GP Synergy
64
GP Synergy Annual Report 2011-2012
Transcript of GP Synergy

GP SynergyAnnual Report 2011-2012

GP Synergy registrar workshop

ContentsAbout us 02
Our training regions 04
Chair report 06
Board 08
Governance 12
Chief Executive Officer report 18
Director of Training report 20
Director of Prevocational Education & Training report 22
Staff 24
Training practice support and development 26
Training competent and confident registrars 30
Aboriginal health 36
Expanding the general practice profession 38
1
GP Synergy Annual Report 2011-2012

2
GP Synergy Annual Report 2011-2012
About us
GP Synergy hospital GP registrar workshop
Our history
GP Synergy is one of 17 Regional Training Providers (RTPs) delivering the Australian General Practice Training (AGPT) and Prevocational General Practice Placements Program (PGPPP).
GP Synergy was formed in 2009 with the merger of training providers the Sydney Institute of General Practice Education and Training (SIGPET) and New England Area Training Services (NEATS).
In January 2010, a further amalgamation occurred with the Institute of General Practice Education and Training (IGPE) training program. The result has been the creation of the second largest training provider in Australia, offering doctors a diverse range of training experiences in both urban and rural environments across metropolitan and outer-metropolitan Sydney and within the New England/Northwest region of NSW.
Our mission
GP Synergy’s mission is “To train highly skilled medical practitioners contributing to healthier communities”.
Providing a supportive and quality learning environment is a shared value amongst all GP Synergy medical educators, supervisors and training practices. GP Synergy’s highly regarded reputation as a leading provider of general practice education and training is a testament to our ongoing commitment to helping doctors build the skills to develop into a confident and highly qualified general practitioners.
Our vision is to:
• provide high quality general practice education and training
• build capacity by supporting and developing quality teaching environments centered on general practice
• promote the privileges, responsibilities and diverse career opportunities of general practice
• develop internal processes and resources to ensure that the organisation learns and grows.
Our organisation is underpinned the following values:
• collaboration
• integrity
• equity
• leadership
• commitment to excellence in life-long learning.

33

4
GP Synergy Annual Report 2011-2012
Our training regions
In 2011-2012 GP Synergy offered vocational and prevocational training opportunities across our urban and rural training regions.
Urban training region
GP Synergy’s urban training footprint is extensive and diverse, stretching across Sydney from Brooklyn and Hornsby in the north down beyond Campbelltown, Camden and Picton in the south. It includes the northern and southern coastal areas from the Northern Beaches to the Sutherland Shire. From the east coast our region extends west across central and inner western Sydney, through Bankstown, Liverpool and Fairfield local government areas.
During the 2011-2012 period, over 160 general practices were accredited to provide general practice training across metropolitan and outer-metropolitan Sydney.
Within our urban training boundaries, we work with a number of Divisions of General Practice as key stakeholders, including:-
• Eastern Sydney Division of General Practice• Sutherland Division of General Practice• Sydney South West GP Link (formerly Macarthur
Division of General Practice)• Bankstown Division of General Practice• Central Sydney General Practice Network• General Practice Northside Network• Manly Warringah Division of General Practice• Northern Sydney General Practice Network• South Eastern Sydney Division of General Practice
GP Synergy also maintains close ties with the four universities located within GP Synergy’s Sydney boundaries – the University of Sydney, the University of NSW, the University of Notre Dame and the University of Western Sydney.
During the 2011-2012 financial year GP Synergy continued to strengthen and build relationships with many of the 18 teaching hospitals located within the Sydney basin in the roll-out of the expanded Prevocational General Practice Placements Program (PGPPP) and other collaborative marketing activities.
Cambelltown
Coogee
Maroubra
Bondi
Fairfield Sydney CBD
Manly
Bankstown
Dee Why
Brooklyn
Liverpool
HurstvilleRockdale
Camden
Leichhardt
Marrickville
Abbotsford Woollahra
Hornsby
Pennant Hills
Ryde
North Sydney
Mosman
CronullaSutherland
Sylvania
Menai
Frenchs Forest
Canterbury
Randwick
Chatswood
Picton
The Oaks
New England/ Northwest
Sydney Central and
South/Southwest

5
Rural training region
GP Synergy’s rural training region is located in the New England/Northwest region of NSW.
The area remains at the centre of rural medical training development, with a medical school in the regional centre of Armidale and an integrated, modern teaching hospital located in Tamworth.
During 2011-2012 there were over 25 general practices accredited to deliver vocational GP training in the region. Practices were located across the region in large regional centres and many smaller communities. Locations included Armidale, Bingara, Glen Innes, Gunnedah, Inverell, Manilla, Moree, Tamworth, Warialda and Wee Waa.
Practices in Inverell and Tamworth were also accredited and provided prevocational training opportunities to junior doctors as part of the PGPPP program.
GP Synergy continued to work closely with the local Divisions of General Practice in the area (Barwon Division of General Practice, New England Division of General Practice and Northwest Slopes Division of General Practice) until their amalgamation into the Medicare Local in April 2012. Following this amalgamation, GP Synergy extended this working relationship to encompass the newly formed entity.
GP Synergy continues to work closely with the local University located within the New England/Northwest region – the University of New England – to foster and develop interest in rural general practice within the region and explore vertical education learning opportunities. We continue to maintain strong relationships with the two training hospitals in the region – Tamworth Rural Referral Hospital and Armidale Hospital. Both sites continued to support procedural skills placements in the 2011-2012 period, with Tamworth Hospital also maintaining support for PGPPP placements and rural general practice recruitment activities.
“ In 2011-2012 GP Synergy offered vocational and prevocational training opportunities across our urban and rural training regions.”
Moree
Wee Waa
Warialda
BingaraInverell
Glen Innes
Narrabri
Manilla
Armidale
GunnedahTamworth
Werris Creek
Sydney1 hour flight
Gold Coast1.5 hour flight
Coffs Harbour2.5 hour drive
New England/ Northwest
Sydney Central and
South/Southwest

6
GP Synergy Fusion Workshop
Chair report
GP Synergy Annual Report 2011-2012
It is a pleasure to be able to take the opportunity to share with you some of the achievements and the ongoing opportunities that have been part of the 2011-12 year for GP Synergy.
The GP Synergy board is made up of highly skilled directors who have all been focused on achieving our vision: “To train highly skilled medical practitioners contributing to healthier communities.”
In March 2012, a strategic plan was developed which articulated that we would commit to:
1. Providing individualised support for all learners and stakeholders:Drawing upon research and evidence to support good practice in advocacy and policy development.
2. Facilitate excellent medical education with contemporary modes of delivery:Provision of core and individualised training supported by a selection of elective modules that facilitate the individual doctors learning interests and aspirations.
3. Creating a workplace that supports, educates and trains all staff to reach their full potential in support of our doctors (supervisors, registrars and PGPPP participants) and stakeholders:Customer service is at the core of our business and we strive to provide tailored professional development to all staff to assist them in understanding the needs of our stakeholders.
4. A system that identifies and uses innovation:We will strive to identify, develop and utilise relevant innovative ideas, ensuring they are adding value and are consistent with our direction and the needs of our stakeholders.
There is no doubt that over 2011-12 the board has seen the GP Synergy team work hard to achieving the goals of this strategic plan.
We have seen the roll-out of videoconferencing equipment to level 1 teaching practices, along with state of the art medical equipment, to assist teaching practices deliver best practice general practice training.
Record numbers of registrars have enrolled into our regional training programs and we have also seen record numbers of new supervisors enlisting to become part of the growing ‘education team’.
The staff are constantly reviewing the ‘what, how, when and why’ of all that we do and endeavour to ensure all the programs are designed to meet the goals of the company. We appreciate constructive feedback at all times so that improvements can be achieved across the organisation as required.
In line with the strategic plan we have also committed funds to redesigning our IT interface with our registrars and supervisors, and look forward to the launch of a new GPRime in early/mid 2013.
I am now looking forward to more exciting projects and innovations in 2012-13.
Dr Charlotte Hespe Chair

77

8
GP Synergy Annual Report 2011-2012
Board directors
Dr Charlotte Hespe – Chair
MB BS (Hons) (Syd), DCH (Lon), FRACGP,
FAICD, GCUT (UNDA)
27 December 2011 - present
Dr Charlotte Hespe is chair of the GP Synergy board. She has also previously been the SIGPET chair. Charlotte works as a GP and supervises registrars for GP Synergy and teaches medical students within her group family medical practice in Glebe. She is actively involved with the Royal Australian College of general Practitioners (RACGP) and is currently on the executive council of the NSW/ACT RACGP Faculty board. She was the national coordinator for the RACGP clinical exam and on the Board of Assessment from 2004-2011. She is currently head of general practice and primary care research for the Notre Dame Post-Graduate Medical Program in Sydney. Charlotte is also a director on the boards of Inner Western Sydney Medical Local and GP NSW. Charlotte has been a board director since SIGPET’s conception in 2001.
Dr Nada Andric
B. MedSci and MB BS (Syd), FRACGP
29 October 2010 - 28 October 2011
Nada is the General Practice Registrars Association (GPRA) nominee for the GP Synergy board, and completed her GP training with GP Synergy in 2011. She currently works at Earlwood General Practice part-time, spending the rest of her time with her two small children.
Dr Owen Brookes
MB BS (Sydney), FRACGP
1 January 2010 - 28 October 2011
Dr Owen Brookes is a full-time GP practising in small suburban practice in Engadine in southern Sydney. He has been a practising GP for over 20 years. He is a member of the board of the Sutherland Division of General Practice and a former chair. Owen was a member of the board for IGPE for six years and chairman for three years.

9
Assoc Prof Lyn Fragar AO
MB BS (USYD), DTM&H (USYD), MPH (USYD), Dip Ag
Ec (UNE), FAFPHM, Grad Dip Ornithology (CSU)
2 January 2009 - present
A/Prof Lyn Fragar is the chair of the Hunter New England Local Health District board. She is a senior researcher with the Australian Centre for Agricultural Health and Safety, a research centre of the University of Sydney based Moree in northwestern NSW. Lyn has previously been employed as the area medical superintendent overseeing six hospitals in the northwest region. She has also spent nine years working in Papua New Guinea, initially as a medical officer, then as a provincial health officer. In 2002 she was awarded the Order of Australia for pioneering service to rural health care and farm safety issues in Australia. Lyn’s other achievements include being awarded the Rotary International Award for Vocational Excellence in 2002, the Australian Medical Association award for ‘The best individual contribution to health care in Australia in 1999’, the Lou Ariotti Award for Excellence in Innovative Rural Health Research in 1996, and the Australian Hospital Association National Outreach Award in 1987.
Assoc Prof Michelle Guppy
MB BS, FRACGP, MPH
2 January 2009 - present
Dr Michelle Guppy is an associate professor of general practice at the School of Rural Medicine, University of New England, and conjoint with the University of Newcastle. She is a practising GP in Armidale. Michelle has been involved in rural undergraduate medical education in Armidale since 2003, and prior to that at the University of Queensland in Brisbane.
Dr Ian KamermanMB BS, FACRRM, FRACGP, DRANZCOG, DA,
ACCAM, Dip CD, SFCD
28 October 2011 - present
Dr Ian Kamerman has been a rural GP trainer for over 10 years. He is a director of GP Synergy, the Rural Doctors Association of Australia and the National GP Supervisors Association. He is a member of the board of Hunter New England Local Health District and a member of the General Practice Council of the NSW Ministry of Health. He is currently chair of the Australian College of Rural and Remote Medicine’s (ACRRM) Professional Development Committee and NSW PESCI panel. He is an enthusiastic trainer with an interest in training within a ‘patient centred medical home’ model and addiction medicine.

