
Guidance Hg 2013
34
GUIDANCE ON MAINTAINING AND CALIBRATING NON-MERCURY CLINICAL THERMOMETERS AND SPHYGMOMANOMETERS INTRODUCTION AND DEFINITIONS The replacement of mercury thermometers and sphygmomanometers ሺblood pressure measuring deviceሻ with non‐mercury alternatives is a major step towards mercury‐free health care. A separate guidance document deals with technical specifications 1 . This guidance presents general procedures for maintaining and calibrating common types of non‐mercury thermometers and sphygmomanometers. General information is also provided on validation protocols for non‐mercury devices. This guidance is intended for several audiences and purposes as described below. The main body of the guidance is for users of non‐mercury devices in healthcare facilities. Annex A describes setting up a maintenance system for large hospitals and medical centers with engineering departments. It suggests minimum requirements for a set‐up in a small primary care facility. Annex B1 provides details on accuracy testing of non‐mercury thermometers. Annex B2 describes accuracy testing and calibration procedures for non‐mercury sphygmomanometers. These annexes are intended for large hospitals and medical centers with engineering departments, for health ministries and institutions that test and set requirements for the procurement of medical devices, and for group purchasing organizations. Annex C gives an overview of validation procedures for non‐mercury thermometers and sphygmomanometers. It is intended for health ministries and institutions that set standards and requirements for medical devices and for group purchasing organizations. The procedures can be used as a guide by large hospitals and medical centers to modify clinical accuracy test procedures. DEFINITIONS Maintenance is the periodic servicing of devices to make certain that they are operating properly. Servicing includes regular inspection, cleaning, testing, replacement of worn parts to prevent faults from occurring, and record‐keeping. Maintenance also includes calibration at regular intervals ሺsee belowሻ. These processes help prevent breakdowns and increase the service life of the device. Maintenance can be done by the health facility, by the manufacturer, by an outside group as part of an outsourcing arrangement ሺsubcontractሻ, or by a combination of these. 1 Emmanuel, J. “Guidance on Technical Specifications for Non-Mercury Medical Devices,” UNDP GEF Project, 2011; Shimek, J, Emmanuel, J, Orris, P and Chartier, Y, “Replacement of mercury thermometers and sphygmomanometers in health care: Technical guidance,” World Health Organization, Geneva, Switzerland, 2011; “Affordable technology: blood pressure measuring devices for low resource settings,” World Health Organization, Geneva, Switzerland, 2005; “WHO CVD-risk management package for low- and medium-resource settings,” World Health Organizations, Geneva, Switzerland, 2002.
description
bloodpressure servicing
Transcript of Guidance Hg 2013
GUIDANCE ON MAINTAINING AND CALIBRATING NON-MERCURY CLINICAL THERMOMETERS AND
SPHYGMOMANOMETERS
INTRODUCTION AND DEFINITIONS The replacement of mercury thermometers and sphygmomanometers blood pressuremeasuringdevice withnon‐mercuryalternativesisamajorsteptowardsmercury‐freehealthcare.Aseparateguidancedocumentdealswithtechnicalspecifications1.Thisguidancepresentsgeneralproceduresfor maintaining and calibrating common types of non‐mercury thermometers andsphygmomanometers.Generalinformationisalsoprovidedonvalidationprotocolsfornon‐mercurydevices.Thisguidanceisintendedforseveralaudiencesandpurposesasdescribedbelow.
Themainbodyoftheguidanceisforusersofnon‐mercurydevicesinhealthcarefacilities. AnnexAdescribessettingupamaintenancesystemforlargehospitalsandmedicalcenters
with engineering departments. It suggestsminimum requirements for a set‐up in a smallprimarycarefacility.
Annex B1 provides details on accuracy testing of non‐mercury thermometers. Annex B2describes accuracy testing and calibration procedures for non‐mercurysphygmomanometers.These annexesare intended for largehospitals andmedical centerswith engineering departments, for health ministries and institutions that test and setrequirements for the procurement of medical devices, and for group purchasingorganizations.
Annex C gives an overview of validation procedures for non‐mercury thermometers andsphygmomanometers.Itisintendedforhealthministriesandinstitutionsthatsetstandardsand requirements for medical devices and for group purchasing organizations. Theprocedurescanbeusedasaguidebylargehospitalsandmedicalcenterstomodifyclinicalaccuracytestprocedures.
DEFINITIONSMaintenance is the periodic servicing of devices tomake certain that they are operating properly.Servicingincludesregularinspection,cleaning,testing,replacementofwornpartstopreventfaultsfromoccurring,andrecord‐keeping.Maintenancealso includescalibrationatregular intervals seebelow . These processes help prevent breakdowns and increase the service life of the device.Maintenancecanbedonebythehealthfacility,bythemanufacturer,byanoutsidegroupaspartofanoutsourcingarrangement subcontract ,orbyacombinationofthese.
1 Emmanuel, J. “Guidance on Technical Specifications for Non-Mercury Medical Devices,” UNDP GEF Project, 2011; Shimek, J, Emmanuel, J, Orris, P and Chartier, Y, “Replacement of mercury thermometers and sphygmomanometers in health care: Technical guidance,” World Health Organization, Geneva, Switzerland, 2011; “Affordable technology: blood pressure measuring devices for low resource settings,” World Health Organization, Geneva, Switzerland, 2005; “WHO CVD-risk management package for low- and medium-resource settings,” World Health Organizations, Geneva, Switzerland, 2002.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
2
Calibrationallowstheusertocheckandadjusttheinternalaccuracyofadevice.Calibrationincludescomparing the measurements provided by a test device a thermometer or sphygmomanometerbeingtested againstthemeasurementsfromanaccuratereference.Then,ifthemeasurementsaredifferent, calibration includes adjusting the output of the test device to match the output of thereference device. Calibration can be done by the health facility on a regular basis or by themanufactureraspartofwarrantiesorserviceagreements.Validationistheprocessoftestingadevicefollowinganinternationallyornationallyapprovedtestprotocol and verifying that the devicemeetsminimum standard criteria. Unlike calibrationwhichonlylooksattheinternalaccuracyofthedevicethroughalaboratorytest,validationalsoexaminesdurability, electrical safety, readability, long‐term stability, etc. as well as accuracy in a clinicalsetting.Validation testingmaybedoneby governmental bodies to setminimumrequirements forfacilities or to guide purchasing decisions by government‐run facilities. Validation can also beconducted by non‐governmental organizations to assist institutional members, group purchasingorganizations,orconsumersingeneral.Somelargefacilitiesdovalidationtestsatthefacilitylevelonsamples provided by vendors before purchasing them in order to confirm that products meetinternational,nationalortheirownspecifications.AnoverviewofthevalidationprocessisgiveninAnnexC.
WHY MAINTENANCE AND CALIBRATION ARE IMPORTANT Maintenance and calibration are essential during the life of all temperature and blood pressuremeasuringdevices tomakesure that they functionandcanbeusedproperly.This is true forbothnon‐mercury and mercury devices. Below are summaries of three major studies that show theproblemsthattypicalwearandtearhaveondevicesthathavenotbeenmaintainedorcalibrated.Inaclinicalcomparisonofnon‐mercurythermometerstostandardmercury‐in‐glassthermometers,Leick‐RudeandBloom2 rejected25%of themercury thermometers.These rejected thermometersdifferedbygreaterthan0.2⁰Ccomparedtoareferencethermometer. Notethatinthekeyrangeof37to39⁰C,therequiredaccuracyforbothmercuryanddigitalthermometersis 0.1⁰C .AtalargeteachinghospitalintheUK,Markanduetal.3examined444mercurysphygmomanometers.Theyfoundthat21%hadmercuryoxidationonthecolumnsand18%hadfadedmarkingsorrotatedcolumnsmakingthemdifficulttoread.Theyalsofoundthat20%hadcolumnsthatwerenotvertical,5%hadblockedairfilters,threewereleakingmercurybutwerestillbeingused,and38%hadruinedtubing at the junction to the mercury reservoir. Of the 17 non‐mercury mechanicalsphygmomanometers,12hadneedlesthatdeviatedfrom0bymorethan5mmHgandonemachinehadtheneedlestuckat120mmHg.Servicehistorywasknownforonly23ofthedevicesandmostofthe staff were unaware that mercury and non‐mercury sphygmomanometers required regularservicing.
2 Leick-Rude, MK, Bloom, LF. A comparison of temperature-taking methods in neonates. Neonatal Netw. 1998 August, 17(5): 21-37. 3 Markandu, ND, Whitchener, F, Arnold A and Carney C. The mercury sphygmomanometer should be abandoned before it is proscribed. J Hum Hypertens 2000, 14(1): 31-36.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
3
AstudybyKnightetal.4lookedatmercuryandnon‐mercurydevicesinuseat86generalpracticesinahealthdistrict in theUK.Of472sphygmomanometers ingeneraluse,onlyahandfulhadservicerecordsandnonemetallthequalitystandards.Alargeportionofmercurydeviceshaddefectslikelytoaffectmeasurementtechniqueandonlytwo‐thirdswereaccurateatallpressurelevelstested.Only38.8%of the non‐mercurymechanical deviceswere accurate at all pressure levels tested. SimilartypesofproblemswerereportedbyMcCartneyandCrawford5.
MAINTENANCE & CALIBRATION OF NON-MERCURY CLINICAL THERMOMETERS ALLTYPESOFNON‐MERCURYTHERMOMETERS:Always follow maintenance procedures in the manufacturer’s instructions. If no maintenanceinstructionsarefound,theproceduresbelowcanbeusedasaguide:Inspection:Checkthe thermometer forgeneralcleanliness.Checkthedisplay tomakesure thatallalphanumeric segments or pixels are working properly to avoid incorrect reading of the display.Checkbuttonsandswitches.Checkforanywornorbrokenparts.Returntothemanufactureriftherearebrokenpartsordisplayproblems.Battery testing:Check thebattery indicator in thedisplayor test thebatterywithabattery tester.Replacespentordefectivebatteriesaccordingtothemanufacturer’sinstructions.Batteriesshouldbedisposedofproperlyashazardouswaste.Ifthedeviceusesacharger,makesurethebatterychargingstationisworkingproperly.Recordkeeping: Keep a maintenance record with the following information: serial number oridentification number of the device; date of servicing; results of inspection, battery testing, andfunctiontesting;typeofreferencethermometerusedandresultofaccuracytesting ifconductedatthattime;actionstaken;andnameofservicepersonnel.DIGITAL: If no maintenance instructions are found for the digital thermometer, the following additionalprocedurescanbeusedasaguide:Inspection:Checktheconditionof theprobetip. If the thermometerhasaremovableprobe,checktheprobecordforbreaksintheinsulationandcheckthecontactsoftheconnector.Ifprobecoversareused,checkthatallprobecoversarenewandundamaged.Returntothemanufacturer if therearebrokenpartsordisplayproblems.Cleaninganddisinfection:Theexteriorofmostdigitalthermometerscanbecleanedwithmildsoapandwarmwaterorwithadampcloth.Todisinfect,use70%isopropylalcoholor70%ethanol.Forsomedigitalthermometers,theprobetipcanbepartiallyimmersedinisopropylalcoholforashorttime.
4 Knight, T, Leech, F, Jones, A, Walker, L, Wickramasinghe, R, Angris, S and Rolfe, P. Sphygmomanometers in use in general practice: an overlooked aspect of quality in patient care. J Hum Hypertens 2001, 15(10): 681-684. 5 McCartney, P and Crawford, D. Inaccurate, leaky sphygmomanometers are still common. Brit J Gen Pract 2003 January, 53(486): 61-62.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
4
Function testing: Manydigital thermometershaveanautomatic internal self‐testwhen turnedonanddisplayanerrormessageorwarningifthethermometerisnotfunctioningproperly.Inadditiontotheautomaticself‐test,checkother functionsandfeaturesthat the thermometermayhave. Forexample, check high and low temperature warnings, memory displays of previous recordedreadings ,indicationwhenpeaktemperatureorfinaltemperatureisreached,audibleorvisualalertsbeepsorlights ,automaticshut‐offafteraspecifiedperiodofinactivity,temperaturescaleselection,etc.Accuracytestingandcalibration:Whilesomemanufacturersrecommendtestingforaccuracyeverytwoyears,anaccuracycheckatleasteverysixmonthsisrecommended.Alwaystesttheaccuracyifthe thermometer has been dropped or if temperature readings are questionable. Many digitalthermometers cannot be adjusted. Some advanced digital thermometers come with a calibrationtester. If the thermometer exceeds the maximum permissible error within the measuring range,followthemanufacturer’sinstructionsforcalibrationandadjustmentorreturnthethermometertothemanufacturer foradjustmentorreplacement. If themanufacturerdoesnotprovideproceduresfortestingaccuracy,seeAnnexB1forsuggestedprocedures.TEMPORALIR:If no maintenance instructions are found for the temporal forehead artery infrared IR thermometer,thefollowingadditionalprocedurescanbeusedasaguide:Inspection:Checktheconditionoftheprobelensandcone.Ifthethermometercomeswithacharger,checkthepoweradapterorchargingstationforcleanlinessandanywornorbrokenparts.Returntothemanufactureriftherearebrokenparts.Cleaninganddisinfection:Theexteriorofmost temporal thermometerscanbecleanedwitha softcloth. The probe lens should be cleaned regularly of any dirt, greasy film andmoisture. Cleaningshould be done bywiping gentlywith a small cloth or swabmoistenedwith alcohol or by gentlyblowingwithcompressedair.Donotuseanyabrasivecleanersthatmayscratchthethermometer.When cleaning the probe lens and cone, one may have to hold the thermometer downwards topreventmoisture from entering the sensor area. If excessmoisture gets in, allow the area to drybeforeusing.Functiontesting:ManytemporalIRthermometershaveanautomaticinternalself‐testwhenturnedon and display an error message or warning if the thermometer is not functioning properly. Inaddition to the automatic self‐test, check other functions and features that the thermometermayhave. For example, check switching from surface to body temperaturemeasurements, focusing ortrackinglights,warningifthemeasuringdistanceistoocloseortoofar,highandlowtemperaturewarnings,memory displaysofpreviousrecordedreadings ,audibleorvisualalerts beeps,buzzers,or flashing lights , backlight, automatic shut‐off after a specified period of inactivity, temperaturescaleselection,continuousscanning,long‐termcalibrationdriftcorrection,etc.Accuracytestingandcalibration:Somemanufacturersrecommendtesting foraccuracyeveryyear.Others recommendmore frequent testing. Some temporal IR thermometershavea self‐calibrationfunction, which, their manufacturers claim eliminates the need for calibration. Always test theaccuracyifthethermometerhasbeendropped.ManytemporalIRthermometershavenomeansofadjustment.Ifthethermometerexceedstheerrorrangedescribedinthemanufacturer’sinstructions,return the thermometer to themanufacturer for adjustment or replacement. If themanufacturerdoesnotprovideproceduresfortestingaccuracy,seeAnnexB1forsuggestedprocedures.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
5
TYMPANICIR:If no maintenance instructions are found for the tympanic ear infrared IR thermometer, thefollowingadditionalprocedurescanbeusedasaguide:Inspection: Check the condition of the probe the cone‐shaped tube that is inserted into the ear ,payingspecialattentiontotheprobewindow.Checkthatprobecoversarenewandundamaged.Ifthethermometercomeswithacharger,checkthepoweradapterorchargingstationforcleanlinessand any worn or broken parts. Return to the manufacturer if the probe window or probe tip isdamagedoralteredinanyway.Cleaninganddisinfection:TheexteriorofmanytympanicIRthermometerscanbecleanedwithasoftclothslightlymoistenedwithalcohol.Theprobewindowmustbecleanedregularlyofanydust,dirt,fingerprints, and cerumen earwax by gentlywipingwith a cotton swab slightlymoistenedwithalcohol.Allowtheprobewindowtodrycompletelybeforeuse.Function testing: If there is an automatic internal self‐test function, use it to determine if thethermometerisfunctioningproperly.Checkotherfunctionsandfeaturesthatthethermometermayhave. For example, check high and low temperature warnings, probe cover ejector, probe coverindicator, ear positioning error warning, memory displays of previous recorded readings ,indicationwhen final temperature is reached,audibleandvisualalerts beepsand flashing lights ,automaticshut‐offafteraspecifiedperiodofinactivity,temperaturescaleselection,etc.Accuracy testing and calibration: Somemanufacturers recommend testing for accuracy every twoyears.Alwaystesttheaccuracyifthethermometerhasbeendropped.Manytympanicthermometershave no means of adjustment. If the thermometer exceeds the error range described in themanufacturer’s instructions, , return the thermometer to the manufacturer for adjustment orreplacement.Ifthemanufacturerdoesnotprovideproceduresfortestingaccuracy,seeAnnexB1forsuggestedprocedures.COMBINEDIR: Combined ear/forehead infrared IR thermometers are similar to temporal and tympanic IRthermometers except that they generally have removable probe covers when used for temporalarterymeasurements.Alwaysfollowmaintenanceproceduresinthemanufacturer’sinstructionsforthe combined IR thermometer. If nomaintenance instructions are provided, amodification of theproceduresabovefortemporalandtympanicIRthermometerscanbeused.
