Health Aff 2011 Maxwell 1451 60
11
At the Intersection of Health, Health Care and Policy doi: 10.1377/hlthaff.2011.0347 , 30, no.8 (2011):1451-1460 Health Affairs Disparities Remain Massachusetts' Health Care Reform Increased Access To Care For Hispanics, But Rosman James Maxwell, Dharma E. Cortés, Karen L. Schneider, Anna Graves and Brian Cite this article as: http://content.healthaffairs.org/content/30/8/1451.full.html available at: The online version of this article, along with updated information and services, is For Reprints, Links & Permissions: http://healthaffairs.org/1340_reprints.php http://content.healthaffairs.org/subscriptions/etoc.dtl E-mail Alerts : http://content.healthaffairs.org/subscriptions/online.shtml To Subscribe: written permission from the Publisher. All rights reserved. mechanical, including photocopying or by information storage or retrieval systems, without prior may be reproduced, displayed, or transmitted in any form or by any means, electronic or Affairs Health Foundation. As provided by United States copyright law (Title 17, U.S. Code), no part of by Project HOPE - The People-to-People Health 2011 Bethesda, MD 20814-6133. Copyright © is published monthly by Project HOPE at 7500 Old Georgetown Road, Suite 600, Health Affairs Not for commercial use or unauthorized distribution at LIBRARY OF MEDICINE on August 5, 2011 Health Affairs by content.healthaffairs.org Downloaded from
-
Upload
brennan-bollman -
Category
Documents
-
view
219 -
download
0
Transcript of Health Aff 2011 Maxwell 1451 60

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 1/11
At the Intersection of Health, Health Care and Policy
doi: 10.1377/hlthaff.2011.0347
, 30, no.8 (2011):1451-1460Health Affairs
Disparities RemainMassachusetts' Health Care Reform Increased Access To Care For Hispanics, But
RosmanJames Maxwell, Dharma E. Cortés, Karen L. Schneider, Anna Graves and Brian
Cite this article as:
http://content.healthaffairs.org/content/30/8/1451.full.html
available at:The online version of this article, along with updated information and services, is
For Reprints, Links & Permissions:http://healthaffairs.org/1340_reprints.php
http://content.healthaffairs.org/subscriptions/etoc.dtlE-mail Alerts :
http://content.healthaffairs.org/subscriptions/online.shtmlTo Subscribe:
written permission from the Publisher. All rights reserved.mechanical, including photocopying or by information storage or retrieval systems, without prior
may be reproduced, displayed, or transmitted in any form or by any means, electronic orAffairs
Health Foundation. As provided by United States copyright law (Title 17, U.S. Code), no part ofby Project HOPE - The People-to-People Health2011Bethesda, MD 20814-6133. Copyright ©
is published monthly by Project HOPE at 7500 Old Georgetown Road, Suite 600,Health Affairs
Not for commercial use or unauthorized distribution
at LIBRARY OF MEDICINEon August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 2/11
By James Maxwell, Dharma E. Cortés, Karen L. Schneider, Anna Graves, and Brian Rosman
Massachusetts’ Health CareReform Increased Access To Care
For Hispanics, But DisparitiesRemain
ABSTRACT Hispanics are more likely than any other racial or ethnic group
in the United States to lack health insurance. This paper draws on
quantitative and qualitative research to evaluate the extent to which
health reforms in Massachusetts, a model for the Affordable Care Act of
2010, have reduced disparities in insurance coverage and access to health
care. We found that rates of coverage and the likelihood of having a usual
provider increased dramatically for Massachusetts Hispanics after the
state’s reforms, but disparities remained. The increase in insurance
coverage among Hispanics was more than double that experienced by
non-Hispanic whites. Even so, in 2009, 78.9 percent of Hispanics had
coverage, versus 96 percent of non-Hispanic whites. Language and other
cultural factors remained significant barriers: Only 66.6 percent of
Hispanics with limited proficiency in English were insured. One-third of
Spanish-speaking Hispanics still did not have a personal provider in
2009, and 26.8 percent reported not seeing a doctor because of cost, up
from 18.9 percent in 2005. We suggest ways to reduce such disparitiesthrough national health care reform, including simplified enrollment
and reenrollment processes and assistance in finding a provider and
navigating an unfamiliar care system.
I
n 2006 Massachusetts enacted compre-hensive health reform legislation,known as Chapter 58, to provide all res-idents of the state with access to insur-ance coverage, regardless of their in-
come, health, or previous insurance status.Chapter 58 was a model for the federal Afford-able Care Act of 2010, in particular through itsprovisions designed to reduce racial and ethnicdisparities. Several studies have tracked the im-plementation and outcomes of Chapter 58 dur-ing its first four years.1,2 The findings indicatethatMassachusetts has achieved the highest rateof health insurance coverage in the nation; em-ployer-based coverage has increased; and thestate’s health reform law is supported by thepublic and a broad coalition of stakeholder
groups.3,4 Evidence of improvements in resi-dents’ health and health care—such as reducedhospitalization rates for preventable conditions,including diabetes, heart disease, and asthma—is emerging.5
One of the secondary goals of health care re-form in Massachusetts was to reduce racial andethnic disparities in coverage. In Chapter 58,Massachusetts legislators explicitly recognizedthe importance of eliminating disparities by es-tablishing it as a goal of the Health Care Quality and Cost Council.6 Chapter 58 also establishedthe Health Disparities Council, which monitorsand makes recommendations regarding racialand ethnic disparities in access to high-quality care and in health outcomes.7
To implement the new law, the state created
doi: 10.1377/hlthaff.2011.0347
HEALTH AFFAIRS 30,
NO. 8 (2011): 1451–1460
©2011 Project HOPE—The People-to-People HealthFoundation, Inc.