10
GP Synergy Annual Report 2011-2012
Board directors (continued)
Dr Jeremy Keh
B.Med.Sc. (Hons), MB BS, DCH, FRACGP
8 November 2011 - present
Dr Jeremy Keh is the GPRA nominee on the GP Synergy board. As a recent successful graduate of the RACGP, Jeremy undertook his registrar training through GP Synergy. He graduated from the University of Queensland in 2007, following which he did his junior medical training at Liverpool Hospital, where he was the Resident Medical Officer Association president. He has a keen interest in paediatrics for which he has successfully completed the Diploma in Child Health.
Dr Jacqueline Korner
MB BS, DRCOG, MRCGP
28 February 2007 - present
Dr Jacqueline Korner is the General Practice National GP Supervisor Association nominee on the GP Synergy board. Jacqueline is a long standing practice principal in Summer Hill and is a supervisor for GP Synergy. She also teaches medical students. Jacqueline has been a director since 20 December 2006.
Prof Siaw-Teng Liaw
MB BS, Dip Obst, GAICD, PhD, FRACGP, FACHI
1 January 2010 - present
Dr Liaw is a professor of general practice at UNSW and director of the Academic General Practice Unit, based at Fairfield Hospital in Sydney. He is a practising GP with extensive experience in using mixed methods research. He has a long-standing interest in the health of Indigenous peoples and is a chief investigator in the NHMRC Centre of Research Excellence in eHealth and the APHCRI Centre of Research Excellence in Obesity. He is a director of the UNSW Research Centre for Primary Health Care and Equity as well as a member of the management committee of the UNSW Asia-Pacific Research Centre for ubiquitous healthcare. He is a member of the NSW Health Acute Care Taskforce and the Sydney Integrated Clinical Training Network Advisory Committee. He chairs the RACGP National Research and Evaluation Ethics Committee. Internationally, he is a member of the American Medical Informatics Association International and Ethics Committees as well as is a member of the International Medical Informatics Association Academy Taskgroup.

11
Dr Harry NespolonMB BS, DipRACOG B.Ec LL.B (Hons), FRACGP,
FACLM, GCLP, MBA, FAICD
31 October 2007 - 28 October 2011
Dr Harry Nespolon is chair of the Northern Sydney GP Network, and a board director for GPNSW and the Sydney North Shore and Beaches Medicare Local. He is the principal of two general practices in Sydney. Harry is a former GP Synergy chair.
Prof Jennifer Reath
MB BS, Dip RACOG, FRACGP, MMed
29 October 2010 - present
Prof. Jenny Reath is the foundation Peter Brennan chair of general practice at the University of Western Sydney (UWS). She has worked for most of her career in Aboriginal and Torres Strait Islander health including as a GP in Aboriginal Community Controlled Health Services in both urban and rural Australia for more than 20 years. She continues as a part-time GP at the Aboriginal Medical Service Western Sydney where she has worked for over 14 years. Prof. Reath has held a number of intersecting roles across general practice and Indigenous health. Prior to her appointment at UWS she was an associate professor of Indigenous primary health care at the Poche Centre for Indigenous Health at the University of Sydney as well as GP manager of the RACGP’s Aboriginal and Torres Strait Islander Health Unit.
Dr Narelle Shadbolt
MB BS, FRACGP, MFM (Monash)
8 November 2011 - present
Dr Narelle Shadbolt is the nominee of the University of Sydney on the GP Synergy board. She is a senior lecturer in general practice in the Discipline of General Practice; associate dean student support and head of the discipline of general practice northern for the Sydney Medical School; sub dean and director of the clinical school and Academic General Practice Unit at Hornsby Hospital and in clinical practice at the Hornsby Hospital General Practice Unit. Narelle’s special area of interest is the health and well-being of doctors and students, medical education and clinical assessment in primary care.

12
GP Synergy Annual Report 2011-2012
Company structure
GP Synergy Limited is a public company limited by guarantee not having share capital and was incorporated under the Corporations Act 2001 (New South Wales) on 27 December 2001 under the name of Sydney Institute of General Practice Education and Training Limited.
Member organisations may nominate a person to serve as a director on GP Synergy’s board subject to successful election at the respective annual general meeting. Nominations open annually in preparation for elections which are generally held late October each year.
In 2011, the constitution was amended to stipulate the GP Synergy’s board may consist of nine member elected directors, with each director requiring to retire after three year’s tenure.
Members
During 2011-2012 members of GP Synergy consisted of:
• Bankstown Division of General Practice
• Barwon Division of General Practice,
• Central Sydney General Practice Network
• Eastern Sydney Division of General Practice
• General Practice Northside Network
• General Practice Registrars Association
• Manly Warringah Division of General Practice
• National General Practitioners Supervisor’s Association
• New England Division of General Practice
• Northern Sydney General Practice Network
• Northwest Slopes Division of General Practice
• South Eastern Sydney Division of General Practice
• Sutherland Division of General Practice
• Sydney South West GP Link (formerly Macarthur Division of General Practice)
• University of New England
• University of Notre Dame
• University of NSW
• University of Sydney
• University of Western Sydney
Many of GP Synergy’s members are Divisions of General Practice who may have amalgamated into Medicare Locals in April 2012. Following these amalgamations, GP Synergy has and continues to extend this working relationship to encompass the newly formed entities.
Board sub-committees
GP Synergy works closely with a range of stakeholders in our delivery of high quality general practice education and training. One of the ways we do this is through board sub-committees.
Education Committee
The Education Committee is a sub-committee of the GP Synergy board.
Members:
• Membership includes people from a broad range of medical education expertise and backgrounds, including at least two board members, one of which is appointed by the board to be chair of the committee.
• The CEO, DoT, medical educators and other staff (by delegation of management) are also members of the committee.
• The committee also includes registrar and supervisor representatives.
Appointment to the committee is for a term of two years, and may be renewed.
The Education Committee meets quarterly with the following objectives:
• To develop and oversee the implementation, delivery and evaluation of GP Synergy’s education and training activities, considering and applying:
1. contractual requirements and college standards
2. best practice, innovation and leadership in medical education
3. vertical and horizontal integration of medical education and training
4. GP Synergy’s Quality Framework
• To develop guidelines for, and oversee the implementation of, research activities in relevant medical education and clinical areas by GP Synergy.
Governance

13
In 2011-2012, under the chairmanship of board director, Dr Siew-Teng Liaw, the committee has been fundamental in the development and implementation of an education and research strategy, underpinned by a quality framework, that aligns with the strategic goals set by the board.
“ GP Synergy works closely with a range of stakeholders in our delivery of high quality general practice education and training.”
Dr Anne Eastwood, Deputy Director of Training

14
Aboriginal and Torres Strait Islander Committee
Following the amalgamation of NEATS and SIGPET, an Aboriginal and Torres Strait Islander Health Advisory committee had been formed to ensure input into issues surrounding the relevant services. While the concept was and is excellent, the actual implementation did not always work as desired.
To improve the effectiveness of this committee, in 2011 the terms of reference were amended to encourage input from all Aboriginal Medical Services within the geographical regions of GP Synergy that have a structure and provide health services.
Members of the Aboriginal and Torres Strait Islander Health Committee include:
• by default, all Aboriginal Community Controlled Health Services (ACCHS) that come within the geographical boundary of GP Synergy, that have an operational structure and provide health delivery services (with the exception of an ACCHS that elects to opt out)
• GP Synergy board director
• GP Synergy CEO
• GP Synergy DoT and / or an educator with expertise in Aboriginal health education and training
• an Aboriginal GP registrar, or if unavailable, a GP registrar who is trained in Aboriginal health
• a representative of the Aboriginal Health and Medical Research Council (AH&MRC)
• other properly constituted Aboriginal and Torres Strait Islander organisations that apply in writing and are accepted by resolution of the committee
• the GP Synergy Aboriginal and Torres Strait Islander Liaison Officer.
The role of the Aboriginal and Torres Strait Islander Committee is to consider the development and delivery of effective education for GP registrars in the area of Aboriginal and Torres Strait Islander Health within the Framework for General Practice Training in Aboriginal and Torres Strait Islander Health.
This involves:
1. interpretation of the most effective ways of applying the relevant parts of the RACGP and ACRRM curricula to training in Aboriginal and Torres Strait Islander health incorporating and reflecting local priorities and concerns.
2. examination all of GP Synergy’s educational activities and equity programs with a view to ensuring that all recognise and help address the concerns and needs of Aboriginal and Torres Strait Islander peoples in a culturally sensitive and appropriate way;
3. establishment of formal and effective relationships between GP Synergy and other organisations and individuals which strive for improvement in the health of the Aboriginal and Torres Strait Islander communities and which facilitate effective Aboriginal and Torres Strait Islander training;
4. assistance in development and implementation of procedures for the recruitment of GP registrars to work in the Aboriginal Medical Services and to support the cultural mentors who in turn support them. GP Synergy recognises:
a. the need for Aboriginal Medical Services to employ registrars who are appropriately sensitive and responsive to the needs of their clients
b. the attractiveness of these posts and the training opportunities offered to registrars
c. the need to maintain continuity of supply and support.
d. guidance and support for GP Synergy’s Aboriginal and Torres Strait Islander Liaison Officer in the discharge of her/his duties
e. identification for ways in which the needs and the aspirations of the Aboriginal and Torres Strait Islander communities can be incorporated into the governance and operations of GP Synergy
f. to monitor and aim to enhance GP Synergy’s compliance with the Aboriginal and Torres Strait Islander Health Framework.
GP Synergy Annual Report 2011-2012
Governance (continued)

15
Finance and Audit Committee
Members 1 July-28 October 2011: A/Prof Lyn Fragar (Chair), Dr Harry Nespolon, Dr Jacqueline Korner, Dr Charlotte Hespe, Dr Nada Andric.
Members 29 October 2011-30 June 2012: A/Prof Lyn Fragar (Chair), Dr Narelle Shadbolt, Dr Jacqueline Korner, Dr Charlotte Hespe, Dr Jeremy Keh.
The Finance and Audit Committee meets monthly.
The committee is responsible for reviewing the integrity of financial reporting and overseeing the independence of auditors. It primarily focuses on: major judgmental areas; significant adjustments, accounting and financial reporting issues and legal requirements resulting from the audit; compliance with accounting policies and standards, and legal requirements; and analysis of the company’s financial performance.
Nominations Committee
Members 1 July-28 October 2011: Dr Owen Brookes (Chair), Dr Charlotte Hespe, Dr Harry Nespolon and Mr John Oldfield.
Members 29 October 2011-30 June 2012: A/Prof Michelle Guppy (Chair), Dr Charlotte Hespe, Dr Jacqueline Korner and Mr John Oldfield.
During the 2011-2012 financial year the committee met in August 2011, October 2011 and May 2012
The role of the Nominations and Constitutional Review Committee is to assist the board with effective discharge of its responsibilities to establish and maintain the nominations and elections processes under the provisions of the company constitution.
The committee is required to review and make recommendations about constitutional matters and oversee the drafting of constitutional amendments as appropriate. The committee also oversees awards programs of GP Synergy.
“ The role of the Aboriginal and Torres Strait Islander Committee is to consider the development and delivery of effective education for GP registrars in the area of Aboriginal and Torres Strait Islander Health.”

