
GOVERNING BODY PAPER - NHS Greenwich CCG body... · GOVERNING BODY PAPER Title of paper: Integrated...
14
i Enclosure: D Agenda item: 6i GOVERNING BODY PAPER Title of paper: Integrated Care Pioneer Status Date of meeting: Wednesday 27 th November 2013 Presented by: Dr Junaid Bajwa Title: GP Clinical Commissioner Prepared by: Langley Gifford Title: AD Integrated Commissioning Summary of Strategic Objectives Supported by this Report (X) Improve health outcomes X To assure and drive improvements in quality X Ensure access to high quality primary care services X Meet statutory obligations X Ensure access to high quality secondary care services Take a long term approach to the health needs of the local population X Building a new Clinical Commissioning Group Enhance communications with practices and patients X Enhance the use of information X Please provide brief executive summary:- Greenwich Co-ordinated Care Eltham test and learn pilot has been successful in being awarded pioneer status for integrated care, by NHS England (NHSE). Nationally 14 organisations have been awarded this status of which four are in London. Pioneer Status does not bring additional financial resources but Greenwich will have access to support from NHSE. Monitoring arrangements have yet to be finalised. Summary of Impact Assessment and Risk Management Issues (x) (please provide detail in the body of the report) Impact on Risk Assurance Framework (x) Yes No N/A Impact on Environment (x) Yes No N/A Legal Implications (x) Yes No N/A Resource implications (x) Yes No N/A Equality impact assessment (x) Yes X No N/A NHS Operating Framework areas of Quality, Reform and Finance (x) Yes X No N/A Patient and Public Involvement (x) Yes X No N/A Communications and Engagement (x) Yes X No N/A Impact on CCG Constitution (x) Yes No X N/A Brief Summary of Recommendations To note and consider.
Transcript of GOVERNING BODY PAPER - NHS Greenwich CCG body... · GOVERNING BODY PAPER Title of paper: Integrated...

i
Enclosure: D Agenda item: 6i
GOVERNING BODY PAPER
Title of paper: Integrated Care Pioneer Status
Date of meeting: Wednesday 27th November 2013
Presented by: Dr Junaid Bajwa Title: GP Clinical Commissioner
Prepared by: Langley Gifford Title: AD Integrated Commissioning
Summary of Strategic Objectives Supported by this Report (X)
Improve health outcomes X To assure and drive improvements in quality X
Ensure access to high quality primary care services
X Meet statutory obligations X
Ensure access to high quality secondary care services
Take a long term approach to the health needs of the local population
X
Building a new Clinical Commissioning Group
Enhance communications with practices and patients
X
Enhance the use of information X Please provide brief executive summary:-
Greenwich Co-ordinated Care Eltham test and learn pilot has been successful in being awarded pioneer status for integrated care, by NHS England (NHSE). Nationally 14 organisations have been awarded this status of which four are in London. Pioneer Status does not bring additional financial resources but Greenwich will have access to support from NHSE. Monitoring arrangements have yet to be finalised.
Summary of Impact Assessment and Risk Management Issues (x)
(please provide detail in the body of the report)
Impact on Risk Assurance Framework (x) Yes No N/A
Impact on Environment (x) Yes No N/A
Legal Implications (x) Yes No N/A
Resource implications (x) Yes No N/A
Equality impact assessment (x) Yes X No N/A
NHS Operating Framework areas of Quality, Reform and Finance (x)
Yes X No N/A
Patient and Public Involvement (x) Yes X No N/A
Communications and Engagement (x) Yes X No N/A
Impact on CCG Constitution (x) Yes No X N/A
Brief Summary of Recommendations
To note and consider.

CNash
TextBox
Enclosure Di

Tim Higginson, Chief ExecutiveLewisham Healthcare NHS Trust
Rosaline Mitchell, ManagerHealthWatch Greenwich
Pauline O’Hare, Development OfficerGreenwich Action for Voluntary Service
Stephen Firn, Chief ExecutiveOxleas NHS Foundation Trust
Dear Norman Lamb
Re: EXPRESSIONS OF INTEREST FOR HEALTH AND SOCIAL CARE INTEGRATION ‘PIONEERS’
Further to your letter (Gateway Reference Number: 00079), please find attached our joint expression of interest to become a health and social care integration Pioneer site. Greenwich has a long history of strong and effective working relationships between all partners (including Healthwatch’s predecessor body, LINK). The Greenwich Health & Wellbeing Board has stated its commitment to working towards full integration of our community services. Becoming a Pioneer site will support this work through helping us access a range of expertise to tackle the outstanding local challenges. We believe our model will improve patient care. We would welcome the platform of becoming a Pioneer site, in order to engage in conversation about better coordinated care, with health and social care economies across the country.