James Maxwell (jmaxwell@ jsi.com) is the director ofresearch at the JSI Researchand Training Institute, inBoston, Massachusetts.
Dharma E. Cortés is a seniorresearch associate at theMauricio Gastón Institute forLatino CommunityDevelopment and Public Policyof the University ofMassachusetts, in Boston.
Karen L. Schneider is a seniorresearch scientist at the JSIResearch and TrainingInstitute.
Anna Graves is a researchassociate at the JSI Researchand Training Institute.
Brian Rosman is researchdirector of Health Care ForAll, in Boston.
A ug us t 2 0 11 3 0: 8 H e a lt h A f f a i r s 1451
States & Reform
at LIBRARY OF MEDICINEon August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 3/11
the Health Care Reform Outreach Grant Pro-gram, which represented a revival of the DirectService Outreach Grants Program that Massa-chusetts had used in the late 1990s to fund localnonprofit groups that helped people enroll inMedicaid programs created at thattime.8 Severalof the community groups that received grants inthe 1990s have pioneered innovative enrollment
assistance programs aimed at Hispanics andother disadvantaged populations.9 In addition,Chapter 58 gives community health centers andpublic hospitalsfinancial incentives to enroll un-insured Hispanics in the state’s new insuranceprogram and to provide care for them.
Hispanics are the largest and fastest-growingethnic minority group in Massachusetts. In 2010the state had 6,547,629 residents, of whom9.6 percent (627,654 people) identified them-selves as Hispanic—a 46.4 percent increase from2000.10 Policy makers and researchers have longrecognized the barriers that Hispanics face in
terms of access to health care and insurancecoverage—obstacles that have serious implica-tions for their health.11,12
This paper evaluates the extentto which Chap-ter58’s comprehensive health reforms improvedaccess to coverage and care for Hispanics inMassachusetts, compared to the state’s non-Hispanic white population, and whether dispar-ities between the groups have been reduced. Weused quantitative data to compare rates of cover-age and access to care before and after the enact-ment of Chapter 58 for Hispanic adults andnon-Hispanic white adults. We also examined
qualitative data, to provide a context in whichto interpret the quantitative data and identify persistent barriers to coverage and care. The pa-per ends with a discussion of the implications of the Massachusetts experience for the implemen-tation of national health care reform and strat-egies that might reduce disparities nationally.
Study Data And MethodsState-Based Telephone Survey Our study re-lied on analysis of 2005 and 2009 data from theMassachusetts Behavioral Risk Factor Surveil-
lance System survey. This state-based telephonesurvey on health-related topics was conductedamong people age eighteen or older by theMassachusetts Department of Public Health incollaboration with the Centers for Disease Con-trol and Prevention.13 The Massachusetts survey was administered in English and Spanish, andcities with a high proportion of minority popu-lations, especially Hispanic communities, wereoversampled.We limited our analysis to respon-dents ages 18–64 because health reform was spe-cifically targeted at this age group.
To measure healthcoverageand access to care,we used the following three questions in thesurvey: (1) “Do you have any health coverage,including health insurance prepaid plans suchas HMOs [health maintenance organizations],or government plans such as Medicare?” (2) “Do
you have one person you think of as your per-sonal doctor or health care provider?” (3) “ Was
there a time in the past 12 months when youneeded to see a doctor but could not becauseof cost?” We coded race or ethnicity as non-Hispanic white or Hispanic, excluding other racial or ethnic groups from the analyses. Wefurther categorized Hispanic adults accordingto whether they completed the survey in Englishor Spanish—information we used as a proxy for English proficiency. Citizenship and legal statuswere not a part of the survey questionnaire.
We present unadjusted and adjusted rates be-cause both provide important information. Un-adjusted rates represent the “real world” experi-
ence, in which not all racial and ethnic groupsare equal with respect to income, health status,education, and so forth. Adjusted rates show where racial and ethnic disparities exist evenwhen there areno differencesin those character-istics between groups.
To adjust for the confounding effects of socialstatus and demographic differences betweengroups, we constructed a multivariate logisticregression model that controlled for householdincome, employment status, age, health status,sex, disability status, education, marital status,smoking status, hypertension diagnosis, and
diabetes diagnosis. This model included maineffects—race or ethnicity, year of survey, and across-classification of these two variables—andmade population-based estimates of access tocare and coverage for each combination of year and racialor ethnicgroup, while adjustingfor allother variables.We tested differences by year andraceor ethnicity using Waldchi-square tests (sig-nificant if p < 0:05).
Focus Groups And Interviews Our qualita-tive data focused on compliance with the new state mandate for health insurance coverage,the process of obtaining coverage, perceptions
of health insurance affordability, the meaning of insurance coverage, thedifficulties in maintainingcoverage,andtheuseofinsuranceonceenrolled.Little research has been done on these topicsfor the newly insured, especially for membersof minority populations. We conducted threefocus groups with newly insured individuals inEnglish—one each in Boston, Cape Cod, and
Worcester —andone group in Spanish, in Lowell.The groups ranged in size from seven to fourteenparticipants.We also conducted a focus group inBoston withenrollment specialists fromcommu-
States & Reform
1452 H e a lt h A f f a i r s A u g u s t 2 0 1 1 3 0 : 8
at LIBRARY OF MEDICINEon August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 4/11
nity health centers. A standardized interview guide was usedwitheach ofthe groups, and eachsession was transcribed.
We also conducted twenty in-depth interviewswith newly insured Hispanics age eighteen or older, who spoke English or Spanish and whoseincome was 150–300 percent of the federal pov-erty level.14 All of the participants were legal
residents of the United States. They had beenborn in Colombia, the Dominican Republic, ElSalvador, Guatemala, Honduras,Mexico, PuertoRico, the mainland United States, or Venezuela.
