Healing and Repair - German University in Cairopbt.guc.edu.eg/Download.ashx?id=580&file=Lecture...
32
Healing and Repair Dr. Nabila Hamdi MD, PhD 1
Transcript of Healing and Repair - German University in Cairopbt.guc.edu.eg/Download.ashx?id=580&file=Lecture...

Healing and Repair
Dr. Nabila Hamdi
MD, PhD 1

ILOs
• Know the classification of human cells according to their ability for proliferation.
• Understand the mechanism of cellular regeneration.
• Identify the types of repair.
• Describe the different steps of tissue repair, including the cell types and growth factors involved, and the approximate timetable for the tissue repair process.
• Compare healing by first intention (primary union) and second intention (secondary union) in terms of time, sequence of events, morphologic changes, and final outcome..
• Be oriented with the factors affecting the process of repair.
2

Outline 1. Overview 2. Cell Regeneration • Control of cell growth, cell cycle • Growth factors • Extracellular matrix 3. Repair by Connective Tissue • Angiogenesis • Fibrosis (Scar formation) • Scar Remodeling 4. Wound Healing • Healing by first intention • Healing by second intention • Wound strength 5. Factors Affecting Healing 6. Overview of the Inflammatory-Reparative Response
3

Overview
4
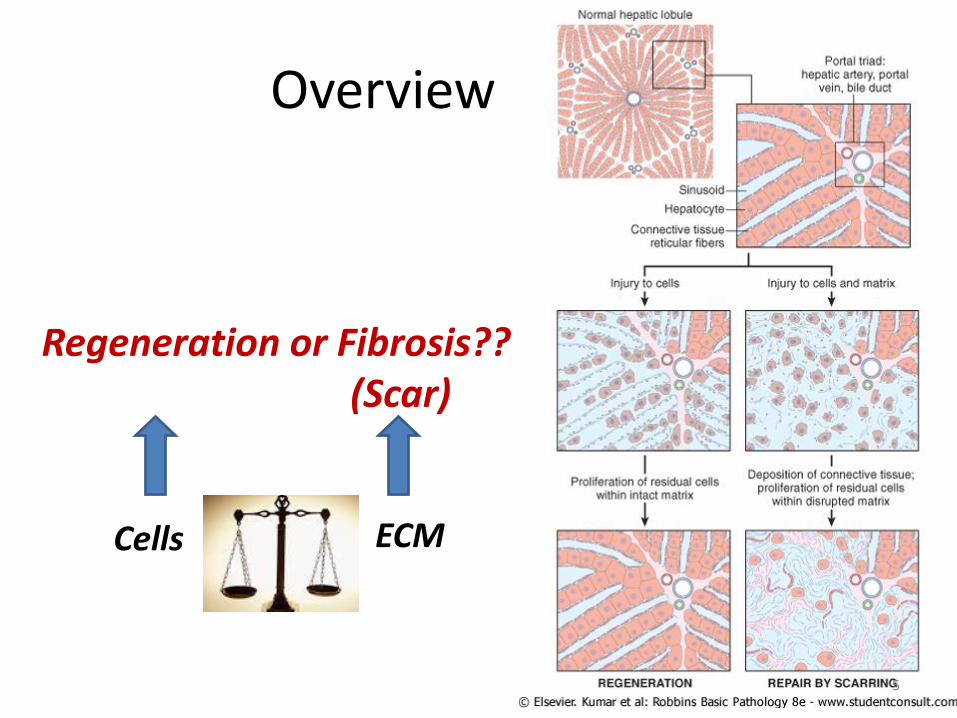
Overview
Regeneration or Fibrosis?? (Scar)
Cells ECM
5
Overview
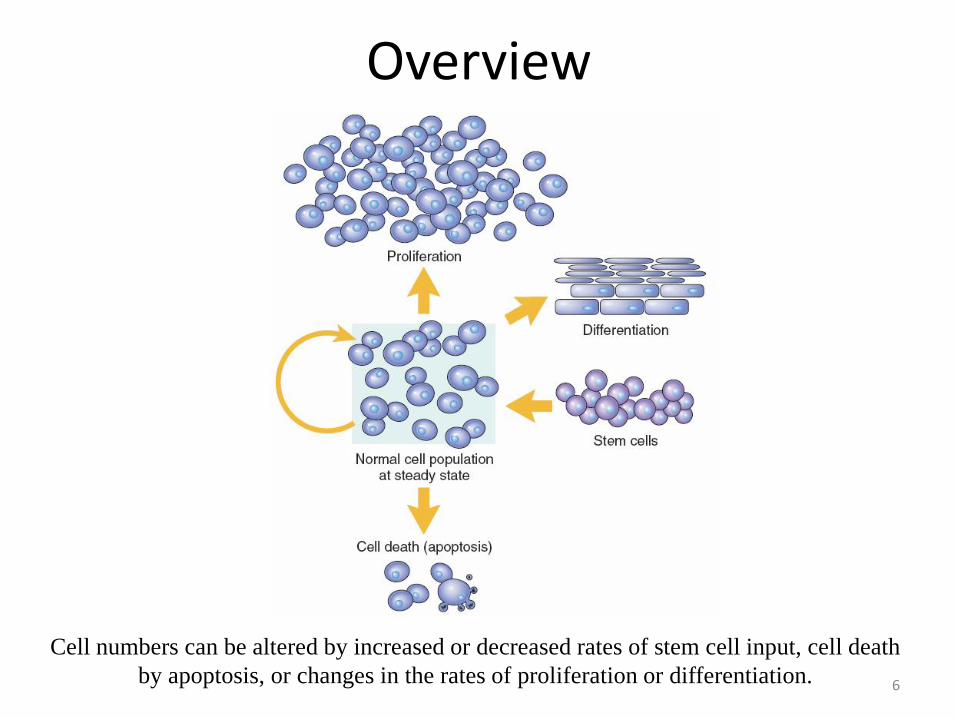
Cell numbers can be altered by increased or decreased rates of stem cell input, cell death
by apoptosis, or changes in the rates of proliferation or differentiation. 6
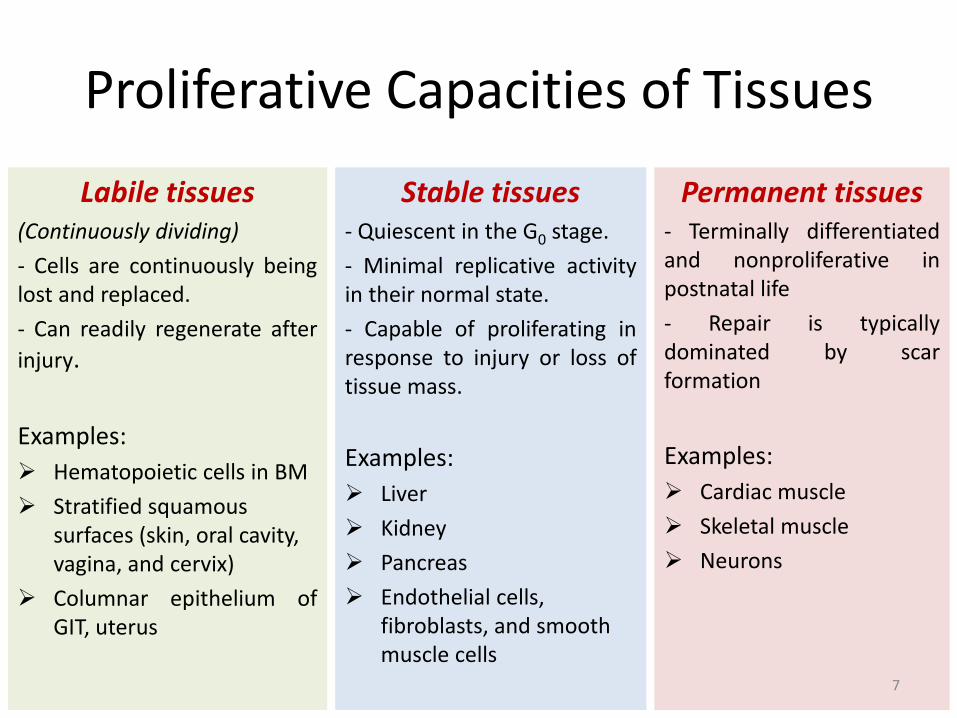
Proliferative Capacities of Tissues
Labile tissues (Continuously dividing)
- Cells are continuously being lost and replaced.
- Can readily regenerate after
injury.
Examples:
Hematopoietic cells in BM
Stratified squamous surfaces (skin, oral cavity, vagina, and cervix)
Columnar epithelium of GIT, uterus
Stable tissues - Quiescent in the G0 stage.
- Minimal replicative activity in their normal state.
- Capable of proliferating in response to injury or loss of tissue mass.
Examples:
Liver
Kidney
Pancreas
Endothelial cells, fibroblasts, and smooth muscle cells
Permanent tissues - Terminally differentiated and nonproliferative in postnatal life
- Repair is typically dominated by scar formation
Examples:
Cardiac muscle
Skeletal muscle
Neurons
7