16
GP Synergy Annual Report 2011-2012
Governance (continued)
Regional Advisory Forums
Regional Advisory Forums are subcommittees of the GP Synergy board and subcommittees have been established to represent interested stakeholders within each regional node of GP Synergy.
There are three advisory committees – Sydney Central, Sydney South/Southwest and New England/Northwest.
The role of the Regional Advisory Forums are to consider regional health services and issues in context to primary care training (particularly GP education and training), investigate and report on GP Synergy’s influence (potential or real) and performance in these areas.
Key areas of focus are:
1. general practice workforce supply and demand issues within the respective node
2. report in GP Synergy’s education and training performance within each node
3. report on GP Synergy’s performance in responding to relevant regional issues where GP Synergy has or might have influence
4. consider and make recommendation to the GP Synergy board on models of best practice in medical education and workforce development that meet the needs of the region
5. consider and make recommendation to the GP Synergy board on opportunities for collaboration with regional industry stakeholders and organisations with the aim of adding value to medical education, training and medical workforce development in the respective region.
Sydney Central Regional Advisory Forum
The Sydney Central Regional Advisory Forum met in March 2012.
Members include representatives from member organisations located within, or spanning across, the Central Sydney region such as universities, Divisions of General Practice/Medicare Locals, National GP Supervisor Association (NGPSA), GP Registrars Association (GPRA), the GP Synergy registrar liaison officer and CEO.
Members in attendance at the March 2012 meeting included: Dr Jacqueline Korner (Chair) – NGPSA, Ms Jenny Sikorski – Northern Sydney General Practice Network Inc, Ms Amanda Jones – South Eastern Sydney Division of General Practice, Prof. Simon Willcock – University of Sydney, Dr Linda Mann – Central Sydney General Practice Network, Mr. John Oldfield – GP Synergy.
The advisory forum shared updates on current issues and matters of interest related to GP Synergy’s training program including distribution of placements in the region, stakeholder communication, Medicare Local developments and GP Synergy membership.
Sydney South/Southwest Regional Advisory Forum
The Sydney South/Southwest Regional Advisory Forum met in August 2011 and March 2012.
Members include representatives from member organisations located within, or spanning across, the South/Southwest Sydney region such as universities, Divisions of General Practice/Medicare Locals, National GP Supervisor Association (NGPSA), GP Registrars

17
Association (GPRA), the GP Synergy registrar liaison officer and CEO.
Members in attendance at meetings held in the 2011-2012 financial period included: Prof Teng Liaw – University of NSW (2), Dr Ashok Chalasani – Bankstown General Practice Division Inc (1), Dr Owen Brookes (1), Dr Alison Rose – St George Division of General Practice (2), Dr John Stanford (1), Prof Jennifer Reath – University of Western Sydney (1).
The advisory forum shared updates on current issues and matters of interest related to GP Synergy’s training program including distribution of placements in the region, IT platform upgrades, PGPPP program expansion, practice accreditation, Medicare Local developments and GP Synergy membership.
The group discussed the ongoing development and implementation of several local strategic initiatives occurring between GP Synergy and stakeholders within the region such as capacity development, expanding Aboriginal Medical Service placements, practice management engagement and outer-metropolitan classification in the Sydney Southwest area.
New England/Northwest Regional Advisory Forum
The New England/Northwest Regional Advisory Forum met in March 2012.
Members include representatives from member organisations located within, or spanning across, the New England/Northwest region such as universities, Divisions of General Practice/Medicare Locals, National GP Supervisor Association (NGPSA), GP Registrars Association (GPRA), the GP Synergy registrar liaison officer and CEO.
Members in attendance at the March 2012 meeting included: A/Prof Michelle Guppy (Chair) – University of New England, A/Prof Lyn Fragar – GP Synergy, Dr Roland Loeve – North West Slopes Division of General Practice, Dr Cheryl McIntyre – Evan St Surgery – Inverell, Lynn Saul – ACRRM, Mr John Oldfield – GP Synergy, Mr Pat Worthing – GP Synergy.
The advisory forum shared updates on current issues and matters of interest related to GP Synergy’s training program including distribution of placements in the region, Rural Generalist Program developments, stakeholder communication, Medicare Local developments, ACRRM fellowship pathway intake and GP Synergy membership.
“ Regional Advisory Forums are subcommittees of the GP Synergy Board and have been established to represent interested stakeholders within each regional node of GP Synergy.”

18
Chief Executive Officer report
GP Synergy Annual Report 2011-2012
For GP Synergy, 2012 marks a decade of active training. We are preparing for the next round of contract negotiations and expect to renew triennial contacts to deliver the Australian General Practice Training program over 2013-2015.
In preparation for the new contracting period with General Practice Education and Training Limited (GPET), GP Synergy has again been successful in its accreditation as a training provider. The feedback report from GPET notes the high calibre of our training and education program and its administration and governance. This is a reflection of the skills and commitment of our directors, medical education team, management and staff, who are all to be congratulated.
As part of our preparations for the new contract period we have undertaken an extensive review of our operations, policy and positioning. Stakeholder surveys and other forms of feedback have informed numerous policy and process changes and ‘how we do things’. These changes are aimed at providing more control and support for our registrars, supervisors and training practices. GP Synergy’s focus is on meeting the needs of our community through the equitable distribution of training activity and through more emphasis on quality management and improvement of the training programs and their administration.
A key initiative of this work has been to modify our term allocation policy and process in ways that will better meet the distribution needs of our region, and to provide registrars and training practices with more control and choice in determining where, and with whom, they train. Self-selection will occur over the latter part of 2012, and in 2013 we hope to report improved distribution and satisfaction as a result of these revised allocation processes.
We are delighted to report that our efforts to close the gap and expand placements in Aboriginal Medical Services (AMS) have been fruitful. For the first time we established active general practice placements across all accredited AMS facilities within our region. We have been working with our highly productive Aboriginal and Torres Strait Islander Health Sub-committee in the development of a Reconciliation Action Plan (RAP) and
related projects. I wish to acknowledge Val Dahlstrom, our Aboriginal Liaison Officer, and all the CEOs and practice managers of our AMS facilities within our region for their active involvement, goodwill and support to make this committee so successful. No doubt we will continue to strive forward in 2013.
This year we also launched the Dr Jeremy Bunker Outstanding Achievement Award in memory of the late Dr Jeremy Bunker who passed away in May 2011. This annual award is announced each November and recognises outstanding achievement by a GP Synergy registrar, supervisor, staff member or alumni member. I congratulate Dr Eloise Warren, the winner in November 2011 for her contribution to the development, and ongoing involvement, with an Indigenous Health Clinic in Bathurst NSW.
We have also initiated the General Practice Registrar Award and in November 2011 this was presented to Dr Vanessa Jones for the highest overall mark in the fellowship exams. We congratulate Vanessa for this exemplar result.
In closing I wish to acknowledge the directors, our management team, medical educators and staff for their contributions. Led by our highly experienced and skilled Chair, Dr Charlotte Hespe, our board of directors continually demonstrates the highest standards of governance in the oversight of GP Synergy. We have benefited greatly as a result.
I thank A/Prof. Rosa Canalese for her incredible work as Director of Training (DoT). Rosa has proven to be invaluable to this organisation and I have great regard for her work and as a person. Rosa leads a skilled medical education team and their combined efforts are evident in the quality of the training program and high calibre of doctors that it processes.
I wish to thank the whole management team; Kate Froggatt who manages our marketing, communications, and events; Dianne Hill and Pat Worthing who are our regional business managers and Pat in his capacity as chief financial officer; Dr Anne Eastwood for her deputy DoT role in support of Rosa and the training program, and Dr Graham Lee who heads up the Prevocational General Practice Placements Program (PGPPP).

19
To our highly valued and skilled administrative staff, I thank you sincerely for your efforts in 2011-2012. One of the most enjoyable aspects of working in GP Synergy is our team ethos and this is demonstrated by all on a daily basis. You make our workplace a productive and enjoyable environment.
And to all our training practice staff and supervisors, we thank you once again for such commitment and
dedication to the training program. You are the front line in general practice training and an extension of our business. We thank you for your efforts in 2011-2012 and look forward to another year working with you.
John Oldfield Chief Executive Officer
“ One of the most enjoyable aspects of working in GP Synergy is our team ethos and this is demonstrated by all on a daily basis.”
GP Synergy registrar

20
Director of Training report
GP Synergy Annual Report 2011-2012
Coming to the director of training position in July 2011, I knew that I was taking on a challenging role given that the second of two mergers that now make GP Synergy the largest RTP in NSW, had occurred not long beforehand. It was a welcome relief to know that the program was being capably managed by Acting Director of Training, Dr Linda Mann, and I thank Linda for taking on this position and for her assistance in transitioning me into the role.
I would also like to thank the team of medical educators for their warm welcome and wonderful support; they are an exceptionally dedicated and talented team who are an integral component to the delivery of the quality education and training program that has become a hallmark of training with GP Synergy.
The Medical Education (ME) team has seen some changes over the last 12 months, especially in New England/Northwest (NE/NW) region. We farwelled Dr Barb Moritz who led the NE/NW ME team through the mergers and built a strong regional education and training program that continues to thrive. We also saw the departure of medical educators Drs Russell King and Roland Loeve, both of whom continue to be involved with training through clinical teaching visits, educational delivery and GP supervisors. We welcomed to the fold Dr Maree Puxty who brings with her a wealth of experience as a GP educator and trainer.
We also welcomed Drs Catherine Casey and Kit Fonseka to the Sydney based ME team.
As our numbers in both the rural and general pathway continue to grow the delivery of a quality education and training program remains the focus of the ME team. Over the past 12 months we have been committed to reviewing the education program delivery across the entire region to ensure that there is consistency and that the GP registrar will gain a similar educational experience regardless of where they train in the region. We have started to implement more robust, standardised GP registrar assessment processes and a comprehensive evaluation process that is reviewed by the whole team on a regular basis with the aim of continuous improvement in our program delivery.
There has been a strong focus on engaging the ME team in more professional development and research activities and our strong presence at last year’s GPET conference through the delivery of presentations and workshops was testimony to this success. The ME team are regularly participating in the monthly journal club and it is anticipated that the upcoming year will see more of the team becoming research active. Our partnership with the University of New South Wales with the co-appointment of a joint research / medical education position continues with Dr Michael Tam, whose research in e-learning and evidence based medicine has resulted in successful presentations both locally and internationally.
The research focus also extends to our GP registrar cohort, with GP Synergy hosting the Academic GP Registrar Orientation Workshop in June 2012. At this workshop GP Synergy GP registrar Dr Darshana Dave presented her experience, having just completed an academic GP term to a group of novice GP registrar researchers. The academic GP posts continue to be popular with GP registrars with increasing interest being seen each term. The planned appointment of a research officer is expected to provide the needed support across all these emerging and developing research areas for the organisation.
Another welcome appointment is Dr Graham Lee in the director of prevocational education and training role. Graham commenced this position in January 2012 in addition to his medical educator role. He has ‘hit the ground running’ and along with the PGPPP team has taken this program from strength to strength, with increasing trainee numbers and high levels of satisfaction with the training experience being a consistent feature of the feedback surveys. We anticipate that this program will continue to grow and become a key component of training with GP Synergy.
A major undertaking in the second term of 2012 was the implementation of the new practice allocation system. The move away from direct placement to allowing GP registrars and practices more flexibility in the timing and location of their training has resulted in a more equitable distribution of GP registrars across the

