Growth patterns in endometrial carcinoma
12
GYNECOLOGIC ONCOLOGY lo, 134-145 (1980) Growth Patterns in Endometrial Carcinoma’ BARRIE ANDERSON, M.D.,*2*3 FARID LOUIS, M.D.,? WATSON G. WATRING, M.D.,* AND DONALD D. EDINGER, JR., M.D.* *Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, New England Medical Center Hospital, Tufts University School of Medicine, Boston, Massachusetts 02111, and tDepartment of Pathology and Medical Research, St. Margaret’s Hospital for Women, Tufts AfYiliated Hospitals, Boston, Massachusetts 02125 Received December 3, 1979 One hundred patients with endometrial carcinoma underwent primary hysterectomy. Classification of the endometrial tumor growth patterns allowed identification of patients at high risk for myometrial penetration with a high degree of accuracy. Tumors with a diffuse origin within the endometrial cavity, and those with a polypoid or shaggy appearance, were at risk for deep myometrial penetration. When both patterns were present, 86.5% of the patients had penetration to a depth of greater than 10% of the myometrial width, and 61.1% had greater than 30% penetration. When only one of these characteristics was present, an intermediate degree of deep penetration was found. When neither diffuse origin nor bulky growth were present, the risk of penetration of greater than 10% was 4.8% and no patient had greater than 30% penetration. All recurrences were found in patients with bulky and diffuse disease. Low-pressure hysterography in the nonirradiated uterus successfully pre- dicted these patterns of tumor growth. Hysterographic information concerning tumor growth patterns can be combined with knowledge of tumor grade to identify patients at high risk for deep myometrial penetration preoperatively. Endometrial carcinoma is now the most common malignancy of the female genital tract in the United States. Major efforts have been directed at understand- ing the growth and spread of this disease. Factors which have been found to influence survival and the rate and route of recurrence include grade, depth of myometrial penetration, uterine size, and location of origin within the uterus [2,4,7,15,17,19,22,24,30]. Some of these factors are reflected in the current FIG0 Staging system (Table 1). A large percentage of patients with endometrial car- cinoma have Stage I disease [6,24]. However, these tumors represent a biologi- cally diverse group, with cure rates varying markedly with degree of differentia- tion and depth of myometrial penetration. Recent surgical studies have been directed at delineating routes of lymphatic r Presented at the June 1979 meeting of the Western Association of Gynecologic Oncology. 9 Supported in part by American Cancer Society Junior Faculty Clinical Fellowship 380B. 3 Address reprint requests to: Barrie Anderson, M.D., New England Medical Center Hospital, 171 Harrison Avenue, Boston, Mass. 02111. 134 0090-8258/80/050134-12$01.00/O Copyri&t @ 1980 by Academic Press, Inc. All rights of reproduction in any form reserved.
-
Upload
barrie-anderson -
Category
Documents
-
view
220 -
download
0
Transcript of Growth patterns in endometrial carcinoma

GYNECOLOGIC ONCOLOGY lo, 134-145 (1980)
Growth Patterns in Endometrial Carcinoma’
BARRIE ANDERSON, M.D.,*2*3 FARID LOUIS, M.D.,? WATSON G. WATRING, M.D.,* AND DONALD D. EDINGER, JR., M.D.*
*Division of Gynecologic Oncology, Department of Obstetrics and Gynecology, New England Medical Center Hospital, Tufts University School of Medicine,
Boston, Massachusetts 02111, and tDepartment of Pathology and Medical Research, St. Margaret’s Hospital for Women, Tufts AfYiliated
Hospitals, Boston, Massachusetts 02125
Received December 3, 1979
One hundred patients with endometrial carcinoma underwent primary hysterectomy. Classification of the endometrial tumor growth patterns allowed identification of patients at high risk for myometrial penetration with a high degree of accuracy. Tumors with a diffuse origin within the endometrial cavity, and those with a polypoid or shaggy appearance, were at risk for deep myometrial penetration. When both patterns were present, 86.5% of the patients had penetration to a depth of greater than 10% of the myometrial width, and 61.1% had greater than 30% penetration. When only one of these characteristics was present, an intermediate degree of deep penetration was found. When neither diffuse origin nor bulky growth were present, the risk of penetration of greater than 10% was 4.8% and no patient had greater than 30% penetration. All recurrences were found in patients with bulky and diffuse disease. Low-pressure hysterography in the nonirradiated uterus successfully pre- dicted these patterns of tumor growth. Hysterographic information concerning tumor growth patterns can be combined with knowledge of tumor grade to identify patients at high risk for deep myometrial penetration preoperatively.
