terminologies, diversity of data infrastructure and databases within and across enterprises and
the community.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 65
Chapter 5 : Communication Networking Schema
The mobile communication technology and sensor networks are the basic building blocks of
m-health and telemedicine. These digital technologies can replace traditional healthcare
model in the context of home care, mobile society, changing population demographics and
expensive healthcare.
Mobile health (m-health) and telemedicine are interesting healthcare models which use wired and
wireless communication technologies for real-time health monitoring of service consumers. Telemedicine
uses transmission of medical data (e.g. health parameters measured by biosensors, medical images)
through communication channels. The people use mobile phones for consulting with doctors and
healthcare service providers during emergency situations or travel. However, the mobile commerce model
of healthcare is not matured as on date. In fact, the healthcare specialists generally like to check the
health conditions of the patients physically through face-to-face meeting. They may be confused by the
misleading communication from the patients due to lack of their knowledge and experience and make
errors in diagnosis and administration of drugs. Sensor networks are necessary to monitor health
parameters of critical patients requiring constant support. A sensor detects the presence and the variation
of physical parameters such as pressure, temperature, humidity, velocity, force, torque, slip, vibration,
contact, proximity, motion and biochemical properties in mechanical, thermal, chemical and optical
domain. Wearable medical sensors are used to monitor health parameters like heart rate, motion, body
temperature, blood pressure, pulse rate, arterial oxygen saturation, body weight, ECG and EEG
waveform. The critical constraints of sensors are cost, size, energy consumption, mobility, processing and
storage capability. The system administrator has found out that the communication schema can be used
in various ways in healthcare like notification, messaging, alert, web access, videoconferencing,
radiology, general and surgical consultation. The deployment of communications technologies and
network infrastructures can reduce the cost of conventional healthcare system and improve quality of
service for scalable operation. But the networking schema often face critical challenges like bandwidth,
channel capacity, noise, congestion, energy consumption and security and privacy of data.
Human Computer Interaction is the basic building block of a smart medical home.
Multimedia supports human computer interaction through visual information processing,
speech processing, emerging sensing modalities and virtual reality. HCI technologies can be
effectively used for surgical education and patient care, simulation of operating theatre,
videoconferencing, online shopping of drugs and healthcare products in virtual environment,
video on demand services and e-learning for remote healthcare.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 66
The system analysts have informed the CIO about the recent trends of human computer interactions and
multimedia technologies and their applications in healthcare services. A smart medical home integrates
the healthcare information system with a patient’s home for comforts, privacy and real-time health
monitoring. Telemedicine uses multimedia technologies such as audio, visual and communication network
for medical diagnosis, treatment and patient care; health data is exchanged between patients and
physicians. Virtual reality integrates different sensing technologies of human computer interaction
seamlessly and allow the users to gain realistic experience. Computer driven simulations of operating
theater in virtual reality support surgical education and training of technical skill. Today’s smart medical
home and surgical operation theatres can use various types of multimedia technologies innovatively such
as human computer interaction, multimedia content management, multimedia delivery, telemedicine,
sensory devices, speech and conversational systems and virtual reality. Smart medical home use
electronic devices (e.g. Internet, mobile phones and interactive digital television), electrical equipments
and security devices for automation of domestic tasks, urgent communication during emergency
situations, human friendly control and personal safety. Seamless integration of different multimedia
technologies is necessary for medical devices used in a smart medical home. The objective of human
computer interaction is to mimic human-human interactions such as basic senses of human cognition.
HCI uses natural human actions such as facial expressions, body movement, speech and eye movement
to interpret and generate output. Vision and speech are two of the most critical senses used in human
computer interaction. Speech processing performs speech recognition and speech synthesis. Visual
information indicates what a man perceives through his eyes and data captured by optical cameras.
Visual information processing systems use face recognition and optical character recognition technology.
Digital technology uses the intelligence of web, videoconferencing and mobile
communication system for collaborative information seeking, virtual and critical patient care
and telemedicine.
The system analysts and networking consultants have deigned an efficient networking schema which is
expected to use web service, video conferencing and mobile communication devices intelligently. Video
conferencing enables critical patient care and virtual patient visit. But, it is a costly option. Web service
provides a trusted computing platform where the agents can share data through secure communication
channels for registration, workflow administration and time scheduling. Rural healthcare infrastructure
needs secure wired and wireless communication system for urgent cases. The system is expected to use
e-mail, social networking and mobile internet service. The rural people from remote places should be able
to communicate with healthcare specialists for necessary advice, fast aid and making transportation
arrangement through ambulances during emergency (e.g. sudden critical sickness or accidents). They