21
entire GP Synergy region and enabled us to increase our training capacity. Not surprisingly there has been a huge learning curve for all involved in this process, but overall it has been seen as positive move forward.
On a final note, it has been my pleasure to host a number of international visitors at GP Synergy. We have had visits from the Ministry of health in China and primary care clinicians from both India and Vietnam.
The main focus of these visits was to improve the training of primary care clinicians in their countries. They were very interested in how we support and deliver GP training and the role of GPs in the delivery of primary care and public health programs in Australia.
Rosa Canalese Director of Training
“ Over the past 12 months we have been committed to reviewing the registrar education program delivery across the entire region to ensure that there is consistency...regardless of where they train in the region.”
GP Synergy registrar

22
Director of Prevocational Education and Training report
GP Synergy Annual Report 2011-2012
2012 marks the second year of GP Synergy delivering the Prevocational General Practice Placements Program (PGPPP). The program had a strong start under the previous leadership of Drs Jeremy Bunker and Linda Mann, and 2012 has seen the program expanding and establishing itself as an important part of GP Synergy’s vertically integrated approach, supporting general practice as a valuable career path for medical students, prevocational doctors, and registrars. GP Synergy’s PGPPP is a large training program that covers all our training regions, and supports junior doctors from 10 hospital networks.
Total yearly PGPPP junior doctor participants have risen from 45 in 2011, to 64 in 2012, with 85-100 projected for 2013. Our training practices in the same period have doubled from 10 to 20, with a wide diversity of practice styles across our training regions, including rural and regional practices, an academic GP unit, and smaller doctor owned surgeries, to larger multi-site corporate run medical centres. Such a variety of practice styles allow GP Synergy to offer clinical exposure to the whole range of general practice medicine. Feedback from junior doctors has shown high levels of satisfaction, not only helping many consider or reconsider general practice as a career, but also appreciate the important role of primary health care. Above all, junior doctors have reported how they have thoroughly enjoyed the range and variety of patient presentations, often debunking commonly held myths that general practice is just about ‘coughs and colds’.
Whilst the in-practice clinical experience is the mainstay of PGPPP training, GP Synergy continues to develop and expand a comprehensive education program that supports and complements the clinical exposure. We continue to deliver an extensive pre-term commencement and term orientation program, access to registrar day release workshops and end of term wrap-up. 2012 has also seen the introduction of two PGPPP specific workshops per term delivered via videoconference that allows our junior doctors to participate in case presentations, sharing the variety of clinical experience across our regions.
To facilitate this education activity, each PGPPP training practice has been set up with a high definition VC240 videoconferencing unit. Future education planning includes developing a weekly online module for PGPPP junior doctors. In addition, GP Synergy will look to further expand a community visits program to allow junior doctors to visit allied health and Aboriginal Medical Services to further promote the team based approach to general practice medicine.
Other program developments in 2012 include:
• Introduction of PGPPP specific supervisor workshops.
• “Meet and Greet” series, that enabled feeder hospital staff to visit their aligned training practices.
• Updated practice manual
• Quarterly newsletter
• Participation in NSW RTP marketing events at participating hospital networks
• New promotional brochures
2012 has also seen some new staffing changes with GP Synergy’s PGPPP team: Dr Graham Lee joined the team as the new DPET in January 2012 and continues to be a medical educator for the registrar training program; Jani Mal was promoted to PGPPP program manager; Lexi Kyle moved from GP Synergy events and marketing to take up the PGPPP support officer role; and Lucy Adams added PGPPP rural practice support to her current administrative portfolio.
GP Synergy is well placed to continue delivering a high quality PGPPP experience.
Dr Graham Lee Director of Prevocational Education and Training

23
Director of Prevocational Education and Training report
Dr Michelle Thurston during her PGPPP term with supervisor Dr Liz Marles
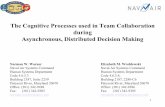
GP Synergy 2012 PGPPP network
NETWORK HOSPITALS IN NETWORK TRAINING PRACTICES
1 Royal Prince Alfred, Balmain and Dubbo Hospitals Hyde Park Medical
2 Bankstown, Campbelltown and Bowral Hospitals AllCare Carnes Hill, Hammondville and Wattlegrove. General Practice for Children and Young Families.
3 Concord, Canterbury and Broken Hill hospitals Excel Medical
4 Liverpool, Fairfield and Tweed Hospitals Total Care Cabramatta
5 Royal North Shore, Ryde, Port Macquarie and Greenwich Hospitals
Cremorne Family Medical Centre, Strathfield Family Medical Centre.
6 Hornsby, Manly and Mona Vale Hospitals Hornsby GP Unit
8 St George, Sutherland and Griffith Hospitals Picton Family Medical Practice
9 Prince of Wales and Lismore Hospitals UNSW Health Service
10 St Vincents and Wagga Wagga Hospitals Kings Cross Traveller’s Clinic
12 Tamworth, Armidale and John Hunter Hospitals Northwest Health Tamworth, Evans Street Surgery Inverell.

24
GP Synergy Annual Report 2011-2012
GP Synergy’s staff’s expertise and dedication underpin our organisation’s success.
At the end of the 2011-2012 financial year just under 50 staff were employed by GP Synergy across our four office locations.
Staff changes
2011-2012 saw some significant staff changes, such as the appointment of A/Prof Rosa Canalese in the Director of Training (DoT) role, formerly held by the
respected Dr Jeremy Bunker who passed away from cancer in May 2011. With over 18 years of medical education experience, Rosa has brought to the role a wealth of knowledge and enthusiasm. Whilst her most recent position prior to her GP Synergy appointment was heading the Medical Education Unit as Associate Dean for Teaching and Learning at the University of Notre Dame, her previous senior medical educator roles with the RACGP training program and the Institute of General Practice Education enabled her to hit the ground running, with a solid understanding of the intricacies of the GP training environment.
Staff
Members of the GP Synergy medical education team

25
In line with PGPPP program growth, the PGPPP department was also expanded to include the appointment of PGPPP support officer roles in Sydney and New England/Northwest, to support program. During the 2011-2012 period, GP Synergy medical educator Dr Graham Lee replaced Acting DoT and Acting Director of Prevocational Education & Training (DPET) Dr Mann in the DPET role. Graham has been instrumental in the leading his department in the expansion of training places and training capacity across our regions.
In 2011 Dr Michael Tam continued in the collaborative joint lecturer position between GP Synergy and the UNSW School of Public Health and Community Medicine. The two year position involves teaching in both the undergraduate medical program at UNSW and vocational education at GP Synergy. During his tenure Michael has developed an extensive online learning module on Evidence Based Medicine, and successfully submitted an abstract in conjunction with GP Synergy Medical Educator Dr Anne Eastwood to present at the highly acclaimed AMEE Conference in Leon, France on ‘The use of web 2.0 tools to build e-learning modules’.
Other medical education staff changes during the 2011-2012 period included the departure of New England/Northwest Regional Education Director, Dr Barb Moritz, and medical educators Drs Roland Loeve, Soheyl Aran and Russell King.
During the same period, we were joined by medical educators Dr Maree Puxty, Dr Catherine Casey, Dr Kit Foneska and return of Dr James Best.
Administrative changes included the appointment of a new accreditations & quality assurance officer, marketing & events coordinators and training coordinator. During this period a rural support officer, dedicated to providing pastoral and networking support for prevocational and vocational trainees in rural locations, was also appointed.
Staff networking and development
In addition to internal staff meetings within, and between, departments and offices, each year GP Synergy holds bi-annual staff meetings where all staff are invited to attend.
In 2011-2012, two company wide staff networking and development workshops were held - one in October 2011 and another in March 2011. Each workshop covers different themes, with the the focus of the first day on topical education and training issues, and the second day dedicated to professional development activities.
During the 2011-2012 financial year, two additional events were held for specifically for administrative staff.
At the first of these events, held in Liverpool in October, the focus was the development of an email etiquette guide for use by staff, and cultural skills training.
The second event, held in Armidale in April, examined customer service training issues and IT developments, as well as a familiarisation of the New England/Northwest region to build staff awareness.
In addition to these events, the GP Synergy medical education team hold monthly journal clubs as a form of professional development knowledge sharing.
Other key staff developments during this time included the development of a medical educator grading scale and staff involvement in several charitable fundraising activities such as the 100km Oxfam Trailwalk and Biggest Morning Tea.
Members of the GP Synergy administration team
“ GP Synergy’s staff’s expertise and dedication underpin our organisation’s success.”