Endometrial carcinoma is now the most common malignancy of the female genital tract in the United States. Major efforts have been directed at understand- ing the growth and spread of this disease. Factors which have been found to influence survival and the rate and route of recurrence include grade, depth of myometrial penetration, uterine size, and location of origin within the uterus [2,4,7,15,17,19,22,24,30]. Some of these factors are reflected in the current FIG0 Staging system (Table 1). A large percentage of patients with endometrial car- cinoma have Stage I disease [6,24]. However, these tumors represent a biologi- cally diverse group, with cure rates varying markedly with degree of differentia- tion and depth of myometrial penetration.
Recent surgical studies have been directed at delineating routes of lymphatic
r Presented at the June 1979 meeting of the Western Association of Gynecologic Oncology. 9 Supported in part by American Cancer Society Junior Faculty Clinical Fellowship 380B. 3 Address reprint requests to: Barrie Anderson, M.D., New England Medical Center Hospital, 171
Harrison Avenue, Boston, Mass. 02111.
134 0090-8258/80/050134-12$01.00/O Copyri&t @ 1980 by Academic Press, Inc. All rights of reproduction in any form reserved.

GROWTH PATTERNS IN ENDOMETRIAL CARCINOMA 135
TABLE 1 FIG0 STAGING SYSTEM FOR CARCINOMA OF THE UTE~NE CORPUS, APRIL 1970
Stage
0 I
IA IB
Gl G2 G3
II
III IV
Carcinoma in situ; histological findings suspicious of malignancy The carcinoma is confined to the corpus The length of the uterine cavity is 8 cm or less The length of the uterine cavity is more than 8 cm Stage I cases should be subgrouped as follows: Highly differentiated adenomatous carcinomas Differentiated adenomatous carcinomas with partly solid areas Predominantly solid or entirely undifferentiated carcinomas The carcinoma has involved the corpus and the cervix but does not extend outside
the uterus The carcinoma has extended outside the uterus but not outside the true pelvis The carcinoma has extended outside the true pelvis or has obviously involved the
mucosa of the bladder or rectum
extension [9,21]. A much greater frequency of pelvic node involvement has been found than was previously suspected. Degree of tumor differentiation has been directly correlated with frequency of nodal metastasis. Although uterine size as an indirect reflection of tumor volume has a positive correlation with rate of metas- tasis to lymph nodes, this relationship is less marked probably due to normal variations in uterine size and enlargement from causes other than malignancy [15,22]. A relationship between the site of origin of the tumor within the uterus (fundus vs lower uterine segment) and the pattern of lymph node metastasis has also been described, although the prognostic importance of lower uterine segment involvement is inconclusive [6,28].
In contrast with the volume of knowledge concerning extrauterine spread of endometrial carcinoma, little is known of the patterns of intrauterine growth. Few objective data are available to support the clinical impression that the intrauterine volume of tumor is correlated with the extent of disease. Hysterographic studies suggest that the intrauterine volume of tumor and its pattern of growth within the endometrial cavity reflect the aggressiveness of the tumor as measured by depth of myometrial penetration [29] and patient survival [16]. No studies to date have attempted to correlate the directly observed characteristics of endometrial surface growth with extent of myometrial penetration. The present retrospective study was undertaken to see if gross and microscopic examination of endometrial carcinoma in the nonirradiated surgically removed uterus would reveal any con- sistent growth patterns that correlated with the depth of myometrial penetration.
MATERIALS AND METHODS
The records of 620 patients with epithelial endometrial carcinoma referred to the Tufts-New England Medical Center between 1958 and July 1, 1978 were surveyed. Preoperative radiation therapy was given to the najority of patients seen between 1968 and May 1972. After May 1972, most patients with hysterographic findings consistent with deep myometrial penetration also received preoperative radiotherapy [29]. One hundred twenty patients with Stage I adenocarcinoma,

136 ANDERSON ET AL.
with or without squamous elements, received no preoperative radiation. These patients were retrospectively studied in detail.