We look forward to hearing from you.
Yours sincerely
John Nawrockyi, Director of Adults and Older People’s ServicesRoyal Borough of Greenwich
GreenwichClinical Commissioning Group
Lewisham HealthcareNHS Trust
OxleasNHS Foundation Trust
Annabel Burn, Chief OfficerNHS Greenwich Clinical Commissioning Group
CNash
TextBox
Enclosure Dii
Greenwich Coordinated CareExpression of interest for health and social care Pioneer pilot
GreenwichClinical Commissioning Group
Lewisham HealthcareNHS Trust
OxleasNHS Foundation Trust
CNash
TextBox
Enclosure Diii
Greenwich Coordinated CareThe DH document ‘Integrated care and support: our shared commitment’ (May 2013) describes how national and local organisations need to take urgent and sustained action to make integrated care and support happen. This document describes how, in the Royal Borough of Greenwich, statutory and voluntary organisations, together with local residents, have taken action and have a shared commitment to make further progress.
In this document we describe the integrated care system we have established in the Royal Borough of Greenwich and our vision for future developments. This initiative has already delivered coordinated services for older people and people with physical disabilities. In the next phase, we will extend integration across all services and rebase health and social care delivery around clusters of GP practices. A comprehensive integrated care system will be in place in one geographical area of the borough by April 2014, with roll out to the whole borough over the following months. Greenwich residents will receive services that work together to focus on prevention, early identification, care navigation and care coordination for patients with emerging complex needs. Support to carers will be integral to this work. As described in ‘Evaluating integrated and community based care’ (Nuffield Trust, June 2013), we recognise that making changes across a whole system is complex and challenging. However, we have the joint commitment, shared focus, established networks and track record to make changes at a scale that will make a true difference to patients.
Contents Page 1. How Greenwich coordinated care will meet the Pioneer site key criteria 22. Introduction to Greenwich 3 2.1 Local views on health and social care challenges 2.2 The partners in this initiative3. What has been achieved to-date? 4 3.1 Background 3.2 Phase 1: Governance arrangements 3.3 Phase 1: Integrated rapid response & intermediate care/reablement 3.4 The Greenwich Advanced Dementia Service 4. Phase 2: Right care, right time, right place 5 4.1 Our plans 4.2 What we hope to achieve 4.3 New financial arrangements 5. How will we know if the new model is making a difference? 7 5.1 Understanding the individual’s experience of our services 5.2 Monitoring performance 6. Will we deliver? 7 6.1 Criteria for success 6.2 Dissemination 7. Outstanding issues 8 Appendices 9
ContactHelen Smith Deputy Chief Executive Oxleas NHS Foundation Trust Pinewood House Pinewood Place Dartford KENT DA2 7WG
T: 01322 625018
1

1. How Greenwich coordinated care will meet the Pioneer site key criteriaPrimary criterion How we will achieve thisArticulate a clear vision of its own innovative approaches to integrated care and support
Through our partnership, we have designed the Greenwich coordinated care programme which has a clearly defined vision of how all parties would like services to develop, the outcomes we are seeking and the mechanism by which this will be achieved and monitored (Section 5). The model is based on agreed principles which are aligned with the Narrative developed by National Voices (Section 6).
Plan for whole system integration Our partnership encompasses mental and physical health, social care and public health, as well as other public services, such as education, and involves the community and voluntary sectors. We are focusing on integrating the delivery of services across the whole system to enable people to manage their healthcare more rather than looking at complex organisational change. (Section 2.2/4.1)
Demonstrate commitment to integrate care and support across the breadth of relevant stakeholders and interested parties within the local area
This initiative is not starting from scratch. We already have strong working relationships and an established track record in integrating care across health and social services, primary and secondary, mental and physical health boundaries. (Sections 3.3/3.4) There is a shared commitment to take this transformational work further.