GP Synergy supervisor Dr Vicki Howell with GP registrar Dr Amanda Johnson
26
GP Synergy Annual Report 2011-2012
Training practices
As of 30 June 2012, approximately 190 practices were accredited by GP Synergy to train vocational doctors with 15 of these accredited to train prevocational doctors.
Across our region, 163 practices of these practices were located in Sydney and 27 in New England/Northwest NSW.
Supervisor professional development program
To support supervisors in their education and training of GP registrars, GP Synergy continues to provide a comprehensive supervisor professional development program.
The program is built on a matrix of resources for GP supervisors which includes education designed to increase knowledge of the general practice curriculum and GP Synergy education program, as well as explore and promote methods of clinical teaching.
In the 2011-2012 period GP Synergy hosted several educational workshops for supervisors across our training regions.
A highlight of this program was the annual GP supervisor development weekend on ‘The art, science and technology of supervision’ which examined strategies to manage challenging patients, a back to basics science and practice of wellbeing session, and the utilization of current and emerging technologies in the teaching armamentarium.
Held on the NSW Central Coast, the workshop was attended by GP Synergy supervisors from both Sydney and New England/Northwest. Led by GP Synergy’s medical education team, the workshop featured a range of hands on practical sessions where supervisors could explore new concepts and acquire new skills.
The supervisor professional development program also included workshops held in each of our three regions in Chippendale, Liverpool and Armidale.
To enable supervisors to meet the requirement to attend a GP Synergy Clinical Teacher Training
Workshop, three of these events were held during the 2011-2012 period. The workshop cover fundamentals of teaching and continue to be highly evaluated by new and existing supervisors who appreciate the refresher and opportunity to engage in small group activities with their peers.
Teaching practice resource grant equipment
In 2011 GP Synergy made a successful submission for a teaching practice resource grant which saw training practices able to make application for a range of equipment including dermatoscope sets, diagnostic otoscopes, f/tip P/Oximeter – alarm and pulse; and spirometers.
Also included in the teaching practice resource grants were executive style videoconference endpoint systems.
These systems were gifted to all Level 1 teaching practices and featured the Scopia VC240 system enabling webinar conferencing (like illuminate) with all the benefits of a high definition executive video conference system. The systems can be used as a standalone endpoint or as an extension for a PC or laptop to provide webinar capabilities utilising the monitor, encoding software and high definition camera.
Registrar in-practice supervision satisfaction
In a study commissioned by GPET undertaken by Piazza Consulting in May 2012, community based GP registrars were asked to rate their level of satisfaction with the quality of teaching and advice provided by their supervisor. 95% of general pathway registrars surveyed were satisfied or highly satisfied, with 100% of rural pathway respondents satisfied or highly satisfied with the quality of teaching and advice.
Training practice support and development

27
“ As of 30 June 2012, approximately 190 practices were accredited by GP Synergy to train vocational doctors with 15 of these accredited to train prevocational doctors”

28
Supervisor feedback
In 2011 GP Synergy launched the inaugural supervisor feedback survey as one method to collect supervisors feedback about key areas of the training program and delivery. This included term placement processes, communication, professional development activities, support, IT and other areas.
The results of the 2011 survey were generally positive however it identified improvements were required to be made to GP Synergy’s online training management system GPRime. As a result of this feedback, the supervisors GPRime interface was given a make-over to help improve navigation and functionality for supervisors as an interim measure until the second version of the platform is released. As part of these improvements, the practice profile page was also enhanced to provide practices a more effective tool to promote their training facility to registrars.
Feedback collected in the survey was also used to form the development of the GP supervisor professional development program and to make improvements in communication and other areas of the organisation.
The feedback survey will form an annual feedback collection tool.
Practice manager engagement
To provide added support and improved advocacy for practice managers in training facilities, in May 2012 GP Synergy appointed Ralph Belshaw in a newly created Practice Manager Liaison Officer position. In this role Ralph is responsible for advocating for the individual and collective needs of practice managers within GP Synergy’s training network; informing policy, systems and process development to enhance practice environment for the purposes of general practice training; and establishing professional development forums that are relevant to the practice manager’s involvement in general practice training, including their interface with GP Synergy’s business systems and processes.
GP Synergy also continued its practice manager workshop program as a vehicle for improving communication between practices and training requirements, holding two events in the 2011-2012 period. This included a workshop in Liverpool focusing on cross cultural training and a workshop in Tamworth where the focus was on administrative processes and identifying ways to improving communication between the organisation and training practices.
GP Synergy Annual Report 2011-2012
Training practice support and development (continued)
GP Synergy registrar Dr Nancy Yiin with GP supervisor Dr Martin Danke
Supervisors at GP Synergy’s Clinical Teacher Training Workshop

29

30
Training competent and confident registrars
GP Synergy Annual Report 2011-2012
Training capacity
GP Synergy is the second largest provider of vocational general practice training in Australia. For the 2012 Australian General Practice Training (AGPT) program, GP Synergy offered a total of 114 training places – 26 rural pathway and 88 general pathway.
As at 30 June 2012, over 300 registrars were actively training with GP Synergy.
Fellowship outcomes
In the 2011-2012 financial year 70 GP Synergy registrars successfully reached their Royal Australian College of General Practice (RACGP) fellowship aspirations.
To assist registrars prepare for these exams GP Synergy continued to offer its popular exam preparation series, featuring a combination of written and clinical interactive workshops. After the success of the 2011 pilot, an online exam component was added as a core component of this exam preparation activity, improving access for registrars in rural locations.
GP Synergy continues to offer registrars training in the rural pathway opportunities to train towards Fellowship of the Australian College of Rural and Remote Medicine (FACRRM) with two registrars currently enrolled in this program.
Fellowship award achievements
For the fourth consecutive year a GP Synergy registrar was awarded the Royal Australian College of General Practitioners (RACGP) Tony Buhagiar Memorial Medal. This medal is awarded to the exam candidate who passed all three RACGP fellowship examinations on their first attempt and received the highest clinical fellowship exam score in the state.
The recipient of this award for the 2012.1 term was GP Synergy GP registrar, Dr Aishah Moore.
Past award winners have included former GP Synergy registrars Dr Cheryl Cheong in 2011, Dr Julia Menzies in 2010 and Dr John Cass-Verco in 2009.
Dr Jeremy Bunker and GP registrar excellence awards
In 2011, two new awards were established.
The first award was developed in recognition of the contribution made to GP training and general practice by GP Synergy’s inaugural Director of Training, the late Dr Jeremy Bunker. The Dr Jeremy Bunker Outstanding Achievement Award identifies and acknowledges an outstanding achievement of staff, supervisors, registrars or former trainees who have completed general practice training within the past three years.
The 2011 recipient of this award was GP registrar Dr Eloise Warren, for her development and ongoing involvement in an Indigenous health clinic in Bathurst.
The second award was the Outstanding Academic Achievement by a Registrar Award. This award recognizes the achievements of the GP Synergy registrar who completed the Royal Australian College of General Practice (RACGP) fellowship exam with the highest overall score each calendar year.
In 2011, the recipient of this award was general pathway registrar Dr Vanessa Jones.
Recently fellowed GP Synergy GP registrar, Dr John Barry

31
“ GP Synergy is the second largest provider of vocational general practice training in Australia. As at 30 June 2012, over 300 registrars were actively training with GP Synergy.”
Remeek Abdulla
Gavin Alison
Alphonsus Amalakumar
Nada Andric
John Barry
Ai Bui
Hera Chan
Vincent Chang
Pei Chen
Cheryl Cheong
Tania Chin
Simone Craig
Amanda Crew
Carla Croaker
Mira Drakos
Sabina Dulic
Penelope Elix
Alexandra Fletcher
Andrew Habig
Katherine Hogg
Viviene Hung
Amal Ibrahim
Gillian Jones
Kate Kelso
Aradhna Khanna
James Koutis
Ying Lan
Khac Le
Rebecca Lee
Renate Liong
Richard Loizou
Kenneth Mackun
Anand Mahadev
Vindan Manomohan
Crystal McKeough
Farah Meher-Homji
Nafi Musa
Hanady Nasreddin
Andrew Newman
Jenny Nguyen-Lam
Julian Northover
Krishna Perera
Nam Pham
Charles Piao
Olga Poutalina
Edwina Pritchard
Matthew Rathjen
Anusha Ravendendran
Denisa Robinson
Shannon Saad
Shanah Salter
Joseph Santos
Sanjala Sharma
Shereena Sinnayah
Ancuta Slimovschi
Cynthia Spiers
Krishna Sura
Myra Tan
Akito Tomita
Steven Tongson
Belinda Tosi
Zhanna Tsukanova
Kylie Vuong
Yvonne Wang
Elly Warren
Victoria Wilkinson
Adrian Wong
Kit Wong
Wicky Wong
Chih-Yueh Yang
GP Synergy Fellows 2011-2012

32
GP Synergy Annual Report 2011-2012
GP registrar education
During the 2011-2012 period GP Synergy delivered 72 workshops for its registrars, providing a variety of learning opportunities across all stages of training.
General pathway registrars in GPT1&2 terms attend educational activities in the GP Synergy office closest to their practice location (i.e. either Chippendale or Liverpool) to ensure relationships with local healthcare services and networks are maximised.
Rural pathway registrars attend most educational events within the New England/Northwest region with the exception of joint pathway educational activities such as the Fusion workshop, held in Sydney.
The GP Synergy registrar education program continues to be highly valued and evaluated by its participants. In the 2012 registrar satisfaction survey commissioned by GPET, undertaken by Piazza Consulting, 98% of community based registrars were either highly satisfied or satisfied with the quality of educational content, presenters, suitability and diversity of educational workshops delivered by GP Synergy.
The program is reviewed annually and mapped against college curriculums. Feedback is collected regularly from participants to ensure relevance and quality standards continue to be achieved.
Highlights of the 2011-2012 program included the combined GP Synergy, General Practice Training – valley to coast & North Coast GP Training Fusion Workshop featuring three days of lectures from specialists and other clinicians, and a fourth hands on practical skills day with interactive sessions on musculo-skeletal medicine, surgical skills, wound management, plastering and implanon insertion,
The Pre-GPT1 Assessment, introduced initially only for rural pathway registrars and then extended to general pathway registrars, continues to be highly regarded by registrars. The assessment allows registrars to reflect on the differences in the consultation styles of the hospital and GP environment, and target their preparation prior to entering a GP term.
Registrar Medical Educator
To foster interest in medical education in general practice, GP Synergy has supported Registrar Medical Education positions for many years.
During the 2011-2012 financial year, this position was held by rural pathway GP registrar Dr Jenny Morrison, who developed an education program for rural pathway registrars in hospital based terms.
To meet the educational needs of hospital based registrars training in hospitals across Australia, a case based program was developed, distributed monthly electronically to registrars for review by the Registrar Medical Educator.
Online education resources
During 2011-2012 a number of online educational resources were made available to registrars.
This included the upgrade of GP Synergy’s written pre-exam workshop into online modules by Dr Vanessa Moran and establishment of a Facebook group where registrars can access weekly cases and interactive dialogue with peers.
An ‘Aged Care’ and ‘Evidence Based Medicine’ online learning module were also added to the registrar education program, and registrars, supervisors and PGPPP doctors were also provided access to the online Therapeutic Guidelines and Australian Medicines Handbook.
Training competent and confident registrars (continued)

33
Training competent and confident registrars (continued)
ADF GP Synergy registrar Dr Joel Hissink on deployment in Pakistan (Photo courtesy of the Australian Defence Force)
“ The GP Synergy registrar education program continues to be highly valued and evaluated by its participants.”
ADF registrars
GP Synergy remains one of the largest trainers of Australian Defence Force (ADF) GP registrars, training 18 ADF GP registrars in various stages of training during the 2011-2012 period.
As these registrars have unique training requirements, GP Synergy has developed and adopted a multidisciplinary management model to oversee the training of this group.
Interest in this model has been shown by other RTPs such as Northern Territory GP Training (NTGPE) and
Central and Southern Queensland Training Consortium (CSQTC) who invited the staff member responsible for overseeing management of this group, Felicity Gemmell-Smith to present and share our approach with their staff.
Felicity also presented the model at the National GPET conference and the Australian Military Medicine Association conference.
Through the efforts of Felicity and GP Synergy DoT, Rosa Canalese, strong and positive working relationships with the ADF and RACGP have been developed to the benefit of the ADF registrars training in our region.