Data were incomplete or unobtainable on 20 patients. All of the remaining 100 patients studied had had a D and C diagnosis of endometrial malignancy prior to primary surgerv. In 64 cases, hysterectomy had been performed nrior to referral. No hysterograpny had been done in any of these patients. Of the remaining 36 patients, hysterographic findings indicated a low risk of deep myometrial penetration in 30 and preoperative radiation therapy was not given. In six cases, primary hysterec- tomy was performed in spite of hysterographic findings consistent with deep myometrial penetration.
Data collected from hospital and clinic records included the depth of sounding and a clinical estimation of size. The FIG0 classification for uterine enlargement was followed, with the uterus considered to be enlarged if it sounded to a depth of greater than 8 cm. To confirm the original descriptions and to complete data collection, hematoxylin and eosin-stained sections were selected by the referring pathologists as representative samples of the observed tumor demonstrating im- portant characteristics.
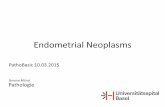
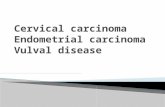
The gross and microscopic pathology reports were also reviewed. Gross de- scriptions by the primary pathologist at the time of hysterectomy were accepted of necessity. Information obtained from this source included external uterine dimen- sions, endometrial cavity size, presence of grossly distorting leiomyomata and adenomyosis, general characteristics of the endometrium and/or tumor surface, measurement of obvious polypoid structures, and estimation of the percentage of the endometrial surface involved with tumor. It was noted that the gross examina- tion carried out in an air medium failed to reveal certain details of the growth pattern that became evident on microscopic examination of the specimen fixed in a fluid medium, paraflin. Thus a gross description of a “granular” or “cobble- stone” endometrial surface was correlated with a microscopic picture of a papillary tumor measuring from l-3 mm in thickness (Fig. 1). A “shaggy,” or “heaped-up” or “polypoid” appearance was correlated with a microscopic picture of a mark- edly thickened and polypoid endometrium of greater than 3-mm thickness (Fig. 2).
Two maj,or growth characteristics were evaluated+xuberance of growth into the endometrial cavity and diffuseness of origin. These characteristics were com- bined into four major categories of gross tumor appearance (Table 2): (1) Both criteria lacking: endometrium described as flat or smooth throughout, or having either a single narrow-based polyp, or a focus of granularity, or small papillary projections confined to less than one-fourth of the entire endometrial surface; (2a) diffuse but not bulky: granular, cobblestone, or finely papillary endometrium covering an area greater than one-fourth of the endometrial surface; (2b) bulky but not diffuse: broad-based grossly polypoid tumor covering less than one-fourth of the endometrial surface; and (3) diffuse and bulky; single or multiple broad-based polyps covering greater than one-fourth of the endometrial surface.
All slides had originally been reviewed by a pathologist at the Tufts-New England Medical Center at the time of referral. The degree of differentiation and the histologic cell type were taken from this description. Review at the time of this survey by two of the authors (B.A. and F.L.) confirmed grade and type and

GROWTH PATTERNS IN ENDOMETRIAL CARCINOMA 137
FIG. 1. Group 1 growth pattern. The endometrium on gross examination appeared predominantly flat with focal granularity. Microscopic appearance is of a Grade 1 papillary adenocarcinoma of the endometrium with invasion of 10% of the myometrium (H&E, x30).
allowed direct measurement of the actual depth and percentage of myometrial penetration. The depth of myometrial penetration was measured from the basalis layer of adjacent areas of normal or minimally invaded myometrium and was recorded in millimeters. The percentage of the myometrium involved was calcu- lated.
A subgroup of 36 patients had low-pressure hysterography performed prior to hysterectomy. Hysterograms had been read prospectively and were recorded as showing focal or diffuse, shallow or large, and single or multiple defects. Radio- grams with single focal shallow defects were considered to be at low risk for deep myometrial penetration according to criteria previously reported [ 1,291. Those with large, multiple, or diffuse defects were considered to be at high risk. These interpre- tations were compared with the actual findings in the removed specimen. No attempt was made to diagnose the presence of endocervical disease, since this had already proved unsuccessful [ 11.
Follow-up for 36 months or greater was available on 47 patients. The prognostic importance of myometrial penetration, pattern of growth, differentiation of tumor, and uterine size were carefully evaluated in this group.

138 ANDERSON ET AL.
FIG. 2. Group 3 growth pattern. Multiple grossly polypoid structures covered most of the en- dometrial cavity. Microscopic appearance is of a Grade 1 adenocarcinoma with over 50% invasion of the myometrium (H&E, x30).