Demonstrate the capability and expertise to deliver successfully a public sector transformation project at scale and pace
We have already shown that the changes we have made together improve the experience for patients, have better outcomes and save money. With the support of the Pioneer programme, we wish to build on this to bring further improvements more quickly across services in the borough and to share learning across the country (Sections 3.2/3.3/4).
Commit to sharing lessons on integrated care and support across the system
Sharing our learning and learning from others is an established part of the way we work. We are already recognised as having some expertise in this area and therefore would use this strong basis to share the lessons learned through the Pioneer programme (Section 6.2)
Demonstrate that its vision and approach are, and will continue to be, based on a robust understanding of the evidence
The Greenwich coordinated care programme has been supported by the Institute of Public Care (IPC), Oxford Brookes University (Section 3.1) Our ongoing commitment to using and developing the evidence base is shown by our agreement with the University of Greenwich to establish an Institute of Integrated Care. (Section 6.2)
2
Greenwich is the 19th most deprived borough in England with 45% of areas among the most deprived 20% in England. Although there are pockets of affluence, the overall picture is one of significant deprivation.
As would be expected in a deprived borough, there are great challenges for health and social care services in reducing avoidable morbidity and mortality. There have been recent improvements, but life expectancy is 75.8 years for men against an England average of 78.3 and 81.9 years for women, against an average of 82.3. The demographic composition of the borough makes equal and easy access to health and social care services an absolute priority and services must be delivered in acceptable ways for Greenwich’s multi-ethnic community.
NHS Greenwich CCG’s Commissioning Strategy Plan (CSP) 2009/10-2013/14, focused on preventing the main conditions in the borough that cause significant levels of premature death or illness, and affect quality of life particularly cancer, cardio-vascular disease and common mental health conditions. An additional focus is on ensuring local children grow up into healthy adults. The CSP set out the following transformation agenda:
• Shifting 55% of secondary acute activity into clinically appropriate, lower cost community settings.
• Integrating care pathways between primary, acute, mental health and social care services.
• Transferring 60% of A&E activity to integrated care networks and avoiding 30% of non complex non-elective acute admissions
• Transferring 59% of minor procedures to integrated care networks and delivering care closer to home.
• Active case management of long-term conditions (LTC), leading to 40% reduction in hospital admissions for this patient cohort.
• Providing more early interventions and health promotion and avoiding 10% non-elective admissions.
• Enabling people to take greater ownership of their health.
2.1 Local views on health and social care challenges
In January 2011, NHS Greenwich and the Royal Borough held two events to provide an opportunity for local people to comment on services and health needs. There were some clear messages: • People are generally satisfied with services once
they get into them, however access must be improved with mobile clinics in convenient venues and at flexible times, not just 9-5 on week days.
• Information should be more widely available in places susch as GP surgeries, leisure centres, libraries, supermarkets and travel hubs. GPs and other health and social care staff need to be better informed about community services and share that information with residents.
• Look after people who are vulnerable and isolated and strengthen the human touch. People want their physical and psychological needs addressed and those with long-term conditions want more psychological support.
• Move more services from hospitals into the community, but make sure agencies work closely to plug any gaps and join-up services.
• Make sure people know about alternatives to A&E, and improve access to GP services to stop people using A&E when they do not need to.
In response to the challenges set out by the CSP and by local residents, local health and social care agencies came together to put in place an integrated care system in Greenwich.
2.2 The partners in this initiative
The partners are: the Royal Borough of Greenwich, Greenwich CCG, Oxleas NHS Foundation Trust, Greenwich Action for Voluntary Services, Healthwatch, Lewisham and Greenwich NHS Trust and primary care. Further details of each organisation are in appendix 1.
Lewisham and Greenwich NHS Trust will be established on 1 October 2013. They have already committed to continuing working on this initiative as they take responsibility for the delivery of acute services in Greenwich – this will build on the good partnership that exists with South London Healthcare NHS Trust, the current acute provider.
This programme is linked to the Trust Special Administrator change programme which was backed by the Secretary of State for Health in February 2013 and requires a change of service provision from hospital to community in the next 3 years.