MAINTENANCE & CALIBRATION OF NON-MERCURY SPHYGMOMANOMETERS ALLTYPESOFNON‐MERCURYSPHYGMOMANOMETERS: Always follow maintenance procedures in the manufacturer’s instructions. If no maintenanceinstructionsarefound,theproceduresbelowcanbeusedasaguide:Inspection:Checkthesphygmomanometer forgeneralcleanliness.Checktheconditionof thebulb,valves,tubingandcuff.Checktubingforcracksandtestforairleaks.Checkforanywornorbrokenparts.Returntothemanufactureriftherearebrokenpartsordisplayproblems.Cleaninganddisinfection:Checkwiththemanufacturerwhichcleaninganddisinfectionmethodtheyrecommend.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
6
Some cuffs can be cleanedwith amild enzymatic detergent followed by brushing with asterilebrush,thenrinsingwithdistilledwaterforfiveminutes.
Somecuffscanbewashedincoolwaterwithamildsoaporwithadetergent‐disinfectant,followedbyrinsing.
Some cuffs have removable bladders. Thebladders canbe cleanedwith ethanolwhile thecuffscanbewashedseparatelyinsoapandwarmwater.
Somecuffs,afterremovingthebladder,canbecleanedinawashingmachinewithagentlecycle,coolorwarmwater,andamilddetergentbutthecuffportmustbecappedtopreventwaterfromgettinginsidethecuff.
Afterwashing,cuffsshouldbeallowedtodryinair. Thebulb, tubes, andvalves canbe cleanedwitha slightlydampclothoralcoholpadwith
70%alcoholor0.5%bleach.If disinfection is needed, some cuffs can be sprayed with a 10% bleach solution, brushed with asterilebrush,thenrinsedwithdistilledwaterforfiveminutes,andallowedtoairdry.Recordkeeping: Keep a maintenance record with the following information: serial number oridentification number of the device; date of servicing; results of inspection, battery testing ifapplicable , and function testing; reference manometer used and result of the accuracy test ifconductedatthattime;actionstaken;andnameofservicepersonnel.ANEROID MECHANICALGAUGE :If no maintenance instructions for the aneroid sphygmomanometer with a mechanical gaugemechanicaldial arefound,thefollowingadditionalprocedurescanbeusedasaguide:Inspection: Check the condition of the gauge glass and the readability of the markings in thefaceplate.Returntothemanufactureriftherearebrokenpartsordisplayproblems.Cleaning and disinfection: Many mechanical manometer gauges can be cleaned with a soft dampclothoranalcoholpadwith70%alcohol.Functiontesting:Checkforleaksinthesystem.Thiscanbedonebyinflatingtheunitandseeingifthegaugepointerdropsslowly.Ifthereisaslowleak,asmallamountofsoapywatercanbeusedtofind the leak. Leaks are usually found in connection points between the tubing and fittings, adefectiveairreleasevalve,orinacrackinthetubing,cuff,orinflationbulb.Leaksbetweenfittingsand tubing or between the inflation bulb and fitting can often be repaired by tightening theconnectionorbycuttinganylooseexpandedtubingandreconnecting.Crackedtubingorbulbshavetobereplaced.Checkforthezeropoint.Thiscanbedonebyfullydeflatingtheunitandseeingifthegaugeneedlereturnstozero 0mmHg orwithinthezerozone asmallmarkedareaaroundthezeropointfoundinsomeaneroidgauges .Iftheneedleisoutsidethezerozone,checkwiththemanufactureronhowtoadjusttheneedle.Belowaresomeofthecommonwaysofadjustingthepointer:
Manygaugeshaveanadjustmentscrewtoresetthezeropoint;theadjustmentscrewmaybeatthebackorinthestemwherethetubingisconnectedtothegauge.
With other models, the glass is removed from the front of the gauge and the pointer iscarefullymovedtothezeroposition.
The zero point in some large‐face gauges can be adjusted by removing the tube from theundersideoftheaneroidface,insertingasmallflat‐headscrewdriverortoolprovidedbythemanufacturer into the connector from where the tube was removed, and turning thescrewdriverortooluntiltheneedleisatzero.
Inothergauges,thezeropointisadjustedbyslightlyrotatingthedialface.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
7
Wheneverthezeropointisoff,anaccuracytestshouldbedone.Accuracy testing and calibration: Somemanufacturers recommend a yearly calibration test,whileothers recommend a calibration check every two years. For frequently used aneroidsphygmomanometers in a healthcare facility, a calibration test every month is ideal unlessmaintenance records indicate the need for more or less frequent checks. A sphygmomanometershouldalwaysbecalibratedif ithasbeendroppedorifthepointerneedleisoutsidethezerozonewhen the unit is fully deflated. Annex B2 provides examples of detailed procedures for accuracytestingandcalibration.ELECTRONIC INCLUDINGDIGITAL,AUTOMATED,SEMI‐AUTOMATED,ANDOSCILLOMETRIC : If no maintenance instructions for the electronic sphygmomanometer are found, the followingadditionalprocedurescanbeusedasaguide:Inspection: Check the display tomake sure that all alphanumeric segments or pixels areworkingproperly.Thiswillavoidincorrectreadingofthedisplay.Checkallcablesforbreaksintheinsulation.Insomeelectronicunits,checkingforairleakscanbedoneasfollows:
a Wrap the cuff around a vertical pipe or tube about the size of an adult’s or child’s armdependingonthecuffsize ;
b Makesurethatthearterymarkispointingdownward;c Temporarilysealthepressurereleasehole usuallyinthebackorsideoftheunit ;d Turnontheunit;ande Seeifthereareanyleaksasthecuffisinflated.
Iftheunitcomeswithacharger,checkthepoweradapterorchargingstationforcleanlinessandanywornorbrokenparts.Returntothemanufactureriftherearebrokenpartsordisplayproblems.Cleaninganddisinfection:Ingeneral,theelectronicunitscanbecleanedwithadry,softcloth.Someunitscanbecleanedwithadamp,softclothorwithaclothmoistenedwithsoapywater.Batterytesting:Iftheunitusesbatteries,checkthebatteryindicatorinthedisplayortestthebatterywith a battery tester. Replace spent or defective batteries according to the manufacturer’sinstructions.Iftheunitusesrechargeablebatteries,replacethebatterieswhentheynolongerholdchargeforverylong.Batteriesshouldbedisposedofproperlyashazardouswaste.Function testing: Manyelectronic sphygmomanometershaveanautomatic internal self‐testwhenturned on and display an errormessage if the unit is not functioning properly. In addition to theautomatic self‐test, checkother functionsand features that theunitmayhave.Forexample, checkautomatic and manual modes, pulse monitoring and pulse indication, arm movement detectionwarning,audibleandvisualalerts beepsandflashinglights ,memoryfunctions,graphdisplays,dateandtime,automaticshut‐offafteraperiodofinactivity,wirelesscommunicationsfunctions,etc.Accuracytestingandcalibration:Somemanufacturersrecommendtesting foraccuracyeveryyear,otherseverytwoyears.Somemanufacturersstatethattheirelectronicsphygmomanometersdonotneed re‐calibration even when dropped because of the characteristics of their technology. For ahealthcarefacility,anaccuracytesteverysixmonthsisidealunlessmaintenancerecordsindicatetheneedformorefrequentchecks.Asphygmomanometershouldbetestedifithasbeendropped.Someelectronicsphygmomanometerscannotbetestedand/orcalibratedbytheuserandmustbesenttothemanufactureroranapprovedtechnicianorservicecenterfortestingandcalibration.Annex B2 provides an example of procedures for accuracy testing and calibration. Digitalsphygmomanometers that are based on the traditional auscultative method listening to internal
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
8
body sounds but use digital displays, electronic sphygmomanometers that have an auscultativemode,andelectronicsphygmomanometerswithacalibrationcheckor testmodecanbe tested foraccuracyusingatestset‐upandproceduressimilartothoseforaneroidsphygmomanometers.Otherelectronicsphygmomanometersthatusetheoscillometricmethod measuringtheoscillationscaused by arterial pressure as the arterial walls expand and contract against the cuff , digitalKorotkofftechnology,oracombinationofthesecanbetestedusingclinicalaccuracytestprocedures.If the sphygmomanometer does not meet the pass criteria, return it to the manufacturer foradjustmentorreplacement.
JorgeEmmanuel,PhDChiefTechnicalAdvisor
withinputfromPeterOrris,MD,MeghaRathi,PhD,andShanthiMendis,MD
UNDPGEFProjectJuly2013
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
9
ANNEXA
SETTING UP A MAINTENANCE SYSTEM Most equipment, including thermometers and sphygmomanometers, require regular, or periodic,maintenance. Reactive maintenance is taking action only when something breaks. Preventivemaintenanceistakingactiononaspecificschedule.Preventativemaintenancecanextendequipmentlife by detecting, avoiding, or reducing the impact of failures and slowing down wear and tear.Another approach, predictive maintenance, is similar to preventive maintenance except that theserviceisdonebasedonusageorconditionoftheequipmentratherthanonapresetschedule.Forexample, ifamanufacturerpredictsbatterylifeofadigitalthermometerat300measurements,thepredictivemaintenanceschedulewouldincludeservicebefore300measurementshavebeentaken.Becauseof the importanceofperiodic testing foraccuracy,a combinationof scheduledpreventivemaintenance and predictivemaintenance is recommended. Preventivemaintenance ismore laborintensive than reactive maintenance and can sometimes lead to unneeded maintenance orunnecessary replacement of parts if not done carefully. However, a well‐planned preventive andpredictivemaintenance system can reduce long‐termcosts andavoidproblems and costly repairswhileincreasingtheconfidenceofhealthprovidersintheuseofthedevices.When developing a preventive and/or predictive maintenance system, support by seniormanagementisessential.Summarizingthefailurehistoriesandinformationonthecostsoffailuresmay help get support from management. A maintenance policy should be issued by the facilitydirector or manager. The policy should define which department is responsible formaintenance,such as the facility’s engineering department. Having well‐respected staff promote the newmaintenance policy will help change workplace culture and attitudes about maintenance.Maintenance is often in‐house but some large health institutions outsource subcontract theirmaintenanceprograms.Developingamaintenancesystemincludes:
1. Conductinganinventoryofeachdeviceinthefacility brandname,serialnumber,locationofuseorstorage,dateofpurchase,datesofpastmaintenanceandactionstaken ,
2. Developingasystemtomanagemaintenance information forexample,amaintenance logbookormaintenancetrackingsoftware ,
3. Developing a maintenance plan and schedule based on preventive and/or predictiveapproachesguidedbymanufacturers’instructionsandthefacility’shistoryofpastfailures,
4. Sharinginformationwithrelevantdepartments suchasprocurement,centralsupply,etc. ,
5. Coordinatinglogisticswithdepartmentsandwardswherethedevicesareusedorstored,
6. Trainingofmaintenancestaff,and
7. Allocatinganannualbudgetformaintenance.Scheduling themaintenanceof thermometers and sphygmomanometers shouldbe spacedout andtimedinsuchawayastoensureavailabilityofthesedeviceswhenandwheretheyareneededbythemedicalandnursingstaff.Themaintenanceplancouldbepartofaqualityimprovementstrategyandincludemeasuresofeffectiveness,annualreview,andupdatingoftheplan.Forasmallhealthcarefacility,thefollowingareminimumrequirementsforsettingupamaintenancesystem:
1. Assignoneormorepersonstoberesponsibleformaintenance.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
10
2. Conductaninventoryofthedevicesthatrequiremaintenance.
3. Developamaintenanceplan, includingabudgetandschedules forperiodic inspectionandtesting.
4. Traintheperson s responsibleformaintenance.
5. Implementperiodicmaintenanceandrecordkeeping.
6. Reviewthemaintenanceplaneveryyearandupdatetheplanasneeded.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
11
ANNEXB1
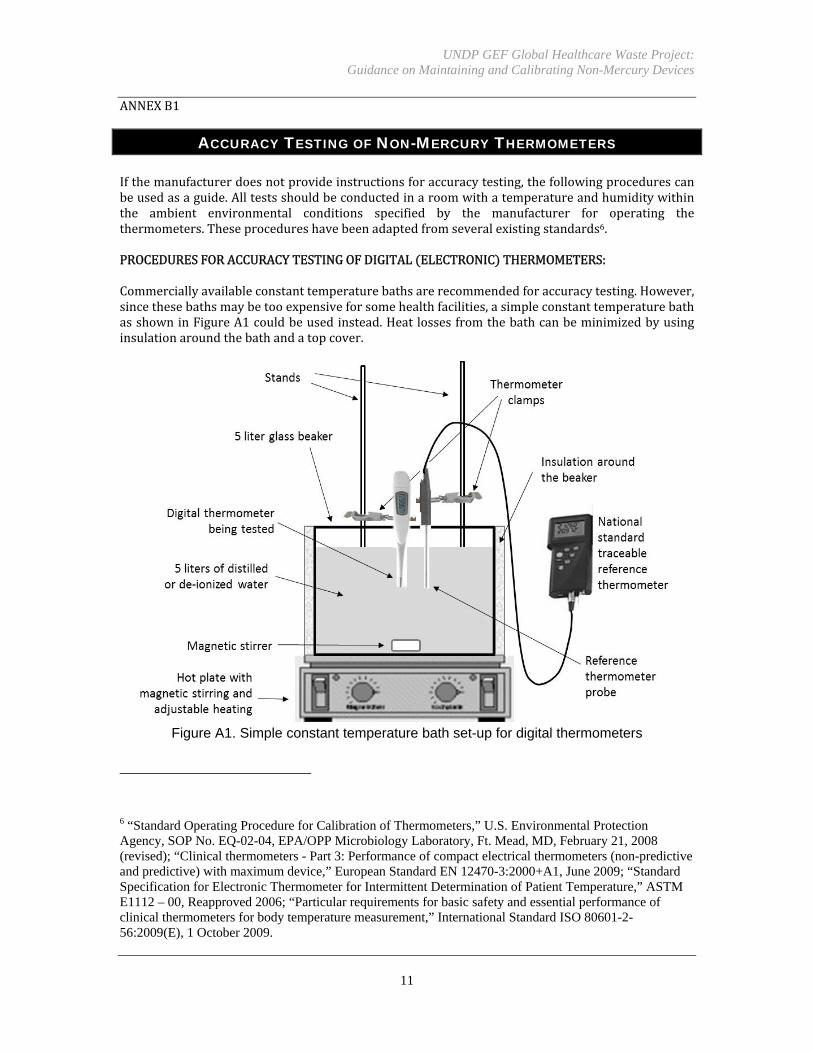
ACCURACY TESTING OF NON-MERCURY THERMOMETERS Ifthemanufacturerdoesnotprovideinstructionsforaccuracytesting,thefollowingprocedurescanbeusedasaguide.Alltestsshouldbeconductedinaroomwithatemperatureandhumiditywithinthe ambient environmental conditions specified by the manufacturer for operating thethermometers.Theseprocedureshavebeenadaptedfromseveralexistingstandards6.PROCEDURESFORACCURACYTESTINGOFDIGITAL ELECTRONIC THERMOMETERS:Commerciallyavailableconstanttemperaturebathsarerecommendedforaccuracytesting.However,sincethesebathsmaybetooexpensiveforsomehealthfacilities,asimpleconstanttemperaturebathasshowninFigureA1couldbeusedinstead.Heatlossesfromthebathcanbeminimizedbyusinginsulationaroundthebathandatopcover.
