Health Questionnaire for Eight Cranes Acupuncture, LLC · PDF file ·...
8
Page 1 of 8 Health Questionnaire for Eight Cranes Acupuncture, LLC This is a confidential questionnaire that is intended to help provide the best treatment for you. If you have any questions, please feel free to ask. Thank you. New Patient Intake Form Date Primary Phone # ______ ______Alternate Phone # __________________ Last First Middle Name Preferred Name Age Date of Birth / / Place of Birth Primary Insurance Holders Name________________________________ Date of Birth_____________________ Height Weight Gender Occupation Address City State Zip E-mail address Referred by Emergency Contact (Name, Phone # & Relationship) Are you under the care of a physician now? □Yes □ No If yes, for what? Physician’s Name Type (ND, DO, MD) Phone # Other Health Care Providers (name, type, phone #) Have you ever been treated with Acupuncture and its related modalities before? □ Yes □ No Have you ever taken Chinese Herbal medicines before? □ Yes □No Main Problem (s) that you would like to be treated for: How Long ago did this problem(s) begin (be specific)?
Transcript of Health Questionnaire for Eight Cranes Acupuncture, LLC · PDF file ·...

Page 1 of 8
Health Questionnaire for Eight Cranes Acupuncture, LLC This is a confidential questionnaire that is intended to help provide the best treatment for you. If you have any questions, please feel free to ask. Thank you.
New Patient Intake Form Date Primary Phone # ______ ______Alternate Phone # __________________
Last First Middle Name Preferred Name
Age Date of Birth / / Place of Birth
Primary Insurance Holders Name________________________________ Date of Birth_____________________
Height Weight Gender Occupation
Address City State Zip
E-mail address Referred by
Emergency Contact (Name, Phone # & Relationship)
Are you under the care of a physician now? □Yes □ No If yes, for what?
Physician’s Name Type (ND, DO, MD) Phone #
Other Health Care Providers (name, type, phone #)
Have you ever been treated with Acupuncture and its related modalities before? □ Yes □ No
Have you ever taken Chinese Herbal medicines before? □ Yes □No
Main Problem (s) that you would like to be treated for:
How Long ago did this problem(s) begin (be specific)?

Page 2 of 8
To what extent does this problem(s) interfere with your daily activities (work, sleep, etc.)?
Have you ever been given a diagnosis for this problem(s)? If so, what?
What kind of treatments have you tried?
Do you have any other health conditions that are causing you worry or discomfort?
Family Medical History (Please circle any conditions family members have had)
Asthma Alcoholism Cancer (type)
Diabetes (type) Epilepsy
High Blood Pressure Heart Disease Multiple Sclerosis Seizures Stroke Seizures Stroke
Thyroid Disease Other
Past Medical History (Please circle any conditions you have had, or are currently experiencing)
AIDS/HIV Alcoholism Arteriosclerosis Asthma Cancer Diabetes Deep Vein Thrombosis
Surgeries (type & date):
Epilepsy Heart Disease Hepatitis Herpes Lupus Lyme Disease High Blood Pressure
Menopause Multiple Sclerosis Pacemaker Rheumatic Fever Seizures Stroke Thyroid Disease
Tuberculosis Venereal Diseases Other (Specify:
Significant Trauma (auto accidents, falls, etc.):
Significant Dental Work:
Birth History (Prolonged labor, c-section, etc.):
Allergies:
Medications, Nutritional Supplements, Homeopathy, Herbs, etc. (please list type and dosage- continue on next page)
Page 3 of 8
Lifestyle Occupational Stress (physical, chemical, psychological, etc.)
Do you have a regular exercise program? □ Yes □ No Please describe
Have you ever been on a restricted diet? □Yes □ No What kind?
Please describe your average daily diet
Morning:
Afternoon:
Evening:
Do you have any cravings for particular foods or tastes? (please list)
How often are you thirsty?