Limitations There are several limitations tothis study. First, the Behavioral Risk Factor Surveillance System survey relies on contact by landline telephone and thus does not captureinformation from people who use only mobilephones—a growing segment of the population.This can lead to the underrepresentation of
younger and low-income groups.Second, the data are self-reported. However,
the question used in the survey to determinecurrent insurance status has been validated inother studies.15
Third, the questionnaire did not include ques-tions on country of origin, citizenship, or legalstatus. Thus, we were unable to estimate thepro-portion of noncitizens—both legal and undocu-mented—whoresponded to thesurvey. These areimportant topicsthatwe soughtto address in our qualitative research.
Finally, the focus-group respondents and theparticipants in the in-depth interviews were notbased on representative samples, and their re-
sponses might not be generalizable to the entireHispanic population or to specific groupswithin it.
Study ResultsPopulation Characteristics Exhibit 1 pro-
vides a summary of the Massachusetts survey sample characteristics in 2005 and 2009. Com-pared to non-Hispanic whites in 2005,Hispanicswere generally younger (58.3 percent wereunder age thirty-five, compared to 32.0 percent),had less education (39.3 percent had not gradu-
ated from high school, compared to 3.5 percent),and had lower incomes (51.4 percent had annualhousehold incomes of less than $25,000, com-pared to 12.2 percent).
In comparison to Hispanics who completedthe survey in English, those who used Spanishinstead had lower incomes (67.3 percent re-ported annual household incomes of less than$25,000, compared to 42.7 percent) and lesseducation (58.1 percent had not graduated fromhigh school, compared to 28.1 percent). Thedemographic characteristics of the 2009 His-
panic sample were similar to those of the samplefrom 2005, although the2009 group wasslightly older and had had more education.
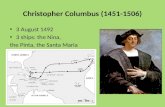
Insurance Coverage As documented in pre- vious studies of Massachusetts’ health care re-form, coverage increased significantly amongstate residents, from 88.3 percent in 2005 to93.9 percent in 2009 (Exhibit 2). Note that these
data arefor thetotalstatepopulation, of allracesand ethnicities. Both the non-Hispanic whitesand the Hispanics in our sample experiencedincreases in coverage. The increase among His-panicswasmorethandoublethatexperiencedby non-Hispanic whites, but a 17.1-percentage-point difference remained in 2009 between thenon-Hispanic white and Hispanic populations.Hispanics who completed the survey in Spanishwere more likely to remain uninsuredthan thosewho completed it in English.
Exhibit 3 shows the results of multivariate re-gression analyses. The adjusted rates of coverage
for the non-Hispanic whites (95.4 percent) andthe Hispanics who completed the survey inEnglish (95.0 percent) were nearly identical in2009. In comparison, the adjusted rate of coverage for Spanish-speaking Hispanics was84.0 percent.
The bivariate and multivariate results of thequantitative data analysis do not offer a full ex-planation of why the disparities in coverage per-sist, nor do they identify the remaining barriersto coverage for Hispanics. However, our quali-tative analyses indicate that coverage disparitiesare related to people’s status as undocumented
immigrants, their familiarity with the insurancemandate, the affordability of coverage, and thecomplexity of the enrollment and reenrollmentprocesses. Cultural attitudes, language differen-ces, and degree of acculturation all influencedecisions to purchase and use health insurance.
Oneof the reasons for the increase in coverageis a broad awareness among Hispanics of theindividual mandate to obtain health insurancecoverage and of the tax penalties for not enroll-ing. Hispanics who knew about the mandatesought out coverage, many reporting a strongdesire to obey the laws of the state.Whether they
are legal residents or undocumented immi-grants, Hispanics are often concerned aboutthe effect of their actions on their immigrationstatus.
Understanding How To Enroll Community-based organizations that provided enrollmentcounseling services were crucial in helpingbridge the disparity in insurance coverage.Focus-group participants expressed their grati-tude to these organizations, and one Spanish-speaking woman indicated that without helpfrom a community-based organization, it would
A ug us t 2 01 1 3 0: 8 H e a lt h A f f a i r s 1453at LIBRARY OF MEDICINE
on August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 5/11
have been impossible for her to obtain health
insurance: “I would not have been able to do iton my own.”
Spanish speakers and individuals with low lit-eracy levels in our focus groups more often re-ported needing help with enrollment than didthose who spoke English, but they were lesslikely to receive such assistance. This problemwas reported in the initial enrollment phase andin the yearly reenrollments for coverage.Some of the programs aimed at Hispanics in Massachu-setts are effective, but their capacity is quite lim-ited.16 Both our qualitative and quantitative data
underscore the point thatSpanish-speaking His-
panics continue to face barriers in acquiringcoverage.