34
Procedural training
GP Synergy continues to be seen as a leading provider of procedural skills training, offering places under the NSW Rural GP Procedural Training Program and more recently, the NSW Rural Generalist Training Program.
GP Synergy maintains close relationships with Tamworth and Armidale Hospitals to offer training in the areas of anaesthesia, obstetrics and gynaecology, emergency medicine and mental health.
With the launch of the NSW Rural Generalist Training Program in the first half of 2012, GP Synergy has and continues to work closely with HETI, the Hunter New England Local Health District and General Practice Training valley to coast, to ensure that both programs flourish in our regions.
In the 2011-2012 period, GP registrars filled posts in anaesthesia, obstetrics, emergency medicine and mental health, with anaesthesia and obstetrics posts filled until the end of 2013.
In 2012 the Emergency Department of Tamworth Regional Referral Hospital has been able to offer the Australasian College of Emergency Medicine (ACEM) Certification in Emergency Medicine to our current emergency medicine procedural trainee.
Rural support for rural registrars
In 2011 GP Synergy appointed a full-time rural support officer dedicated to providing practical on the ground and pastoral assistance to registrars during their rural training. This includes relocation assistance, development of social and professional support networks, counselling and pastoral support, etc.
Registrar Liaison Officer
Between 2011-2012, GP Synergy registrar Dr Shamini Ramoo was the Registrar Liaison Officer (RLO) for GP Synergy registrars. In this role, she was responsible for advocating on behalf of GP Synergy registrars and representing them at the RTP management level.
Alumni program
Forming part of GP Synergy’s succession planning strategy, the GP Synergy Alumni Program continued in 2011-2012 with former registrars invited to attend a number of educational events. The GP Synergy alumni website continues to be used by practices as a promotional platform to advertise general practitioner vacancies and businesses for sale.
GP Synergy Annual Report 2011-2012
Training competent and confident registrars (continued)
Dr Sascha Sarahov during his anaesthesia advanced rural skills placement in Armidale

3535

36
GP Synergy recognises that too many Aboriginal people experience unacceptable levels of disadvantage.
Our goal is to develop mutually beneficial relationships with Aboriginals by building a culturally diverse health workforce and by raising the awareness of all our stakeholders about the unique cultural history that Aboriginal people enjoy, particularly in our regions.
During the 2011-2012 financial period, GP Synergy employed several different strategies towards reaching this goal.
Remote AMS supervision model
The major impediment to registrars working in the AMS system is the lack of supervision available. In May of this year both GP Synergy and the AH&MRC indicated an interest in setting up a system of remote supervision.
While the two programs had the same aims and objectives, the methods to achieve them were entirely different. One hoped to provide the services through a regional roaming program where one person was available to provide the supervision and the other provided the services through either local GP or within local driving distances.
Pius X Aboriginal Medical Service (Moree), Armajun Aboriginal Medical Service (Inverell) and Tamworth Aboriginal Medical Service have all become actively involved in the remote supervision program using either local doctors or doctors from nearby towns.
For Pius X and Armajun AMS, this model enabled registrars to be able to train in these facilities for the first time.
Aboriginal and Torres Strait Islander health curriculum working group
As part of the Aboriginal & Torres Strait Islander Health Committee board sub-committee a working group has been established to review and map the RACGP & ACRRM curriculums against the GP Synergy education program.
Registrar education
Aboriginal health continues to be a core part of the registrar education program with sessions collaboratively delivered with local Aboriginal Medical Service staff and community. Where possible, these sessions are held at local AMS facilities within our regions.
GP Synergy Annual Report 2011-2012
Aboriginal health
Armajun Aboriginal Medical Service

3737

38
GP Synergy Annual Report 2011-2012
Expanding the general practice profession
Intake
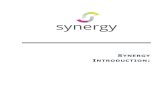
For the 2012 training year, GP Synergy offered 26 rural pathway training places and 88 general pathway training places. This was an increase from 20 rural pathway training places and 83 general pathway training places available in 2011.
In line with the increases in training places, GP Synergy has continued to increase the number of training places filled, with 24 of the 26 training places filled in the rural pathway and all of the 88 general pathway training filled in 2012.
In the rural pathway in particular, these figures represent a significant increase from 2009 when the number of training places filled was 10.
Nationally, the challenge remains attracting Australian Medical Graduates (AMGs) into the rural pathway. For the 2012 program, 73% of AMG applicants selecting general pathway, compared with only 27% selecting rural pathway (a decrease from 36% in 2011).
Selection
In 2011, the selection process for the 2012 AGPT program changed to a nationally consistent format whereby applicants are required to attend an assessment centre and participate in Multiple Mini Interviews (MMIs) and a written Situational Judgement Test (SJT).
GP Synergy played an instrumental role in the collaborative running of these centres with the other five NSW RTPs.
Promotion and engagement
To encourage and foster an interest in general practice as a career, and to undertake GP training within our regions, GP Synergy has a comprehensive marketing activity plan to ensure exposure across a range of target audiences such as medical students and prevocational doctors.
This program includes working closely with GP Student Network (GPSN) clubs and medical societies at universities located within our boundaries; meaningful engagement with prevocational doctors through programs such as the GP registrar/prevocational doctor education program and PGPPP; as well as participation in the NSW RTP marketing collaborative.
In 2011-2012 GP Synergy’s print marketing communications material were updated and refreshed, featuring images and testimonials from real registrars and supervisors currently training and teaching within our regions. A specific rural pathway training guide was developed, in addition to a PGPPP and medical student brochure.
Improving the look and content of our communication was a key focus of 2011-2012. These improvements included an refresh to our promotional print publications and internal and external communications. A staff ‘Netiquette Guide’ was developed with input from all staff to guide email correspondence content and style; a comprehensive communications strategy was developed to accompany the roll-out of the new term placement process; and the GP Synergy Applicant Pack for prospective applicants was also updated.
0
5
10
15
20
25
30
2009 Program(NEATS)
Training places
Places filled
Linear (Places filled)
2010 Program(GP Synergy)
2011 Program(GP Synergy)
2012 Program(GP Synergy)
0102030405060708090
100
2009 Program(NSIGPET)
Training places
Places filled
Linear (Places filled)
2010 Program(GP Synergy)
2011 Program(GP Synergy +
IGPE)
2012 Program(GP Synergy)
GP Synergy rural pathway training places and number filled
GP Synergy general pathway training places and number filled

FinancialsDirector’s Report 40
Declaration of Auditor Independence to the Directors of GP Synergy Ltd 44
Independent Audit Report to the Members of GP Synergy Ltd 45
Directors Declaration 47
Statement of Financial Position as at 30 June 2012 48
Statement of Comprehensive Income for the year ended 30 June 2012 49
Statement of Changes in Equity for the year ended 30 June 2012 50
Statement of Cash Flows for the year ended 30 June 2012 51
Notes to the Financial Statements for the year ended 30 June 2012 52
39
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
Directors’ Report
The directors present their report together with the financial report of GP Synergy Limited for the year ended 30 June 2012 and the auditors’ report thereon.
1. Directors
The directors at any time during or since the financial year were as follows:
NAME PERIOD AS DIRECTOR
Dr C Hespe 27 December 2001-present
Dr J Keh 8 November 2011-present
Dr I Kamerman 28 October 2011-present
Dr N Shadbolt 8 November 2011-present
Dr J Korner 28 February 2007-present
Prof J Reath 29 October 2010-present
A/Prof M Guppy 2 January 2009-present
Dr H Nespolon 31 October 2007-28 October 2011
A/Prof L Fragar 2 January 2009-present
Prof T Liaw 1 January 2010-present
Dr O Brookes 1 January 2010-28 October 2011
Dr N Andric 29 October 2010-28 October 2011
2. Principal Activities during the Year
The principal activity of the company during the financial year was to promote and deliver general practice education and training.
The company is economically dependent on Government funding to carry out its principal activity.
The net surplus for the year was $Nil (2011: $48,896)
There was no significant change in the nature of business activity during the financial year.
3. Description of Short and Long-term Objectives
Promote and deliver integrated general practice education and training.
40

4. Strategy for Achieving Objectives
Continue to deliver general practice education and training within the terms of the Australian General Practice Training contract. The program will be integrated to include pre-vocational training.
5. How Principal Activities Contributed to Achieving these Objectives
By continued compliance with the requirements of the AGPT contract for general practice education and training.
6. How Performance is Measured
AGPT measures company performance under terms of contract specific performance indicators. GP Synergy is obliged to report against the performance indicators.
The company has established internal performance indicators under its quality framework and strategic plans. It periodically audits risk and tracks its performance against these indicators.
7. Members Liabilities
21 Members limited to $10 per member.
8. Directors’ Meetings
During the financial year, the attendances of the directors were as follows:
NAME ATTENDED ELIGIBLE
Dr C Hespe 8 8
Dr N Shadbolt 4 4
Dr J Keh 5 5
Dr J Korner 7 8
A/Prof M Guppy 8 8
Dr H Nespolon 1 2
A/Prof L Fragar 7 8
Dr I Kamerman 5 6
Prof T Liaw 7 8
Dr O Brookes 2 2
Prof J Reath 7 8
Dr N Andric 2 2
41

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
42
DIRECTORS’ REPORT (continued)
Sub-committees of the Board
During the financial year, the attendances of the directors at sub-committees were as follows:
FINANCE AND AUDIT COMMITTEE
NAME ATTENDED ELIGIBLE
Dr C Hespe 8 11
A/Prof L Fragar 11 11
Dr N Andric 3 4
Dr J Korner 9 11
Dr H Nespolon 4 4
Dr J Keh 3 7
Dr N Shadbolt 4 7
NOMINATIONS AND CONSTITUTIONAL REVIEW COMMITTEE
NAME ATTENDED ELIGIBLE
Dr C Hespe 3 3
A/Prof M Guppy 1 1
Dr O Brookes 2 2
Dr J Korner 1 1
Dr H Nespolon 1 2
Dr I Kamerman 0 1
EDUCATION COMMITTEE
NAME ATTENDED ELIGIBLE
A/Prof M Guppy 2 3
Prof T Liaw 3 3
Prof J Reath 2 3

43
ABORIGINAL AND TORRES STRAIT ISLANDER HEALTH COMMITTEE
NAME ATTENDED ELIGIBLE
Prof T Liaw 1 3
Prof J Reath 2 3
REGIONAL ADVISORY COUNCIL – SYDNEY CENTRAL
NAME ATTENDED ELIGIBLE
Dr J Korner 1 1
REGIONAL ADVISORY COUNCIL – NEW ENGLAND/NORTH WEST
NAME ATTENDED ELIGIBLE
A/Prof L Fragar 1 1
REGIONAL ADVISORY COUNCIL – SOUTH/SOUTH WEST
NAME ATTENDED ELIGIBLE
Prof T Liaw 1 1
9 Lead Auditor’s Independence Declaration
The lead auditor’s independence is set out on the next page and forms part of the directors’ report for the financial year ended 30 June 2012.
Signed in accordance with a resolution of the directors:
DIRECTOR:
DIRECTOR:
Sydney