2. Introduction to Greenwich
• In 2011, there were 274,951 people registered with a Greenwich GP
• Currently 35% of the population are from Black and Minority Ethnic (BME) groups
• By 2021, BME groups will account for 47.2% of the population
• Population is expected to increase by 13% by 2015• Life expectancy is significantly lower than the
national average, particularly for men
Source: The Greenwich Joint Strategic Needs Assessment (2012)
3
3. What has been achieved to date?3.1 Background
Mental health and social care services in Greenwich have a long history of working together within a single management structure. Multi agency teams offering health and social care interventions and support through one assessment route have been established for children, adults and older adults with mental health needs and people with learning disabilities, for over 15 years.
Community health services transferred to Oxleas NHS Foundation Trust on 1 July 2011, in order to integrate physical and mental health services and facilitate the necessary transformation for integrated care. Physical health community services are now integrated with social services and some mental health services, for both adults and children.
In April 2011, Greenwich community health services, as part of Oxleas, and local authority adult social care, launched phase 1 of an integrated service that supports adults and older people with urgent health and social care needs, often with comorbidities of long term conditions and complex personal care needs (see 3.3). In April 2013, Public Health moved into the local authority strengthening and enabling further integration in the health and wellbeing agenda.
3.2 Phase 1: Governance arrangements
An Integrated Care System (ICS) Project Board was established, consisting of the partners detailed in 2.2. Lewisham and Greenwich NHS Trust does not come into being until 1 October 2013 but is fully committed to the work of the Board. The Board oversees the strategic direction, delivery and implementation of the Greenwich Integrated Care System project. Each agency retains responsibility for authorising and delivering its own areas of work.
The ICS Board commissioned the Institute of Public Care (IPC), Oxford Brookes University, to coordinate and facilitate the project, providing change management, training and academic support. IPC remain closely involved with this work.
Through providing better coordinated care, closer to home, the project objectives were for:
• more accessible and flexible services, giving fair access via a single point of entry
• seamless and holistic health and social care in the right place, at the right time
• the promotion of self care of long term conditions and maximising people’s independence
• support to live healthy and fulfilled lives by reducing the requirement for intensive and costly interventions
• support to people to retain or improve levels of
independence via short-term reablement• a decrease in domiciliary care packages• a reduction in admissions to hospital and long term
residential/nursing care
3.3 Phase 1: Integrated rapid response & intermediate care/reablement
• Social and healthcare teams were engaged through workshops to redesign the service; they mapped pathways and identified gaps, blockages and bottlenecks. A multi-professional group then developed the (as was) new model. This included:
• A single initial point of access for referrals and an immediate response to patient need
• Establishing a Joint Emergency Team (JET) to provide a fast immediate response to prevent hospital admission
• A Hospital Intervention Discharge team to provide speedy discharge to intermediate or social care
• Three Community Assessment and Rehabilitation teams (CARs) providing up to 6 weeks rehabilitation and on-going social care
• Joint management of flow through intermediate care beds via a collective KPI
• Co-located teams of nurses, physiotherapists, OTs, social workers and care managers.
The phase 1 project won the HSJ Secretary of State Award in 2011, the HSJ Award for staff engagement 2011 and was a finalist in the DH NHS Leaders Awards for partnership working in 2012. The critical success factors were: a commitment to a shared vision, a willingness to change the culture of both health and social care organisations, excellent clinical engagement which led to shared values and approaches, excellent leadership, good governance and risk management and integrated performance management. The wider stakeholder engagement in phase 1 included service users, carers and staff unions.The integrated rapid response and reablement model forms part of a Virtual Admission Avoidance team established in 2010 (which won an HSJ Award for Efficiency in 2011). This team brings together key services to prevent potential A&E presentations, including LAS diverts to other community services through agreed protocol, with encouraging results.
In summary, this model has been very successful and has reduced emergency hospital admissions, numbers of long-term care placements and people going straight from hospital into long term care, acute hospital bed days, re-admission rates within 30 days and the size or need for social care packages. It has increased the numbers of people using assistive technology.
In the first year, admissions to care homes reduced by 35%. After reablement, over 60% people required no care packages. This saved the Local Authority £900k. The number of avoided admissions continues to increase year-on-year. This shows that improved care coordination is leading to better outcomes for our residents, including improved quality of life as people continue to be able to live at home.
4

• Our work so far has seen a decrease in emergency admissions for people with conditions that could be treated in the community. Greenwich is now ranked the 15th best performing borough nationally (see appendix 2).
• Over the last 2 years, we have seen an 8% reduction each year in the number of people supported with a social care package.