Figure A1. Simple constant temperature bath set-up for digital thermometers
6 “Standard Operating Procedure for Calibration of Thermometers,” U.S. Environmental Protection Agency, SOP No. EQ-02-04, EPA/OPP Microbiology Laboratory, Ft. Mead, MD, February 21, 2008 (revised); “Clinical thermometers - Part 3: Performance of compact electrical thermometers (non-predictive and predictive) with maximum device,” European Standard EN 12470-3:2000+A1, June 2009; “Standard Specification for Electronic Thermometer for Intermittent Determination of Patient Temperature,” ASTM E1112 – 00, Reapproved 2006; “Particular requirements for basic safety and essential performance of clinical thermometers for body temperature measurement,” International Standard ISO 80601-2-56:2009(E), 1 October 2009.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
12
1. Prepareawell‐stirredconstant‐temperaturebathwithacapacityofatleast5liters.Fillthe
containertocapacitywithdistilledorde‐ionizedwater.Heatthebathgraduallytothelowesttemperature of themeasuring range. Verify the temperature of the bathwith a referencethermometercalibratedwithin0.03°ContheInternationalTemperatureScaletraceabletoanationalstandardlaboratory.
2. Upon reaching the desired temperature, monitor the temperature of the bath for several
minutestomakesurethebathisinthermalequilibrium.
3. Insertthedigitalthermometertobetestedasnearaspossibletothereferencethermometer.Make sure there is adequate space for water to flow between them. More than onethermometercanbetestedatatime.Makesurethatalldevicesareimmersedtotheproperdepthsaccordingtomanufacturers’instructions.Note:Ifthethermometerusesadisposableprobe coveror sheath, be sure to place a probe cover or sheathon the test thermometerbeforeinsertinginthewaterbath.
4. Conductthetestsatthreepointswithinthepracticaltemperaturerangeofthedevice,such
asat36,38,and40°C.Recordmeasurementswhenthe thermometerhasreachedthermalequilibriumwiththewaterbathorforthetimeperiodspecifiedbythemanufacturer.
5. Calculate the error for each individual temperature using the equation
Error Test thermometer reading – Reference thermometer reading . Note that theerrorcanbepositiveornegative.Forexample:
Error ‐0.2°C 35.8°C–36.0°C
6. Comparethemaximumerrorforthemeasuringrangewiththatofthetwostandardsshownbelow in Tables A1 and A2 to determine if the digital thermometer meets the requiredaccuracy.Themaximumpermissibleerroristheabsolutevalue,i.e.,regardlessoftheplusorminussign.
7. Thetestscanbeconductedthreetimestotestforrepeatability.
8. Keep a record of the test, including: serial number or identification number of the
thermometer; date of testing; type of reference thermometer used; for each testtemperature,thetestthermometerreading,referencethermometerreading,andcalculatederror;actiontakenifany;andnameofservicepersonnel
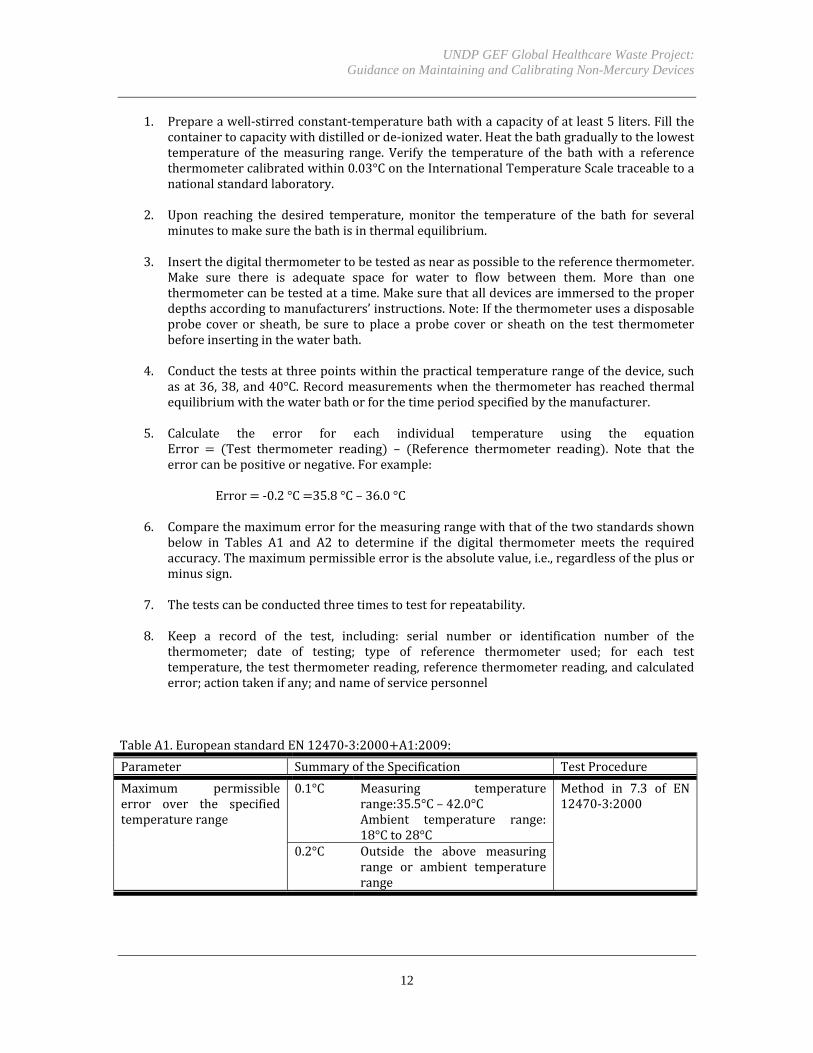
TableA1.EuropeanstandardEN12470‐3:2000 A1:2009:
Parameter SummaryoftheSpecification TestProcedure
Maximum permissibleerror over the specifiedtemperaturerange
0.1°C Measuring temperaturerange:35.5°C– 42.0°CAmbient temperature range:18°Cto28°C
Method in 7.3 of EN12470‐3:2000
0.2°C Outside the above measuringrange or ambient temperaturerange
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
13
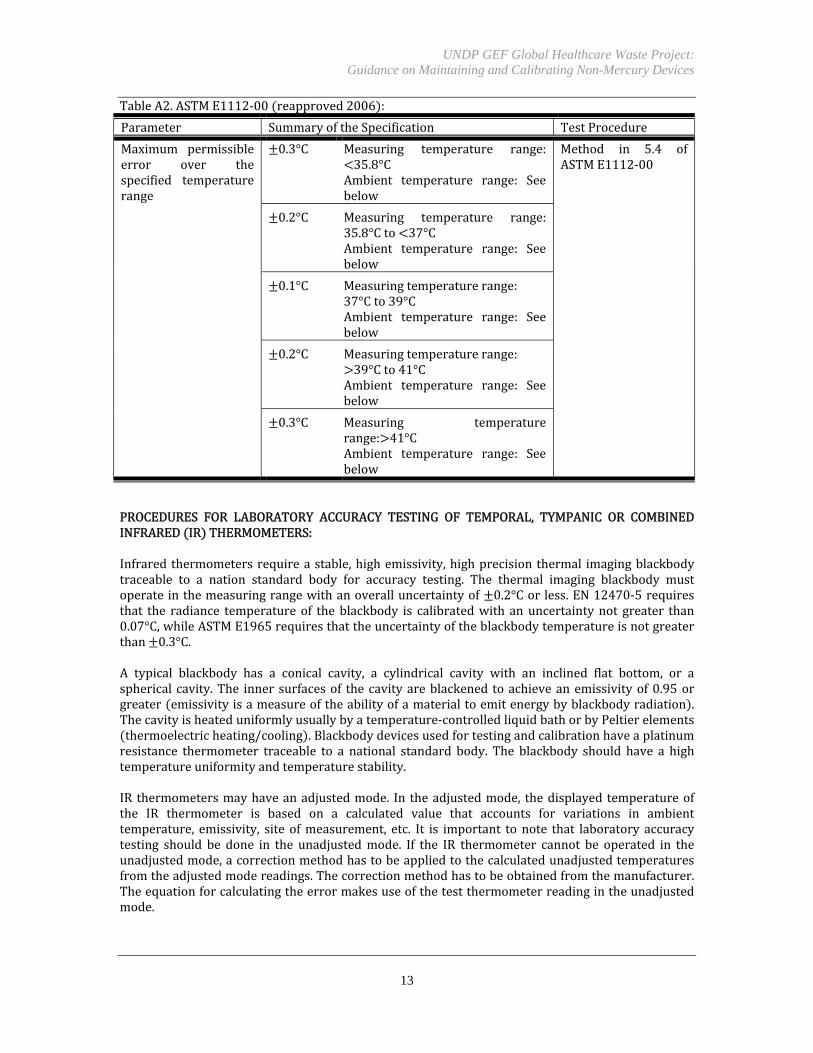
TableA2.ASTME1112‐00 reapproved2006 :
Parameter SummaryoftheSpecification TestProcedure
Maximum permissibleerror over thespecified temperaturerange
0.3°C Measuring temperature range:35.8°C
Ambient temperature range: Seebelow
Method in 5.4 ofASTME1112‐00
0.2°C Measuring temperature range:35.8°Cto 37°CAmbient temperature range: Seebelow
0.1°C Measuringtemperaturerange:37°Cto39°CAmbient temperature range: Seebelow
0.2°C Measuringtemperaturerange:39°Cto41°C
Ambient temperature range: Seebelow
0.3°C Measuring temperaturerange: 41°CAmbient temperature range: Seebelow
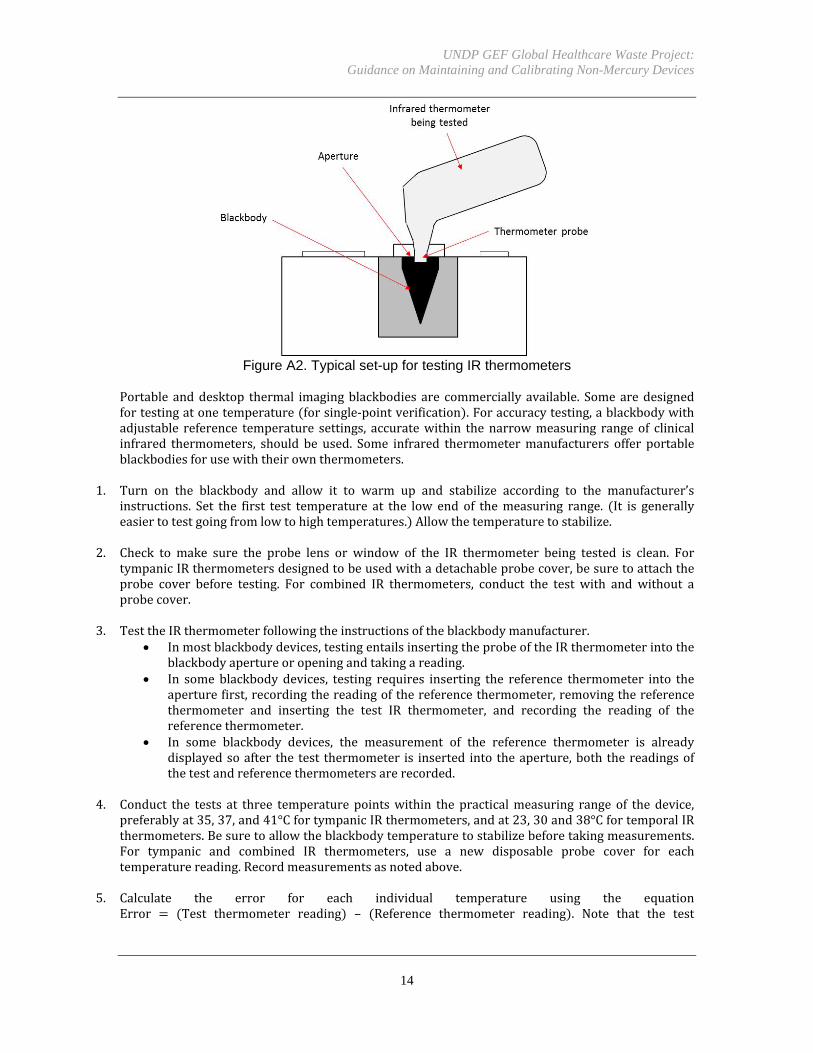
PROCEDURES FOR LABORATORY ACCURACY TESTING OF TEMPORAL, TYMPANIC OR COMBINEDINFRARED IR THERMOMETERS:Infraredthermometersrequireastable,highemissivity,highprecisionthermal imagingblackbodytraceable to a nation standard body for accuracy testing. The thermal imaging blackbody mustoperateinthemeasuringrangewithanoveralluncertaintyof 0.2°Cor less.EN12470‐5requiresthat the radiance temperature of theblackbody is calibratedwith anuncertaintynot greater than0.07°C,whileASTME1965requiresthattheuncertaintyoftheblackbodytemperatureisnotgreaterthan 0.3°C.A typical blackbody has a conical cavity, a cylindrical cavity with an inclined flat bottom, or asphericalcavity.The inner surfacesof thecavityareblackened toachieveanemissivityof0.95orgreater emissivityisameasureoftheabilityofamaterialtoemitenergybyblackbodyradiation .Thecavityisheateduniformlyusuallybyatemperature‐controlledliquidbathorbyPeltierelementsthermoelectricheating/cooling .Blackbodydevicesusedfortestingandcalibrationhaveaplatinumresistance thermometer traceable to a national standard body. The blackbody should have a hightemperatureuniformityandtemperaturestability.IR thermometersmayhaveanadjustedmode. In theadjustedmode, thedisplayed temperatureofthe IR thermometer is based on a calculated value that accounts for variations in ambienttemperature, emissivity, site ofmeasurement, etc. It is important to note that laboratory accuracytesting should be done in the unadjustedmode. If the IR thermometer cannot be operated in theunadjustedmode,acorrectionmethodhastobeappliedtothecalculatedunadjustedtemperaturesfromtheadjustedmodereadings.Thecorrectionmethodhastobeobtainedfromthemanufacturer.Theequationforcalculatingtheerrormakesuseofthetestthermometerreadingintheunadjustedmode.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
14
Figure A2. Typical set-up for testing IR thermometers
Portable anddesktop thermal imagingblackbodies are commercially available. Somearedesignedfortestingatonetemperature forsingle‐pointverification .Foraccuracytesting,ablackbodywithadjustable reference temperature settings, accuratewithin the narrowmeasuring range of clinicalinfrared thermometers, should be used. Some infrared thermometermanufacturers offer portableblackbodiesforusewiththeirownthermometers.
1. Turn on the blackbody and allow it to warm up and stabilize according to the manufacturer’sinstructions. Set the first test temperature at the low end of themeasuring range. It is generallyeasiertotestgoingfromlowtohightemperatures. Allowthetemperaturetostabilize.