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
44
Declaration of Auditor Independence to the Directors of GP Synergy Limited
As lead auditor of GP Synergy Limited for the year ended 30 June 2012, I declare that, to the best of my knowledge and belief, there have been no contraventions of:
– the auditor independence requirements of the Corporations Act 2001 in relation to the audit; and
– any applicable code of professional conduct in relation to the audit.
This declaration is in respect of GP Synergy Limited during the period.
KS Black & Co Chartered Accountants
FAIZAL AJMAT
Partner
Sydney

45
Independent Audit Report to the Members of GP Synergy Limited
Report of the financial report
We have audited the accompanying financial report of GP Synergy Limited (the “company”) which comprises the statement of financial position as at 30 June 2012, and the statement of comprehensive income, statement of changes in equity, and statement of cash flows for the year ended on that date, a summary of significant accounting policies, other explanatory notes and the directors’ declaration of the company.
Directors’ Responsibility for the Financial ReportThe directors of the company are responsible for the preparation and fair presentation of the financial report in accordance with Australian Accounting Standards (including the Australian Accounting Interpretations) and the Corporations Act 2001. This responsibility includes establishing and maintaining internal control relevant to the preparation and fair presentation of the financial report that is free from material misstatement, whether due to fraud or error, selecting and applying appropriate accounting policies; and making accounting estimates that are reasonable in the circumstances.
Auditors’ ResponsibilityOur responsibility is to express an opinion on the financial report based on our audit. We conducted our audit in accordance with Australian Auditing Standards. These Auditing Standards require that we comply with relevant ethical requirements relating the audit engagements and plan and perform the audit to obtain reasonable assurance whether the financial report is free from material misstatement.
An audit involves performing procedures to obtain audit evidence about the amounts and disclosures in the financial report. The procedures selected depend on the auditors’ judgement, including the assessment of the risks of material misstatement of the financial report, whether due to fraud or error. In making those risk assessments, the auditor considers internal control relevant to the company’s preparation and fair presentation to the financial report in order to design audit procedures that are appropriate in the circumstances, but not for the purpose of expressing an opinion on the effectiveness of the company’s internal control. An audit also includes evaluating the appropriateness of accounting policies used and the reasonableness of accounting estimates made by the directors, as well as evaluating the overall presentation of the financial report.
We believe the audit evidence we have obtained is sufficient and appropriate to provide a basis for our audit opinion.
Independence
In conducting our audit, we have complied with the independence requirements of the Corporations Act 2001. We confirm that the independence declaration required by the Corporations Act 2001 would be in the same terms if it had been given to the directors at the time this auditors’ report was made.

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
46
INDEPENDENT AUDIT REPORT TO THE MEMBERS OF GP SYNERGY LIMITED (continued)
Audit Opinion
In our opinion, the financial report of GP Synergy Limited is in accordance with the Corporations Act 2001, including:
(i) giving a true and fair view of the company’s financial position as at 30 June 2012 and of its performance for the year ended on that date; and
(ii) complying with Australian Accounting Standards (including the Australian Accounting Interpretations) and the Corporations Regulations 2001.
KS Black & Co
Chartered Accountants
FAIZAL AJMAT
Partner
Sydney

47
Directors’ Declaration
In the opinion of the directors of GP Synergy Limited:
a. the financial statements and notes, as set out on the following pages are in accordance with the Corporations Act 2001, including:
(i) giving a true and fair view of the financial position of the company as at 30 June 2012 and of its performance for the financial year ended on that date; and
(ii) complying with Australian Accounting Standards and the Corporations Regulations 2001; and
b. there are reasonable grounds to believe that the company will be able to pay its debts as and when they become due and payable.
Signed in accordance with a resolution of the directors:
DIRECTOR: DIRECTOR:
Sydney

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
48
Statement of Financial Position as at 30 June 2012
NOTE 2012 $
2011 $
CURRENT ASSETS
Cash and cash equivalents 4 5,720,068 6,004,470
Trade and other receivables 5 137,415 257,617
Other assets 6 217,741 202,007
TOTAL CURRENT ASSETS 6,075,224 6,464,094
NON-CURRENT ASSETS
Property, Plant & Equipment 7 1,415,959 1,501,740
TOTAL NON-CURRENT ASSETS 1,415,959 1,501,740
TOTAL ASSETS 7,491,183 7,965,834
CURRENT LIABILITIES
Payables 8 1,224,665 1,137,445
Unearned revenue 9 5,779,170 6,408,417
Provisions 10 297,028 217,858
TOTAL CURRENT LIABILITIES 7,300,864 7,763,720
NON-CURRENT LIABILITIES
Provisions 10 74,197 85,991
TOTAL NON-CURRENT LIABILITIES 74,197 85,991
TOTAL LIABILITIES 7,375,060 7,849,711
NET ASSETS 116,123 116,123
SHAREHOLDERS’ EQUITY
Issued Capital 170 170
Retained Profits 115,953 115,953
116,123 116,123
These financial statements must be read in conjunction with the accompanying notes

49
Statement of Comprehensive Income for the year ended 30 June 2012
NOTE 2012 $
2011 $
REVENUE * 2 14,513,340*** 12,053,704**
Employee benefits expense 3,439,408*** 2,855,417**
Depreciation 3(a) 296,716*** 237,732**
Practice reimbursements 1,970,382*** 1,639,779**
Registrars expense 1,784,560*** 1,071,842**
Supervisors costs 778,388*** 101,259**
Teaching allowance 1,407,987*** 1,263,479**
Board expenses 129,070*** 177,076**
Consultants and contractors 521,848*** 551,795**
Insurance 3(b) 81,637*** 86,110**
Rent 3(a) 372,815*** 303,152**
Administration Fee 3(d) 644,316*** 280,488**
(Gain)/Loss on disposal of non current assets 5,152*** (1,361)**
Other expenses 3(c) 3,081,061*** 3,438,067**
14,513,340*** 12,004,808**
Surplus before income tax expense –*** 48,896**
Income tax expense –*** –**
SURPLUS FOR THE YEAR –*** 48,896**
* Revenue includes income recognised during the period for PGPPP totalling $4,488,655; income recognised in relation to Aboriginal and Torres Strait Islander grants totalling $663,287 and overall increased training activity.
** $48,896 was recognised as surplus arising from cessation of the NSW Health One Programme.
*** Includes purchases for equipment grants for training practices.
These financial statements must be read in conjunction with the accompanying notes

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
50
Statement of Changes in Equity for the year ended 30 June 2012
2012 $
2011 $
Total Equity at the beginning of the financial year 116,123 67,227
SURPLUS FOR THE YEAR – 48,896
116,123 116,123
These financial statements must be read in conjunction with the accompanying notes

51
Statement of Cash Flows for the year ended 30 June 2012
NOTE 2012 $
2011 $
CASH FLOWS FROM OPERATING ACTIVITIES
Cash receipts from government and other sources 15,534,665 12,943,398
Interest received 390,917 286,978
Cash paid to suppliers and employees (15,993,600) (11,042,620)
Net Cash (Used in)/Provided by Operating activities 14(b) (68,018) 2,187,756
Cash Flows from Investing Activities
Payment for plant and equipment (216,384) (660,973)
Net Cash Used in Investing Activities (216,384) (660,973)
NET (DECREASE)/INCREASE IN CASH AND CASH EQUIVALENTS (284,402) 1,526,783
Cash and Cash Equivalents at the beginning of the Financial Year 6,004,470 4,477,687
CASH AND CASH EQUIVALENTS AT THE END OF THE FINANCIAL YEAR 14(a) 5,720,068 6,004,470
These financial statements must be read in conjunction with the accompanying notes

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
52
Notes to the Financial Statements for the year ended 30 June 2012
1. SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
The principal accounting policies adopted in the preparation of the financial report are set out below. These policies have been consistently applied to all the years presented, unless otherwise stated.
(a) Basis of Preparation This general purpose financial report has been prepared in accordance with Australian Accounting Standards
(including Australian Accounting Interpretations) adopted by the Australian Accounting Standards Board and the Corporations Act 2001.
The financial report has been prepared on an accruals basis and is based on historical costs.
(b) Revenue Recognition Revenue is measured at the fair value of the consideration received or receivable.
Interest Revenue
Interest revenue is recognised as it accrues.
Other Income Income from other sources is recognised when the income in respect of other products or services provided is
receivable.
(c) Government Grants Grants from the government are recognised at their fair value where there is a reasonable assurance that the
grant will be received and the Company will comply with all attached conditions.
Government grants are deferred and recognised in the Statement of Comprehensive Income over the period necessary to match them with the costs that they are intended to compensate.
(d) Goods and services tax Revenues, expenses and assets are recognised net of the amount of goods and services tax (GST), except where
the amount of GST incurred is not recoverable from the Australian Taxation Office (ATO). In these circumstances, the GST is recognised as part of the cost of acquisition of the asset or as part of an item of the expense.
The net amount of GST recoverable from or payable to, the ATO is included as a current asset or liability in the Statement of Financial Position.
Cash flows are included in the Statement of Cash Flows on a gross basis. The GST components of cash flows arising from investing and financing activities which are recoverable from or payable to, the ATO are classified as operating cash flows.
(e) Income Tax The income of the company is exempt from income tax under the provisions of the Income Tax Assessment Act.
f) Impairment of assets Assets that are subject to depreciation are reviewed for impairment whenever events or changes in circumstances
indicate that the carrying amount may not be recoverable. An impairment loss is recognised for the amount by which the asset’s carrying amount exceeds its recoverable amount. The recoverable amount is the higher of an asset’s fair value less costs to sell and depreciated replacement cost. For purposes of assessing impairment, assets are grouped at the lowest levels for which there are separately identifiable cash flows (cash generating units).

53
(g) Trade receivables Trade receivables are recognised initially at fair value and subsequently measured at amortised cost, less provision
for doubtful debts. Trade receivables are due for settlement no more than 60 days from the date of recognition.
Collectibility of trade receivables is reviewed on an ongoing basis. Debts which are known to be uncollectible are written off. A provision for doubtful receivables is established when there is an objective that the company will not be able to collect all amounts due according to the original terms of receivables.
(h) Plant and equipment Plant and equipment is stated at historical cost less depreciation. Historical cost includes expenditure that is directly
attributable to the acquisition of the items.
Subsequent costs are included in the asset’s carrying amount or recognised as a separate asset, as appropriate, only when it is probable that future economic benefits associated with the item will flow to the company and the cost of the item can be measured reliably. All other repairs and maintenance are charged to the Statement of Comprehensive Income during the financial period in which they are incurred.
Plant and equipment 2.5 to 13.3 years Computer and software 2.5 years Leasehold improvements Shorter of lease term and useful life
The assets’ residual values and useful lives are reviewed, and adjusted if appropriate, at each balance sheet date.
An asset’s carrying amount is written down immediately to its recoverable amount if the asset’s carrying amount is greater than its estimated recoverable amount.
Leasehold improvements are required to be written down over the shorter of the assets useful life and the term of the lease.
(i) Trade payables
These amounts represent liabilities for goods and services provided to the Company prior to the end of financial year which are unpaid. The amounts are unsecured and are usually paid within 30 days of recognition.
(j) Employee benefits
(i) Wages and salaries, annual and long service leave Liabilities for wages and salaries, including non-monetary benefits, and annual leave are recognised in
provisions, in respect of employees’ services up to the reporting date and are measured at their nominal values.
Long service leave is measured at present value as it not expected to be settled within 12 months.
(ii) Retirement benefit obligations The company contributes to accumulation superannuation plans. Contributions are charged against income
as they are made.