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 67
can learn the basic knowledge of medicare, hygienic life-style, family planning and preventive measures
through television and radio broadcasts conducted by the healthcare service provider.
Intelligent location based services can be effectively used for emergency situations. The system should
have a mobile device and biosensors attached with the patient’s body, a device monitored by a doctor, a
central monitoring unit embedded with location based services and wireless sensor network. The sensors
measure and collect health parameters of the patient, the doctor receives the alarm signals and CMU
controls the communication between the devices associated with the patient and doctor. Alternatively,
the patient can use global positioning system (GPS) enabled mobile device which can indicate his location
during sudden illness during emergency situation. The mobile device should be able to inform his location
details (location name, longitude, latitude) to his family member or emergency contact number
intelligently. Additionally, he should carry an identity proof with his contact, address and the name of
family members. During sudden illness, he should get the help of the police or the public or his friends
or family members in time for fast admission to the hospitals. The service consumers and the healthcare
service provider should be able to interact effectively during emergency. However, the poor people
should be able to buy such costly mobile devices and use the same in a simple way.
Knowledge is a significant asset of any healthcare service provider. It is the state of knowing and
understanding the medical problems of the patients. Data is raw numbers and facts, information is
processed data and knowledge is processed information. Knowledge management focuses on exposing
individuals to potentially useful information and facilitating assimilation of information. It involves
enhancing individuals learning and understanding through provision of correct information. The
healthcare experts should use a cooperative communication system for effective learning, solving
complex problems and intelligent decision making.
A cooperative communication schema enables creation, storage, sharing, distribution and transfer of
knowledge and information among a group of authorized entities of a complex healthcare organization. It
also provides effective search and retrieval mechanisms for locating relevant information. It is essential
for collaborative information search which may be explicit or implicit. The level of mediation implies how
aware a system is of the contribution of different searching agents and how it uses those contributions to
influence the search of the investigators. The decision making agents can collaborate synchronously or
asynchronously; they may work at the same place at the same time or may be distributed at different
sites. Different agents may play different roles in the searching process. The agents can divide the task
in different ways depending on the roles. The allocation of tasks depends on the nature of tasks, skill
and experience of the agents and the capabilities of the system that mediates information seeking.
Collaborative information seeking is gradually becoming essential in healthcare management; the
specialists should be able to find out good solutions for critical cases.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 68
Videoconferencing is an important component of cooperative communication schema that gives
support to critical patient care and virtual patient visit, medical board meeting, consulting, dispute
resolution, telemedicine and negotiation in trading process. It provides many benefits in terms of reduced
travel cost, faster decision making, wider participation in decision making, improved quality of service,
increased productivity, improved customer relationship, better team management and expanded global
reach. It is particularly very useful for critical patient care and emergency situations when the required
skill and domain knowledge is rare at a healthcare institute. But, a field study on medical professionals
found that people process information differently between videoconference and face-to-face
communication. In videoconference, people tend to be more influenced by heuristic cues and
communication skill and likeability of the speaker rather than by the quality of arguments of the speaker.
Communication through videoconference presents the challenges of difficult audio localization, turn
taking, conversation speed, change in cue salience, asymmetrical personal distance and high level of self-
awareness and all these factors increase the cognitive workload demand from the participants as
compared to face-to-face communication. Cognitive theory has a significant implication on sense making
through videoconference. In spite of all these constraints, videoconference is useful to streamline
knowledge adoption and transfer in healthcare management. Alternatively, the healthcare specialists can
share knowledge through netmeeting software or cloud computing services.
The rapid expansion of global market, the explosive growth of information and communication
technologies, aggressive competition and the changing economic and social conditions have triggered
tremendous opportunities to provide healthcare service electronically. E-health is a significant
development of the use of emerging information and communication technologies in healthcare. E-health
while promising also presents new business challenges in terms of acceptable standards, choice of
technologies, overcoming traditional jurisdictional boundaries, upfront investment, privacy and
confidentiality of critical data. New and evolving information and communication technologies are being
adopted by healthcare service providers worldwide. It is essential for an efficient healthcare information
system to integrate different enterprise applications such as analytics, ERP, SCM and KMS through
extranet, intranet and internet for proper information flow, rational decision making and fast and correct
transaction processing. E-health requires an efficient and intelligent mechanism to provide various
benefits such as improved customer service, accuracy, ease of processing, increased productivity, quick
access to information, greater geographical reach, better coordination, reduced transaction costs, rational
decision making and efficient knowledge management. But, it has several constraints and challenges like
high cost of computation and communication, information flow, privacy of data, coordination, economic
modeling, pricing strategy, payment, fairness and correctness of service transactions and behavior of the
service consumer and provider.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 69
Another important component of a cooperative communication schema is internet, intranet and extranet.
Web enabled enterprise applications are essential for efficient coordination, integration and workflow
control. The trading agents should be able to share strategic information with confidentiality through a
trusted computing environment. The online transactions should be processed through web maintaining
privacy, confidentiality, message integrity and non-repudiation. Secure Service Oriented Computing
(SSOC) is the basic building block of enterprise application integration. It integrates a network of
enterprises by positioning web services as the primary elements. Each web service exists as an
independent software program with distinct design characteristics. Each service is assigned a specific
function and capabilities. A service composition is a coordinated, aggregate of services that integrates
different applications through robust interfaces. A service oriented computing platform is comprised of a
distinct set of components; each component encapsulates specific business logic and service.
A service oriented computing model is expected to provide a trusted computing environment to the users
of the system. Otherwise, the malicious agents can attack the healthcare system in different ways. The
most promising technology that supports SSOC is web service. It supports the execution of various
business processes that are distributed over a network and available through standard interfaces and
protocols. Service oriented computing model requires an intelligent design paradigm to protect its users
from miscellaneous types of malicious attacks such as phishing, cross site scripting, malicious file
injection, insecure direct object reference, cross site request for query, information leakage, improper
error handling, broken authentication and session management, insecure cryptographic storage and
failure to restricted URL access. The healthcare information system should have service oriented
architecture to enhance the efficiency, agility and productivity of the agents.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 70
Chapter 6 : Security Schema
The CIO is discussing with the system analysts, system administrator and information security
consultants on various aspects of security schema for the digital technology platform: computational
intelligence in terms of cryptography and secure multi-party computation, web security, biometric access
control and healthcare security policy. The main focus of security schema is to ensure fairness and
correctness in computation of registration card, appointment slip for consulting, prescription by
consultant, surgery schedule, quality control certificate, medical test report, discharge certificate, bills and
payment receipt, feedback form and patient’s guide. The other important issue is to preserve the privacy
of patient’s personal and medical data. There may be the risks of failure of secure multi-party
computation in terms of authentication, authorization, correct identification, privacy, audit, fairness and
correctness due to various reasons:
Incorrect data provided by the service consumers or patients to the registration associate during
registration intentionally or due to lack of knowledge or incorrect perception of the patients or
their attendants; the patients or their attendants may be irrational in information sharing properly
with the service providers.
No verification of patient’s identity correctly during registration; the cases of emergency situation
or accidents may skip verification due to unavailability of data about the patients;
Wrong entry of data into various information systems by the healthcare associates due to time
and resource constraints or misunderstanding or lack of validation of input data;
Computational errors due to wrong configuration of enterprise applications and / or errors in the
heuristics, algorithms and quantitative models and / or no updating of data (e.g. service charge,
tariff of testing, price of drugs and healthcare products; low accuracy of pattern recognition
algorithms in image processing system may result incorrect medical diagnosis.
Access control problem causing dangerous errors in information system; a malicious agent may
enter false data into HIS during the absence of authorized users;
Swap or mixing of test data of various patients or drugs administration due to confusion, poor
document management, lack of clear understanding or training of the healthcare workforce;
Errors in decision making by the health consultants due to lack of proper knowledge
management or misperception or lack of coordination among the workforce of various
departments or inappropriate enterprise application integration or error in test reports;
incomplete prescription due to memory failure or silly mistakes;
Errors in scheduling due to exceptions (e.g. unfit patients, non-availability of doctors and
surgeons);

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 71
Intentional errors due to malicious business practice, lack of ethics, casual approach and dull HR
policy; unintentional errors due to physical and mental fatigue for excessive workload and
sickness;
Lack of verification of correctness of computation in medical billing and payment processing by
the service provider and / or service consumer;
Incorrect data in patient’s help guide may cause confusions and mismatch between the
computed results and perceived one;
Incorrect feedback by the patients or their attendants due to misperception, misunderstanding of
feedback form, lack of knowledge and critical observations or casual attitude;
The system analysts and security consultants have performed a detailed risk assessment and mitigation
analysis and explored countermeasures to prevent the occurrence of these flaws and errors in future.
They have also analyzed the computational intelligence of secure multi-party computation and
cryptography and have outlined a security policy for the protection of digital technology assets. The
security policy spans over miscellaneous critical issues such as access control, inference control, web
security, data validation and verification, data recovery and back up, system maintenance schedule, user
training, work culture and HR practice.
6.1 Cryptography and Secure Multi-party Computation
Privacy is a critical concern of healthcare data; the issue can be addressed utilizing the concept of
cryptography including secure multiparty computation. The CIO, system administrator and system
analysts have designed jointly the basic building blocks of the security schema. The computational
intelligence depends on the efficiency of encryption, decryption, digital signature and signcryption
algorithms. The fundamental objectives of cryptography are to provide confidentiality, data integrity,
authentication and non-repudiation. Cryptography ensures privacy and secrecy of information through
encryption methods. The sender (S) encrypts a message (m) with encryption key and sends the cipher
text (c) to the receiver (R). R turns c back into m by decryption using secret decryption key. In this case,
an adversary may get c but cannot derive any information. R should be able to check whether m is
modified during transmission. R should be able to verify the origin of m. S should not be able to deny the
communication of m. There are two types of key based algorithms - symmetric and public key.
Symmetric key encryption scheme provides secure communication for a pair of communication partners;
the sender and the receiver agree on a key k which should be kept secret. In most cases, the encryption
and decryption key are same. In case of asymmetric or public-key algorithms, the key used for encryption
(public key) is different from the key used for decryption (private key). The decryption key cannot be