The Cell Cycle
Cell cycle is the sequence of events that control DNA replication and mitosis
(G1) Presynthetic growth phase
(S) DNA synthesis phase (G2) Premitotic growth phase
(M) Mitotic phase
8

How Does Regeneration Occur?
Cell
ECM
Cell Response (proliferation, locomotion, and differentiation)
Growth factor (GF)
Growth factor receptor (GFR)
9

Soluble Mediators Definition: by convention "growth factor" is used for a protein that expands cell populations by stimulating cell division and by promoting cell survival.
General Properties: Most growth factors have pleiotropic effects: in addition to stimulating cellular
proliferation, they stimulate migration, differentiation and contractility, and enhance the synthesis of specialized proteins (such as collagen in fibroblasts)
A growth factor may act on a specific cell type or on multiple cell types
They induce cell proliferation by binding to specific receptors and affecting the expression of growth control genes
Adjacent cells communicate via gap junctions (narrow, hydrophilic channels that
effectively connect the two cell cytoplasm), allowing movement of small ions, various metabolites, second messengers but not larger macromolecules. 10

Soluble Mediators Extracellular Signaling Mechanisms
Autocrine Signaling: substance acts on the cell that secretes it. Example: compensatory hyperplasia (e.g., liver regeneration)
Paracrine signaling: a substance affects cells in the immediate vicinity of the cell that released the agent. Example: inflammatory cells recruitment to the site of infection and wound healing.
Endocrine signaling: a regulatory substance is released into the bloodstream and acts on target cells at a distance. Example: hormones 11

Soluble Mediators
Cell Surface Receptors Receptors with intrinsic kinase activity can activate other intracellular proteins (e.g.,
RAS, phosphatidylinositol 3-[PI3] kinase, phospholipase Cγ [PLC-γ]).
G-protein-coupled receptors: largest family of plasma membrane receptors. Activate cyclic AMP (cAMP), and generates inositol-1,4,5,-triphosphate (IP3), which releases calcium from the endoplasmic reticulum.
Receptors without intrinsic enzymatic activity: Phosphorylation of Janus kinases (JAKs) activates cytoplasmic transcription factors called STATs (signal transducers and activators of transcription), which shuttle directly into the nucleus.
Intracellular Receptors ligands must be sufficiently hydrophobic to enter the cell (e.g., vitamin D, or steroid and thyroid hormones). Ligand binding leads to the formation of receptor-ligand complexes that directly associate with nuclear DNA and activate or turn off gene transcription.
12

Cell Surface Receptors
RAS activation stimulates the mitogen-activated protein (MAP) kinase cascade, which is involved in the intracellular signaling of many
growth factors (EGF, VEGF, FGF, HGF…)
Transcription factors bind to gene promoters and enhancers to trigger or inhibit transcription
EGF, VEGF, FGF, HGF
Not all ligands induce stimulatory signals!
13
Multiple inflammatory mediators, hormones, all chemokines