2. Check to make sure the probe lens or window of the IR thermometer being tested is clean. FortympanicIRthermometersdesignedtobeusedwithadetachableprobecover,besuretoattachtheprobe cover before testing. For combined IR thermometers, conduct the test with and without aprobecover.
3. TesttheIRthermometerfollowingtheinstructionsoftheblackbodymanufacturer. Inmostblackbodydevices,testingentailsinsertingtheprobeoftheIRthermometerintothe
blackbodyapertureoropeningandtakingareading. In some blackbody devices, testing requires inserting the reference thermometer into the
aperturefirst,recordingthereadingofthereferencethermometer,removingthereferencethermometer and inserting the test IR thermometer, and recording the reading of thereferencethermometer.
In some blackbody devices, the measurement of the reference thermometer is alreadydisplayedsoafter the test thermometer is inserted into theaperture,both thereadingsofthetestandreferencethermometersarerecorded.
4. Conduct the tests at three temperaturepointswithin the practicalmeasuring range of thedevice,
preferablyat35,37,and41°CfortympanicIRthermometers,andat23,30and38°CfortemporalIRthermometers.Besuretoallowtheblackbodytemperaturetostabilizebeforetakingmeasurements.For tympanic and combined IR thermometers, use a new disposable probe cover for eachtemperaturereading.Recordmeasurementsasnotedabove.
5. Calculate the error for each individual temperature using the equationError Test thermometer reading – Reference thermometer reading . Note that the test
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
15
thermometerreadingmustbeintheunadjustedmodeandtheerrorcanbepositiveornegative.Forexample:
Error ‐0.2°C 35.8°C–36.0°C
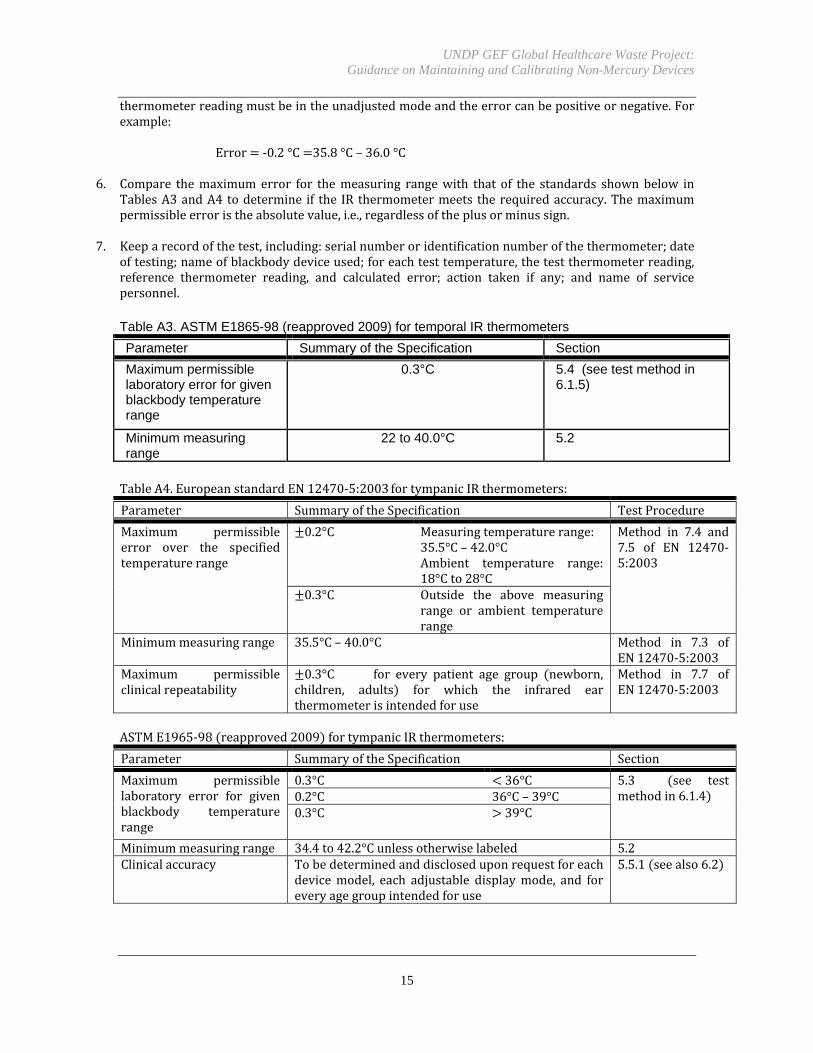
6. Compare themaximumerror for themeasuring rangewith that of the standards shownbelow inTablesA3andA4todetermine if the IR thermometermeets therequiredaccuracy.Themaximumpermissibleerroristheabsolutevalue,i.e.,regardlessoftheplusorminussign.
7. Keeparecordofthetest,including:serialnumberoridentificationnumberofthethermometer;dateoftesting;nameofblackbodydeviceused;foreachtesttemperature,thetestthermometerreading,reference thermometer reading, and calculated error; action taken if any; and name of servicepersonnel.
Table A3. ASTM E1865-98 (reapproved 2009) for temporal IR thermometers
Parameter Summary of the Specification Section
Maximum permissible laboratory error for given blackbody temperature range
0.3°C 5.4 (see test method in 6.1.5)
Minimum measuring range
22 to 40.0°C 5.2
TableA4.EuropeanstandardEN12470‐5:2003fortympanicIRthermometers:
Parameter SummaryoftheSpecification TestProcedure
Maximum permissibleerror over the specifiedtemperaturerange
0.2°C Measuringtemperaturerange:35.5°C– 42.0°CAmbient temperature range:18°Cto28°C
Method in 7.4 and7.5 of EN 12470‐5:2003
0.3°C Outside the above measuringrange or ambient temperaturerange
Minimummeasuringrange 35.5°C– 40.0°C Method in 7.3 ofEN12470‐5:2003
Maximum permissibleclinicalrepeatability
0.3°C for every patient age group newborn,children, adults for which the infrared earthermometerisintendedforuse
Method in 7.7 ofEN12470‐5:2003
ASTME1965‐98 reapproved2009 fortympanicIRthermometers:
Parameter SummaryoftheSpecification Section
Maximum permissiblelaboratory error for givenblackbody temperaturerange
0.3°C 36°C 5.3 see testmethodin6.1.40.2°C 36°C– 39°C
0.3°C 39°C
Minimummeasuringrange 34.4to42.2°Cunlessotherwiselabeled 5.2Clinicalaccuracy Tobedeterminedanddiscloseduponrequestforeach
devicemodel, each adjustable displaymode, and foreveryagegroupintendedforuse
5.5.1 seealso6.2

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
16
ANNEXB2
ACCURACY TESTING AND CALIBRATION OF NON-MERCURY
SPHYGMOMANOMETERS Thetraditionalmethodtomeasurebloodpressureisauscultation listeningtointernalbodysounds of the Korotkoff sounds using a mercury sphygmomanometer. The mercury column manometerincludingitsplacement,angle,clarityofmarkingsandscaleresolution isonlyonepotentialsourceoferrorinbloodpressuremeasurements.Othersourcesoferrorrelateto:
Usererror includingwrongplacementof thecuff,poorarmpositioning, inappropriateairpressuredeflationrate,inadequatepatientrestperiod,wrongplacementofthestethoscopediscorcup,clothingobstructiononthearm ;
Observer bias including prejudicial influence by what the observer wants the bloodpressure to be, uncertainty in hearing the auscultatory gap for systolic pressure and theKorotkoff phase IV versus phase V for diastolic pressure, visual acuity in reading themeniscus,terminaldigitpreferencewhenroundingoff ;
Problems with associated pieces of equipment including wrong cuff size, leaks in thetubing ;
Patients’ clinical conditions that result in inter‐observer variability including atrialfibrillation,pre‐eclampsia ;or
Whitecoathypertension thetendencyforapatient’sbloodpressuretoincreaseinaclinicalsettingcomparedtomeasurementsmadeathome .
Laboratoryaccuracytestingisusedtochecktheaccuracyofthepressureindicatingdevice,whetherit is a mercury column, aneroid gauge, or digital display. In the lab, the aneroid gauge or digitaldisplay can bemeasured against and calibrated to a referencemanometer, such as an electronicmanometer with a high accuracy of 0.1 mmHg compared to a well‐maintained mercurysphygmomanometerwithratedaccuraciesofonly 3mmHg .Butaftertheaccuracyofthepressureindicating device has been tested and adjusted, the accuracy of blood pressuremeasurements inclinicalandgeneralpracticewillstilldependontechnique,observerbias,patients’conditions,andtheothersourcesoferrordescribedabove.This section presents procedures for laboratory testing of auscultative sphygmomanometersincluding aneroid mechanical dial and face gauges, shock‐resistant gearless gauges, digitalauscultative sphygmomanometers, and automated or semi‐automated electronicsphygmomanometerswithanauscultativeorcalibrationcheckmode.Automated electronic sphygmomanometers using oscillometric techniques, some of which aredesignedforthearm,wristorfinger,aredifficulttotestforaccuracyina laboratory.Oscillometricsphygmomanometers measure the oscillations caused by arterial pressure as the arterial wallsexpandandcontractagainstthecuff.Thepressuretransducerinthecufforelectronicunitgenerateselectrical signals. Oscillometric sphygmomanometers use algorithms that determine pulse andmaximumamplitudes or analyze dynamicwaveforms to calculate systolic and diastolic pressures.Some electronic sphygmomanometers also employ an infrasoundmethod to detect low frequencyand sub‐audibleKorotfoffvibrations.Othershavea soundsensorand integrateadigitalKorotkoffsoundanalysisintheiralgorithms.Forthesetypesofsphygmomanometers,aclinicalaccuracytestisappropriate.However,clinicalaccuracyvalidationprotocolsare involvedandtime‐consuming seeAnnexB butscreening‐typetestsmaybepossibleasdescribedattheendofthissection.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
17
PROCEDURESFORLABORATORYACCURACYTESTINGANDCALIBRATINGANEROID MECHANICALGAUGE SPHYGMOMANOMETERSFigureA3belowshowscommonaneroidsphygmomanometers:
FigureA3.PartsofCommonAneroidSphygmomanometers
Theproceduresinthissectionareadaptedfromexistinglaboratoryaccuracytestprotocols.7Totesttheaccuracyofananeroidpressuregauge,thefollowingdevicesareneeded:
A reference manometer preferably an electronic manometer traceable to a nationalstandard
Oneortwo“Y”orteeconnectorswithtubingandLuerfittings Aninflationbulbwithvalveoranadjustablemanualsyringepump
Some test set‐ups recommendusing the cuff placed around a cylinder or adding a 500 cc volumevessel e.g.,metalcontainer toallowthetesterto increasepressuregraduallyandavoidsuddenlyexceedingthemaximumgaugepressure.Sometestset‐upssuggestusingamercurysphygmomanometerasthereferencemanometerbutasexplainedabove,mercurysphygmomanometersmay themselvesbe inaccurate. Awell‐maintainedmercury sphygmomanometer has a rated accuracy of 3 mmHg, whereas typical referenceelectronicmanometershaveaccuraciesintheorderof 0.1mmHgtoaround 1mmHgtraceabletoanationalstandard.Thesereferenceelectronicmanometerswithhighaccuraciesandanoperatingrangeofatleast0to300mmHgarecommerciallyavailable.Figure A4 below gives examples of various accuracy test set‐ups for aneroid sphygmomanometergauges.
7 Section 7.1 of “Non-invasive sphygmomanometers – Part 1: Requirements and test methods for non-automated measuring type.” ANSI/AAMI/ISO 81060-1:2007; Annex A.2. of “Non-invasive automated sphygmomanometers.” International Recommendation OIML R 16-2, Edition 2002 (E); and calibration instructions in the users manuals of various sphygmomanometers.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
18
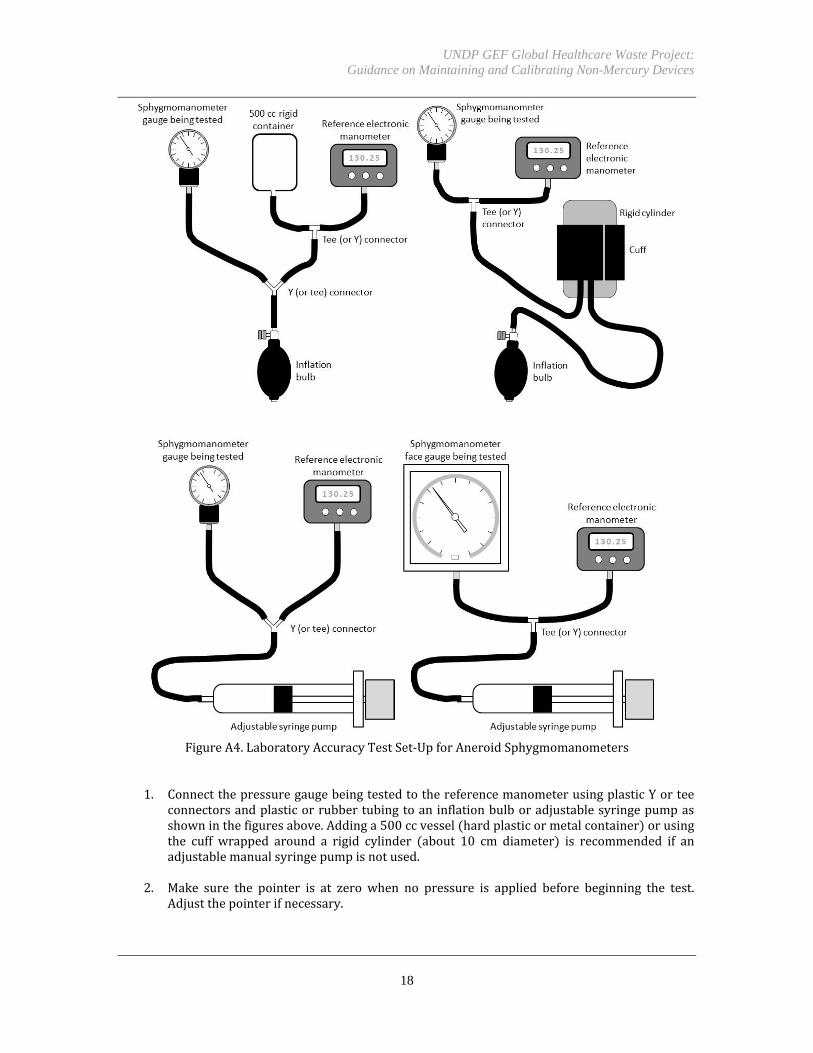
FigureA4.LaboratoryAccuracyTestSet‐UpforAneroidSphygmomanometers
1. ConnectthepressuregaugebeingtestedtothereferencemanometerusingplasticYorteeconnectorsandplasticorrubbertubingtoaninflationbulboradjustablesyringepumpasshowninthefiguresabove.Addinga500ccvessel hardplasticormetalcontainer orusingthe cuff wrapped around a rigid cylinder about 10 cm diameter is recommended if anadjustablemanualsyringepumpisnotused.
2. Make sure the pointer is at zero when no pressure is applied before beginning the test.Adjustthepointerifnecessary.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
19
3. Usingtheinflationbulborsyringepump,pressurizethegaugetoabout280mmHgandclosethevalve.Observeifthepressureisstable.Ifnot,checktheset‐upforairleaks.
4. Ifthepressureisstable,increasethepressuretoslightlyabove300mmHgandreleasethepressurenofasterthan10mmHgpersecond.
5. Stopthepressurereleasenolessthanevery50mmHg.Recordboththereadingofthegaugebeing testedand the referencemanometer reading.Forexample, readingscanbe takenat300,250,200,160,120,100,80,60,40,and0mmHg.Ataminimum,takereadingsat300,250, 200, 150, 100, 60, and 0mmHg. Check tomake sure the pointer returns to the zeromark.