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 72
calculated from the encryption key at least in any reasonable amount of time. The widely-used public–
key cryptosystem are RSA cryptosystem (1978), Elgamal’s cryptosystem (1985) and Paillier’s
cryptosystem (1999).
In case of secure communication, cryptography ensures privacy and secrecy of sensitive data through
encryption method. The sender (S) encrypts a message (m) with encryption key and sends the cipher
text (c) to the receiver (R). R transforms c into m by decryption using secret decryption key. An
adversary may get c but cannot derive any information. R should be able to check whether m is modified
during transmission. R should be able to verify the origin of m. S should not be able to deny the
communication of m. There are two types of key based algorithms: symmetric and public key.
Symmetric key encryption scheme provides secure communication for a pair of communication partners;
the sender and the receiver agree on a key k which should be kept secret. In most cases, the encryption
and decryption keys are same. In case of asymmetric or public-key algorithms, the key used for
encryption (public key) is different from the key used for decryption (private key). The decryption key
cannot be calculated from the encryption key at least in any reasonable amount of time.
A digital signature is a cryptographic primitive by which a sender (S) can electronically sign a message
and the receiver (R) can verify the signature electronically. S informs his public key to R and owns a
private key. S signs a message with his private key. R uses the public key of S to prove that the message
is signed by S. The digital signature can verify the authenticity of S as the sender of the message. A
digital signature needs a public key system. A cryptosystem uses the private and public key of R. But, a
digital signature uses the private and public key of S. A digital signature scheme consists of various
attributes such as a plaintext message space, a signature space, a signing key space, an efficient key
generation algorithm, an efficient signing algorithm and an efficient verification algorithm. There are
various forms of digital signature such as group signature and ring signature. A group signature scheme
allows a member of a group to sign a message anonymously on behalf of the group. A designated entity
can reveal the identity of the signer in case of any dispute.
Traditional signature-then-encryption is a two step approach. At the sending end, the sender signs the
message using a digital signature and then encrypts the message. The receiver decrypts the cipher text
and verifies the signature. The cost for delivering a message is the sum of the cost of digital signature
and the cost of encryption. Signcryption is a public key primitive that fulfills the functions of digital
signature and public key encryption in a logically single step and the cost of delivering a signcrypted
message is significantly less than the cost of signature-then-encryption approach. The service oriented
computing model is vulnerable to insecure communication. An application may fail to encrypt network
traffic for sensitive communications. The basic objective of the proposed secure service oriented
computing model is that the application properly signcrypts all sensitive data. A pair of polynomial time
algorithms (S,U) are involved in signcryption scheme where S is called signcryption algorithm and U is

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 73
unsigncryption algorithm. The algorithm S signcrypts a message m and outputs a signcrypted text c. The
algorithm U unsigncrypts c and recovers the message unambiguously. (S,U) fulfill simultaneously the
properties of a secure encryption scheme and a digital signature scheme - confidentiality, unforgeability
and nonrepudiation. In a triplet Elgamal signature scheme (r,e,s), the commitment r is computed as r =
gk(mod p) where g and p are part of the public key and the commitment k is an integer independent to
such values. The signature generation scheme permits the receiver to recover the commitment by
computing r = gsye(mod p). The sender computes the commitment in such a way that it is only
recoverable by the receiver. The commitment value can be used as a symmetric key shared between the
sender and the receiver and this symmetric encryption provides message confidentiality. The recoverable
commitment value of Elgamal triplet signature scheme is used as the symmetric key to achieve
symmetric encryption of the message while the triplet signature serves the signature.
Secure Multi-party Computation : Two or more agents want to conduct a computation based on
their private inputs but neither of them wants to share its proprietary data set to other. The objective of
secure multiparty computation (SMC) is to compute with each party’s private input such that in the end
only the output is known and the private inputs are not disclosed except those which can be logically or
mathematically derived from the output. In case of secure multi-party computation, a single building
block may not be sufficient to do a task; a series of steps should be executed to solve the given problem.
Such a well-defined series of steps is called a SMC protocol. Secure multi-party computation should have
a set of properties such as privacy, fairness, correctness, independence of inputs and guaranteed output
delivery. A SMC protocol ensures correctness if each party receives correct output. Corrupted (or
malicious) parties select their inputs independently of the inputs of honest parties and honest parties
must receive their output. Corrupted parties should receive their outputs if and only if the honest parties
receive their outputs and this ensures fairness of the protocol.
A protocol preserves privacy if no agent learns anything more than its output; the only information that
should be disclosed about other agent’s inputs is what can be derived from the output itself. Secure
multi-party computation preserves privacy of data in different ways such as such as adding random noise
to data, splitting a message into multiple parts randomly and sending each part to a DMA through a
number of parties hiding the identity of the source, controlling the sequence of passing selected
messages from an agent to others through serial or parallel mode of communication, dynamically
modifying the sequence of events and agents through random selection and permuting the sequence of
messages randomly. In the study of SMC problems, two models are commonly assumed : semi-honest
model and malicious model. A semi-honest party follows the protocol properly with correct input. But
after the execution of the protocol, it is free to use all its intermediate computations to compromise
privacy. A malicious party does not need to follow the protocol properly with correct input; it can enter
the protocol with an incorrect input. A third party may exist in a protocol. A trusted third party is given all

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 74
data; it performs the computation and delivers the result. In some SMC protocols, an untrusted third
party is used to improve efficiency. This section analyzes the computational intelligence of the security
schema.
6.2. Cloud Security
Application : Web enabled enterprise solutions associated with cloud computing schema;
Agents : User of web application, system administrator;
Protocol : verify the design flaws in service oriented computing schema.
logic attack : check the main flow, sub flows and exception flows as per business rules of the application;
cross site scripting: check whether all parameters of the web application are validated properly; check the
risk of phishing attack;
injection flaws : check whether user data modify the meaning of command and queries sent to any
interpreters invoked by web application;
malicious file injection : check the use of dangerous application programming interfaces by testing and
code review;
insecure direct object reference : check through code review whether the web application allows direct
object references;
cross site request forgery : check whether web application generates authorization token that is not
automatically submitted by the web browser;
information leakage and improper error handling: check whether web application leaks any data through
error messages; check whether the application builds a trusted computing environment;
broken authentication and session management: check through code review whether the web application
properly authenticates users and protects their identities and credentials;
insecure cryptographic storage: check whether web application properly encrypts sensitive data; check
configuartion of the web server;
insecure web communication: check whether the web application ensures private communication
between the sending and receiving agents; assess the risk of snooping;
failure to restrict URL access : check whether proper access control is enforced at the presentation layer
and business logic for all URLs in the web application;
Figure : Cloud Security Verification Mechanism (CSVM)
CSVM verifies service oriented cloud computing schema to mitigate the risk of common
vulnerabilities.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 75
CSVM addresses a set of dangerous attacks against web enabled distributed computing system. The basic
objective of CSVM is to protect the healthcare information system from phishing attacks, privacy
violations, identity theft, system compromise, data alternation, data destruction, financial and reputation
loss. Cross site scripting (XSS) flaw allows an attacker to execute malicious code in the web browser of
the user that can hijack user session, deface websites, possibly introduce worms or insert hostile content
or conduct phishing attack and take over the browser of the victim through malware. The best protection
of XSS is a combination of validation of all incoming data and appropriate encoding of all output data.
Validation allows the detection of XSS attacks and encoding prevents injection of malicious script into the
browser. Cross site request forgery (CSRF) forces the web browser of the logged on user to send a
request to a vulnerable web application which forces the victim’s browser to perform a hostile action.
Web applications rely solely on automatically submitted credentials such as session cookies, basic
authentication credentials, source IP address, SSL certificates or windows domain credentials. CSRF is
applicable to any web application that has no authorization checks against vulnerable actions.
Injection flaws allow the attacker to create, read, update or delete any arbitrary data available to the
application. Even, it may compromise the web application completely bypassing firewalled protection.
SQL injection occurs when the data input of the user is sent to an interpreter as part of a command and
query. The hostile data of the attack forces the interpreter to change the data or execute unintended
command. The common protection measures are to use strong and safe interpreters, do input validation,
use strongly typed parameterized query APIs, enforce least privileges, avoid detailed error messages, use
stored procedures, do not use dynamic query interfaces and do not use simple escaping functions.
Web application developers often trust input files improperly and the data is checked insufficiently.
Arbitrary, remote and hostile content may be processed or invoked by the web server. It allows an
attacker to perform execution of malicious code, installation of tool kit and system compromises
remotely. Flawless design is required during the construction of system architecture, design and
software testing. The application developers should use indirect object reference map, check errors,
validate user’s input and implement firewall rules appropriately. Another critical problem is insecure direct
object reference; a direct object reference occurs when a reference is exposed to a file, directory,
database records or key as a URL or form parameter. A malicious agent can manipulate these references
to access other objects without authorization. The web application should avoid exposing direct object
reference to the users by using an index, indirect reference map or other indirect validated method that
is easy to validate.
An web application can unintentionally leak information about their configuration, internal state or violate
privacy through error messages and it can launch dangerous attacks. The application should get support
from a standard exception handling mechanism to prevent the leakage of unwanted information; detailed
error handling should be limited; errors should be properly checked and should not be exploited by the
intruders. Broken authentication and session management is caused due to the failure of protection of