Finding The Money For Coverage Another reason for continuing disparities is the fact thatinsurance premiums put a strain on low-incomeHispanic households. Even after signing up for insurance plans, our focus-group participantsreported reconsidering their commitment be-cause they felt they would not be able to affordthe copayments and monthly premiums. OneSpanish-speaking person commented, “ We werein a double bind: we wanted to pay for [insur-
Exhibit 1
Characteristics Of Adult Hispanic And Non-Hispanic White Massachusetts Respondents To Telephone Survey, 2005 And 2009
Hispanic (%)
Total (%)Non-Hispanicwhite (%) Total English-speaking Spanish-speaking
Characteristic
2005(n =6,103)
2009(n =10,314)
2005(n =5,371)
2009(n =9,106)
2005(n =732)
2009(n =1,208)
2005(n =428)
2009(n =607)
2005(n =304)
2009(n =601)
Female 51.0 51.6 50.9 51.9 51.9 49.2 56.4 50.8 43.9 46.8Employed 74.3 74.2 75.7 75.8 63.2 61.3 61.2 65.4 66.3 55.8
Age (years)
18–25 15.8 17.0 14.2 15.6 28.7 28.7 35.1 27.8 18.0 29.726–34 19.1 17.5 17.8 16.9 29.6 22.1 23.4 24.1 40.0 19.635–49 36.3 34.2 37.3 34.4 28.0 32.7 25.3 33.5 32.6 31.650 or more 28.8 31.3 30.7 33.2 13.6 16.6 16.2 14.7 9.4 19.1
Household income
Less than $15,000 6.5 6.1 4.8 4.3 22.3 21.3 17.7 13.6 30.6 32.6$15,000–$24,999 9.7 9.2 7.4 6.7 29.1 31.4 25.0 26.2 36.7 39.0$25,000–$34,999 9.5 7.5 8.1 7.1 21.9 11.4 20.9 12.1 23.4 10.4$35,000–$49,999 13.5 11.4 13.6 11.1 12.3 14.8 15.1 14.7 7.3 14.7$50,000 or more 60.9 65.8 66.2 70.9 14.4 21.1 21.3 33.4 2.0 3.3
Education status
Less than high schooldiploma 7.5 6.3 3.5 3.6 39.3 27.7 28.1 13.0 58.1 46.9
High school diploma only 23.5 22.3 23.0 21.4 27.6 29.4 29.7 27.4 24.1 32.2Some college/technical
school 23.4 24.6 24.1 24.6 17.9 24.6 21.7 33.3 11.5 13.1Bachelor’ s degree or
more 45.7 46.8 49.5 50.4 15.2 18.3 20.5 26.3 6.3 7.8
Marital status
Married/partnered 63.4 66.7 65.3 68.6 47.7 52.2 42.5 52.2 56.3 52.1Divorced/separated 10.9 8.8 10.4 8.4 15.0 12.0 14.8 10.9 15.2 13.3Widowed 1.6 1.3 1.7 1.2 1.1 1.6 1.1 1.8 1.0 1.4Never married 24.1 23.2 22.6 21.9 36.3 34.3 41.6 35.0 27.5 33.2
Health status
Fair/poor overall healthstatus 10.9 9.5 9.7 7.8 20.7 23.2 15.6 13.7 29.0 35.7
Disabled 15.0 15.6 15.2 15.3 13.2 19.7 12.6 15.1 14.0 26.3Currently smokes 20.4 16.4 20.6 16.5 18.9 15.3 16.4 18.8 23.0 10.8High blood pressurea 18.1 18.8 18.3 18.7 16.4 19.6 16.4 19.2 16.5 20.0Diabetesa 4.6 5.3 4.4 5.1 6.4 6.8 7.0 5.6 5.2 8.4
SOURCE Note 13 in text. NOTES Sample sizes are unweighted. Percentages are weighted, and not all percentages sum to 100 because of rounding. English-speaking andSpanish-speaking refer to the language the person used to take the Behavioral Risk Factor Surveilla nce System telephone survey. Disabled means that a person’ s activitiesare limited by a health condition. aHave you ever been told by a health provider that you have this condition?
States & Reform
1454 H e a l t h A f f a i r s A u g u s t 2 0 1 1 3 0 : 8
at LIBRARY OF MEDICINEon August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 6/11
ance], but we did not have enough money, andwe did not even know how we were going to beable to pay the [state tax] penalty for noncompliance with the mandate.”
Access To Care Access to care,as measured interms of having a personal provider, has in-creased across Massachusetts (Exhibit 3). Usingunadjusted rates, we found that Hispanics had a
higher percentage increase between 2005 and2009 (15.2 percentage points) than non-Hispanic whites (1.8 percentage points), but sig-nificant differences remained in 2009 betweennon-Hispanic whites and Hispanics. One-thirdof Spanish-speaking Hispanics still did not havea personal provider in 2009.
Cost remained a key barrier to care. Althoughthis problem decreased somewhat between 2005and 2009 for most groups in the study, usingboth adjusted and unadjusted rates, it increasedsignificantly for Spanish-speaking Hispanics(Exhibit 3). The unadjusted rates for 2005 show
that 18.9 percent of that group reported not see-ing a doctor because of cost, but the number was26.8 percent in 2009.
Our multivariate regression analyses show that non-Hispanic whites and English-speakingHispanics had similar rates of having a personalprovider in 2009, while Spanish-speaking His-panics had a significantly lower rate (Exhibit 3).Even after the variables listed in the notes toExhibit 3 were adjusted for, the difference be-tween Spanish-speaking and English-speaking
Hispanics was 10 percentage points, while thedifference between Spanish speakers and non-Hispanic whites was 10.7 percentage points.Similarly, the adjusted 2009 rates for not seeinga doctor in the past year because of cost werenearly identical for non-Hispanic whites (7.1 per-cent) and English-speaking Hispanics (6.8 per-cent), while the rate for Spanish-speaking His-
Exhibit 2
Rates Of Health Insurance Coverage For Adult Hispanic And Non-Hispanic WhiteMassachusetts Respondents To Telephone Survey, 2005 And 2009
P e r c e n t I n s u r e d
HispanicSpanish-speaking
HispanicEnglish-speaking
Total HispanicNon-Hispanic whiteTotal
SOURCE Note 13 in text. NOTE The rates are unadjusted (see the explanation in the text).