6. Comparethegaugereadingswiththecorrectvalueindicatedbythereferencemanometer.Ifthe gauge is accurate towithin 3mmHg, the aneroid sphygmomanometer iswithin therequiredaccuracyandacceptableforclinicaluse.
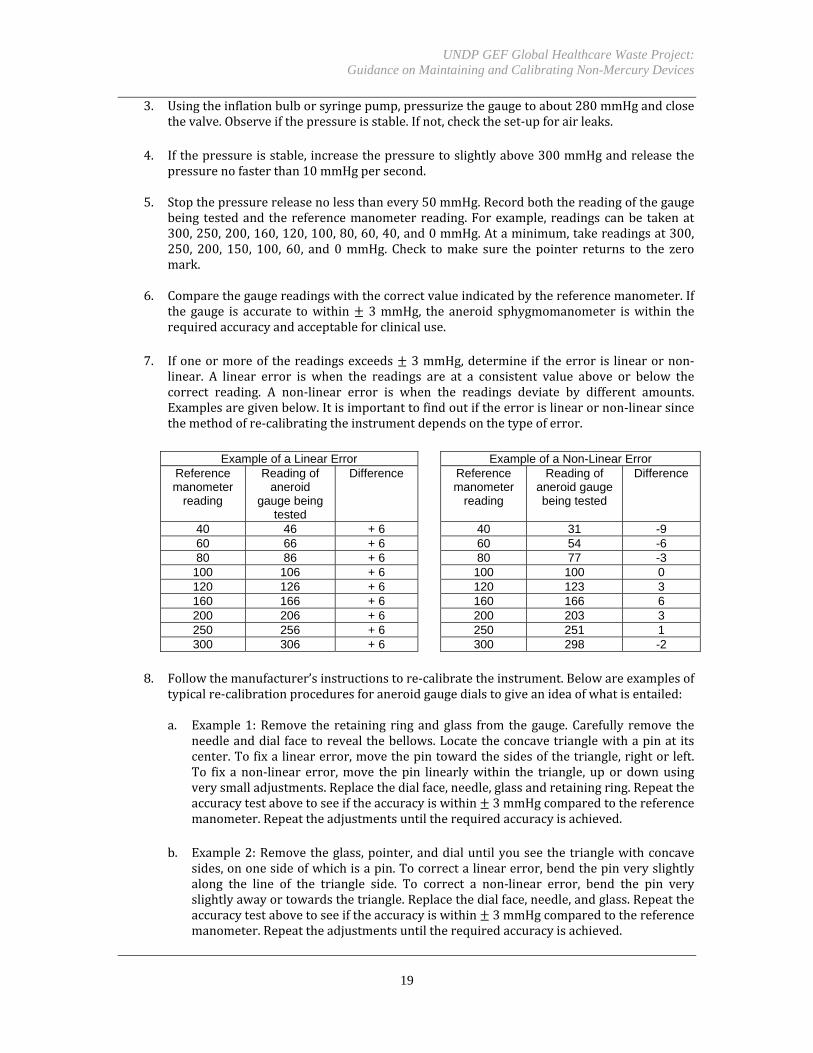
7. Ifoneormoreof thereadingsexceeds 3mmHg,determine if theerror is linearornon‐linear. A linear error is when the readings are at a consistent value above or below thecorrect reading. A non‐linear error is when the readings deviate by different amounts.Examplesaregivenbelow.Itisimportanttofindoutiftheerrorislinearornon‐linearsincethemethodofre‐calibratingtheinstrumentdependsonthetypeoferror.
Example of a Linear Error Example of a Non-Linear Error Reference manometer
reading
Reading of aneroid
gauge being tested
Difference Reference manometer
reading
Reading of aneroid gauge being tested
Difference
40 46 + 6 40 31 -9 60 66 + 6 60 54 -6 80 86 + 6 80 77 -3
100 106 + 6 100 100 0 120 126 + 6 120 123 3 160 166 + 6 160 166 6 200 206 + 6 200 203 3 250 256 + 6 250 251 1 300 306 + 6 300 298 -2
8. Followthemanufacturer’sinstructionstore‐calibratetheinstrument.Belowareexamplesof
typicalre‐calibrationproceduresforaneroidgaugedialstogiveanideaofwhatisentailed:
a. Example1:Remove the retaining ringandglass from thegauge. Carefully remove theneedleanddial facetorevealthebellows.Locatetheconcavetrianglewithapinat itscenter.Tofixalinearerror,movethepintowardthesidesofthetriangle,rightorleft.To fix a non‐linear error,move thepin linearlywithin the triangle, up or downusingverysmalladjustments.Replacethedialface,needle,glassandretainingring.Repeattheaccuracytestabovetoseeiftheaccuracyiswithin 3mmHgcomparedtothereferencemanometer.Repeattheadjustmentsuntiltherequiredaccuracyisachieved.
b. Example2:Removetheglass,pointer,anddialuntilyouseethetrianglewithconcavesides,ononesideofwhichisapin.Tocorrectalinearerror,bendthepinveryslightlyalong the line of the triangle side. To correct a non‐linear error, bend the pin veryslightlyawayortowardsthetriangle.Replacethedialface,needle,andglass.Repeattheaccuracytestabovetoseeiftheaccuracyiswithin 3mmHgcomparedtothereferencemanometer.Repeattheadjustmentsuntiltherequiredaccuracyisachieved.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
20
c. Example3:Unscrewthebezelandremovethecrystal,pointer,anddial.Placeatestdial
andtestpointeronthepinionandconnectthegaugetothetestset‐up.Apply320mmHgpressuretothegaugeandthenreleasepressureto300mmHg.Placethemanufacturersuppliedcalibrationtoolintotheradiusplateslot.Ifthereadingislessthan300mmHg,rotatethetoolcounter‐clockwiseuntil thegaugereaches300. If thereading isgreaterthan 300 mmHg, rotate the tool clockwise until the gauge reaches 300. Release thepressureandtextforthezeropoint.Rotatethedial if thepointer isoffthezeromark.Repeat the test at 300mmHg until the span is set. Replace the crystal and bezel andrepeat the calibration test at different pressure intervals to ensure that the requiredaccuracyisachieved.
PROCEDURES FOR LABORATORY ACCURACY TESTING AND CALIBRATING ELECTRONIC DIGITAL,AUTOMATED OR SEMI‐AUTOMATED SPHYGMOMANOMETERS WITH AUSCULTATIVE ORCALIBRATIONCHECKMODESSomeelectronicsphygmomanometerscannotbetestedorcalibratedbytheuserbuthavetobesenttothemanufactureroranapprovedservicecenter.Theproceduresbelowareforelectronicsphygmomanometersthathaveacalibrationcheckortestmode where the pressure can be set manually or provided by an external source. This test cancomparethereadingsfromthedeviceagainstareferencemanometer.Totesttheaccuracyofanelectronicmonitor,thefollowingdevicesareneeded:
A reference manometer preferably an electronic manometer traceable to a nationalstandard
Oneortwo“Y”orteeconnectorswithtubingandLuerfittings Aninflationbulbwithvalveoranadjustablemanualsyringepump,unlessthepressurecan
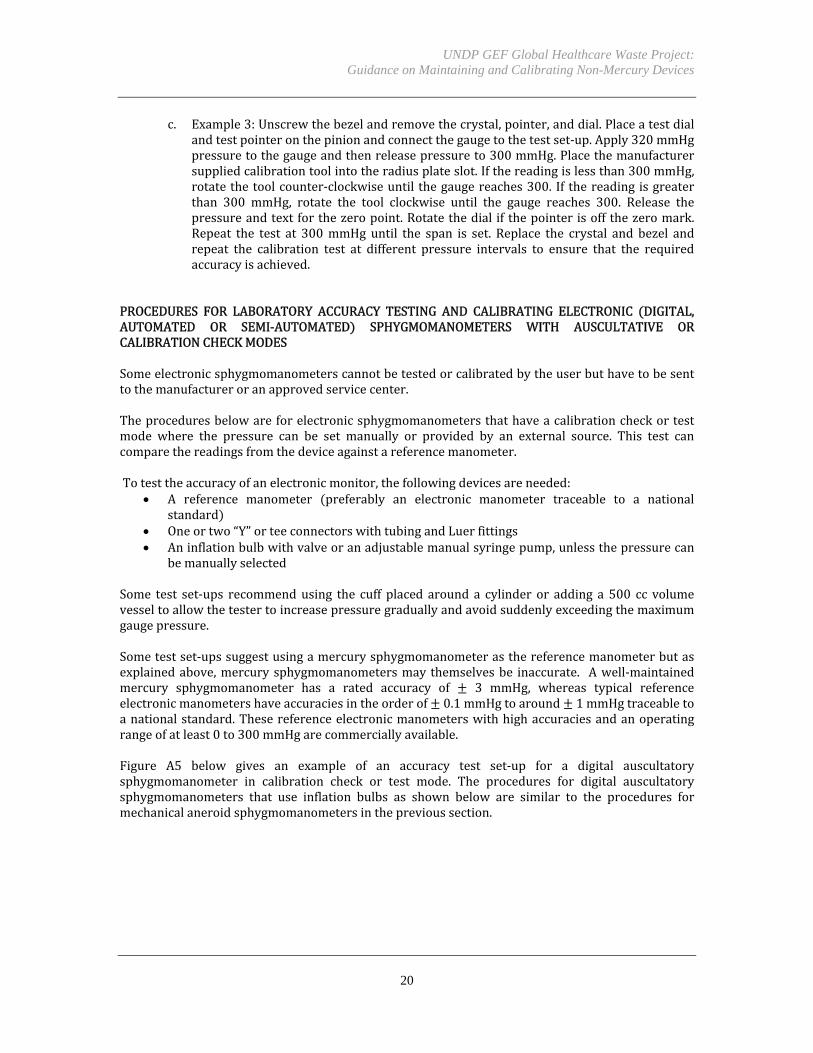
bemanuallyselectedSome test set‐ups recommendusing the cuff placed around a cylinder or adding a 500 cc volumevesseltoallowthetestertoincreasepressuregraduallyandavoidsuddenlyexceedingthemaximumgaugepressure.Sometestset‐upssuggestusingamercurysphygmomanometerasthereferencemanometerbutasexplainedabove,mercurysphygmomanometersmay themselvesbe inaccurate. Awell‐maintainedmercury sphygmomanometer has a rated accuracy of 3 mmHg, whereas typical referenceelectronicmanometershaveaccuraciesintheorderof 0.1mmHgtoaround 1mmHgtraceabletoanationalstandard.Thesereferenceelectronicmanometerswithhighaccuraciesandanoperatingrangeofatleast0to300mmHgarecommerciallyavailable.Figure A5 below gives an example of an accuracy test set‐up for a digital auscultatorysphygmomanometer in calibration check or test mode. The procedures for digital auscultatorysphygmomanometers that use inflation bulbs as shown below are similar to the procedures formechanicalaneroidsphygmomanometersintheprevioussection.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
21
FigureA5.LaboratoryAccuracyTestSet‐UpforDigitalSphygmomanometers
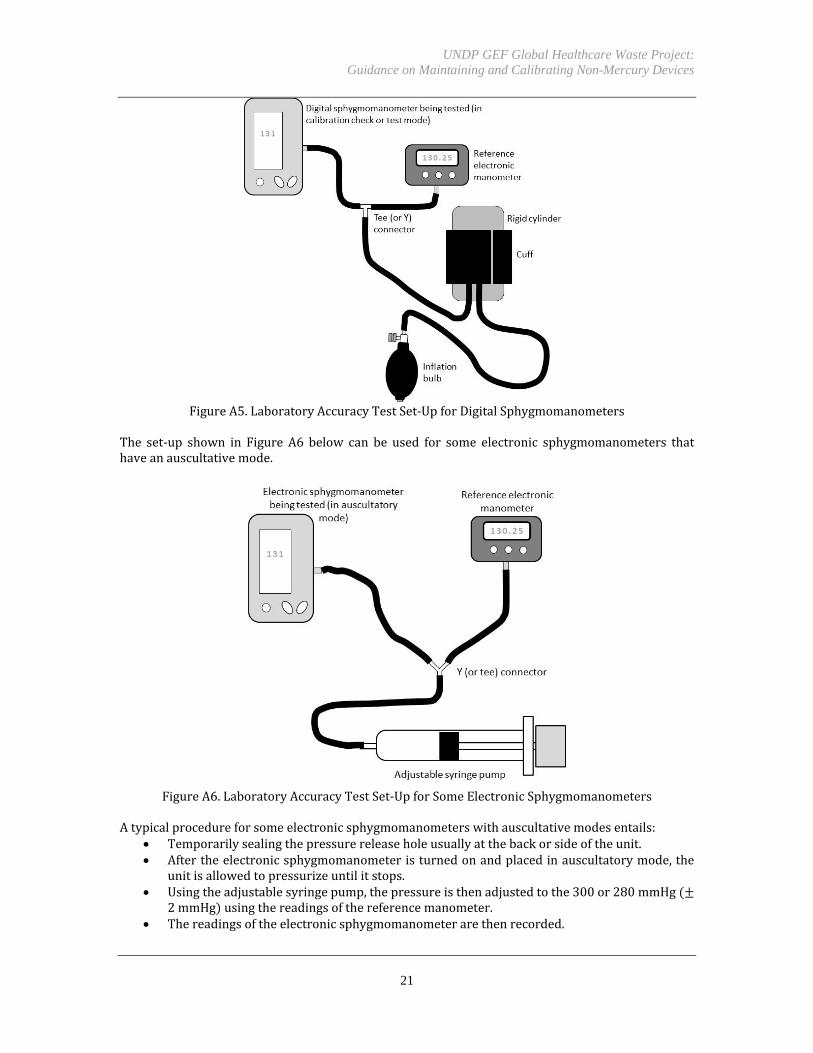
The set‐up shown in Figure A6 below can be used for some electronic sphygmomanometers thathaveanauscultativemode.
FigureA6.LaboratoryAccuracyTestSet‐UpforSomeElectronicSphygmomanometers
Atypicalprocedureforsomeelectronicsphygmomanometerswithauscultativemodesentails:
Temporarilysealingthepressurereleaseholeusuallyatthebackorsideoftheunit. Aftertheelectronicsphygmomanometeristurnedonandplacedinauscultatorymode,the
unitisallowedtopressurizeuntilitstops. Usingtheadjustablesyringepump,thepressureisthenadjustedtothe300or280mmHg
2mmHg usingthereadingsofthereferencemanometer. Thereadingsoftheelectronicsphygmomanometerarethenrecorded.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
22
The procedure is repeated every 20mmHg decrements down to 20mmHg following thereadingsofthereferencemanometer.