• Between 11/12 and 12/13, there was a 7% reduction in the number of people supported in long-term care placements throughout the year.
• We have increased the number of people aged 65+ to remain at home following discharge from hospital through a reablement intervention and who are at home 91 days later. During 12/13, 89% were still at home at 91 days, up from 79% in 11/12.
• For assistive technology, we have seen an increase in the number of referrals for alarms and telecare sensors, up 46% from 11/12 to 12/13, which represents an additional 372 referrals.
• During 11/12, the number of people re-admitted to hospital within 14 days reduced. Our performance remains better than national and peer group figures.
• From the end of 10/11, the number of bed days spent in hospital has reduced and fallen below national and peer group comparison.
3.4 The Greenwich Advanced Dementia Service
Alongside the development of phase 1 above, other integrated initiatives were being developed. For example Oxleas led the development of a service that linked staff and resources from community health and older people’s mental health into a virtual team to support people with advanced dementia and their carers to receive care at home, through to the end of life. The team is centred around each person through care coordination and regular multidisciplinary meetings.
Outcomes for people who need care and support and their carers have been excellent from the start. For example, previously 50% of the carers in the project had to negotiate with more than eight different service providers, whereas now everything is coordinated via the team. In addition, people were able to remain at home, avoiding care home and hospital admission, whereas the evidence is that more than 80% of people in this group generally would have had at least one hospital admission in their last year of life.
The economic analysis has been very encouraging, with a conservative estimate of £2m savings on 100 cases. In 2012, the project successfully applied to become a ‘demonstrator site’ with the King’s Fund’s Comparison of UK based models of care coordination for people with complex conditions. The project was accepted as one of five national sites and has been part of this prestigious research project during 2012/13.
4. Phase 2: ‘Right care, right time, right place’4.1 Our plans
The ICS Board now has plans to consolidate, develop and extend the achievements to date. Phase 2 of our integration project moves beyond the care of vulnerable older and physically disabled people to target adults and older adults with complex needs across all care groups identified as being at high risk of ill health and hospitalisation. We have a preferred overall model and currently are talking to staff and people who need care and support about how this could be operationalised.
The proposal to extend current integrated care arrangements and create the Greenwich Coordinated Care (GCC) system was presented to the Shadow Health and Wellbeing Board in Greenwich. This approach was strongly endorsed by all partners, and complements the top three corporate priorities recently agreed by the Royal Borough of Greenwich in terms of enhancing existing integrated services in the borough to improve access to primary care and reduce reliance on acute services. The plan was well-received by GP representatives as a major opportunity to engage primary care in the whole system approach. Progress under the ICS Board was discussed by the members of the newly-formed H&WB earlier this year at a specially-convened meeting to look at further opportunities for integrated commissioning and service development. The Greenwich Health & Wellbeing Board will monitor the ICS Board’s implementation of phase 2 of the integrated model.
Importantly in this second phase, we are learning from recent research into the cost of co-morbidity between long term conditions and mental health. This demonstrates that many people with long term conditions also have mental health problems, leading to significantly poorer health outcomes and reduced quality of life. The impact of long term conditions and poor mental health is estimated to cost between 12 – 18% of NHS expenditure expenditure alone. In addition, we know that people with serious mental illness have significantly reduced life expectancy and poor physical health.
Thus our mental health services for working age and older adults will be fully included in this work. This also allows the wider care system to benefit from the substantial knowledge within mental health services of delivering multi-agency care planning to patients and their families. Individualised care planning has been at the heart of our mental health services for over a decade. We know how to deliver person centred care.
5

The diagram below shows how we will stratify patients and respond to their needs:
Our intention is to coordinate resources across health (acute, primary, community services), social care and the third sector to build a ‘team around the person’ for individuals with complex health and social care needs.
To do this, local services will ‘coalesce’ around clusters of GP practices; we expect there to be four clusters across the borough. These GP clusters can be viewed as ‘communities of practice’ with aligned health and social care services, the functions of which are:
• Complex and urgent treatment• Utilisation of reablement and domiciliary care• Multi-disciplinary care planning for high risk people
with health and social care needs, identified via risk stratification and emerging concern, recognising that one service can prevent admission but without a holistic focus of care coordination, may not make a difference to the individual’s life (eg, housing, bereavement).