RESULTS
The age distribution of the patients studied is shown in Table 3. Seventy-five percent were postmenopausal and 7% were premenopausal. The menstrual state for 18% was unknown. Thirty-two percent of the patients had been on estrogen and 41% had not. The estrogen ingestion history for 23% of the patients was not available. Two premenopausal patients had taken oral contraceptives, and two postmenopausal patients had hepatic cirrhosis. Fifty-five percent had Stage IA disease and 45% had Stage IB. Seventy-seven percent of the tumors were adenocarcinomas, 12% were adenoacanthomas, 8% were adenosquamous car- cinomas, and 3% were adenocarcinomas with clear cell elements. Fifty-eight percent were Grade 1,3 1% Grade 2, and 11% Grade 3. Seventy-three percent had identifiable myometrial penetration. These characteristics identify the population studied as similar to those in other reports [18,20,21,24,26].
Classification of the tumors using the growth pattern groupings revealed a strong correlation of these groupings with depth of myometrial penetration (Table 4). Of 21 specimens in Group 1, twenty had Grade 1 or 2 lesions. The uterus was

GROWTH PATTERNS IN ENDOMETRIAL CARCINOMA 139
TABLE 2 GROWTH PATTERN GROUPINGS BASED ON DESCRIPTION OF GROSS SPECIMEN AND CORRELATED
MKROSCOPIC APPEARANCE
Growth pattern group
1
Gross description
Endometrial surface flat throughout or generally flat with a single narrow-based polyp or an area of ‘granular” appear- ante confined to less than one-fourth of the endometrial surface
Microscopic appearance
Intraepithelial growth or benign polyp with focal malignant change or focal papillary growth
2a “Granular, ” “cobblestone,” or “finely Diffuse papillary growth with endome- papillary” area covering greater than trium averaging from 1 to 4 mm in one-fourth of the endometrial surface height
2b Broad-based, grossly polypoid structures covering less than one-fourth of the endometrial surface
Focal coarsely papillary growth with endometrial height exceeding 3-4 mm
3 Single or multiple broad-based polyps covering greater than one-fourth of the endometrial surface
Diffise markedly thickened and poly- poid endometrium
normal or small in size in 10 and enlarged in 11. Histologically, 16 were adenocar- cinemas and 5 were adenoacanthomas. Five specimens had no residual tumor, and 15 had less than 10% invasion. One patient with a Grade 3 tumor had 20-2% myometrial invasion; she also had a history of pyometra and two D and C’s within 3 months prior to hysterectomy with the last D and C within 1 week of surgery.
Eleven specimens were in Group 2a. Nine of the tumors were Grade 1, one was Grade 2, and one was Grade 3. Six specimens were normal or small and five were enlarged. Ten adenocarcinomas and one adenoacanthoma were seen in this group. All had residual tumor. Seven had myometrial penetration of less than 10%. Invasion of lo-2% of the myometrium was present in two and 40-4% in two. None had greater than 50% invasion.
Sixteen tumors were in Group 2b. Ten tumors were Grade 1, five Grade 2, and one Grade 3. Eleven uteri were small or normal in size and five were enlarged. Fifteen were adenocarcinomas and one was an adenoacanthoma. In this group less than 10% of the myometrium was invaded in eight. Three had invasion of
TABLE 3 AGE DISTRIBUTION OF STUDY GROUP OF 100 PATIENTS
Age
30-34 35-39 40-44 45-49 XI-54 55-59 60-64 65-69 70-74 75-79 80-84
Number 2 2 5 7 9 21 17 20 9 6 2

TABL
E 4
DEP
TH O
FPEN
ETR
ATIO
N
IN
100
PATI
ENTS
ACC
OR
DIN
GTO
GR
OW
TH
PATT
ERN
GR
OU
P,H
ISTO
LOG
ICG
RAD
E,AN
D
UTE
RIN
E SI
ZE
Perc
enta
ge o
f m
yom
etriu
m
pene
trate
d
Gro
wth
Pa
ttern
G
roup
G
rade
U
terin
e si
ze
No
resi
dual
tu
mor
0
10
10-1
9 20
-29
30-3
9 40
-49
50-5
9 60
-69
70-7
9 80
-89
90-1
00
1 (2
1)
2a (
11)
2b (
16)
3 (5
2)
1 (1
7)
2 (3
)
3 (1
)
1 (9
)
2 (1
)
3 (1
)
1 (1
0)
2 (5
)
3 (1
)
1 (2
2)
2 (2
2)
3 (8
)
A (9
) B
(8)
A (0
) B
(3)
A (1
) B
(0)
A (5
) B
(4)
A (1
) B
(0)
A (0
) B
(1)
A
03)
B
(2)
A (3
) B
(2)
A
(0)
B
(1)
A (
10)
B (
12)
A (
16)
B
(6)
A
(2)
B
(6)
2 5
2 1
5 2
2 1
1
4 1
1 2
1 1
4 1
1 1
1 1
1 1
1 1
1 1
1
2 1
2 2
2 1
1 2
3 3
1 1
1 1
1 1
2 5
1 3
2 2
1 1
1 1
1 1
1 2
1 1

GROWTH PATTERNS IN ENDOMETRIAL CARCINOMA 141
lo-2%, two had 30-4% invasion, and in two more than 50% of the myometrium was invaded.