Exhibit 3
Rates Of Insurance Coverage And Access To Care For Adult Hispanic And Non-Hispanic White Massachusetts Respondents To Telephone Survey,2005 And 2009
Responses to survey questions
Total (%)Non-Hispanicwhite (%)
Hispanic (%)
Total English-speaking Spanish-speaking
2005(n =6,103)
2009(n =10,314
2005(n =5,371)
2009(n =9,106)
2005(n =732)
2009(n =1,208)
2005(n =428)
2009(n =607)
2005(n =304)
2009(n =601)
Unadjusted rates
Has health coverage 88.6 94.1 91.2 96.0a 67.9b 78.9a,b 78.1b 88.3a,b 50.8b 66.6a,b
Has a personal provider 85.8 89.1 89.0 90.8a 60.6b 75.8a,b 72.8b 83.4a,b 40.2b,c 66a,b,c
Didn’ t see a doctor in thepast year because ofcost 9.4 7.4 8.3 6.3a 19.2b 18.7b 19.3b 12.4b 18.9b 26.8b,c
Adjusted rates
Has health coverage 89.4 94.4 90.5 95.4a 85.8b 90.7b 90.5 95.0 75.5b,c 84.0b,c
Has a personal provider 86.8 89.3 88.6 90.1 76.9b 86a 82.6b 89.4 63.2b,c 79.4a,b,c
Didn’ t see a doctor inthe past year because ofcost 8.6 7.5 8.2 7.1 10.4 9.3 11.7 6.8 8.6 12.4b,c
SOURCE Note 13 in text. NOTES The three survey questions are listed in the text. Adjusted rates are adjusted for household income, employment, age, health status,disability, sex, education, marital status, smoking status, hypertension diagnosis, and diabetes diagnosis. For all significant differences, p < 0:05. aSignificant compared to2005. bSignificant compared to non-Hispanic whites. cSignificant compared to English-speaking Hispanics.
A ug us t 2 01 1 3 0: 8 H e a lt h A f f a i r s 1455at LIBRARY OF MEDICINE
on August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 7/11
panics was significantly higher (12.4 percent).Our qualitative interviews helped explain why
Hispanics continued to be less likely to have aregular source of care and why cost remained asignificant barrier to care for Hispanics.
Providers’ Language Skills And CulturalCompetence Hispanics were less likely to havea primary care provider to begin with, and they
may have had extra difficulty finding a provider with the appropriate language skills and culturalcompetence. Some Hispanic interviewees andfocus-group participants said that finding a pro-
vider was just as challenging as finding a healthinsurance plan.
One Spanish-speaking participant reportedobtaining health insurance coverage but not us-ing it because shecouldnot find a provider:“Igotone [a health insurance plan]. I pay for it. I havenot used it yet because of the inconvenience of finding a doctor.” She said that the hospital sheusually visited did not accept her new insurance,
so she had to change providers. Then she had towait for an appointment with her new primary care physician. Another Spanish-speakingwoman complained that she had to wait four months to see her new physician, even thoughshe had been suffering from a painful and swol-len leg for months.
Another challenge for Hispanics was finding aprovider withwhom theyfelt comfortable discus-sing sensitive health issues. Our focus-groupparticipants reported that they would have pre-ferred to see Spanish-speaking providers insteadof relying on interpreters, but such providers
were difficult to find and had long waiting lists.Common reasons for feeling less comfortable
with interpreters included concern over confi-dentiality, unease about having a third party be-tween them and their provider, and both mis-communication and uncertainty over whether the interpreter was accurately translating their words. One participant commented, “How do
you know if the interpreter said what I said ex-actly?” A few participants reported saying “ yes”to providers’questions despite being unsure thatthey had understood what the provider wasasking.
Some insurance plans guaranteed that they would provide interpreters. Although at leastone focus-group participant had had a good ex-perience with this approach, others reportedbringing their own paid interpreter or anEnglish-speaking acquaintance whom they trusted.
Financial Barriers Low-income groups, in-cluding Hispanics with public coverage, may beat a particular disadvantage in finding a provider because many providers accept only patientswith private insurance. One Hispanic focus-
group participant said, “ You need to do your research. Call doctors first and see if they acceptMassHealth [thestate Medicaidprogram]. Many do not.”
Among Spanish-speaking Hispanics, the pro-portion of individuals not seeing a doctor inthe past year because of cost increased—although not significantly —between 2005 and
2009 (Exhibit 3). Even when they have a regular source of care, some Hispanics reported reluc-tance to see their providers because of copayment fees for office visits and medication.Participants who ended up with high copay-ments reported forgoing medications and rou-tine preventive care. Some were surprised whenthey had to pay for medication in addition tomaking copayments for visits to a provider. Thisconfusion about what costs are covered may in-fluence whether or not people decide to keeppaying their insurance premiums.
DiscussionMassachusetts’ comprehensive health care re-form has greatly expanded the portion of thestate’s population with health insurance. Likeother national and state studies, ours found thatHispanics were much less likely to have insur-ance than other residents prior to the passage of reform legislation.17,18 Since the enactment of Chapter 58, the rate of coverage increased morerapidly among Hispanics than among non-Hispanic whites, but important disparities re-mained. Although only 4 percent of the non-
Hispanic white population was uninsured in2009, 21 percent of Hispanics still lacked cover-age at that time (Exhibit 2), which translates toapproximately 82,752 Hispanic adults. The dis-parities were most pronounced among His-panics with limited English proficiency.
Also like national studies, our research foundthat much of the disparity in coverage betweennon-Hispanic whites and Hispanics in Massa-chusetts could be explained by differences indemographic factors, social status, language,and health status.19 After confounding factorswere adjusted for, the rates of coverage for
non-Hispanic whites and English-speaking His-panics were similar in 2009.
This result implies that if policies could ad-dress the social determinants of health, dispar-ities in coverage could be greatly decreased.However, the differences in coverage betweennon-Hispanic whites and Spanish-speaking His-panics persisted even after these observabledemographic characteristics were controlledfor. This finding is consistent with our qualita-tive research, which suggests that language, ac-culturation, and other cultural factors remain
States & Reform
1456 H e a lt h A f f a i r s A u g u s t 2 0 1 1 3 0 : 8
at LIBRARY OF MEDICINEon August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 8/11
significant barriersto coverage for Hispanics.Weexpected that some of this disparity would per-sist, given that Chapter 58 excludes undocu-mented immigrants from coverage. However,our data do not provide a precise estimate of the percentage of Hispanics who lack coveragebecause of their immigration status.