• Promoting health and healthy lifestyles.
Each cluster will have a core team that will consist of GPs, clinical nurse team lead, district nursing, community matrons, continence, podiatry, IAPT, memory services, social care, housing, telecare/telehealth, domiciliary care, physiotherapists, occupational therapists and community psychiatric nurses (CPNs). Referrals to professionals will be via a single point of access.
In addition each core team will have:
1. Named links from a range of long term conditions teams, specialist mental health services, specialist social workers, learning disability team, JET, secondary care acute services, and pharmacists in the cluster. This extended cluster team will have strong bonds and shared values.
2. A risk stratification team/function responsible for identifying people who are high risk and reviewing their needs. Regular meetings to review the complex cohort will be coordinated by a borough-wide care navigator service. The care navigator will ensure that individuals in the risk stratified group have a
named key worker from within the core or linked membership of the cluster team, to deliver a co-created care and support plan with each patient.
3. Named links with local third sector organisations to facilitate their involvement in a multi-agency approach to care
4. Named links to London Ambulance Service and Bexley and Greenwich Community Hospice
5. Access to the medical diagnostic centre/ambulatory care at the acute trust and outreach specialist opinion.
6. Access to social care staff to develop integrated personal budgets to maintain independence alongside a commitment to implement personal health budgets
7. Public Health colleagues have a strong track record around prevention programmes, e.g. smoking, exercise, healthy eating and will link healthy living services into the core team.
8. The Local Authority are currently re-tendering all our domiciliary home care services and will commission services on a geographical patch basis to align with the span of the clusters and core teams. This will give staff within the Greenwich coordinated care system the opportunity to work closely with their local home care providers to develop person centred approaches to care.
Integrated intermediate care teams with adult social care will work across the borough and serve the clusters.
4.2 What we hope to achieve
We will know that clusters are working effectively when the core team sees itself as responsible for the ongoing treatment, care and support of their population. The concept of ‘discharge back to primary care’ will be replaced with the expectation of the lifetime management of people’s health and social care needs. This approach will encourage health promotion and prevention and help people manage their condition through self management programmes. All cluster teams will focus on intervening early to prevent an escalation in health or social care need. This will only be
Multi-disciplinary Teams
Complex Multi-Morbidity ?%
Co-morbidity ?%
More than 1 Specialist Team
Single Morbidity?%
Single Professional Input
Known Clients (Those already on the system)
Known Unknown Clients (Those we expect to be in the system but are not)
Unknown Clients (Those who we yet don’t know)
6
achieved if cluster teams get to know their patch well, and use their local community and voluntary sector resources. We want our cluster teams to take pride in supporting their population to remain fully engaged, happy citizens.
4.3 New financial arrangements
The advantages of working with a foundation trust include access to a range of financial and other freedoms to innovate and provide care in new ways. All partners recognise that we need to change the current financial arrangements, in order to incentivise prevention, reduce use of health service resources and deliver services through community based alternatives.
There is some experience locally, of different contractual models. For example, the CCG established a collaborative prime contractor model, whereby Greenwich and Bexley Community Hospice and Marie Curie contract with Oxleas for the provision of coordinated end of life care. In phase 2, we will explore this and other financial models to determine what delivers the best patient outcomes.
5. How will we know if the new model is making a difference?5.1 Understanding the individual’s experience of our services
All partners involved in the Greenwich Coordinated Care programme are fully committed to putting local people at the heart of the redesign and reorganisation of our services. Oxleas NHS Foundation Trust, the Royal Borough of Greenwich and the CCG have a strong track record in engagement and consultation. We are working closely with Greenwich Healthwatch to ensure that the needs and expectations of local residents strongly inform future arrangements for coordinating and streamlining health and social care in Greenwich. The local authority has well developed arrangements in place with each of its key user groups (older people, mental health, learning disabilities and drug and alcohol) which routinely inform and shape changes to its services, and its commissioning plans, and these are supplemented locally by patient feedback and local health surveys collected by community and mental health services and the CCG. The GCC partners are also analysing national data, including reports by National Voices, and this, together with local feedback will inform the development of a set of outcomes and performance measures which will monitor and track and the impact of its work.
We are committed to ongoing work with Healthwatch, so that they can monitor progress from a patient
perspective.