How many packs of cigarettes do you smoke per day? How much coffee, tea, or energy drinks do you drink per day? How much alcohol do you drink per week? Please describe any use of recreational drugs
Symptomatology {Please check any that you have had in the last 3 months)
General □ Sweat easily □ Night sweats □ Localized weakness □ Body heaviness □ Bleed or bruise easily □ Peculiar tastes or smells □ Peculiar sensations (please
describe)
□ Strong thirst (cold or hot) □ Thirst, no desire to drink □ Sudden energy drop; what
time of day? □ Poor sleep
□ Dream disturbed sleep □ Chills □ Fevers □ Tremors □ Poor balance □ Fatigue □ Cravings □ Weight gain □ Weight loss □ Poor appetite □ Excessive appetite □ Prefer hot drinks □ Prefer cold drinks
Skin and Hair □ Rashes □ Itching □ Dandruff □ Change in hair or skin □ Ulcerations □ Eczema □ Psoriasis □ Loss of Hair □ Hives □ Pimples □ Recent moles □ Fungal infections □ Other hair or skin problems
Page 4 of 8
Head, Eyes, Ears, Nose, & Throat □ Dizziness □ Glasses □ Poor vision □ Cataracts □ Glaucoma □ Eye pain □ Color blindness □ Spots in front of eyes □ Eye strain □ Night blindness □ Blurry vision □ Poor hearing □ Earaches □ Ringing in ears □ Sinus problems □ Nose bleeds □ Teeth problems □ Grinding teeth □ Jaw clicks □ TMJ □ Gum problems □ Recurrent sore throats □ Sores on lips or tongue □ Facial pain □ Concussions □ Migraines □ Headaches - where and
when □ Other head or neck concerns
Cardiovascular □ High blood pressure □ Low blood pressure □ Irregular heartbeat □ Poor circulation □ Cold hands or feet □ Blood clots □ Swelling of hands □ Swelling of feet □ Phlebitis
□ Chest pain □ Fainting □ Difficulty in breathing □ Other heart or blood vessel concerns
Respiratory □ Cough □ Bronchitis □ Production of phlegm
what color? Thick or Thin (circle one)
□ Coughing blood □ Pneumonia □ Difficulty in breathing when
lying down □ Shortness of breath □ Asthma □ Pain with a deep breath □ Other lung concerns
Gastrointestinal □ Nausea □ Vomiting □ Acid reflux □ Constipation □ Blood in stools □ Black stools □ Bad breath □ Abdominal pain or cramps □ Chronic laxative use □ Gas □ Rectal pain □ Diarrhea □ Belching □ Indigestion □ Hemorrhoids □ Itchy anus □ Burning anus □ Other stomach or intestinal
concerns □ Bowel movements: (please describe your bowel movements)
Frequency Color Texture
Odor Other
Genito-urinary □ Pain on urination □ Urgency to urinate □ Frequent urination □ Unable to hold urine □ Blood in urine □ Kidney stones □ Sores on genitals □ Urinary tract infection □ Other genital or urinary
system concerns Do you wake up to urinate?
□ Yes □ No How often? Any particular color to your urine?
Andrology □ Impotency □ Prostatitis □ Difficult urination □ Seminal emission □ Premature ejaculation □ Groin pain □ Infertility □ Other
Pregnancy and Gynecology □ Number of pregnancies □ Number of births □ Premature births □ Miscarriages □ Abortions □ Age at first menses □ Days between menses □ Duration □ First day of last menses
What kind of flow?
□ Heavy □ Light □ Absent
□ Painful periods □ Vaginal discharge □ Changes in body/psyche prior to menstruation
Page 5 of 8
□ Clots □ Vaginal sores □ Irregular periods □ Last Pap □ Breast lumps Do you practice birth control?
□ Yes □ No What type and for how long?