Extra-Cellular Matrix (ECM)
14
Extra-Cellular Matrix (ECM)
Components: The interstitial matrix between cells
The basement membranes (nonfibrillar collagen and laminin)
Integrins are transmembrane glycoproteins, the main cellular receptors for ECM components
Collagen is a structural proteins that confer tensile strength
Elastin confers tissue elasticity (ability of tissues to recoil and return to a baseline structure after physical stress)
Adhesive glycoproteins connect cells to underlying ECM components. They include fibronectin (major component of the interstitial ECM) and laminin (major constituent of basement membrane)
Proteoglycans form highly hydrated compressible gels conferring lubrication (such as in the cartilage in joints) and serve as reservoirs for growth factors secreted into the ECM
15

Extra-Cellular Matrix (ECM)
Functions: Mechanical support to tissues (collagens and elastin)
Substrate for cell growth and the formation of tissue microenvironments.
Regulates cell proliferation and differentiation
Determination of cell orientation (polarity)
An intact ECM is required for tissue regeneration, and if the ECM is damaged, repair can only be accomplished by scar formation.
Storage and presentation of regulatory molecules (FGF is excreted and stored in the BM in normal tissues, to be readily involved after local injury)
16

Repair by Connective Tissue
17

Repair by Connective Tissue When? If nondividing cells are injured.
If tissue injury is severe or chronic, and results in damage to parenchymal cells and epithelia as well as the stromal framework
How? 1. within 24 hours of injury: fibroblasts emigration, and fibroblast and endothelial
cell proliferation.
2. By 3 to 5 days, granulation tissue appears. This specialized tissue is characteristic of healing; it is pink, soft with a granular gross appearance, such as that seen beneath the scab of a skin wound. Its histologic appearance is characterized by proliferation of fibroblasts and new thin-walled, delicate capillaries (angiogenesis), in a loose ECM.
3. Progressively, granulation tissue accumulates connective tissue matrix, eventually resulting in the formation of a scar, which may remodel over time.
18
Repair by Connective Tissue
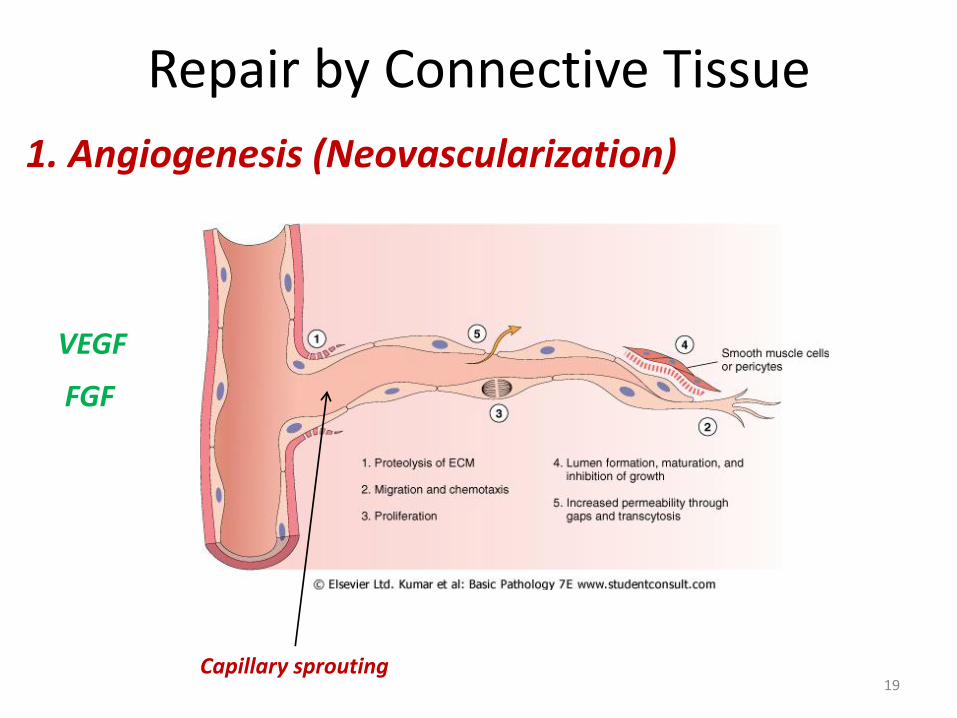
1. Angiogenesis (Neovascularization)
VEGF
FGF
Capillary sprouting 19