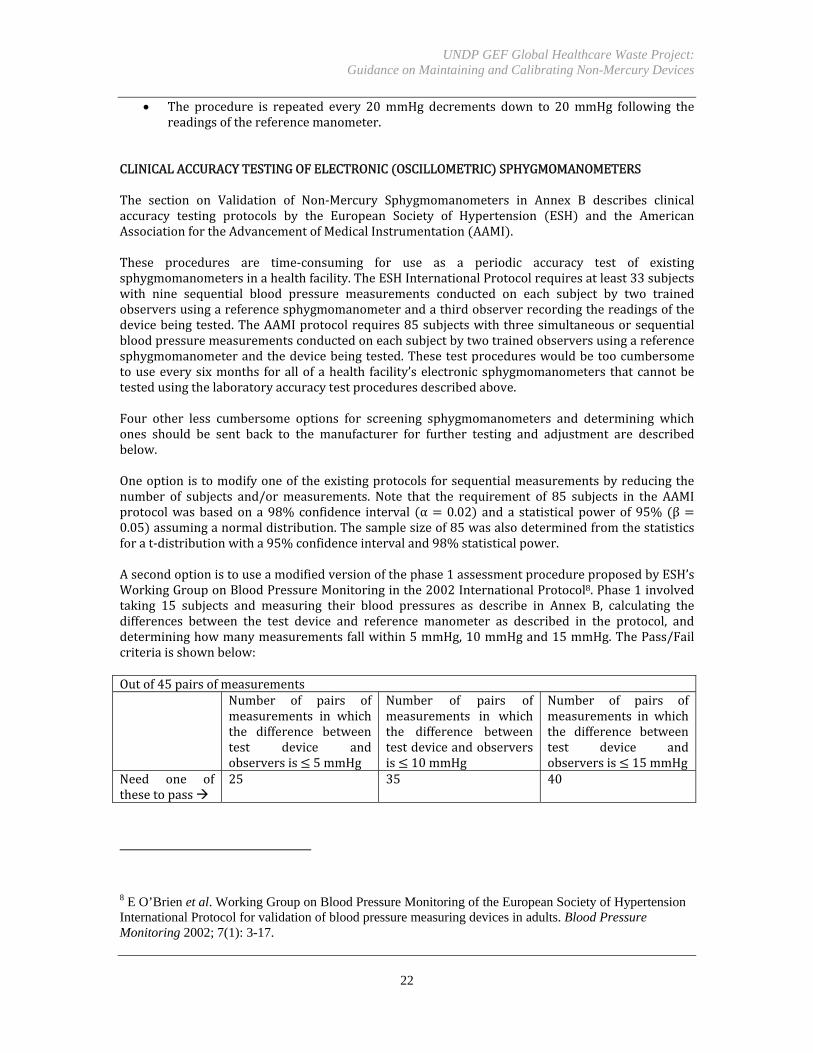
CLINICALACCURACYTESTINGOFELECTRONIC OSCILLOMETRIC SPHYGMOMANOMETERSThe section on Validation of Non‐Mercury Sphygmomanometers in Annex B describes clinicalaccuracy testing protocols by the European Society of Hypertension ESH and the AmericanAssociationfortheAdvancementofMedicalInstrumentation AAMI .These procedures are time‐consuming for use as a periodic accuracy test of existingsphygmomanometersinahealthfacility.TheESHInternationalProtocolrequiresatleast33subjectswith nine sequential blood pressure measurements conducted on each subject by two trainedobserversusingareferencesphygmomanometerandathirdobserverrecordingthereadingsofthedevicebeingtested.TheAAMIprotocolrequires85subjectswiththreesimultaneousorsequentialbloodpressuremeasurementsconductedoneachsubjectbytwotrainedobserversusingareferencesphygmomanometerandthedevicebeingtested.Thesetestprocedureswouldbetoocumbersometouseeverysixmonths forallofahealth facility’selectronicsphygmomanometers thatcannotbetestedusingthelaboratoryaccuracytestproceduresdescribedabove.Four other less cumbersome options for screening sphygmomanometers and determining whichones should be sent back to the manufacturer for further testing and adjustment are describedbelow.Oneoptionistomodifyoneoftheexistingprotocolsforsequentialmeasurementsbyreducingthenumber of subjects and/ormeasurements. Note that the requirement of 85 subjects in the AAMIprotocolwasbasedona98%confidence interval α 0.02 and a statistical powerof95% β 0.05 assuminganormaldistribution.Thesamplesizeof85wasalsodeterminedfromthestatisticsforat‐distributionwitha95%confidenceintervaland98%statisticalpower.Asecondoptionistouseamodifiedversionofthephase1assessmentprocedureproposedbyESH’sWorkingGrouponBloodPressureMonitoringinthe2002InternationalProtocol8.Phase1involvedtaking 15 subjects and measuring their blood pressures as describe in Annex B, calculating thedifferences between the test device and reference manometer as described in the protocol, anddetermininghowmanymeasurementsfallwithin5mmHg,10mmHgand15mmHg.ThePass/Failcriteriaisshownbelow:Outof45pairsofmeasurements Number of pairs of
measurements in whichthe difference betweentest device andobserversis 5mmHg
Number of pairs ofmeasurements in whichthe difference betweentestdeviceandobserversis 10mmHg
Number of pairs ofmeasurements in whichthe difference betweentest device andobserversis 15mmHg
Need one ofthesetopass
25 35 40
8 E O’Brien et al. Working Group on Blood Pressure Monitoring of the European Society of Hypertension International Protocol for validation of blood pressure measuring devices in adults. Blood Pressure Monitoring 2002; 7(1): 3-17.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
23
AthirdoptionistouseamodifiedversionofamethodproposedbytheJapanISOWorkingGroupfora sphygmomanometer standard9. They suggested four simultaneous measurements between thereferencemanometerandtestdeviceusingbotharms,switchingsideseachtime,andchangingtheorder of measurement between reference and test devices with every subject. Compensation forlateralbloodpressuredifferencesbetweenthetwoarmsisdonebyaveragingthefourreadings thetwo reference and two test readings in each arm . They reported that their four simultaneousmeasurementswithbotharmsandalternatingdeviceswitheacharmprovidedbetterreproducibilityand inter‐participant consistency in the error calculation than using the standard two‐armsimultaneousandsame‐armsequentialmethods.A fourth option is based on a rapid accuracy estimation method for automatic blood pressuremeasuring devices proposed by Naschitz and co‐workers10. In their 1999 study, they selected 15subjectsindifferentbloodpressurerangecategories.Bloodpressurewasmeasuredsimultaneouslyontheleftarmwithacuffconnectedtoboththetestdeviceandreferencesphygmomanometer.Thereadings from the test device and reference device were taken simultaneously by two trainedobservers who could not see each other’s data. Numerous measurements were taken with eachsubjectatrestandinstandardizedposturalstresswhilethesubjectwassecuredtoatilttablewithadhesivegirdles.Measurementsweremadestartinginthesupine horizontal position,followedbytiltingtoa70°head‐uppositionwiththearmsupportedatheart level, followedbyanothersupinephase,etc.Theyusedthecriteriathatthedevicewasacceptableifatleast65%ofreadingsfellwithin5mmHg,85%within10mmHg,and95%within15mmHgofthereferencesphygmomanometer.ThemethodbyNaschitzandcolleaguesisasame‐armsimultaneoustechniquebuttakingmeasurementsusing a tilt table at different postural challenges. This allowed them to take many pairedmeasurementswithonly15subjects.
9 Shirasaki, O, Asou, Y and Takahashi, Y. New clinical validation method for automated sphygmomanometer: a proposal by Japan ISO-WG for sphygmomanometer standard. Blood Pressure Monitoring 2002; 12(6): 381-383. 10 Naschitz, JE et al. Rapid estimation of the accuracy of automatic blood pressure measuring devices (READ). Journal of Human Hypertension 1999; 13(7): 443-447; Naschitz, JE et al. In-field validation of automatic blood pressure measuring devices. Journal of Human Hypertension 2000; 14(1): 37-42.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
24
ANNEXC
IMPORTANCE OF VALIDATION IN THE PROCUREMENT PROCESS Validationistheprocessoftestingadevicefollowinganinternationallyornationallyapprovedtestprotocol and verifying that the device meets minimum standard criteria. Validation examinesdurability,electricalsafety,readability,long‐termstability,etc..Italsoexaminesaccuracyinaclinicalsetting.Clinicalaccuracytakesintoaccounttheinherentvariabilityofwhatisbeingmeasured e.g.,bloodpressurechanging frommoment tomoment , the techniqueusedby theclinician,andotherfactors in a clinical setting and measure clinical bias and repeatability. Unfortunately, the term“validation”hassometimesbeenusedtomeanthatadevicehasbeensubjectedtoavalidationtestprotocolwithouthavingnecessarilypassedthetest.11Inthisguidance,validationreferstobothtestingthedeviceandconfirmingthatitmeetsminimumrequirementsunderinternationalstandards.Reliable and up‐to‐date validation data provide purchasing staff and individual purchasers withevidence‐based informationondeviceaccuracyandotherperformancecriteria.The importanceofvalidationwas highlighted in a study by Akpolat et al.12who found a direct relationship betweenaccuracy and validation. The researchers requested individuals to bring their homesphygmomanometers to a university hospital for testing. Of 74 automated sphygmomanometerstested, theresearchers foundthat68%ofvalidatedsphygmomanometerswereaccuratecomparedtoonly15%ofnon‐validateddevices.Validateddevicesmeantthatthesamemakeandmodelhadbeen independently evaluated for accuracy following the International Protocol of the EuropeanSociety ofHypertension, the Association for the Advancement ofMedical Instrumentation, and/ortheBritishHypertensionSociety,andthemakeandmodelwerereportedbythedabl©EducationalTrustashavingpassedvalidationtesting.
VALIDATION OF NON-MERCURY CLINICAL THERMOMETERS Validation of digital clinical thermometers can be done in accordance with EN 12470‐3:2000 A1:2009,ASTME1112‐00 2006 , and ISO80601‐2‐56:2009.This section gives a generaloverviewofthevalidationprocessforthermometersundereachofthethreestandards.A reference thermometer is needed to test accuracy of a test thermometer towithin 0.1⁰C. Theuncertainty in the temperature reading of the reference thermometermust be less that 0.02⁰C.Importantly,thecalibrationofthereferencetemperaturemustbetraceabletoanationalstandard13.
11 “Turning up the pressure: Phasing out mercury sphygmomanometers for professional use,” European Environmental Bureau, Brussels, Belgium, June 2009. 12 Akpolat, T, Dilek, M, Aydogdu, T, Adibelli, Z, Erdem, D and Erdem, E. Home sphygmomanometers: validation versus accuracy. Blood Pressure Monitoring 2009; 14(1): 26-31. 13 Examples of national standards bodies are: Instituto Nacional de Tecnología Industrial (Argentina), National Institute of Metrology (China), National Physical Laboratory of India, National Institute for Standards (Egypt), Laboratoire National de Métrologie et d'Essais (France), Physikalisch-Technische Bundesanstalt (Germany), National Metrology Institute of Japan, Latvian Metrology Bureau, National Metrology Laboratory of the Philippines, Federal Institute of Metrology (Switzerland), National Physical Laboratory (United Kingdom), National Institute of Standards and Technology (United States), Vietnam Metrology Institute - Directorate for Standards and Quality, and the World Meteorological Organization.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
25
Referencethermometersaregenerallyplatinumresistancethermometers PRTs .Standardplatinumresistancethermometershaveaccuraciesashighas0.0001⁰Cbutareexpensiveandsusceptible toshock. Industrialplatinumresistancethermometershaveaccuracies in theorderof0.02⁰Candaremoreruggedandmuchlessexpensive.VALIDATIONTESTSUNDEREN12470‐3Under EN 12470‐3, tests can be done on each individual lot or on a statistically representativesampling.Thetestshouldbecarriedoutinaroomwithanambienttemperatureof23⁰C 5⁰Cwitharelativehumidityof50% 20%.Thetestapparatusiscomprisedofawellregulatedandwellstirredwaterbathcontainingatleast5litersofwaterandthereferencethermometer.Thetemperatureofthewaterbatchshouldbecontrolledtohaveatemperaturestabilityofbetterthan 0.02⁰Candthetemperature difference within the test space of the bath should not exceed 0.01⁰C. The ENstandardrequiresthatthethermometerprovidesavisualorauditorywarningwhenthemeasuredtemperatureisoutsidethemeasuringrangespecifiedbythemanufacturer,typically35.5to40.2⁰C.Thestandardalsorequiresamaximumpermissibleerrorof0.1⁰Cwithinthemeasuringrange.Thetest thermometer is immersed in thewater bath to the depth specified by themanufacturer.At aconstant temperature 0.3⁰C below the minimum and 0.3⁰C above the maximum values of themeasuring range, the thermometer should give a visual or auditory warning. At a constanttemperature 0.3⁰C above theminimumand 0.3⁰C below themaximum, there should be no alarm.Withinthemeasuringrange,measurementsshouldbeobtainedateveryfulldegreeCelsiuswhenthethermometerhas reached thermalequilibriumoras specifiedby themanufacturer.Thedifferencebetweenthereadingsofthetestthermometerandthereferencethermometershouldnotexceedthemaximumpermissibleerror.Thistestmustbeperformedonatleast10thermometerstodetermineif thereareany inhomogeneities that could result inexceeding themaximumpermissibleerror insmallsub‐ranges.Iftherearenoinhomogeneities,thesubsequenttestscouldbedoneonjustthreeequallyspacedpointswithinthemeasuringrange.In addition to accuracy andwarningswhenoutside themeasuring range, the full set of validationtests under EN 12470‐3 include: visual inspection of the digital increment and size of numericalvalues,timeresponse,effectofenergydissipationintheprobe,longtermstability,ambientoperatingrange, effect of storage, effect of thermal shock, effect of humidity, electromagnetic compatibility,effectofmechanicalshock,waterresistance,warningwhensupplyvoltageisoutsidespecifiedlimits,functionalsafetest,electricalsafetyaccordingtoEN60601‐1,andinspectionofinformationsuppliedbythemanufacturerandmarkings.14VALIDATIONTESTSUNDERASTME1112Under ASTM E1112, the well stirredwater bathmust have a volume greater than 1 liter and itstemperaturemustbeaccuratelycalibratedwithin0.03⁰C.Testsareconductedwithinthemeasuringrange to comparemeasurementsof the test thermometer against the reference thermometer.Thefullsetofvalidationtestsalso includestestsofaccuracyunderdifferentenvironmentalconditions,effects of storage conditions, inspection of labeling, inspection of the graduated intervals in thedisplay,inspectionofresolutionandreadability,batteryindication,electricalsafetyaccordingtoUL544, cleaning tests, and inspection of instructions provided by the manufacturer includingrecommendedrecalibrationinstructions.15
14 “Clinical thermometers - Part 3: Performance of compact electrical thermometers (non-predictive and predictive) with maximum device,” European Standard EN 12470-3:2000+A1, June 2009. 15 “Standard Specification for Electronic Thermometer for Intermittent Determination of Patient Temperature,” ASTM E1112 – 00, Reapproved 2006.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
26
VALIDATIONTESTSUNDERISO80601‐2‐56ISO80601‐2‐56,issuedbytheInternationalOrganizationforStandardization ISO ,appliestodigitalclinical thermometers. Laboratory accuracy tests require a water bath with temperature stabilitybetter than 0.02⁰C anda temperature gradient not exceeding 0.01⁰C.The temperature of thebath should be measured by a reference thermometer with a total uncertainty not greater than0.07⁰C.Testsareconductedinaclimatechamberandthetestthermometerisallowedtostabilizefora minimum of 30 minutes at the mid‐range of the operating environmental conditions i.e., theambient temperature and humidity . Measurements of the test thermometer and the referencethermometerarerecorded,andthetestsarerepeatedat1⁰Coftheupperlimitand1⁰Cofthelowerlimit of the rated output temperature range. The tests are again repeated at four points of theoperating environmental conditions, combining the upper and lower limits of temperature andhumidity. The standard also describes a test for time response; clinical accuracy validation tests;inspectionsandfunctionaltestingrelatedtomarkings,unitsofmeasure,instructionsforuse,alarmconditionsornooutputifthetemperatureorambientconditionisoutsidetherangeorincaseofalowvoltageof thepowersource;andbasicsafetyofmedicalelectricalequipmentaccordingtoIEC60601‐1.16Theultimategoaloftemperaturemeasurementinmedicineistoobtainanaccuratedeterminationofcore body temperature of a patient. Laboratory accuracy—which reflects an instrument’s design,internal randomfluctuations inelectrical signals,electricaldrift,manufacturing tolerances,etc.—istestedbycomparingmeasurementsofatemperature‐controlledliquidorblackbodyastakenbythetestthermometerversusareferencethermometer.Clinicalaccuracyisbasedonmeasurementsofabodysiteofahumansubject.EN12470‐5andASTME1965alsodescribetestingforclinicalaccuracyfortympanicIRthermometers.EN12470‐5requiresamaximumpermissibleclinicalrepeatabilityof 0.3°C for every patient age group newborn, children, and adults for which the infrared ear
thermometerisintendedforuse.ASTME1965requiresthattheclinicalaccuracymustbediscloseduponrequestforeachdevicemodel,eachadjustabledisplaymode,andforeveryagegroupintendedforuse.Clinicalaccuracytestsmeasurebothclinicalbiaswithstateduncertainty,andclinical repeatability.Thesetestsaredoneonthreegroupsofsubjects: infantsfromnewborntooneyear,childrenfromgreaterthanoneyeartofiveyears,andadultsgreaterthanfiveyearsold.ASTME1965recommendsat least 30 test subjects for each group, while EN 12470‐5 requires at least 50 subjects. Bothstandardsrequirebothfebrileandnon‐febrilesubjects,withEN12470‐5requiringat least30%ofsubjects in each group to be febrile temperatureover38°C . The clinical trial is performedat anambient temperature of 21 3°C and a relative humidity of 50% 20%under EN12470‐5. Fortympanic IR thermometer tests, ASTM E1965 recommends excluding subjects with external earinflammation, auditory canal obstructions, use of medication that affect body temperature withinthreehoursofthetest,orimmunizationwithinsevendaysofthetest.UnderEN12470‐5,threeconsecutivereadingsaretakenwiththetestIRthermometeronthesamesubject at the same body site and by the same operator. The time between readings should bebetween1and3minutes.TheclinicalrepeatabilitySRforeachagegroupiscalculatedby
16 “Particular requirements for basic safety and essential performance of clinical thermometers for body temperature measurement,” International Standard ISO 80601-2-56:2009(E), 1 October 2009.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
27
1
1.65
Equation1 where Ri is the span between the maximum and minimum readings of the three consecutivemeasurementsofsubjecti,andnisthetotalnumberofsubjectsintheagegroup.Under ASTM E1965, clinical repeatability SR as the pooled standard deviation of all temperaturedeviationsforallnsubjectsiscalculatedby
∑
6
Equations2‐5 whereT1i,T21,andT31arethefirst,second,andthirdtemperaturereadingsbythesameoperatorofthesamebodysiteofthesubjecti.Inadditiontorepeatability,bothstandardsalsorequireameasurementofclinicalbiaswhichreflectsthe difference between temperature measurements by the IR thermometer being tested and thetemperatures of the subjects as measured by a reference thermometer at a reference body site.Laboratoryaccuracyof thereferencethermometershouldbevalidatedbeforehand.ThetestunderEN12470‐5requiresthreeconsecutivereadingsofthetemperaturewiththetestIRthermometeratthe same body site of the same subject by the same operator, followed by one reading with thereference thermometer by the same operator, with the time between readings not less than oneminute.EN12470‐5givesthefollowingequationsforclinicalbiasΔTbandΔTbitheclinicalbiasforsubjecti,aswellasthestandarddeviationSboftheclinicalbias:
∆ 1 ∆
∆ 13
∑ ∆ ∆
1
Equations6‐8 For ASTM E1965, clinical bias for each adjusted mode of operation of the IR thermometer iscalculated as the root‐sum‐of‐squares of the standard deviation of the data comparing themeasurementfromthetestIRthermometerinagivenadjustedmodeversusthemeasurementusingareferencethermometerataselectedbodyreferencesite.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
28
Becauseof the importanceofvalidation,manyvendorsprovidecertificatesofcomplianceorotherdocumentationtoindicatethattheirthermometershavebeenvalidatedaccordingtooneormoreofthese international standards. An example of a report that provides data on validation ofthermometers is the thermometer review by the Device Evaluation Service of the Medicines andHealthcareproductsRegulatoryAgencyoftheUKDepartmentofHealth.17
17 Crawford, D, Greene, N and Wentworth S. “Thermometer review: UK market survey 2005,” MHRA 04144, Medicines and Healthcare products Regulatory Agency, London, UK. January 2005.

UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
29
VALIDATION OF NON-MERCURY SPHYGMOMANOMETERS There are several validation standards and protocols for evaluating blood pressure devices. TheyincludetheInternationalProtocolbytheEuropeanSocietyofHypertension ESH 18;ANSI/AAMI/ISO81060‐1 and ‐219 joint standard of the American National Standards Institute ANSI , AmericanAssociationfortheAdvancementofMedicalInstrumentation AAMI andInternationalOrganizationfor Standardization ISO ; ANSI/AAMI/IEC 80601‐2‐3020 joint standard of ANSI, AAMI and theInternational Electrotechnical Commission IEC ; European Standard EN 106021 also adopted asBritishStandardBS1060andGermanStandardDIN58130 ;theBritishHypertensionSociety BHS protocol of 1990 revised in 1993 22; and International Recommendation OIML R 16‐223 of theInternational Organization of Legal Metrology OIML . As of early 2013, IEEE P1708 and P1721standards24werealsobeingdeveloped.In the overview below, the topics covered by the ANSI/AAMI/ISO/IEC standards and the OIMLrecommendations are presented as examples. Clinical accuracy protocols are also compared anddiscussed.TheANSI/AAMI/ISO81060‐1:2007standardcoversarangeofrequirementsincluding:theunitsofmeasurement, legibility and durability of markings, markings of non‐automatedsphygmomanometers, usability of reading,markingof the cuff, electrical safety,mechanical safety,mechanical strength, the measuring range, error limits of the pressure indicator, requirementsrelatedtoairleakage,pressurereductionrate,rateofrapidexhaust,cuffsizes,integrityofcuffandbladder, tubing connectors, tamper proofing,marking and zero for aneroid sphygmomanometers,hysteresis error error of the measurement value when approaching it with increasing pressureversus decreasing pressure , materials of construction, ability to be cleaned and disinfected or 18 O’Brien, E et al. European Society of Hypertension International Protocol revision 2010 for the validation of blood pressure measuring devices in adults. Blood Pressure Monitoring 2010; 15(1): 23-38. 19 “Non-invasive sphygmomanometers – Part 1: Requirements and test methods for non-automated measuring type.” ANSI/AAMI/ISO 81060-1:2007; “Non-invasive sphygmomanometers – Part 2: Clinical validation of automated measurement type.” ANSI/AAMI/ISO 81060-2-2009. 20 “Medical electrical equipment – Part 2-30: Particular requirements for the basic safety and essential performance of automated non-invasive sphygmomanometers.” ANSI/AAMI/IEC 80601-2-30:2009. 21 “Non-invasive sphygmomanometers. General requirements.” BS EN 1060-1:1995+A2:2009; “Non-invasive sphygmomanometers. Supplementary requirements for mechanical sphygmomanometers.” BS EN 1060-2:1995+A1:2009; “Non-invasive sphygmomanometers. Supplementary requirements for electro-mechanical blood pressure measuring systems.” BS EN 1060-3:1997+A2:2009; “Non-invasive sphygmomanometers. Test procedures to determine the overall system accuracy of automated non-invasive sphygmomanometers.” BS EN 1060-4:2004. 22 O’Brien, E et al. The British Hypertension Society protocol for the evaluation of automated and semi-automated blood pressure measuring devices with special reference to ambulatory systems. J Ambulatory Monitoring 1991; 4(3): 207-228; O’Brien, E et al. Short report: An outline of the revised British Hypertension Society protocol for the evaluation of blood pressure measuring devices. J Hypertension 1993; 11(6): 677-679; O’Brien, E et al. The British Hypertension Society protocol for the evaluation of blood pressure measuring devices. J Hypertension 1993; 11(suppl 2): S43-S62. 23 “Non-invasive automated sphygmomanometers.” International Recommendation OIML R 16-2, Edition 2002 (E). 24 “P1708 - Standard for Wearable Cuffless Blood Pressure Measuring Devices (draft)” and “P1721 - Standard for Objective Measurement of Systemic Arterial Blood Pressure (draft)” Institute of Electrical and Electronics Engineers, under development.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
30
sterilized, and the instructions for use. The ANSI/AAMI/IEC 80601‐2‐30:2009 standard covers,among others: protection against electrical and mechanical hazards, protection against radiationhazards, protection against excessive temperatures and other hazards, accuracy of controls andinstruments, protection against hazardous outputs, fault conditions, electromagnetic compatibility,maximuminflatingtime,automaticcyclingmodes,andclinicalaccuracy.For automated sphygmomanometers, the OIML recommendations include: units of measurement,maximumpermissibleerrorsofthecuffpressureindicationandoftheoverallsystem,performanceunderspecificenvironmentalconditions,requirementsforthecuffandbladder,requirementsforthedisplay,effectsofvoltagevariations,requirementsrelatedtothepneumaticsystem,electromagneticcompatibility,stabilityofcuffpressureindication,measuringrange,digitalscaleinterval,signalinputandoutputports,alarms,safety,metrologicalcontrols,testingandverification,sealing,marking,andinformationtobesuppliedbythemanufacturer.With regards to clinical accuracy, the International Protocol of the European Society forHypertensionrequirestwomercurysphygmomanometersasreferences,goodqualitystethoscopes,thetestdevice,twotrainedobserversandasupervisor,andatleast33subjectsofwhichatleast10aremale and 10 are female, all 25 years or older. In order to test the range of blood pressures,subjectsshouldbechosensuchthatthereare10to12subjectsineachofthethreesystolicandthreediastolicbloodpressureranges.Lowsystolicis 130,mediumis130‐160,andhighis 160mmHg;lowdiastolicis 80,mediumis80‐100,andhighis 100mmHg.Thenumberoftestmeasurementsmustbebetween22and44ineachpressurerange.Theoverallsystolicrangemustbefrom 100to170mmHg,andtheoveralldiastolicrangemustbefrom 50to 120mmHg.
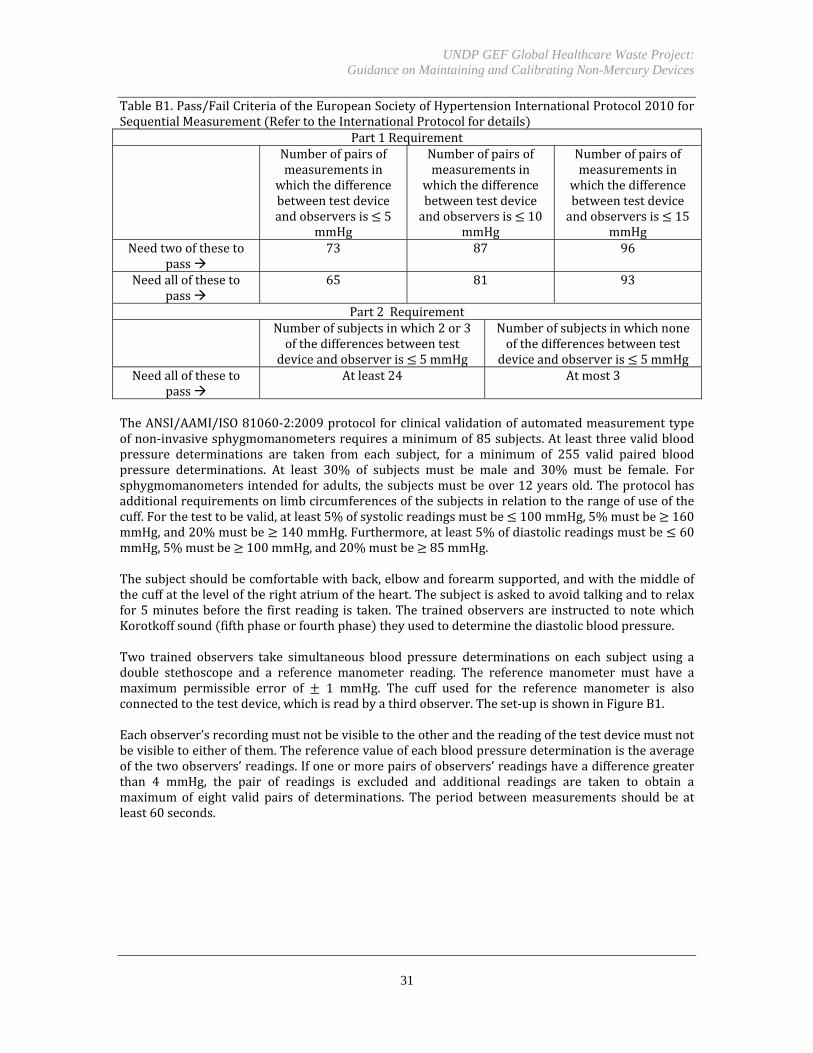
The subject is asked to relax for 10‐15 minutes and should be seated with legs uncrossed, backsupported,andtestarmsupportedatheart levelduringthetest.Allbloodpressuremeasurementsaretakensequentiallyononearm,whicheverismorecomfortableforthesubject.Measurementsaretaken sequentially, starting with measurements by the observers then alternating withmeasurementsbythetestdevice.Thefirstmeasurements observerA,observerBandtestdevice areusedtodeterminetowhichsystolicanddiastolicbloodpressurerangesthesubjectbelongs.Afterthefirstmeasurements,atotalofsevensequential,same‐armmeasurementsaretakenstartingwith theobserversusing themercurysphygmomanometer measurement1byobserverAandB ,thenthetestdevice measurement2 ,thenobserversAandBagain measurement3 ,thenthetestdevice measurement4 ,continuinguntilmeasurement7 observersAandB .Theperiodbetweenmeasurementsshouldbeatleast30secondsbutnomorethan60seconds.Measurementsshouldberecordedtothenearest2mmHg.Observersmustnotbeabletoseeeachother’smeasurementsandshouldnotbeabletoseethetestdevice’sreadingsthroughoutthestudy.Bothobserversshouldrecordtheirreadingssimultaneouslyandifthesupervisorseesthattheobservers’measurementsdifferbymorethan4mmHgfromeachother,themeasurementsshouldbetakenagain.Thedifferencebetweenthereadingofthetestdeviceandthemeanreadingofthetwoobserversarecalculated for eachmeasurement. The pairs of blood pressuremeasurement differences are thenclassified into three categories 5, 10, and 15 mmHg . The number of differences in eachcategoryisthencomparedwiththePass/FailcriteriaundertheInternationalProtocol.Similarly,thenumber of subjects with two or three of the absolute differences between observer and devicemeasurementswithin 5mmHg and the number of subjectswith none of the absolute differencesbetweenobserveranddevicemeasurementswithin5mmHgarecomparedtothePass/Failcriteria.