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 76
credentials and session tokens. It can hijack user’s or administration’s accounts, undermine authorization
and accountability controls and cause privacy violations. The common protective measures are the
adoption of efficient authentication mechanisms, secure communication and credential storage, use of
efficient session management mechanisms; invalid session identifiers should be rejected.
Insecure cryptographic storage is caused due to the failure in encrypting sensitive data; it leads to
disclosure of sensitive data and compliance violation. It is required to avoid inefficient weak cryptographic
algorithms and check whether sensitive data are encrypted properly. An web application may fail to
encrypt network traffic to protect sensitive communications. The adversary can sniff traffic from the
communication network and access sensitive data, credentials, authentication or session token. The
application should properly encrypt critical data. The only protection for a URL is that links to a page are
not presented to unauthorized users. The adversary may get access to these pages and view private
data. All URLs and business functions should be protected by an effective access control mechanism.
Web security is a very broad topic; some common critical issues have been discussed above very briefly.
There are several open issues in the design of service oriented computing schema. It is an interesting
option to interview Internet experts, web developers and programmers and analyze the complexities and
challenges in web programming issues.
6.3 Access Control
Biometrics are used for automated recognition of the users and system administrators based on their
biological and behavioral traits such as finger prints, face image, iris and voice. Traditional authentication
methods like passwords and identity documents may fail to meet reliable security and performance of
identification systems. Some physical and behavioral attributes of human beings are uniquely associated
with an individual. Biometrics capture these traits with sensors; represent them in digital format; compare
the recorded data with the data acquired from the same user previously and performs recognition.
Biometrics are applicable to the access control of enterprise solutions.
Healthcare digital technology should be protected by a robust access control mechanism. Access control
is the process of receiving the requests of the users for specific resources and data and determining
whether the request should be granted or denied. The access control system is a combination of access
control policy, model and mechanism. Access control may be based on user’s identity or role or the
regulatory constraints as defined by the system administrator. Credential based access control grant or
deny access to the resources by exploiting digital certificates and make access decisions on the basis of a
set of properties that the client should have fulfilled. This trust negotiation process may suffer from
privacy problem since the server discloses its access control policy entirely and the client exposes its
credentials certificates to gain access to a resource. An efficient negotiation strategy should restrict the

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 77
disclosure of information. The service accessibility rules specify the necessary and sufficient conditions for
accessing a resource while credential disclosure rules define the conditions that govern the release of
credentials and declarations. The server should discloses the minimal set of policies for granting access
while the client releases the minimal set of certificates to access the resource. Prerequisites are the
conditions that must be satisfied for a service request. Requisites are conditions that allow the service
request to be successfully granted. The server should not disclose a requisite rule until the client satisfies
a prerequisite rule. Biometrics can be also used for credential based access control of distributed
computing systems.
Agents: Client (C), Healthcare system server (S);
check the correctness of enrollment and recognition mechanisms for biometric access control;
C requests S for the access to a resource r such as data or application;
S requests C for prerequisites;
C informs prerequisites to S;
S requests for requisites to C;
C informs requisites to S;
S verifies the credentials provided by C;
if the verification is true, then S grants C the access to r;
else S asks C the required credentials;
C selects the requested credentials (if possible) and informs S;
S verifies the credentials of C;
if the verification is true, then S grants C the access to r;
else S rejects the request of C;
intrinsic failure: check false match, non-match and failure to enroll or acquire biometric data;
adversary attacks: check collusion, coercion, negligence, enrollment fraud, exception abuse;
infrastructure attacks: check sabotage overloading, attacks on user interface, system modules, databases
and interconnections, modification of data and information leakage, spoofing, impersonation, man in the
middle attack, replay and hill climbing.
Figure : Biometric Access Control Mechanism
Credential based access control strategy grants or denies access to the resources based on
biometric prerequisites and requisites as specified by the client during trust negotiation
process.
The biometric access control mechanism verifies the security intelligence of a biometric access control
system associated with healthcare information system. It basically explores the risks of various threats on

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 78
biometric access control. A user presents his or her biometric identity to a biometric system for the
purpose of being recognized. Biometric systems can be used efficiently for authentication, nonrepudiation
and identity recognition claim. Biometric recognition is the science of establishing the identity of the user
based on his or her physical and or behavioral characteristics either in fully automated or a semi-
automated way. A biometric system measures one or more physical or behavioral traits such as finger
print, palm print, face, iris, retina, ear, voice, signature, gait, hand vein, odor or DNA information of an
individual to determine or verify his identity. These characteristics are known as traits, indicators,
identifiers or modalities. The biometric mechanism has two phases – enrollment and recognition. During
enrollment, biometric data is acquired from the individuals and stored in a database along with the
person’s identity. During recognition, biometric data is acquired from the individual and compared with
the stored data to determine the identity of the user.
The failure to a biometric system is basically a security threat - denial of service (DoS), intrusion,
repudiation and function creep. The legitimate users may be prevented from obtaining access to the
information assets. An unauthorized user may gain illegitimate access to the system and this intrusion
affects the basic integrity of the system. A legitimate user denies the usage of system or data after
having access to it. Corrupted users may deny their actions. An adversary may exploit the biometric
system for different function. The biometric system may fail due to flaws in enrollment and recognition
mechanisms. It may also fail due to manipulation by adversaries which could either be insider or external
entities. External entities may be imposters and attackers. Insiders may be system administrators or
legitimate corrupter users. Insider attacks may be collusion, coercion, negligence, enrollment fraud and
exception abuse. Infrastructure attacks may be due to sabotage overloading; it may be attacks on user
interface, system modules, interconnections and template databases. Attacks on user interface result
impersonation spoofing alternation. Attacks on system modules cause modification and exploit faults.
Attacks on interconnections cause man-in-the-middle, replay or hill climbing. Attacks on template
database result modification and leakage of critical sensitive data.
An adversary may attack human element or system infrastructure associated with a biometric system.
The system administrators may do mistakes in enrollment, disenrollment of users or in adjustment of
security parameters controlling the performance of a biometric system such as threshold on match scores
and minimum limits on the quality of acquired biometric sample. The administrator may do mistakes and
breach the security of biometric system. In case of collusion, an authorized user willingly turns malicious
and attacks the system either individually or in collaboration with external adversaries. A coerced user
does not carry out any attack willingly. An authorized user is forced to turn malicious through physical
threat or blackmail. External attackers can also exploit the negligence of authorized users such as log out
of the system after completing transactions. In case of enrollment fraud, an adversary may be able to
enroll into the biometric system illegally with a false identity and credentials. The system administrator
should detect a duplicate identity by matching the biometric traits of a new user against the traits of all