Repair by Connective Tissue
Angiogenesis is a critical process in: Healing at sites of injury Development of collateral circulations at sites of
ischemia Allowing tumors to increase in size beyond the
constraints of their original blood supply
Targeting angiogenesis: • Stimulation, e.g., to improve blood flow to a heart
ravaged by coronary atherosclerosis. • Inhibition, to frustrate tumor growth.
20

Repair by Connective Tissue
2. Migration and Proliferation of Fibroblasts Driven by PDGF, FGF, and TGF-β secreted by activated endothelium
and chronic inflammatory cells.
3. ECM Deposition (Scar Formation) Fibroblasts progressively assume a more synthetic phenotype, and
hence there is increased deposition of ECM.
Collagen synthesis, in particular, is critical to the development of strength in a healing wound site.
21

22
Keloid Excess collagen deposition in the skin forming
a raised scar

Repair by Connective Tissue
4. Remodeling of Connective Tissue The degradation of collagens and other ECM components is
accomplished by a family of matrix metalloproteinases (MMPs), which are dependent on zinc ions for their activity
Interstitial collagenases, which cleave fibrillar collagen (type 1,2 and 3)
Gelatinases (Type IV collagenases), which degrade amorphous collagen and fibronectin
MMPs are produced by a variety of cell types (fibroblasts, macrophages, neutrophils, some epithelial cells)
The outcome of the repair process is, in part, a balance between ECM synthesis and degradation
23
Wound Healing Clean, uninfected surgical incision approximated by surgical sutures
The incision causes only focal disruption of epithelial basement membrane continuity and death of a relatively few epithelial and connective tissue cell
Epithelial regeneration predominates over fibrosis (a small scar is formed)
Healing by first intention or primary union
24

Wound Healing Large wounds, abscess formation, ulceration, infarction
Cell or tissue loss is more extensive Regeneration of parenchymal cells alone cannot restore the original
architecture Abundant development of granulation tissue Accumulation of ECM and scarring
Healing by second intention or secondary union
Wound Care in the Wilderness, January 24, 2013
25
Pressure ulcer of the skin, commonly found in diabetic patients