Fifty-two specimens were in Group 3. Twenty-two lesions were Grade 1, 22 Grade 2, and 8 Grade 3. Twenty-eight patients had normal or small uteri, 24 were enlarged. Forty were adenocarcinomas, three of which had clear cell components. Five were adenoacanthomas and seven were adenosquamous carcinomas. All specimens contained residual tumor. Only seven of this group had myometrial penetration of less than 10%. Invasion of lo-2% was present in 13, 30-39% in 9, and greater than 50% in 23.
Eleven patients had recurrent disease and of these 9 died (Table 5). Thirty-six percent of those with recurrent disease had distant spread. Forty-four percent had recurrence confined to the pelvis. Only two are currently alive at less than 2 years after treatment of the recurrence. Two additional patients died without evidence of recurrence, one of a myocardial infarction at 65 months and one of unknown cause following completion of therapy.
All 11 patients who developed recurrence originally had disease in growth pattern Group 3. None of these patients had had hysterography. Eight had adenocarcinomas, three of which were Grade 1 with myometrial penetration of less than 10,20-29, and 80-8%. Three of the adenocarcinomas were Grade 2 and penetration was 50-59, 70-7% and full thickness. Two adenocarcinomas were Grade 3 and had 30-39 and 70-7% penetration. One patient had a Grade 2
TABLE 5
CHARACTERISTICS OF RECURRENT TUMORS
Histologic type
Growth Time to Uterine pattern Percentage recurrence Site of
Grade size group invasion (months) recurrence
A.F. Adenocarcinoma
G.D. Adenocarcinoma B.B. Adenocarcinoma M.G. Adenocarcinoma
J.L.
E.C.
K.H. L.M. R.H. T.F.
Adenocarcinoma Adenocarcinoma with
clear cell component
Adenocanthoma Adenocarcinoma Adenocarcinoma Adenocarcinoma
1
1 2
2 2
<8 cm
>8 cm 3 20-29 120 >8 cm 3 80-89 34 <8 cm 3 50-59 6
<8 cm 3 full thickness 29 <8 cm 3 30-39 16
<8 cm 3 full thickness 30 Vagina, lung >8 cm 3 10-19 12 Lung >8 cm 3 30-39 60 Pelvis >8 cm 3 70-79 15 Pelvis and
3 <lO 9 Pelvis and distant Pelvis
Omentum Pelvis and
distant Vaginal vault”
Lung
E.S. Adenosquamous 3 >8 cm distant
3 50-59 12,17 Lower vagina;* supraclavicular node
D Alive, without evidence of disease 14 months after treatment for recurrence. b Alive, without evidence of disease 12 months after treatment for first recurrence, 7 months after
treatment for second recurrence.

142 ANDERSON ET AL.
TABLE 6 FREQUENCY OF HISTOLOGIC GRADE IN EACH GROWTH PATTERN GROUP
Grade 1 Grade 2 Grade 3 Number Percentage Percentage Percentage of Percentage of of Percentage of Of Percentage of of
Group patients No. group grade No. group grade No. group grade
1 21 17 81 29 3 14.3 10 1 4.8 9 2a 11 9 81.9 16 1 9.9 3 1 9.9 9 2b 16 10 62.5 17 5 31.3 16 1 6.3 9 3 52 22 42.3 38 22 42.3 71 8 15.4 73
adenoacanthoma with clear cell foci and 30-3% penetration; and one had a Grade 3 adenosquamous carcinoma with 50-5% penetration.