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 79
enrolled users. Another critical issue is exception abuse where exceptional situations may cause denial of
service to legitimate users. It may be the failure of hardware and software components of a biometric
system or poor quality of data (e.g. noise, missing data) during enrollment phase.
An adversary may attack the functional modules of a biometric system infrastructure such as sensor,
extractor, template database, matches or attacks at the interface of the modules and decision modules.
The common types of attacks are overloading and sabotage. A malicious agent may cause physical
damage to one or more components of the biometric infrastructure such as putting off power supply,
damaging of sensor interfaces or introducing excessive noise that affects the normal operation of
biometric system. An imposter may attempt to intrude the biometric system by posing himself as an
authorized user either casually or targeted way. The imposter does not modify his biometric traits in the
first case. In the second case, the imposter may target an identity whose biometric characteristics are
known to be similar to its traits. The imposter may execute mimicry attack by modifying his biometric
characteristics. It may adopt the strategy of obfuscation by changing biometric characteristics to avoid
detection. It is mainly applicable in negative recognition applications. Obfuscation can be done by
presenting a poor quality image or noisy biometric sample. The solution is to improve the robustness of
biometric algorithm.
Spoofing is the most common attack at user interface level and it involves the presentation of spoof
biometric trait. A spoof is any counterfeit biometric that is not obtained from a live person. It includes the
presentation of fake or artificial traits such as gummy finger, thin film on the top of a finger, recorded
voice or mask of a face. If the sensor is unable to distinguish between spoofed and genuine biometric
traits, an adversary can easily intrude the system under a false identity. Spoof detection is done through
liveness detection by checking the signs of human vitality or liveness through blood pulse. Spoofing can
be done by directly colluding with or coercing an authorized user, covert acquisition, hill climbing attacks
or stealing the biometric template from the database. For spoof detection, common psychological
properties used include pulse rate, blood pressure, perspiration, spectral or optical properties of human
skin, electrical conductivity of human tissues and skin deformation. A malicious agent can subvert
biometric processing by directly undermining the core functional modules of a biometric system such as
signal processing or pattern making algorithms or by manipulating the communication between these
modules. Template database can be hacked or modified by an adversary to gain unauthorized access or
to deny access to legitimate users. There may be leakage of stored biometric template information due to
lack of strict database access control.
The biometric system is a costly option in information security management; it requires complex data
schema in terms of data warehousing and data structure. It ensures non-repudiation authentication and
integrity, only legitimate or authorized users are able to access physical or logical resources protected by
it. The imposters can not access the protected resources or information. Another important issue is
availability where authorized users must have timely and reliable access to the protected data. It also

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 80
ensures confidentiality; it must be used for the intended functionality i.e. credential based access control.
A user can be recognized by what he knows (e.g. passwords, PIN or cryptographic key), what he
possesses (e.g. passport, driving license, mobile phone, ID card) and who he is intrinsically (e.g. inherent
physical and behavioral characteristics). The proliferation of web based services and deployment of
distributed computing systems have led to the risks of identity theft significantly. Facial recognition
software, voice recognition system and digital fingerprint or palm scanning are emerging trends of
biometrics. The traits such as fingerprints, retina, vein patterns and facial dimensions are generally
considered unique user profile but these features may be associated with a fake user ID intentionally or
by mistake during registration process. Biometric data management should take care of user privacy and
institutional convenience simultaneously.
6.4 Inference Control
Agents: Client (C), Healthcare system administrator (A);
Input: Query for sensitive patient data (q);
Output : Private data (dps);
CA: q;
A: Retrieve patient data (ds); Call move (Mi) for privacy preserving data mining;
M1: Suppress ds partially;
M2: Randomize ds;
M3: Achieve k-anonymity through generalization, suppression, de-identification;
M4: Summarize or aggregate ds;
M5: Replace ds with a small sample;
A C: dps ;
Verify the performance and efficiency of algorithms: encryption, decryption, digital signature, digital
certificate, signcryption;
Verify the degree of information leakage in inference control.
Figure : Inference Control Mechanism
A client interacts with the healthcare information system administrator through enterprise applications or
web; submits simple or complex queries and searches for intelligent information. A malicious agent may
be able to attack the server during this communication between sending and receiving agents. The
inference control mechanism tries to protect sensitive data from unsolicited or unsanctioned disclosure of
patient’s medical data by calling different statistical disclosure control and privacy preserving data mining
techniques. The privacy of sensitive patient’s data may be preserved by suppressing the data intelligently
before any disclosure or computation. Specific attributes of particular records may be suppressed

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 81
completely. In case of partial suppression, an exact attribute value is replaced with a less informative
value by rounding or using intervals. K-anonymity is achieved through generalization, suppression and
de-identification. The attribute values are generalized to a range to reduce the granularity of
representation. Quasi-identifier attributes are completely or partially suppressed. De-identification is
achieved by suppressing the identity linked to a specific record or altering the dataset to limit identity
linkage. Summarization releases the data in the form of a summary that allows approximate evaluation
of certain classes of aggregate queries while hiding individual records. The sensitive data set may be
replaced with a small sample. Aggregation presents data in the form of sum, average or count.
Randomization perturbs the data randomly before sending them to the server and introduces some noise.
The noise can be introduced by adding or multiplying random values to numerical attributes. The system
administrator generally preserves the privacy of sensitive data through encryption, decryption, digital
signature and certificates and signcryption. PVM checks whether different statistical disclosure control
techniques are really able to preserve the privacy of sensitive DCS data from the adversaries during
communication with the client through web or different enterprise applications.
The mechanism allows the service consumer and healthcare service provider to verify the
fairness and correctness of transactions through an efficient dispute resolution protocol.
Dispute resolution is a critical issue of patient care, strategic sourcing, accounts payable and receivables
management and contracts negotiation in healthcareflow mechanism. If the trading agents violate the
regulatory compliance of the mechanism, a trusted entity should resolve the issues of dispute and ensure
the credibility, reliability and robustness of the mechanism. The service consumer verifies the fairness
and correctness of invoice computation before clearing the payment to the service provider. The disputes
may occur among multiple tiers of the healthcare supply chain such as between tier 1 and tier 2 or tier 2
and tier 3 or tier 3 and 4/5/6 (Figure 1).
In case of accounts payable management, the receipt of an invoice from a vendor triggers the invoice
verification process. The procedure involves a three way match between purchase order, goods receipt
note and invoice. If the quantity and price of the three documents match, the payment will be paid to the
vendor as per payment terms. If there is any mismatch, the invoice will be blocked. The account payable
associate investigates the disputes; takes the necessary corrective action and unblocks the invoices. If
the vendor does not accept the recommendations of accounts payable management system, a third party
trustee should review the fraud case and should verify the contract between the healthcare service
provider and the vendor. The rating of the vendor may be reevaluated on the basis of such disputes and
the vendor may be blacklisted for any malicious business practice.
In figure 8, Alice sends a contractual message m to Bob. Bob can verify that the message is sent by Alice
since the public key of Alice is used for verification. The public key of Alice can not verify the signature