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
31
TableB1.Pass/FailCriteriaoftheEuropeanSocietyofHypertensionInternationalProtocol2010forSequentialMeasurement RefertotheInternationalProtocolfordetails
Part1Requirement Numberofpairsof
measurementsinwhichthedifferencebetweentestdeviceandobserversis 5
mmHg
Numberofpairsofmeasurementsin
whichthedifferencebetweentestdeviceandobserversis 10
mmHg
Numberofpairsofmeasurementsin
whichthedifferencebetweentestdeviceandobserversis 15
mmHgNeedtwooftheseto
pass73 87 96
Needallofthesetopass
65 81 93
Part2Requirement Numberofsubjectsinwhich2or3
ofthedifferencesbetweentestdeviceandobserveris 5mmHg
Numberofsubjectsinwhichnoneofthedifferencesbetweentestdeviceandobserveris 5mmHg
Needallofthesetopass
Atleast24 Atmost3
TheANSI/AAMI/ISO81060‐2:2009protocolforclinicalvalidationofautomatedmeasurementtypeofnon‐invasivesphygmomanometersrequiresaminimumof85subjects.Atleastthreevalidbloodpressure determinations are taken from each subject, for a minimum of 255 valid paired bloodpressure determinations. At least 30% of subjects must be male and 30% must be female. Forsphygmomanometersintendedforadults,thesubjectsmustbeover12yearsold.Theprotocolhasadditionalrequirementsonlimbcircumferencesofthesubjectsinrelationtotherangeofuseofthecuff.Forthetesttobevalid,atleast5%ofsystolicreadingsmustbe 100mmHg,5%mustbe 160mmHg,and20%mustbe 140mmHg.Furthermore,atleast5%ofdiastolicreadingsmustbe 60mmHg,5%mustbe 100mmHg,and20%mustbe 85mmHg.Thesubjectshouldbecomfortablewithback,elbowandforearmsupported,andwiththemiddleofthecuffattheleveloftherightatriumoftheheart.Thesubjectisaskedtoavoidtalkingandtorelaxfor5minutesbefore the first reading is taken.The trainedobserversare instructed tonotewhichKorotkoffsound fifthphaseorfourthphase theyusedtodeterminethediastolicbloodpressure.Two trained observers take simultaneous blood pressure determinations on each subject using adouble stethoscope and a reference manometer reading. The reference manometer must have amaximum permissible error of 1 mmHg. The cuff used for the reference manometer is alsoconnectedtothetestdevice,whichisreadbyathirdobserver.Theset‐upisshowninFigureB1.Eachobserver’srecordingmustnotbevisibletotheotherandthereadingofthetestdevicemustnotbevisibletoeitherofthem.Thereferencevalueofeachbloodpressuredeterminationistheaverageofthetwoobservers’readings.Ifoneormorepairsofobservers’readingshaveadifferencegreaterthan 4 mmHg, the pair of readings is excluded and additional readings are taken to obtain amaximum of eight valid pairs of determinations. The period betweenmeasurements should be atleast60seconds.
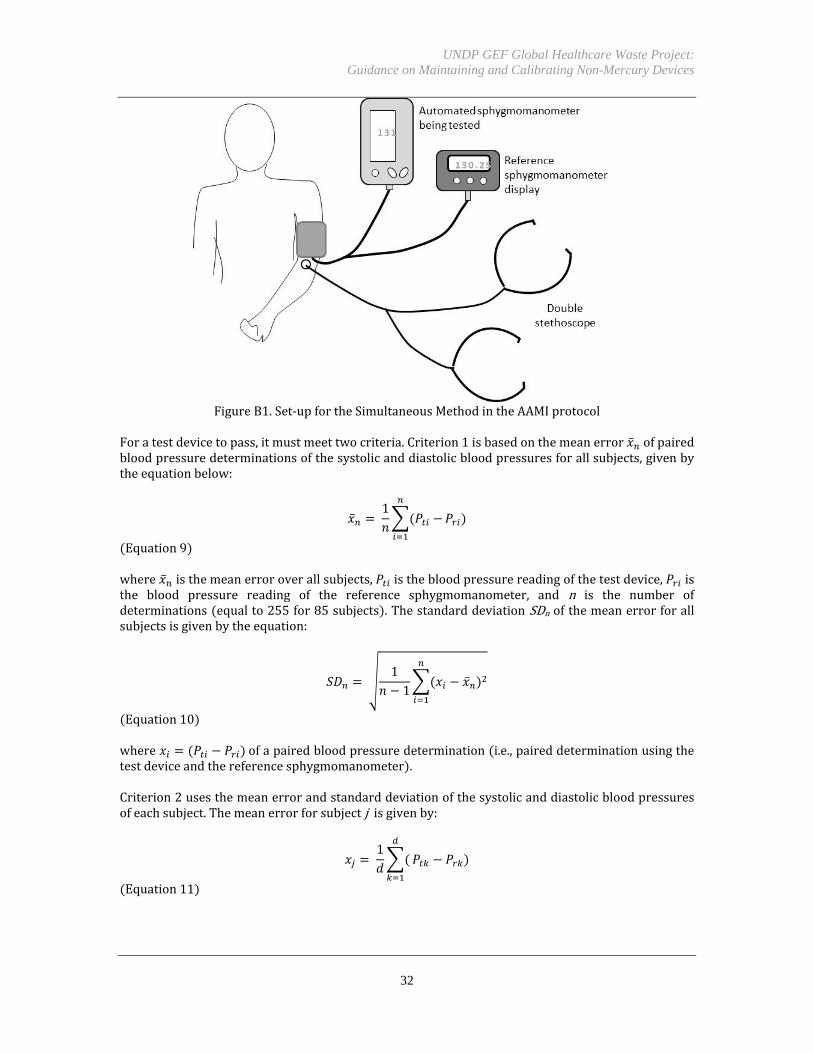
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
32
FigureB1.Set‐upfortheSimultaneousMethodintheAAMIprotocol
Foratestdevicetopass,itmustmeettwocriteria.Criterion1isbasedonthemeanerror ofpairedbloodpressuredeterminationsofthesystolicanddiastolicbloodpressuresforallsubjects,givenbytheequationbelow:
1
Equation9 where isthemeanerroroverallsubjects, isthebloodpressurereadingofthetestdevice, isthe blood pressure reading of the reference sphygmomanometer, and n is the number ofdeterminations equalto255for85subjects .ThestandarddeviationSDnofthemeanerrorforallsubjectsisgivenbytheequation:
11
Equation10 where ofapairedbloodpressuredetermination i.e.,paireddeterminationusingthetestdeviceandthereferencesphygmomanometer .Criterion2usesthemeanerrorandstandarddeviationofthesystolicanddiastolicbloodpressuresofeachsubject.Themeanerrorforsubjectjisgivenby:
1
Equation11
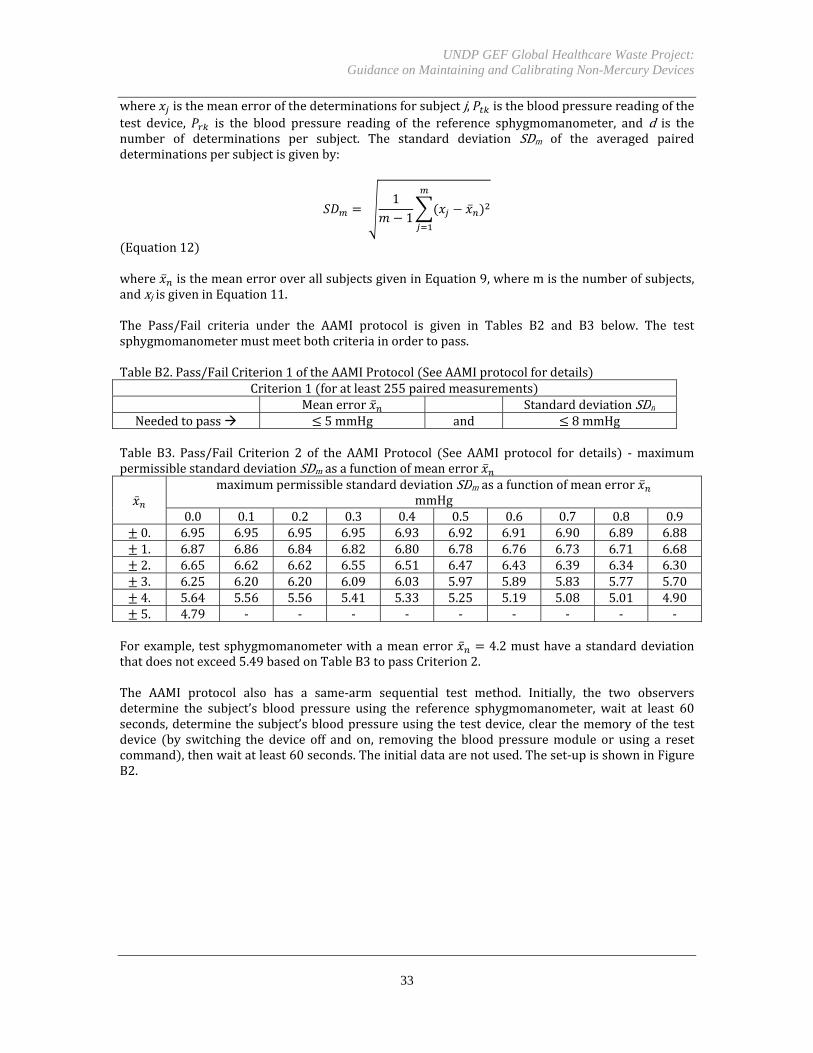
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
33
where isthemeanerrorofthedeterminationsforsubjectj, isthebloodpressurereadingofthetest device, is the blood pressure reading of the reference sphygmomanometer, and d is thenumber of determinations per subject. The standard deviation SDm of the averaged paireddeterminationspersubjectisgivenby:
11
Equation12 where isthemeanerroroverallsubjectsgiveninEquation9,wheremisthenumberofsubjects,andxjisgiveninEquation11.The Pass/Fail criteria under the AAMI protocol is given in Tables B2 and B3 below. The testsphygmomanometermustmeetbothcriteriainordertopass.TableB2.Pass/FailCriterion1oftheAAMIProtocol SeeAAMIprotocolfordetails
Criterion1 foratleast255pairedmeasurements Meanerror StandarddeviationSDn
Neededtopass 5mmHg and 8mmHgTable B3. Pass/Fail Criterion 2 of the AAMI Protocol See AAMI protocol for details ‐maximumpermissiblestandarddeviationSDmasafunctionofmeanerror
maximumpermissiblestandarddeviationSDm asafunctionofmeanerror
mmHg0.0 0.1 0.2 0.3 0.4 0.5 0.6 0.7 0.8 0.9
0. 6.95 6.95 6.95 6.95 6.93 6.92 6.91 6.90 6.89 6.881. 6.87 6.86 6.84 6.82 6.80 6.78 6.76 6.73 6.71 6.682. 6.65 6.62 6.62 6.55 6.51 6.47 6.43 6.39 6.34 6.303. 6.25 6.20 6.20 6.09 6.03 5.97 5.89 5.83 5.77 5.704. 5.64 5.56 5.56 5.41 5.33 5.25 5.19 5.08 5.01 4.905. 4.79 ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐ ‐
Forexample,testsphygmomanometerwithameanerror 4.2musthaveastandarddeviationthatdoesnotexceed5.49basedonTableB3topassCriterion2.The AAMI protocol also has a same‐arm sequential test method. Initially, the two observersdetermine the subject’s blood pressure using the reference sphygmomanometer, wait at least 60seconds,determinethesubject’sbloodpressureusingthetestdevice,clearthememoryofthetestdevice by switching the device off and on, removing the bloodpressuremodule or using a resetcommand ,thenwaitatleast60seconds.Theinitialdataarenotused.Theset‐upisshowninFigureB2.
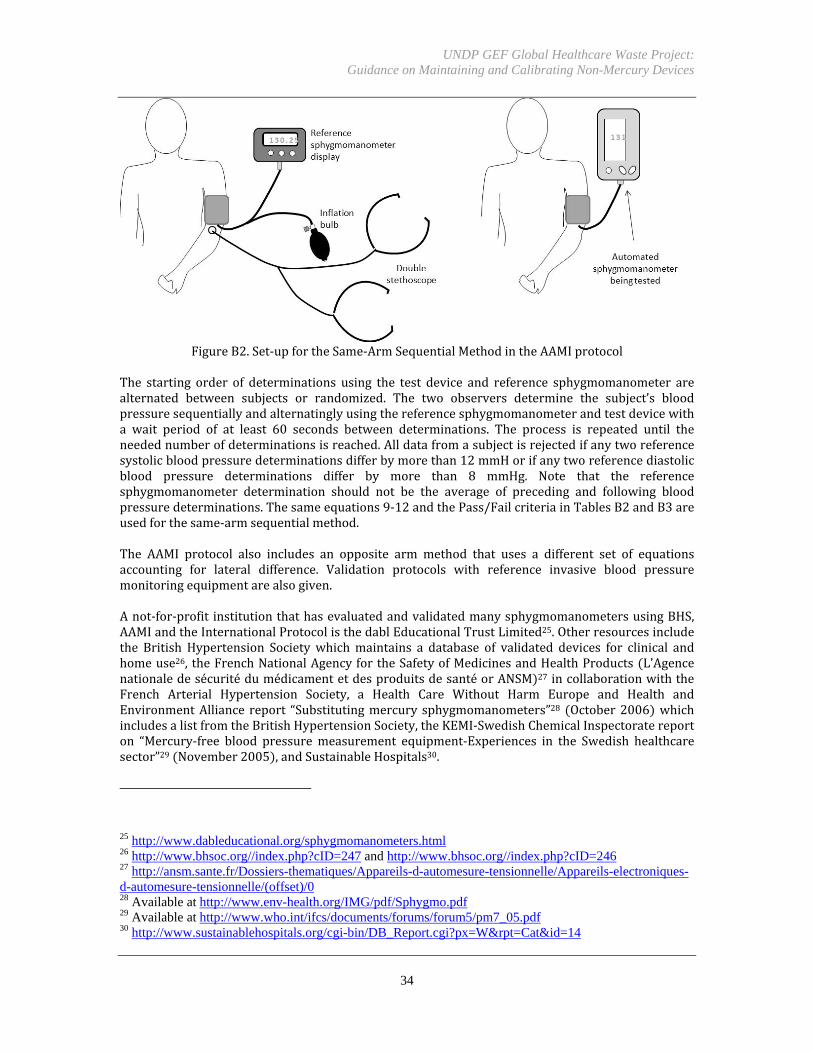
UNDP GEF Global Healthcare Waste Project: Guidance on Maintaining and Calibrating Non-Mercury Devices
34
FigureB2.Set‐upfortheSame‐ArmSequentialMethodintheAAMIprotocol
The starting order of determinations using the test device and reference sphygmomanometer arealternated between subjects or randomized. The two observers determine the subject’s bloodpressuresequentiallyandalternatinglyusingthereferencesphygmomanometerandtestdevicewitha wait period of at least 60 seconds between determinations. The process is repeated until theneedednumberofdeterminationsisreached.Alldatafromasubjectisrejectedifanytworeferencesystolicbloodpressuredeterminationsdifferbymorethan12mmHorifanytworeferencediastolicblood pressure determinations differ by more than 8 mmHg. Note that the referencesphygmomanometer determination should not be the average of preceding and following bloodpressuredeterminations.Thesameequations9‐12andthePass/FailcriteriainTablesB2andB3areusedforthesame‐armsequentialmethod.The AAMI protocol also includes an opposite arm method that uses a different set of equationsaccounting for lateral difference. Validation protocols with reference invasive blood pressuremonitoringequipmentarealsogiven.Anot‐for‐profit institutionthathasevaluatedandvalidatedmanysphygmomanometersusingBHS,AAMIandtheInternationalProtocolisthedablEducationalTrustLimited25.Otherresourcesincludethe British Hypertension Societywhichmaintains a database of validated devices for clinical andhomeuse26, theFrenchNationalAgencyfortheSafetyofMedicinesandHealthProducts L’AgencenationaledesécuritédumédicamentetdesproduitsdesantéorANSM 27incollaborationwiththeFrench Arterial Hypertension Society, a Health Care Without Harm Europe and Health andEnvironmentAlliance report “Substitutingmercurysphygmomanometers”28 October2006 whichincludesalistfromtheBritishHypertensionSociety,theKEMI‐SwedishChemicalInspectoratereporton “Mercury‐free blood pressuremeasurement equipment‐Experiences in the Swedish healthcaresector”29 November2005 ,andSustainableHospitals30.
25 http://www.dableducational.org/sphygmomanometers.html 26 http://www.bhsoc.org//index.php?cID=247 and http://www.bhsoc.org//index.php?cID=246 27 http://ansm.sante.fr/Dossiers-thematiques/Appareils-d-automesure-tensionnelle/Appareils-electroniques-d-automesure-tensionnelle/(offset)/0 28 Available at http://www.env-health.org/IMG/pdf/Sphygmo.pdf 29 Available at http://www.who.int/ifcs/documents/forums/forum5/pm7_05.pdf 30 http://www.sustainablehospitals.org/cgi-bin/DB_Report.cgi?px=W&rpt=Cat&id=14


