Musculoskeletal □ Neck pain □ Back pain □ Hand/wrist pain
□ Muscle pain □ Muscle weakness □ Shoulder pain □ Knee pain □ Foot/ankle pain □ Hip pain □ Joint pain
Neuropsychological □ Seizures □ Areas of numbness □ Concussion
□ Bad temper □ Dizziness □ Lack of coordination □ Depression □ Easily susceptible to stress □ Loss of balance □ Poor memory □ Anxiety □ Other neurological or
psychological concerns
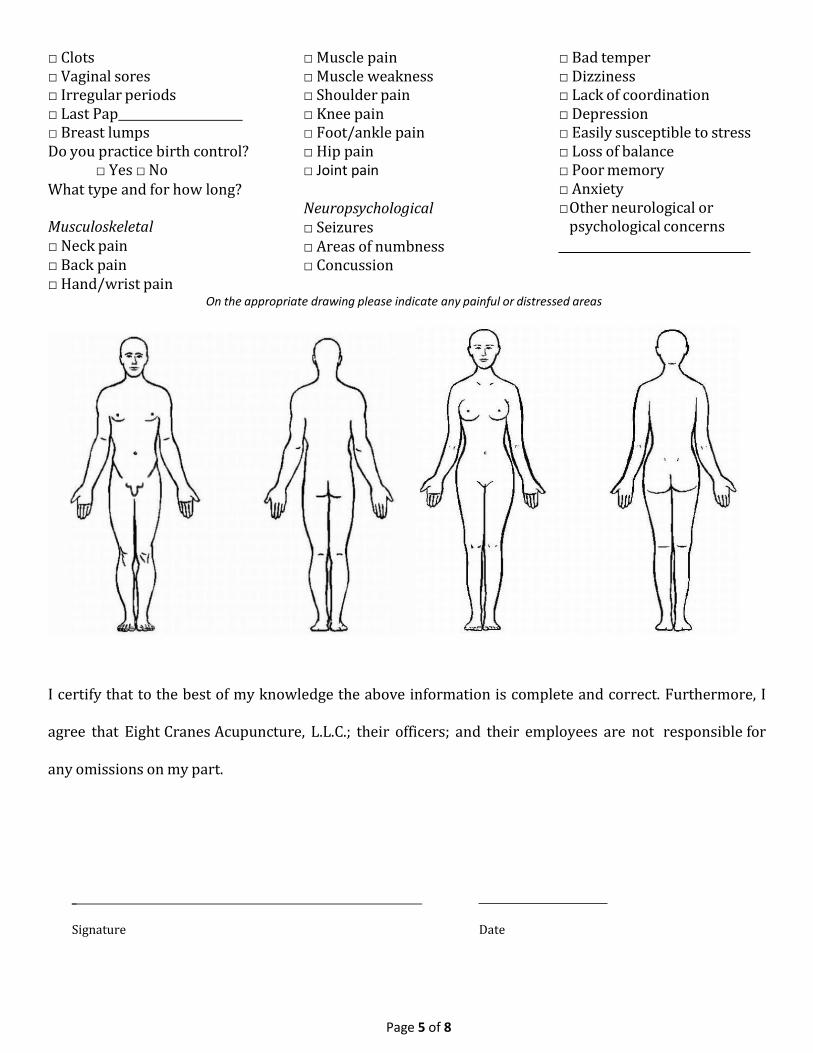
On the appropriate drawing please indicate any painful or distressed areas I certify that to the best of my knowledge the above information is complete and correct. Furthermore, I
agree that Eight Cranes Acupuncture, L.L.C.; their officers; and their employees are not responsible for
any omissions on my part.
_
Signature Date

Page 6 of 8
Eight Cranes Acupuncture, LLC 305 East 38th Street
Savannah, GA 31401
Specific Fee Schedule Information for New Patients
We adhere to a strict 24-hour cancellation or no-show policy. Each scheduled appointment cancelled with less than 24 hours notice will incur a $25 charge.
Telephone consultations lasting longer than 10 minutes will be billed at normal office rates. Current office rates as of January 2007 are $80 per hour, prorated in fifteen- minute increments. Office rates are subject to change.
Payments are due at time of service. Under extenuating circumstances, we may extend credit, but credit arrangements must be arranged before services are rendered.
Fees more than ninety days old may be submitted to a collections agency or litigated.
Informed Consent Waiver
I, the undersigned, do agree and consent to all care and services provided by Eight Cranes Acupuncture, LLC; Benjamin R. Brodhead, L.Ac, and the staff of said corporation. I understand that Eight Cranes Acupuncture, LLC is not a walk-in or emergency services clinic. In the event that an emergency care need arises, I realized that I must go to a medical facility qualified to treat such conditions. I understand that any services provided to me by Eight Cranes Acupuncture, LLC do not constitute those for life-threatening situations.
I agree to hold harmless and to indemnify Eight Cranes Acupuncture, LLC and its professionals and staff from any and all claims involving the care provided by the Eight Cranes Acupuncture, LLC. Further, I understand that Eight Cranes Acupuncture, LLC does not guarantee results and will not assure me of progress of any condition or conditions I may have. I further understand that programs and protocols employed by the that Eight Cranes Acupuncture, LLC may be those other than Standard of Care, and considered Complementary and Alternative Medicine (CAM).