When analyzed by degree of differentiation (Table 4), of 89 patients with Grades 1 and 2 disease, 42 (47.2%) had less than 10% myometrial penetration, 28 (31.5%) had lo-4% invasion, and 19 (21.3%) had greater than 50% invasion. All of those with greater than 50% invasion were in Groups 2b or 3. None of the 10 patients with Grade 3 histology had less than 20% myometrial invasion; 8 (61.5%) had 20-4% invasion; and 5 (38.5%) had greater than 50% invasion. Although there was a tendency for Grade 3 lesions to be in growth pattern Group 3 (Table 6), Grade 1 and 2 lesions were fairly evenly distributed throughout the groups.
Forty-nine specimens had uterine leiomyomata; 21 of these uteri had been sounded to greater than 8 cm preoperatively. Twenty-one specimens had sig- nificant adenomyosis; 12 of these had an enlarged uterus. An additional eight patients had focal adenomyosis; two of these had a clinically enlarged uterus. Several patients had both leiomyomata and adenosis. A total of 24 patients with one or both of these changes had an enlarged uterus.
Thirty-six patients had hysterography prior to hysterectomy. Myometrial penetration of greater than 10% was present in 10 patients, and was successfully predicted in 8 (80%). Early in the hysterographic study, two patients (20%) had hysterograms prospectively interpreted as being at low risk for deep penetration, but the specimens did show penetration of 30-39 and 60-6%. When a blind review of all hysterograms was performed for this study using growth pattern criteria, all the cases with deep invasion were correctly identified.
DISCUSSION
In this attempt to correlate endometrial growth characteristics with the depth of myometrial penetration, two important correlates appeared: Diffuse lesions and those with profuse endometrial growth were at greatest risk for myometrial penetration. When these two patterns were combined (Group 3), myometrial penetration of greater than 10% was seen in 86.5% of the specimens regardless of grade of tumor or uterine size. Penetration of greater than 30% of the myometrium was present in 61.1%. When neither large nor diffuse lesions were present (Group 1) only one specimen (4.8%) had greater than 10% myometrial penetration, while 95% had less than 10% penetration. When only one criteria was present, the likelihood of deep penetration was progressively greater with invasion of more

GROWTH PATTERNS IN ENDOMETRIAL CARCINOMA 143
than 10% seen in 36.4% of patients with diffuse disease (Group 2a) and in 50.7% of those with bulky disease (Group 2b). Penetration greater than 30% was present in 18.2% in Group 2a and 12.5% in Group 2b.
Most studies have concluded that increased rates of recurrence and distant metastasis and decreased survival are associated with deep myometrial penetra- tion [3,6,8,11,12,14,28]. Since there is no uniform definition for intermediate depths of invasion, the relationship to prognosis of such invasion is not as clear.
“Supeficial” invasion of the myometrium is reported to imply no worse a prognosis than tumor confined to the endometrium [2,6,11,14]. However, in many studies, the level of invasion corresponding to “superficial” is not defined. In studies in which superficial is defined as myometrial penetration of one-third or less, recurrences are increased in patients with “deep” or greater than one-third penetration [7,15]. Studies using a 50% criterion for deep penetration have gener- ally reported less marked differences in rates of lymph node metastasis and survival [18,21,30]. A correlation of prognosis with distance of tumor invasion from the serosal surface has been found [ 11,211, but this method of measurement of penetration ignores the normal variability in width of the myometrium. Thus, a tumor penetrating to within 2 mm of the serosa may have involved from 30-90% of the uterine wall. Considering the known compartmentalization of lymphatic drainage in the uterus, a more logical approach would be to measure the actual percentage of the uterine wall that is involved.
The uterine lymphatics have three subdivisions that correspond to the three types of tissues in the organ-the endometrial epithelium, the muscularis, and the serosa [27]. The endometrial lymphatics originate in meshes surrounding the endometrial glands and drain in a peripheral direction toward the basalis layer. There they form lacunae which run in the basalis parallel to the junction with the muscularis. In addition, small lymphatic nodules have been found in the basal endometrium.