Our qualitative research shed additional light
on the coverage issues and barriers that may beunique to Hispanics. Regardless of their ethnic-ity, many of the newly insured did not fully graspthemeaning of health insuranceand thepurposeof their premium payments. Many of them alsofound the enrollment and reenrollment proc-esses confusing. Our findings suggest that theseproblems were magnified for Hispanics, espe-cially non-English speakers, who were morelikely than English-speaking Hispanics to be re-cent immigrants. Limited English proficiency made it difficult for them to navigate the state’scomplex enrollment and reenrollment proc-
esses. Because Massachusetts did not establishspecial enrollment programs for these His-panics, they had to seek out enrollment counsel-ing on their own. Given the limited capacity andgeographic scope of enrollment programs con-ducted in Spanish, many Hispanics did not re-ceive assistance and remained uninsured.
Peoplewho have insurance arealsomorelikely to have a personal provider and less difficulty paying for care compared to people without in-surance.20 The percent of Hispanics with a per-sonal provider increased from 60.6 percent in2005 to 75.8 percent in 2009 (unadjusted rates;
see Exhibit 3), but that left 94,310 people with-out a provider. Cost also remained a barrier toreceiving care.
Our multivariate analyses showed that havinga low income andnot being proficient in Englishhelped explain why a lower percentage of His-panics than non-Hispanic whites had a personalprovider and why a higher percentage reportednot seeing a doctor because of cost. However,these factors did not fully explain the disparitiesbetween Spanish-speaking Hispanics and non-Hispanic whites.
Key features of the health delivery system con-
tinued to be barriers to access for Hispanics.Many newly insured Hispanics did not have aprimary care provider before they had coverageand did not know how to find one, unless their insurer automatically assigned one to them.Many Hispanics indicated their preference for seeing Spanish-speaking primary care provid-ers, but because such providers are relatively rare, a new patient may have to wait for weeksor even months to get an appointment. In addi-tion, affordability of careremained a problem for Hispanics, even those with insurance.
Lessons For National ReformSimilarities The Affordable Care Act is similar to the Massachusetts health reform law both ingeneral and in the way in which it deals withhealth disparities.The federal law makes it easier to qualify for subsidized coverage, on theassumption that the change will give ethnicminority groups better access to coverage and
care. It addresses racial and ethnic disparitiesby taking steps similar to those in the Massachu-setts law. Specifically, the federal law expandsthe monitoring of health disparities, establishesOffices of Minority Health in federal healthagencies—such as the Agency for HealthcareResearch and Quality, the Centers for DiseaseControl and Prevention, and the Centers for Medicare and Medicaid Services—and providesfunding to the states for independent consumer outreach and assistance programs.21
Differences The Affordable Care Act differsfrom the Massachusetts approach in that the
federal government has provided funds for ahuge expansion of community health centersthat traditionally serve disadvantaged popula-tions, including Hispanics. The Affordable Care
Act also differs from Chapter 58 in that the for-mer expands funding for the education and re-cruitment of more minority health professionalsto work in medically underserved areas.
Policy Implications Although deeply rootedsocial and environmental factors play a decisiverole in health disparities, as our findings show,health policy makers can take certain actions toreduce racial and ethnic disparities in the con-
text of health reform. As the numbers of His-panics continue to increase and their rates of insurance coverage remain lower than those of other groups, it is imperative that we design andimplement more-effective strategies for expand-ing Hispanics’ insurance coverage and access tocare. Developing policies specifically for His-panics is a national priority, but it is especially important in states with large Hispanic popu-lations.
Our research has three major implications for implementing a national strategy aimed at His-panics. First, theMassachusettsexperience dem-
onstrates that existing outreach and enrollmentprograms for theuninsuredmay notbe sufficientto meet thecomplex cultural,linguistic, and eco-nomic needs of Hispanics. Massachusetts wasfortunate that the state had a successful grantprogram for outreach and enrollment and thatcommunity and provider groups took the initia-tive to develop programs for Hispanics by ex-tending outreach to churches, community clin-ics, and other institutions that chiefly servedHispanics.
However, many of these programs were under-
A ug us t 2 01 1 3 0: 8 H e a lt h A f f a i r s 1457at LIBRARY OF MEDICINE
on August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 9/11
funded, and collectively they reached only asmall percentage of the Hispanic population.More state and national programs specifically for Hispanics are needed, and they must havestable funding sources. In addition, programsneed to be targeted to those Hispanics who aremost at risk of not having insurance or access tocare. The Massachusetts experience suggests the
need for both a top-down and a bottom-up ap-proach to addressing disparities. In other words,federal and state governments need to explicitly adopt strategies for enrolling Hispanics—especially Spanish-speaking Hispanics—whileat the same time encouraging local initiativesand innovations.
Second, our study shows that programs serv-ing Hispanics need to do more than simply pro-
vide outreachand assistance at thetimeof enroll-ment. Enrollment is not a single-step process for many Hispanics, who need to reenroll annually and find newcoverage if their income or employ-
ment changes. Simplified enrollment and re-enrollment processes, coupled with staff whohave appropriate cultural and linguistic train-ing, could make enrollment easierbut still would
not eliminate the need for ongoing assistance.Because many of the newly insured have never before had health insurance, they may also re-quire help in finding a provider and navigatingan unfamiliar care system. Ongoing training andtechnical assistance would be beneficial.