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 82
signed by the private key of any other malicious agent. The scheme also preserves the integrity of the
message. If a message is altered during communication, the receiver can detect this change. Another
important issue is non-repudiation. If Alice signs a message and then denies it, Bob can prove that Alice
signs the message. A trusted center (TC) resolves any dispute. Alice creates a signature from her
message and sends the message, her identity, Bob’s identity and the signature to TC. TC verifies the
source of the message using Alice’s public key. TC saves a copy of the message with the identity of Alice,
the identity of Bob and a timestamp. TC generates a new signature from the message using its private
key and sends the message, the new signature, Alice’s identity and Bob’s identity to Bob. Bob verifies the
message using the public key of TC and his private key. In future, if Alice denies that she is the sender of
the message, TC can show a copy of the saved message. Alice will lose the dispute if the message
received by Bob is the duplicate of the message saved by TC.
Figure 8. Dispute resolution protocol
The healthcare information system is expected to be a resilient system. The resiliency measures the
ability to and the speed at which the system can return to normal performance level following a
disruption. Real-time security management involves high cost of computation and communication. The
vulnerability of HIS to a disruptive event should be viewed as a combination of likelihood of a disruption
and its potential severity. The HIS administrator must do two critical tasks: assess risks and mitigate the
assessed risks. To assess risks, the system administrator should explore basic security intelligence: what
can go wrong in HIS operation? what is the probability of the disruption? how severe it will be? what are
the consequences if the disruption occurs? A HIS vulnerability map can be modeled through a set of
expected risk metrics, probability of disruptive event and the magnitude of consequences. For example,
the map has four quadrants in a two dimensional space; the vertical axis represents the probability of
disruptive event and the horizontal axis represents the magnitude of the consequences.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 83
The system administrator faces a set of challenges to solve the problem of resiliency: what are the critical
issues to be focused on? what can be done to reduce the probability of a disruption? what can be done to
reduce the impact of a disruption? How to improve the resiliency of the healthcare information system?
The critical steps of risk assessment are to identify a set of feasible risk metrics; assess the probability of
each risk metric; assess severity of each risk metric and plot each risk metric in HIS vulnerability map.
The critical steps of risk mitigation are to prioritize risks; do causal analysis for each risk metric; develop
specific strategies for each cell of vulnerability map and be adaptive and do real-time system monitoring.
The security consultant has proposed a roadmap for digital defense of healthcare information system.
Figure 9: Digital Transformation Security Roadmap
E-health system faces critical legal, ethical and psychological issues from the perspectives of security,
privacy, confidentiality and organizational policy. Security and privacy of data is important from the
perspectives of access control, data storage, version control of critical applications, accountability,
traceability and transparency E-healthcare information should be managed in a digital environment
through efficient security principles, privacy laws and policies in the domain of shared and managed care.
Shared care is a healthcare service that is delivered at multiple locations and by multiple service providers
through sharing of the medical information of the patients. Managed care is characterized by cost
reduction and quality enhancement techniques practiced by either healthcare service providers or
insurance companies. Both paradigms require secure exchange of patient’s private data through internet.
Pseudonymisation and anonymisation may be good techniques for distributed e-health system.
Compliance requires a good security policy for a set of standards for data acquisition, storage,
communication, authentication and authorization. The CIO and security analysts have pointed out the
critical challenges of security schema such as law, policy, standards, human factors and data exchange.
It is really complex to manage the issues of mandatory disclosure, mapping to formal technical
specification, legal and compliance factors, trust, patient’s consent, identity theft, confidentiality
breaches, theft of hardware, electronic interception of exchanged data, accidental disclosure and
dissemination. Patient’s data privacy and the sharing of healthcare data may result disputes. The law
seeks to protect patient privacy. Many standards support exchange of patient’s data. Law and standards
should cooperate and complement each other in privacy protection.
Identify the scope of digital defense, define objectives, constraints and allocate optimal budget
Maintain and upgrade security schema for a resilient healthcare information system
Deploy security solutions for trusted computing, data, networking and application schema
Develop a set of verification mechanisms for security intelligence
Call threat analytics: assess risks, mitigate risks and define security policy
Identify digital technology assets and computevaluation of the assets

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 84
Chapter 7 : Information Management Schema
7.1 Organization Structure
The business analysts have developed intelligent organization structures for digital transformation. The
digital technology department is governed by the Chief Manager. The managers of information,
communication and biomedical engineering report to the Chief Manager. The analysts of application,
data, security, computing and system maintenance report to the information technology manager. The
system department is responsible for management of digital technology i.e. information, communication
and biomedical instrumentation, DT investment analysis and DT portfolio optimization. The Chief
Manager coordinates with finance, innovation and HR departments.
The whole organization is governed by the Chief Executive Officer (CEO) who looks after corporate
strategy and policy formulation and overall coordination among various departments. The Chef Managers
of digital technology (CIO), finance (CFO), healthcare operations, HR and Innovation departments report
to the CEO. The Mangers of registration, admission and discharge, healthcare consultants and surgeons,
supply chain coordination, test lab, nursing, billing and payment processing report to the Chief Manager,
Healthcare Operations. The finance department is responsible for financial and cost accounting, pricing,
revenue management budget planning, capital allocation and project management. The innovation
department has separate cells for business consulting, technology consulting and research on medical
science. The medical science cell manages the administration of academy of medicine. The supply chain
manager controls supply chain planning, collaboration and execution, purchasing, warehousing, quality
control and inspection and transportation functions. The HR department is responsible for talent
acquisition, training, performance evaluation, career growth planning, reward and retirement planning.
Figure 10 : Organization Structure of Healthcare Service Provider
The Chief Executive(CEO)
The Chief Manager Digital
Technology
The Chief Manager
Innovation(R&D)
The Chief Manager Human
Resources
The Chief Manager
HeathcareOperations
The Chief Manager Finance(CFO)
Billing & Payment
ProcessingManager
Test Lab & Nursing Manager
Supply chain Manager
HealthcareConsultants &
Surgeons
Registration Admission &
DischargeManager

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 85
Figure 11 : Organization Structure of Digital Technology Department
7.2 Investment Analytics for Digital Technology Portfolio Optimization
The healthcare service provider needs financial investment analytics for digital technology
portfolio optimization.
The CIO and CFO have jointly discussed various options of financial investment for digital transformation.
The options are transformation, renewal, process improvement and experiment. The drivers for
transformation are the core technology schema not suitable for modern healthcare business model.
Executive level fund allocation is required for ERP and business intelligence system implementation and
the whole enterprise may be the owner of the project. The drivers of system renewal are obsolete
outdated technology, threat of new technology, cost reduction and improvement of quality of service.
Business case based funding approach is required by CIO for the replacement old obsolete technology
and purchasing of new technology. The owner of the project is a specific service unit. The drivers of
process improvement are the opportunities to improve business performance and operational excellence.
Strategic business unit and process owner own the project through business case based funding
approach for automation and streamlining of business processes. The drivers of various types innovative
experiments are the new technology (e.g. SMAC), product, process and business model. IT unit and
functional head own these projects through business level and executive level allocation. The system and
business analysts have identified the priority of various types of projects. Experimental projects are
needed for SMAC technology, HCI and smart home; ERP, E-health and m-health projects are important
for digital transformation and process improvement. The old word processing and spreadsheets systems
should be renewed to manage large amount of complex transactional data.
The Chief Manager Digital Technology
Manager InformationTechnology
Manager CommunicationTechnology
Manager Biomedical Engineering
ApplicationAnalysts
DataAnalysts
SecurityAnalysts
ComputingAnalysts
SystemMaintenance