From the lacunae in the basalis, perpendicular vessels perforate the muscularis and drain peripherally, joined along the way by capillaries draining the myome- trium. As they reach the subserosa, the lymphatics turn sharply again and flatten to form lacunae with intercommunicating branches that invest the entire uterus. Although these general compartments exist, numerous anastomoses at all levels prevent the absolute isolation of any one portion of the uterus.
The third collecting system originates in the serosa itself. Capillaries that drain inward toward the subserosal network form terminal collecting trunks which then drain toward the regional lymph nodes.
The presence of this triple drainage system becomes important when consider- ing the prognostic significance of the depth of myometrial penetration. In the current study, long-term follow-up is not yet available on a sufficient number of patients to make a valid correlation of depth of penetration with survival. How- ever, 36 month follow-up is considered significant in endometrial carcinoma [10,13], and was available in 47 patients (Table 6). Ten of the tumors that recurred (90.9%) were in patients with greater than 20% myometrial invasion, a group that accounted for only 48% of all patients in the study. The 1 lth recurrence was in a patient with less than 10% myometrial invasion by a Grade 1 adenoacanthoma.

144 ANDERSON ET AL.
This patient died at 8 months with both local and distant disease. Although larger numbers are needed, there does seem to be a correlation of depth of myometrial penetration with poorer prognosis.
There was an even stronger correlation of recurrence with extensive endome- trial tumor growth patterns. All 11 patients who recurred were in Group 3. This is a disproportionate number since 100% of the recurrences occurred in a group which accounted for only 52% of all patients in the study. This correlation of greater tumor bulk with worsening prognosis has previously been reported [16].
In well or moderately differentiated tumors prognosis correlated well with endometrial growth patterns. When the pattern was diffuse and/or there was a large endometrial component, risk of penetration of greater than 20% was high. Poorly differentiated tumors (Grade 3) always behaved in an aggressive fashion, regardless of growth pattern. Of 10 patients with Grade 3 lesions, none had less than 20% myometrial invasion and 8 (80%) were in Group 3. When Grade 3 lesions were found in other groups, they were associated with deeper invasion.
Uterine size had no correlation with depth of penetration, either alone or within grades or groupings. This may be partially explained by the fact that 24% of the patients had leiomyomata and/or adenomyosis of sufficient degree to lead to uterine enlargement.
All recurrences seen to date have occurred in patients with bulky and extensive disease (Group 3). This observation indicates that close evaluation of the tumor growth pattern on the endometrial surface may be useful in identifying patients at highest risk for myometrial penetration and for decreased survival.
When the tumor growth pattern criteria described are used, low-pressure hys- terography has been successful in predicting the presence of deep myometrial penetration. When interpreting the hysterogram care must be taken to include the effect of such factors as pyometra and vigorous D and C within 1 week of evaluation.
REFERENCES 1. Anderson, B., Marchant, D. J., Munzenrider, J. E., Moore, J. P., and Mitchell, G. W., Jr. Routine
noninvasive hysterography in the evaluation and treatment of endometrial carcinoma, Gynecol. Oncol. 4, 354-367 (1976).
2. Austin, J. H., and McMahon, B. Indicators of prognosis in carcinoma of corpus uteri, Surg. Gynecol. Obstet. 128, 1247 (1969).
3. Barber, K. W., Dockerty, M. B., Pratt, J. H., and Hunt, A. B. Prognosis in endometrial carcinoma by moditied Duke’s typing, Surg. Gynecol. Obstet. 114, 155 (1%2).
4. Beck, R. P., and Latour, J. P. Necropsy reports on 36 cases of endometrial carcinoma, Amer. J. Obstet. Gynecol. 85, 307-311 (1963).
5. Boutselis, J. G., Blair, J. R., Vorys, N., and Ullery, J. C. Carcinoma of the uterine corpus, Amer. J. Obstet. Gynecol. 85, 994 (1%3).
6. Carmichael, J. A., and Bean, H. A. Carcinoma of the endometrium in Saskatchewan, Amer. J. Obstet. Gynecol. 97, 294 (1967).
7. Cheon, H. D. Prognosis of endometrial carcinoma, Obstet. Gynecol. 34, 680 (1%9). 8. Corscaden, J. A., and Tovell, H. M. The management of carcinoma of the corpus, Amer. J.