Finally, it is important to maintain the healthcare safety net. Federal health reform is unlikely
to secure health insurance for 100 percent of theHispanic or other historically disadvantagedpopulations, and the safety net is critical for those who remain outside the system. The Af-fordable Care Act greatly expands funding for the federal health center program, but it is toosoon to know whether this funding will bedirected to Hispanics. The safety net in other states that are implementing health reformshould include tools for outreach to Hispaniccommunities and other disadvantaged popula-tions, and funding to pay for their care.Withoutspecialized tools and adequate funding, the
widespread disparities in coverage and accessto care in the current system may be reduced,but they are not likely to be eliminated. ▪
Some elements of this article werepresented at the National Congress onHealth Insurance Reform, Washington,D.C., January 17, 2011, and the FamiliesUSA Conference, Washington, D.C.,January 28, 2011. The authors thank PatFairchild and Natalie Truesdell of John
Snow Inc. (JSI) for their contributions tothe Care beyond Coverage Project—sponsored by the Blue Cross Blue Shieldof Massachusetts Foundation—on whichthis article was based. Dharma Cortesappreciates the contributions of RodolfoVega to the qualitative research
reported here. This research wassupported by a contract with the BlueCross Blue Shield of MassachusettsFoundation to JSI and by grant fundingto Cortes from the Robert WoodJohnson Foundation’ s New Connectionsprogram.
NOTES
1 Massachusetts Division of HealthCare Finance and Policy. Health in-surance coverage in Massachusetts:results from the 2008–2010 HealthInsurance Surveys [Internet].Boston (MA): The Division;2010 Dec [cited 2011 Jun 3]. Avail-able from: http://www.mass.gov/Eeohhs2/docs/dhcfp/r/pubs/10/mhis_report_12-2010.pdf
2 Long SK, Masi PB. Access and af-fordability: an update on health re-form in Massachusetts, fall 2008.Health Aff (Millwood). 2009;28(4):w578–87. DOI: 10.1377/hlthaff
.28.4.w578.3 Long SK, Stockley K. Sustaining
health reform in a recession: anupdate on Massachusetts as of fall2009. Health Aff (Millwood). 2010;29(6):1234–41.
4 Gabel JR, Whitmore H, Pickreign J,Sellheim W, Shova KC, Bassett V.
After the mandates: Massachusettsemployers continue to supporthealth reform. Health Aff (Mill-wood). 2008;27(6):w566–75.DOI: 10.1377/hlthaff.27.6.w566.
5 Kolstad JT, Kowalski AE. The impact
of healthcare reformon hospital andpreventive care: evidence fromMassachusetts [Internet]. Cam-bridge (MA): National Bureau of Economic Research; 2010 May [lastrevised 2010 Oct 13; cited 2011Jun 28]. (NBER Working Paper No.16012). Abstract available from:http://www.nber.org/papers/w16012
6 187th General Court of theCommonwealth of Massachusetts.Massachusetts General Laws, chap.6A,sec. 16K, HealthCare QualityandCost Council [Internet]. Boston
(MA): The Court; 2010 Oct 1 [cited2011 Jun 28]. Available from: http://www.malegislature.gov/Laws/GeneralLaws/PartI/TitleII/Chapter6A/Section16K
7 187th General Court of theCommonwealth of Massachusetts.Massachusetts General Laws, chap.6A, sec. 160, Health DisparitiesCouncil; duties; composition; meet-ings; annual reports [Internet].Boston (MA): The Court; 2010 Oct 1[cited 2011 Aug 1]. Available from:http://www.malegislature.gov/
Laws/GeneralLaws/PartI/TitleII/Chapter6A/Section16O
8 MassHealth. MassHealth fact sheet:Health Care Reform Outreach GrantProgram [Internet]. Boston (MA):MassHealth; 2010 Feb [cited 2011Jun 28]. Available from: http://outreachgrants.ehs.state.ma.us/uploadedFiles/Outreach_Grants/Outreach%20Grants%20Fact%20Sheet%20cy2009.pdf
9 Abreu M, Hynes HP. The LatinoHealth Insurance Program: a pilotintervention for enrolling Latinofamilies in health insurance pro-
grams, East Boston, Massachusetts,2006–2007. Prev Chronic Dis.2009;6(4):A129.
10 Ennis SR, Ríos-Vargas M, Albert NG.The Hispanic population: 2010 [In-ternet]. Washington (DC): CensusBureau; 2011 May [cited 2011Jun 28]. (2010 Census Brief).
Available for download from: http://2010.census.gov/2010census/data/
11 Haider AH, Chang DC, Efron DT,Haut ER, Crandall M, Cornwell EE3rd. Race and insurance status asrisk factors for trauma mortality.
States & Reform
1458 H e a lt h A f f a i r s A u g u s t 2 0 1 1 3 0 : 8
at LIBRARY OF MEDICINEon August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 10/11
Arch Surg. 2008;143(10):945–9.12 Insaf TZ, Jurkowski JM, Alomar L.
Sociocultural factors influencingdelay in seeking routine health careamong Latinas: a community-basedparticipatory research program.Ethn Dis. 2010;20(2):148–54.
13 Centers for Disease Control andPrevention. Behavioral Risk Factor Surveillance System: 2005 and 2009
survey data. Atlanta (GA): CDC;[last updated 2010 Oct 28; cited2011 Jun 28]. Available from: http://www.cdc.gov/brfss/technical_infodata/surveydata.htm
14 Cortez DE. “No one asked me”: Lat-inos’ experiences with Massachu-setts health care reform [Internet].Princeton (NJ): Robert WoodJohnson Foundation; 2010Feb [cited 2011 Jun 28]. (LessonsLearned). Available from: http://www.rwjf.org/files/research/4268.52233.pdf
15 Nelson DE, Holtzman D, Bolen J,Stanwyck CA, Mack KA. Reliability
and validity of measures from theBehavioral Risk Factor SurveillanceSystem (BRFSS). Soz Praventivmed.2001;46(Suppl 1):S3–42.