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 86
Figure 12: IT investment analysis
7.3 Strategic Roadmap of Digital Transformation Project
The top management are interested in investment on value adding digital technology and
bioinstrumentation. They are interested to adopt a rational fund allocation approach through systematic
project management, planning, monitoring and effective coordination among various units and
departments. The fundaments steps of any digital technology project involve scope analysis, business
process mapping in terms of analyze as-is process, gap analysis and design to-be process, program
planning and project team formation, selection of application schema like products, modules, vendors
and consultants, selection of computing schema, hardware sizing and networking schema, master
database configuration, customization of reports, screens and interfaces, system and user acceptance

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 87
testing, user training, migration to the new system, system monitoring and performance optimization.
The CIO has proposed a cross functional project team for digital transformation comprising business and
technical analysts, consultants, researchers and users. There are various options of system
implementation approaches such as big bang, phased, selective modular and pilot implementation. The
top management would like to adopt phased approach for digital transformation. The CIO has presented
a list of critical success factors of digital transformation projects to the top mangement.
Understand corporate culture in terms of readiness and capability for change.
Begin business process changes prior to implementation.
Communicate continuously with all levels of new users in business, not only technical terms. Set
reasonable expectations.
Obtain top executive sponsorship for the project.
Ensure the project managers are capable of negotiating equally between the technical, business
and change management requirements.
Choose a balanced team and provide it with clear role definitions.
Select a good proven project methodology with performance measurements.
Evaluate vendors and consultants carefully. Be sure that the software more-or-less fits your
organizational requirements and the consulting firm has delivery capabilities.
Train users and provide support for job changes.
Remain alert for political influences on the project and deal with them appropriately.
Ensure process team’s ownership of the process during implementation.
7.4 Rural Healthcare
Digital transformation is not only applicable to urban healthcare system, but also important for rural
healthcare. Rural healthcare faces various types of constraints such as non-availability of drugs in time
due to lack of supply chain coordination, old and obsolete information and communication technology
infrastructure, poor quality of service and outcome due to operational and administrative failure,
malnutrition of mothers and children, poor healthcare programme management, flawed HR model with
poor incentives, nonavailability of knowledge management system and performance scorecard and lack
of skilled healthcare experts. Rural healthcare system may fail to deliver quality of service due to lack of
proper infrastructure, skill, medical errors, hospital acquired infection and suffering from injury illness as
a consequence of treatment and surgical operations. Regularity compliance and economic incentives can
improve the commitment of the rural healthcare service providers. The rual healthcare system needs
efficient mechanism which can reward the health specialists based on patient’s outcome instead of
number of patients treated. The system requires improvement in lowering infections, primary care,
nursing care, medication administration and the improvement of clinical and nonclinical processes. It has

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 88
direct impact on safety, quality, efficiency, reliability and timeliness of healthcare. The system also
requires good coordination mechanisms for complex treatment procedure and good performance of the
healthcare workforce. They need good medical practice and standards. They should be clear about their
tasks that must be done; who should be doing what and how to perform that task. Typically, care is
organized around different functions and those function need proper coordination and integration. The
rural healthcare system needs a group of bright, dedicated and skilled workforce. The rural healthcare
also needs disruptive innovations through proper integration among insurers, regulators, managed care
organizations, hospitals and health specialists. Instead of following old practice, the system
administrators should ask how they can enable or facilitate disruptive innovations to emerge.
Digital transformation is an innovative approach to ensure fairness, correctness and good outcome in
rural healthcare system. The top management have asked the CIO and his team and also innovation cell
to explore critical problems of their rural healthcare units. Is it possible to organize care into integrated
practice units around patient medical conditions, measure outcomes and costs, reimburse flexibly through
combinatorial pricing scheme for care cycles, integrate care delivery across separate facilities, expand
areas of excellence across villages and create an enabling information and communication technology
platform?
Conclusion
The algorithmic mechanisms and protocols presented in this work assumes that the agents act rationally
to achieve their objectives and follow the protocols correctly with correct inputs. They are effective in a
trusted service oriented computing environment. It is an emerging cross-disciplinary paradigm of
distributed computing that is changing the design pattern and architecture of complex information
system. A set of autonomous service components act in a collaborative computing environment. The
mechanisms and protocols do not study any malicious behavior of the trading agents and specific types
of administrative inefficiencies which can disrupt normal healthcare service. It includes the collusion of
the trading agents against regulatory compliance, financial fraud in e-transactions, quality problems in
testing and sourcing, non-availability, poor performance and failure of medical equipments, malicious
work culture, medical negligence, unauthorized absence (excluding casual leave, earned leave and
medical leave), excessive work load, strikes and physical security problem of healthcare service provider.
The healthcare workforce expect to work freely in a collaborative, flexible and ethical work culture
without any financial, physical, mental and cultural constraints and pressures.
Globally healthcare organizations are undertaking massive business process reengineering initiatives and
many of these reforms are supported by the strategic use of advanced information and communication
technology. The proposed outline of digital transformation should provide better integration and
improved coordination of flows of material, information and funds within and across healthcare firms,

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 89
experts and patients. This results improved patient care, greater accuracy, cost efficiency, ease of
processing, increased productivity and fast response time in healthcare service. Service oriented
computing results improved interoperability, increased federation, and organizational agility through a
standardized, flexible, reliable and scalable architecture. An intelligent mechanism should explore other
strategic moves such as medical education technology, corporate social responsibilities, integrated
healthcare networks, childcare, improved monitoring system, RFID, GPS, video-conferencing, virtual
patient visit, telemedicine, real-time human computer interaction, bio-sensors, biotechnology, bio-
instrumentation, bio-informatics and effects of environmental pollution (e.g. air, water, soil, sound,
sunlight) and climate change for improved quality of service at reasonable cost.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 90
References
A.K.Jain. Biometric recognition. Nature, 449:38-40. 2007.
B.Schneier. Applied Cryptography. John Wiley, New York,1996.
C.Ferran and S.Watt. Videoconferencing in the field: A heuristic processing model. Management Science,
volume 54, no. 9, September, 2008, 1565 - 1578.
C.McGregor and J.M.Eklund. Real-time Service-oriented architectures to support remote critical care:
trends and challenges. Annual IEEE International Computer software and applications conference,2008.
D.B.Leake (editor). Case based reasoning experience, lessons and future directions. AAAI Press / MIT
Press,1996.
D.Kim. An integrated supply chain management system: a case study in healthcare. volume 3590,
Lecture Notes in Computer Science, Springer,2005.
D. Seifert. Collaborative planning, forecasting and replenishment. Galliers Business,2002.
F.Kart, G.Miao, L.E.Moser and P.M.Melliar-Smith. A distributed e-healthcare system based on the service
oriented architecture. IEEE International Conference on Services Computing, 2007, pp.652-659.
G.Anandalingam, R.W.Day and S.Raghavan. The landscape of electronic market design. Management
Science, 51(3), 2006, pp. 316-327.
G.Ateniese, R.Curtmola, B. Medeiros and D.Davis. Medical information privacy assurance: Cryptographic
and system aspects. Technical Report, John Hopkins University,2003.
G.Ateniese and B.Medeioros. Anonymous E-prescription, Proceedings of ACM Workshop on Privacy in the
Electronic Society,USA,2002.
G.Ateniese, M.Joye, J.Camenish and G.Tsudik. A practical and provably secure coalition resistant group
signature scheme. Advances in cryptology, Crypto’00, Volume 1880, LNCS, Springer Verlag, 2000, pp.
255-270.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 91
G.Kramer, I.Meric and R.D.Yates. Cooperative communications. Foundations and trends in networking,
volume 1, no. 3-4, 2006, 271- 425.
G. Peterson. Service oriented security architecture. Information Security Bulletin, vol.10,2005.
J.L.Kolodner. Case based reasoning. Morgan Kaufmann. CA.1993.
J.L.Kolodner. An introduction to case based reasoning. Artificial Intelligence Review, 6(1):3-34,1992.
J.L.Kolodner and W.Mark. Case based reasoning. IEEE Expert, 7(5):5-6,1992.
http://www.owasp.org accessed on 15.08.2008.
I.Watson. Applying Case-based reasoning: Techniques for enterprise systems. CA. 1997.
J.Emanuele and L.Coetter. Siemens Medical Solutions, USA. Workflow opportunities and challenges in
healthcare. www.usa.siemens.com/medical. 2007.
J.Kalvenes and A.Basu. Design of robust business-to-business electronic marketplace with guaranteed
privacy. Management Science, 11, 2006, pp. 1721-1736.
J.Liebowitz. Knowledge management handbook. CRC Press,1999.
J. Y. Kim, P. Farmer, M. E. Porter (2013). Redefining global healthcare delivery, The Lancet. 2013
May 20, 2013
K.Althoff, R.Bergmann and L.K. Branting. Case based reasoning research and development. Proceedings
of 3rd International Conference on Case Based Reasoning, Germany, 1999.
K. Ramdas, E. O. Teisberg, A. L. Tucker. Four Ways to Reinvent Service Delivery. Harvard Business
Review. December, 2012.
K. Sayood. Introduction to Data Compression. 3rd ed. Morgan KauVman Publishers, 2006.
M.Alavi and D.E.Leidner. Review: Knowledge management and knowledge management systems:
Conceptual foundations and research issues, MIS Quarterly Review. Volume25, March’2001