Obstet. Gynecol. 68, 737 (1954). 9. Creasman, W. T., Boronow, R. C., Morrow, C. P., DeSaia, P. J., and Blessing, J. Adenocar-
cinema of the endometrium: Its metastatic lymph node potential, Gynecol. Oncol. 4, 239-243 (1976).

GROWTH PATTERNS IN ENDOMETRIAL CARCINOMA 145
10. Dede, J. A., Plentl, A. A., and Moore, J. G. Recurrent endometrial carcinoma, Surg. Gynecol. Obster. 126, 533 (1968).
11. Finn, W. F. Time, site and treatment of recurrences of endometrial carcinoma, Amer. Obsret. Gynecol. 60, 773 (1950).
12. Gusberg, S. B., Jones, H. C., and Tovell, H. M. M. Selection of treatment for corpus cancer,Amer. J. Obstet. Gynecol. 80, 374 (1960).
13. Gusberg, S. B., and Yannopoulos, D. Therapeutic decisions in corpus cancer, Amer. J. Obster. Gynecol. 88, 157 (1964).
14. Hirabayashi, K., and Graham, J. Clinical classification of carcinoma of the uterine body, Surg. Gynecol. Obstet. 126, 75 (l%S).
15. Homesley, H. D., Boronow, R. C., and Lewis, J. L., Jr. Treatment of adenocarcinoma of the endometrium at Memorial-James Ewing Hospitals, 1949-1%5, Obstet. Gynecol. 47, 100-105 (1976).
16. Johnsson, J. E., and Norman, 0. Relation between prognosis in early carcinoma of the uterine body and hysterographically assessed localization and size of tumor, Gynecol. Oncol. 7,71-78 (1979).
17. Jones, H. W. Treatment of adenocarcinoma of the endometrium; Obstet. Gynecol. Surv. 30, 147-169 (1975).
18. Joslin, C. A, et al. The treatment of early cancer of the corpus uteri, Brit. J. Radiol. 50, 38-45 (1977).
19. Kagan, A. R., Nussbaum, H., Ziel, A., and Gordon, J. Adenocarcinoma of the endometrium. Vaginal recurrences and mortality, Amer. J. Radiol. 123, 567-570 (1975).
20. Kistner, R. W., Reagan, J. W., Krantz, K. E., et al. Endometrial cancer: Rising incidence, detection and treatment, J. Reprod. Med. 10, 53 (1973).
21. Lewis, B. V., Stallworthy, J. A., and Cowdell, R. Adenocarcinoma of the body of the uterus, J. Obstet. Gynecol. Brit. Commonw. 77, 343 (1970).
22. Lewis, G. C., Mortel, R., and Slack, N. H. Endometrial cancer. Therapeutic decision and the staging process in early disease, Cancer 39, 959-966 (1977).
23. Lutz, M. H., Underwood, P. B., Kreutner, A., Jr., and Miller, M. C. Endometrial carcinoma: A new method of classification of therapeutic and prognostic significance, Gynecol. Oncol. 6, 83-94 (1978).
24. Malkasian, G. D., McDonald, T. W., and Pratt, J. H. Carcinoma of the endometrium-Mayo Clinic experience, Mayo Clin. Proc. 52, 175-180 (1977).
25. Morrow, C. P., DiSaia, P. J., and Townsend, D. E. Current management of endometrial car- cinoma, Obstet. Gynecol. 42, 399-406 (1973).
26. Parsons, L., and Cesare, F. Wertheim hysterectomy in the treatment of endometrial carcinoma, Surg. Gynecol. Obsfet. 108, 582 (1959).
27. Plentl, A. A., and Friedman, E. A. Lymphatic system of the female genitalia: The morphologic basis of oncologic diagnosis and therapy, Vol2: Major problems in obstetrics and gynecology, Saunders, Philadelphia Chap. 9 (1971).
28. Schwartz, A. E., and Brunschwig, A. Radical panhysterectomy and pelvic node excision for carcinoma of the corpus uteri, Surg. Gynecol. Obstet. 105, 675 (1957).
29. Tak, W. K., Anderson, B., Vardi, J. R., Beecham, J. B., and Marchant, D. J. Myometrial invasion and hysterography in endometrial carcinoma, Obstet. Gynecol. 50, 159-165 (1977).
30. Thiede, H. A., and Lund, C. J. Prognostic factors in endometrial adenocarcinoma, Obstet. Gynecol. 20, 149 (1962).