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
54
2012 $
2011 $
2. REVENUE
Grants received 13,263,625 10,963,281
Other revenue 858,798 803,445
Interest received 390,917 286,978
14,513,340 12,053,704
3. EXPENSES
(a) Surplus includes the following specific expenses
Depreciation 296,716 237,732
Rent 372,815 303,152
(b) Insurance
Insurance 81,637 86,110
(c) Other expenses
Advertising 36,252 11,400
Compliance costs 46,203 60,639
Consumables 200,978 159,189
Freight & cartage 9,222 16,695
Motor vehicles 17,446 7,337
Office maintenance 88,495 96,438
Office equipment leasing 8,683 –
Telecommunications 132,503 123,750
Trading surplus (un-acquitted) 2,541,279 2,962,619
3,081,061 3,438,067
(d) Administration Fee representing cost allocation for PGPPP 644,316 280,488
4. CASH AND CASH EQUIVALENTS
Current
Cash on hand 1,340 2,020
Cash at bank 5,718,728 6,002,450
5,720,068 6,004,470
5. RECEIVABLES
Current
Trade receivables 29,190 146,663
Other receivables 108,225 110,954
137,415 257,617
6. OTHER
Current
Prepayments 217,741 202,007
NOTES TO THE FINANCIAL STATEMENTS FOR THE YEAR ENDED 30 JUNE 2012 (continued)

55
2012 $
2011 $
7. PLANT AND EQUIPMENT
Non-Current
Plant & equipment – at cost 1,076,403 964,559
Less: accumulated depreciation (469,625) (325,168)
606,778 639,391
Computer and software – at cost 366,283 378,623
Less: accumulated depreciation (213,888) (254,831)
152,395 123,792
Leasehold improvements – at cost 811,857 811,857
Less: accumulated depreciation (155,071) (73,300)
656,786 738,557
1,415,959 1,501,740
Reconciliations
Reconciliations of carrying amounts for each class of plant and equipment are set out below:
Plant and equipment
Carrying amount at beginning of year 639,391 597,117
Additions 111,843 186,268
Disposals – (4,252)
Depreciation (144,457) (139,742)
CARRYING AMOUNT AT END OF YEAR 606,778 639,391
Computer and software
Carrying amount at beginning of year 123,792 75,406
Additions 104,541 94,569
Disposals (116,880) (4,059)
Depreciation (70,488) (42,124)
Depreciation written back on disposal 111,430 –
CARRYING AMOUNT AT END OF YEAR 152,395 123,792
Leasehold improvements
Carrying amounts at beginning of year 738,557 415,931
Additions – 380,136
Disposals – (1,643)
Depreciation (81,771) (55,867)
CARRYING AMOUNT AT END OF YEAR 656,786 738,557

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
56
2012 $
2011 $
8. PAYABLES
Current
Trade payables 454,495 597,636
Accrued expenses 820,263 344,666
Other payables 50,093 195,143
1,224,665 1,137,445
9. UNEARNED REVENUE
Unearned revenue
AGPT (Operational & accumulated funds) 5,779,170 6,408,417
5,779,170 6,408,417
Unearned revenue for the current and prior years represents grant funding from General Practice Education and Training (GPET). Until these funding organisations and the company finalise an agreement relating to this excess, the funds remain liable to claim by the funding organisation and are disclosed as a liability.
2012 $
2011 $
10. PROVISIONS
Current
Employee entitlements 297,028 217,858
Non-Current
Employee entitlements 74,197 85,991
11. TERM ALLOCATION REVIEW
Audit review of adherence to policy and procedures with respect to training placement and allocation.
From a corporate governance perspective, the Auditor is satisfied that the policies and processes with respect to GP Synergy training allocation processes have been generally adhered to.
NOTES TO THE FINANCIAL STATEMENTS FOR THE YEAR ENDED 30 JUNE 2012 (continued)

57
12. KEY MANAGEMENT PERSONNEL
(a) Key management personnel include the directors, the CEO and the Director of Training.
(b) Directors
The names of each person holding the position of GP Synergy Limited during the financial year are:
Dr C Hespe Dr J Keh Dr J Korner Dr N Shadbolt Dr O Brookes A/Prof L Fragar Dr H Nespolon Dr N Andric Prof T Liaw Dr I Kamerman A/Prof M Guppy Prof J Reath
(c) The compensation paid, payable or provided to other key management personnel consisted of short-term benefits of $455,104 (2011: $490,212).
(d) The compensation paid, payable or provided to directors consisted of short-term benefits in the nature of Board fees of $159,604 (2011: $174,874), practice payments of $199,022 (2011: $178,033), teaching fees of $3,438 (2011: $1,167) and conference attendance fees of $6,182 (2011: $6,798).
Board fees of $159,604 (2011: $174,874) represent grossed up salary packaging including non-cash items, whereas actual payments made and received were $102,261 (2011: $117,991) (see table page 21).
Practice payments of $199,022 (2011: $178,033) represent payments made to practices which are connected with directors. However, these payments are not necessarily received directly by directors, as funds are paid to supervisors attached to the practice.

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
58
NOTES TO THE FINANCIAL STATEMENTS FOR THE YEAR ENDED 30 JUNE 2012 (continued)
2011
Director
A
Gross Fees Excl salary package
B
Salary Packaged Amount
C
Grossed Up Salary Package
D
Salary Sacrifice
Super
E
Super SGC 9%
F
Payroll Benefits Received
(A+C+D+E)
Adair, Ian(Ceased 29/10/2010) 50 2,835 5,299 – 260 5,609
Andric, Nada(Appointed 29/10/2010) 3,982 – – – 358 4,304
Baker, Martyn John(Ceased 29/10/2010) 2,970 – – – 267 3,237
Brookes, Owen David – 7,288 13,622 – 656 14,278
Chalasani, Ashok Kumar(Ceased 29/10/2010) – – – 2,700 243 2,943
Fragar, Lyn – 8,870 16,580 – 798 17,378
Gray, Matthew James(Ceased 29/10/2010) – 5,110 9,552 – 460 10,012
Guppy, Michelle 6,480 – – – 583 7,063
Hespe, Charlotte Mary – 13,370 24,991 5,380 1,203 31,575
Korner, Jacqueline – 9,091 16,993 – 818 17,812
Liaw, Siaw – Teng – 6,480 12,112 – 583 12,696
Martin, Rod(Ceased 29/10/2010) – 4,300 8,038 – 387 8,425
Nespolon, Harry Michael 18,130 – – – 1,389 19,519
Reath, Jennifer(Appointed 29/10/2010) 1,080 2,700 5,047 – 340 6,467
Rose, Alison(Ceased 29/10/2010) – 2,700 5,047 – 243 5,290
Shadbolt, Narelle(Ceased 29/10/2010) 2,700 – – – 243 2,943
Woollard, Leslie(Ceased 29/10/2010) – 2,700 5,047 – 243 5,490
TOTAL 35,392 65,444 122,327 8,080 9,075 174,874

59
2012
Director
A
Gross Fees Excl salary package
B
Salary Packaged Amount
C
Grossed Up Salary Package
D
Salary Sacrifice
Super
E
Super SGC 9%
F
Payroll Benefits Received
(A+C+D+E)
Andric, Nada (Ceased 28/10/2011) 1,080 540 1,009 – 146 2,235
Brookes, Owen(Ceased 28/10/2011 – 2,105 3,935 – 189 4,124
Fragar, Lyn – 9,226 17,246 – 816 18,062
Guppy, Michelle 5,972 – – – 537 6,509
Hespe, Charlotte Mary – 17,780 33,234 19,373 3,344 55,950
Kamerman, Ian(Appointed 28/10/2011) – 4,352 8,135 – 392 8,526
Keh, Jeremy(Appointed 08/11/2011) – 4,352 8,135 – 392 8,526
Korner, Jacqueline – 8,960 16,747 – 806 17,553
Liaw, Siaw – Teng – 5,972 11,163 – 537 11,700
Nespolon, Harry(Ceased 28/10/2011) 893 1,890 3,533 – 250 4,676
Reath, Jennifer – 5,972 11,163 – 537 11,700
Shadbolt, Narelle(Appointed 08/11/2011) 540 4,825 9,018 – 483 10,041
TOTAL 8,485 65,973 123,317 19,373 8,430 159,604

Financials
GP Synergy Limited (A.B.N. 62 099 141 689) Annual Report for the year ended 30 June 2012
60
NOTES TO THE FINANCIAL STATEMENTS FOR THE YEAR ENDED 30 JUNE 2012 (continued)
2012 $
2011 $
13. REMUNERATION OF AUDITORS
Audit Services
Audit of the financial report
K S Black & Co 14,100 13,365
Other services – KS Black & Co 3,360 3,200
14. NOTES TO THE STATEMENT OF CASH FLOWS
(a) For the purposes of the Statement of Cash Flows, cash and cash equivalents included cash on hand and cash at bank.
Cash and cash equivalents as at the end of the financial year as shown in the Statement of Cash Flows is reconciled to the related items in the Statement of Financial Position as follows:
2012 $
2011 $
Cash on hand 1,340 2,020
Cash at Bank 5,718,728 6,002,450
5,720,068 6,004,470
(b) Reconciliation of Net Surplus in Net Cash
Provided by Operating Activities:
NET SURPLUS – 48,896
Depreciation 296,716 237,732
(Gain)/Loss on disposal of noncurrent assets 5,152 (1,361)
Changes in Assets and Liabilities
Decrease/(increase) in trade receivables and other assets 104,785 328,613
Increase/(decrease) increase in trade and other payables 87,220 58,754
Increase/(decrease) in provision for employee entitlements 67,376 9,763
(Decrease)/increase in unearned revenue (629,247) 1,505,359
NET CASH (USED IN)/PROVIDED BY OPERATING ACTIVITIES (68,018) 2,187,756

61
15. CONDUCT OF RISK AUDIT PROGRAMME
GP Synergy Limited conducts a risk audit programme which is internally reviewed during the year. This programme is set against the AN/NZS 4360;2004 Standards. This programme is an extension of the risk management function of the company using National Audit Office Guidelines and the Standards promulgated by the Institute of Internal Auditors.
I have reviewed the audits against the audit objectives identified and I am satisfied that the policies and processes have been adhered to.

GP SynergyChippendale: 02 9818 4433Liverpool: 02 9756 5711Armidale: 02 6776 6225Moree: 02 6752 7354E: [email protected]: www.gpsynergy.com.au