Wound Healing by First Intention
Neutrophils are seen at the incision margin, migrating toward the fibrin clot. Basal cells of the epidermis begin to show increased mitotic activity.
Neutrophils have been largely replaced by macrophages Granulation tissue progressively invades the incision space Epithelial cell proliferation continues By day 5, neovascularization reaches its peak as granulation tissue fills the incisional space Collagen fibers are present at the incision margins
By the end of the first month, the scar comprises a cellular connective tissue largely devoid of inflammatory cells and covered by an essentially normal epidermis. The tensile strength of the wound increases with time to reach 70%-80% by 3 months
2nd week
Continued collagen accumulation and fibroblast proliferation
leukocyte infiltrate, edema, and increased vascularity are substantially diminished.
26
3 to 7 days
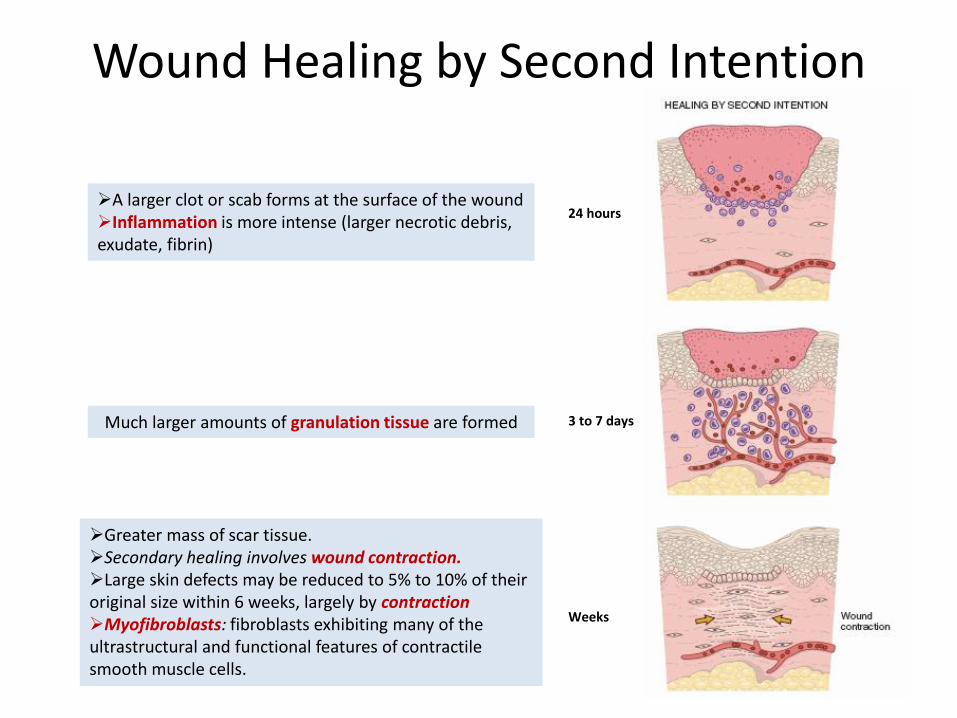
Wound Healing by Second Intention
A larger clot or scab forms at the surface of the wound Inflammation is more intense (larger necrotic debris, exudate, fibrin)
Much larger amounts of granulation tissue are formed
Greater mass of scar tissue. Secondary healing involves wound contraction. Large skin defects may be reduced to 5% to 10% of their original size within 6 weeks, largely by contraction Myofibroblasts: fibroblasts exhibiting many of the ultrastructural and functional features of contractile smooth muscle cells.
27
24 hours
3 to 7 days
Weeks
Wound Strength
• Carefully sutured wounds have approximately 70% of the strength of unwounded skin, largely because of the placement of the sutures.
• When sutures are removed, usually at 1 week, wound strength is approximately 10% of that of unwounded skin, but this increases rapidly over the next 4 weeks.
• The recovery of tensile strength results from collagen synthesis exceeding degradation during the first 2 months
• Wound strength reaches approximately 70% to 80% of normal by 3 months but usually does not substantially improve beyond that point.
28

Factors Affecting Healing
Infection is the single most important cause of delay in healing; it prolongs the inflammation phase of the process and potentially increases the local tissue injury.
Nutrition has profound effects on wound healing. Protein deficiency and
particularly vitamin C deficiency, inhibits collagen synthesis and retards healing.
Glucocorticoids have well-documented anti-inflammatory effects, and their
administration may result in poor wound strength due to diminished fibrosis.
Poor perfusion, due to arteriosclerosis, diabetes…
29

• Complete restoration can occur only in tissues composed of stable and labile cells.
• Even if cells are able to divide, extensive injury will probably result in incomplete tissue regeneration and at least partial loss of function.
• Injury to tissues composed of permanent cells must inevitably result in scarring with, at most, attempts at functional compensation by the remaining viable elements (myocardial infarct).
• Depending on the type and extent of injury, the nature of the injured tissue, and persistence of inflammatory stimuli, injury results often in some degree of residual scarring.
30
References
• ROBBINS Basic Pathology 8th Edition
• Basic Pathology 7th Edition, by Kumar, Cotran and Robbins
• Fibroblast cover image: http://www.gegeonline.nl/anatomie/bindweefsel.html
31

32