16 Fairchild P, Maxwell J, Schneider K,Truesdell N, Mathur J. Access tohealth care in Massachusetts: thelandscape in 2009. Boston (MA):John Snow Inc.; 2009 Nov. (Un-published report).
17 Massachusetts Division of HealthCare Finance and Policy. Health carein Massachusetts: key indicators[Internet]. Boston (MA): The Divi-sion; 2009 Feb [cited 2011 Jun 28].
Available from: http://www.mass.gov/Eeohhs2/docs/dhcfp/r/pubs/09/key_indicators_02-09.pdf
18 Patel N, Bae S, Singh KP.Associationbetween utilization of preventiveservices and health insurance status:findings from the 2008 BehavioralRisk Factor Surveillance System.Ethn Dis. 2010;20(2):142–7.
19 Crow SE, Harrington ME,McLaughlin CG. Sources of vulner-
ability: a critical review of the liter-ature on racial/ethnic minorities,immigrants, and persons withchronic mental illness [Internet].
Ann Arbor (MI): University of Michigan Economic Research Ini-tiative on the Uninsured; 2002 Oct[cited 2011 Jun 28]. (ERIU WorkingPaper No. 14). Available from:http://www.rwjf-eriu.org/pdf/
wp14.pdf 20 Cerise FP, Chokshi DA. Orienting
health care reform around universalaccess. Arch Intern Med. 2009;169(20):1830–2.
21 Foster J. Moving toward healthequity: health reform creates afoundation for eliminating dispar-ities [Internet]. Washington (DC):Families USA; 2010 May [cited 2011Jun 29]. (Issue Brief). Available for download from: http://www .familiesusa.org/issues/health-equity/resource-center/other-health-equity-topics.html
ABOUT THE AUTHORS: JAMES MAXWELL, DHARMA E. CORTES,
KAREN L. SCHNEIDER, ANNA GRAVES & BRIAN ROSMAN
James Maxwell is
the director ofresearch at the JSIResearch andTraining Institute.
In their paper in Health Affairs thismonth, James Maxwell andcoauthors present Massachusetts asa model for reducing disparities incoverage and access as other statesimplement national health reform.The paper builds on an earlier study on health care accesssponsored by the Blue Cross Blue
Shield of MassachusettsFoundation. That study surveyed100 newly insured people—mostly Hispanic and Spanish- or Portuguese-speaking—and heldfocus groups with Hispanics andnon-Hispanics who were newly insured.
Maxwell is the director of research at the JSI Research andTraining Institute, health care
consultants in Boston, and isnationally recognized for hisexpertise on health insurance andfinancing issues. He was the leadconsultant to the Douglasadministration in the development
of Vermont’s 2006 comprehensivehealth care reform plan, and hehelped establish that state’sGovernor ’s Commission on Healthy
Aging.Maxwell also recently has
reviewed payment reformmethodologies used by public andprivate payers, including pay-for-performance, rate setting, andaccountable care organizations. Hepreviously was a consultant for Colorado’s health care quality
council. He received a doctorate inpublic policy from theMassachusetts Institute of Technology.
Dharma E. Cortés isa senior researchassociate at theMauricio Gastón
Institute for LatinoCommunityDevelopment andPublic Policy.
Dharma Cortés is an instructor atCambridge Health Alliance andHarvard Medical School, a senior research associate at the MauricioGastón Institute for LatinoCommunity Development andPublic Policy of the University of Massachusetts, and an adjunctassociate professor at Northeastern
University ’s Institute on UrbanHealth Research. She has beenconducting community-basedresearch with Latinos in the UnitedStates for fifteen years. Her workfocuses on culture, mental andphysical health, health literacy, andthe use of health and mental healthservices. She has a doctorate insociology from Fordham University.
A ug us t 2 01 1 3 0: 8 H e a lt h A f f a i r s 1459at LIBRARY OF MEDICINE
on August 5, 2011Health Affairs bycontent.healthaffairs.orgDownloaded from

8/6/2019 Health Aff 2011 Maxwell 1451 60
http://slidepdf.com/reader/full/health-aff-2011-maxwell-1451-60 11/11
Karen L. Schneideris a senior researchscientist at the JSI
Research andTraining Institute.
Karen Schneider, a senior research scientist at the JSIResearch and Training Institute,has extensive experience analyzinglarge secondary data sets to exploredisparities in health and access tocare. At JSI, Schneider has beenthe data and statistical consultanton evaluation projects, designingstudies, creating surveys, andwriting reports. She has adoctorate in epidemiology fromBrown University.
Anna Graves is aresearch associateat the JSI Research
and TrainingInstitute.
Anna Graves is a researchassociate at the JSI Research andTraining Institute. She has beenaccepted into the Medical ScientistTraining Program at the University of Alabama at Birmingham. Her research interests include perinatalepidemiology and maternal andchild health policy issues amongminority populations. She recently received a master ’s degree inepidemiology and medicalanthropology from BostonUniversity.
Brian Rosman is
research director ofHealth Care For All.
Rosman is research director of Health Care For All, a Boston-basedhealth advocacy organization. Hiswork focuses on policy researchand analysis related toMassachusetts and national healthreform, health payment methods,and other policy issues. He wasresearch director and generalcounsel for the House staff of theJoint Committee on Health Care of the Massachusetts legislature andwas counsel to the MassachusettsSenate Committee on Ways andMeans. He has a law degree fromthe University of Pennsylvania.
States & Reform
1460 H e a lt h A f f a i r s A u g u s t 2 0 1 1 3 0 : 8A t 5 2011H lth Aff ibt t h lth ff iD l d d f