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 92
M. Armburst et al. A view of cloud computing, Communications of the ACM, 53(4), 50-58. 2010.
M.Beyer, A.Kuhn, C.Meiler, S.Jablonski and R.Lenz. Towards a flexible process oriented IT architecture for
an integrated healthcare network. Proceedings of ACM Symposium on Applied Computing, 2004, pp. 264-
271.
M.C.Reddy, S.Purao and M.Kelly. Developing IT infrastructure for rural hospitals: A case study of benefits
and challenges of hospital-to-hospital partnerships. Journal of American Medical Inform Association, vol.
15, 2008,pp. 554-558.
M. Fitzgerald, N. Kruschwitz, D. Bonnet and M. Welch. Embracing Digital Technology A New Strategic
Imperative, MIT Sloan Management Review, Research report, 2013.
M. E. Porter, E. A. Pabo and T.H.Lee. Redesigning Primary Care: A Strategic Vision To Improve Value By
Organizing Around Patients' Needs. Health Affairs. 2013.
M.E.Porter and E.O.,Teisber. Redefining healthcare Creating Value-Based Competition on Results.
Harvard Business School Press, 2006.
M.K.Bourke. Strategy and architecture of healthcare information systems, Springer,1994.
M.K.Franklin and M.K.Reiter. The design and implementation of a secure auction service. IEEE
Transactions Software Engineering, 22(5), 1996, pp.302-312.
M.Gertz and S.Jajodia. Handbook of database security applications and trends. 2008.
M. Rosen, B.Lublinsky, K.T. Smith and M.J. Balcer. Applied SOA Service oriented architecture and design
strategies. Wiley India,2008.
M.Subramanian, A.S. Ali, O. Rana, A. Hardisty and E.Conley. Healthcare@Home: Research models for
patient centered healthcare services. Proceedings of International symposium on Modern Computing,
2006, pp. 107-113.
O. Goldreich. Foundations of Cryptography, Basic Applications. Volume 2. Cambridge University Press.
2004.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 93
P.Bonatti and P. Samarat. A unified framework for regulating access and information release on the web.
Journal of Computer Security 10(3) (2002) 241-272.
P.N.Tan, M.Steinbach and V. Kumar. Introduction to data mining. Pearson, Addison-Wesley. 2006.
P. Weill and S. L. Woerner, Optimizing Your Digital Business Model, MIT Sloan Management Review,
Spring 2013, Volume 54, No. 3.
R.Buyya, R., C.S.Yeo, S.Venugopal, j. Broberg,J. and I.Brandic. Cloud computing and emerging IT
platforms: Vision, hype and reality for delivering computing as the 5th utility. Future generation computer
systems. 2009.
R.Bottle, J.Konnell, S.Pankanti, N.Ratha and A.Senior. Guide to Biometrics. Springer. 2003.
R.McAdam and S.McCreedy. A critical review of knowledge management models. The Learning
organization, volume 6, No. 3, 1999, 91-100
R.S.Sriram, V. Arunachalam and D.M.Ivancevich. EDI adoption and implementation an examination of
perceived operational and strategic benefits and controls. Journal of Information Systems Spring, 14(1),
2000, pp. 37-52.
S. Chakraborty. A study of several privacy-preserving multi-party negotiation problems with applications
to supply chain management. Doctoral dissertation (unpublished), Indian Institute of Management
Calcutta. 2007.
S. Chaudhuri. An overview of query optimization in relational systems. ACM PODS 1998.
S.Chaudhuri, S. and U.Dayal. An overview of data warehousing and OLAP technology. SIGMOD Record
26, 1 (1997).
S.Chaudhuri, S., U. Dayal, U. and V. Ganti. Database technology for decision support systems. IEEE
Computer 34, 12 (2001).
S. Chaudhuri, S. and V.Narasayya. Self-tuning database systems: a decade of progress. In Proceedings of
VLDB 2007.

Author : Sumit Chakraborty; Reference : HSIDT/ V1.0/ CR 15082014 Page 94
S.G.Stubblebine, P.F. Syerson and D.M.Goldschlag. Unlinkable serial transactions: protocols and
applications. ACM Transactions Information System Security, 2(4), 1999, pp. 354-389.
S.Johnson. Modeling security concerns in service oriented architecture, 2004.
S.K.Sharma, H. Xu, N.Wickramsinghe and N.Ahmed. Electronic healthcare: issues and challenges.
International Journal Electronic Healthcare, 2(1),2006.
S.Prabhakar, S.Pankanti and A.K.Jain. Biometric recognition: security and privacy concerns. IEEE security
and privacy magazine. 1(2):33-42, March - April. 2003
T. Earl. SOA Principles of service design. Prentice Hall,2007.
T.J.Parenty. Digital defense what you should know about protecting your company’s assets. Harvard
Business School Press. 2003.
W.M.Omar and A.Taleb-Bendiab. Service oriented architecture for e-health support services based on grid
computing. Proceedings of IEEE International Conferences on Service Oriented Computing, 2006, pp.
135-142.
W. Mao Modern Cryptography Theory & Practice. Pearson Education,2007.
Y. Lindell and B. Pinkas. Privacy preserving data mining. In Advances in Cryptology - Crypto 2000, LNCS
1880. 2003.
Y. Lindell. Composition of secure multi-party protocols a comprehensive study. Springer. 2003
Y.Zheng. Digital signcryption or how to achieve cost (signature & encryption) << cost (signature) + cost
(encryption). Lecture Notes in Computer Science, vol. 1318, Springer-Verlag.
Book price : Rs. 5000