I agree that payment is considered due, in full, at time of service. Payment may be made
by cash, check, or credit card.
I acknowledge that any questions that I have about this agreement have been fully explained to me and I understand its contents.
Patient’s signature: X Date_
Page 7 of 8
Eight Cranes Acupuncture, L.L.C. 305 East 38th Street
Savannah, GA 31401
SUMMARY OF (JOINT) NOTICE OF PRIVACY PRACTICES
Our legal duty: We have a legal duty to protect the confidentiality of medical information about you. We are required to provide you with a Notice of Privacy Practices explaining ways we may use and disclose your medical information.
Parties following this notice: This notice will be followed by Eight Cranes Acupuncture, LLC and its affiliates, together with their health care professionals, staff, and volunteers; members of the staff and participants in managed care networks with the Eight Cranes Acupuncture, LLC; and other legal entities that provide services to the Eight Cranes Acupuncture, LLC.
How we may use and disclose medical information about you: We may use or disclose identifiable medical information about you for many reasons, including:
Treatment Payment Health Care Operations Health Oversight Activities Auditing Public Health Purposes Worker’s Compensation Lawsuits and Disputes Activities of Managed Care Networks Activities of our Affiliates Follow-up Information Procedure Callbacks Otherwise As Required by Law
National Security and Protective Services Law Enforcement Purposes Organ Donation Fund Raising Coroners, Medical Examiners, and Funeral Directors Military Command Authorities
In general, other uses and disclosures of your medical information will require your written authorization.
Your privacy rights: You have the following rights with respect to your health information:
The right to request confidential communications and alternative means of communication. The right to request restrictions on certain uses of your health information. The right to inspect and to copy certain health information. The right to request an amendment of your health information. The right to an accounting of certain disclosures of your health information.
Changes to this notice: We reserve the right to change this Notice within the bounds of the law. We will post any revised notice in the Center.
Complaints: If you believe that your rights have been violated, you may file a written complaint with Eight Cranes Acupuncture, LLC or with the Secretary of the U.S. Department of Health and Human
Services.
ACKNOWLEDGEMENT
Printed Patient Name:
Patient Acknowledgement: I acknowledge that I have reviewed a copy of the Notice of Privacy Practices for Eight Cranes Acupuncture, LLC, and that I have had an opportunity to ask questions regarding the Notice and its contents.
Signature of patient: Date:
Page 8 of 8
PATIENT INFORMATION AND CONSENT FORM WHAT IS ACUPUNCTURE?
Acupuncture is a form of therapy in which fine needles are inserted into specific points on the body.
WHAT IS THE ROLE OF ACUPUNCTURIST IN GEORGIA? The Georgia Code 360-6-.16 states that an acupuncturist is not licensed to practice medicine in the
State of Georgia. Accordingly, an acupuncturist is not able to make a medical diagnosis of the
person’s disease. Therefore, if you are seeking to obtain a medical diagnosis, then you should see a
licensed physician and seek medical advice from a licensed physician.
DOES ACUPUNCTURE HAVE SIDE EFFECTS?
Acupuncture is generally very safe.
• Serious side effects are rare – less than one per 10,000 treatments
• Drowsiness occurs after treatment in a small number of patients
• Minor bleeding or bruising occurs after acupuncture in about 3% of treatments.
• Pain during treatment occurs in about 1% of treatments.
• Symptoms can get worse after treatment (less than 3% of patients). You should tell your
acupuncturist about this, but it is usually a good sign.
• Fainting can occur in certain patients, particularly at the first treatment. In addition, if there are particular risks that apply in your case, your practitioner will discuss these with
you.
IS THERE ANYTHING YOUR PRACTITIONER NEEDS TO KNOW? • If you have ever experienced a seizure, dizziness, or fainting episode
• If you have a pacemaker or any other electrical implants
• If you have a bleeding disorder
• If you are taking anti-coagulants or any other medications
• If you have damaged heart valves or have any other particular risk of infection
SINGLE-USE, STERILE, DISPOSABLE NEEDLES ARE USED BY ACUPUNCTURISTS.
STATEMENT OF CONSENT I am seeking to be treated with acupuncture for the condition of . I confirm
that I have read and understood the above information and I consent to having acupuncture treatment.
I understand that I can refuse treatment at any time.
Signature
Print name in full
Date