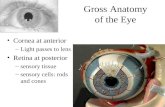
Gross Anatomy
33
Gross Anatomy Gross Anatomy “Big” and Really Cool
description
Gross Anatomy. “Big” and Really Cool. The Skeleton. 206 Bones Axial: Skull, Vertebral, Sternum, Ribs Appendicular. General Features: Long Bones. Diaphysis : Shaft, cylindrical medullary cavity, Compact bone Epiphysis : Expanded Ends, Cancellous Bone Articular Cartilage. More Features:. - PowerPoint PPT Presentation
Transcript of Gross Anatomy

Gross AnatomyGross Anatomy
“Big” and Really Cool

The SkeletonThe Skeleton206 BonesAxial: Skull,
Vertebral, Sternum, Ribs
Appendicular

General Features: Long BonesDiaphysis: Shaft, cylindrical
medullary cavity, Compact boneEpiphysis: Expanded Ends,
Cancellous BoneArticular Cartilage

More Features:More Features:Periosteum: Outside
membranous covering, dense connective tissue, blood vessels, nerves, osteoblasts
Endosteum: Medullary lining, osteoblasts


Movement MomentsMovement MomentsFlexion / ExtensionPlantar Flex / Dorsi Flex: FootPronate / Supinate: HandEversion / Inversion: FootAbduct /Adduct

HistologyHistology
Tissue Organization within Skeletal Bone
Tissue

Microscopic AnatomyMicroscopic Anatomy Compact:
“solid”, ~80% of the bone mass
Cancellous: “spongy”, 20%

Compact: TerminologyOsteon or Haversian System:
“Packed tree rings” around the Haversian canal (blood vessels)
Lamellae: “laminated” layersLacunae: “lakes” with osteocyte
“islandsCanaliculus: “Little canals”


Cancellous: TerminologyCancellous: TerminologyTrabecula: Networks of rods and
plates in spongy boneRed Marrow: Blood cell production
Children more abundantAdults: mostly axial, proximal
Yellow Marrow: Mostly Fat


The “Osteo” Cells:The “Osteo” Cells:Osteoblasts: perimeters of
the trabeculae or periosteum and endosteum of compact bone
Osteocytes: lacunae, “old blasts”
Osteoclasts: Perimeter

Bone Growth and Bone Growth and RemodelingRemodeling

Template: Model - FormTemplate: Model - FormOsteoblasts begin
depositing mineralized ECM in some type of connective tissue:Intramembranous: skull etcEndochondral: all other
bones


DirectionsDirections of bone of bone growthgrowthEndochondral: lengthening
ends with closure of epiphyseal plates
Appositional: widening - can continue throughout life

What?What?Endochondral or
Endochondral?Template
MaterialGrowth
Direction

Growth TermsGrowth TermsPrimary Ossification Centers:
Diaphysis, periosteum “collar”Secondary Ossification
Centers: Epiphyses, Epiphyseal Plates:
cartilagenous joints between Primary & Secondary centers

Assignment:Assignment:Check out on your Surface
IdentificationPredict Questions: Pages 114, 117,
149Open and Bookmark the following
website:eSkeleton: eSkeleton: http://www.eskeletons
.org/

Wrapping Up Skeletal Anatomy and Physiology

The JointsSynarthrosis:
Fibrous - immovable
Amphiarthrosis: Cartilaginous - some movement

Synovial Joints: CapsulesHighly
movable, Hinge, Pivot,
Saddle, Ball & Socket etc.

Structure /Function: Structure /Function: JointsJointsShape of articulating surfaces
determines range of motion (ROM) / Stability
Connective tissue influences ROM
Soft tissue influences ROM

Back Health - Vertebral Back Health - Vertebral ColumnColumnNormal Curves:
Cervical = anterior, Thoracic = posterior, Lumbar = anterior, Sacral = posterior
Functions: Balance, strength, and “shock absorption”

Excessive CurvesKyphosis: “Hunchback”Lordosis: “ Swayback”Scoliosis: Lateral curves
resulting in hip/shoulder uneveness

Bone RemodelingBone RemodelingMaintenance of Bone: Balance
between Osteoclasts vs Osteoblasts
Calcium demands vs. Calcium intake
Healthy bones = Osteoblast=/> than Osteoclast activity


Bone RepairBone RepairClot formation: ImmediateCallus formation: Beginning 2-
3 days after injuryCancellous Bone: Osteoblasts
invade callus - 4-6 weeks laterCompact bone: Replacing
Cancellous - months later


QuestionQuestion:Why do we immobilize
fractured bones?What are the negative
effects of prolonged immobilization?

Answer:Answer:To assist formation of good
callus, reduce painMuscle atrophy, joint
mobility, reduced stimulus to bone growth

And Now, A Movement Moment
Flex / ExtPronate /
SupinateEvert / InvertAbduct /AdductCircumduction