5.2 Monitoring performance
Alongside collecting data on the outcomes of integrated care, we are developing a set of KPIs based on the NHS Outcomes Framework 2012/13 and 2011/12 Adult Social Care Outcomes Framework. We will set targets to:
• Improve patient reported outcomes• Improve clinical indicators• Reduce A&E attendance and unplanned admissions
to hospital eg for people with long term conditions
6. Will we deliver?
6.1 Criteria for success
We identified a set of design principles to test the model. The model must:
• Improve people’s experience (as defined by the National Voices Narrative and local feedback)
• Engage GPs• Provide the shortest path to the most appropriate
care• Identify people needing support and care as early as
possible• Provide care as close to/in home as possible• Be effective for long term conditions and complex
needs• Make it easy to refer into and access services• Facilitate pooling and sharing of expertise• Increase health and social care staff knowledge and
understanding of each others roles• Address ‘frailty’ as a gap• Create flexibility so that people do not get ‘stuck’
between services.• Facilitate specialist input for people in the
community• Focus on all parts of the system from admission
avoidance to hospital and residential care• Align the goals and objectives of providers• Enable effective working with other services ie
housing, voluntary sector, substance misuse• Be developed within existing resources
This level of change can only take place within stable, sustainable organisations with extensive experience of successfully delivering large-scale change. Within Greenwich, we have a long history of strong and effective working relationships. We already have transformed the delivery of mental health, learning disability and community health services. We understand the need to focus on changing culture and values and not just on putting new structures in place – our partnership provides a firm foundation for transformation and innovation.
We have tested the new model against the design principles detailed above and – on the basis of this assessment – are confident that we will deliver this second phase.
7
9
6.2 Dissemination
We are committed to disseminating the lessons learnt from our project. Evidence of this can be found in the extensive series of talks, presentations and workshops given by Royal Borough of Greenwich and Oxleas, following the HSJ Award last year. Learning was shared at all the national LTC QIPP events (led by Sir John Oldham). The Royal Borough of Greenwich’s AD is now part of Sir Oldham’s Committee on developing integrated care.
Annabel Burn, the Chief Officer for NHS Greenwich Clinical Commissioning Group is the Senior Responsible Officer for the South East London Community Based Care Strategy which is taking forward the commissioning intentions for all 6 CCGs in south east London in the areas of primary and community care, planned care and Integrated Care. In addition Jay Stickland, the Deputy Director of Adult and Older People’s Services is the Integration Lead for this programme. This will enable Greenwich to spread its learning as it develops integration more widely across south east London but also to import new ways of working from neighbouring organisations who are at different stages in their development.
Our partnership with the Kings Fund for the Advanced Dementia Care project is another example of our willingness to share our experiences. Being part of this project enables us to publicise our integrated approach. A film has been made about the service, which will be available on the Kings Fund website. The project, which also includes the Torbay initiative and Sandwell ‘wellbeing hub’, has allowed us to visit other successful ’care co-ordinators/integrators’ and given us a platform to disseminate lessons learned from our own work.
We will continue to work closely with IPC, Oxford Brookes University, to disseminate information about the project through articles and conferences. In addition, the Trust has secured agreement from the University of Greenwich to establish an Institute of Integrated Care. This will facilitate local research into integration and will provide a platform for the academic dissemination of this work.
7. Outstanding issuesThere are a number of areas where we have not resolved problems relating to service delivery, that we will address in Phase 2. It is these areas where we would benefit hugely from the support of being a Pioneer project and we would greatly welcome contact with other organisations who could help us resolve the issues.
1. Principal amongst these is a shared patient record across agencies and a working interface across different patient/client management systems in health and social care. This would both improve the quality of care and give the ability to link and analyse data to commission for best outcomes
2. The size and make up of the populations held in each cluster.
3. There are very few examples of mental health services being fully integrated into local systems. We will redesign local mental health care pathways so that these can be delivered within the new integrated structure – this work is already underway.
4. We appreciate the potentially destabilising effect that competition, choice and control may have on integrated care systems. The H&WB Board is committed to supporting a sustainable system, based on transparency and openness that stands up to scrutiny and to market testing.
5. As noted above, we will need a new financial infrastructure to change the incentives at points along the patient pathway. All partners, particularly the providers, are committed to an ‘open book’ approach whereby we can understand the true cost of different services and how income/payment can be linked to practice that promotes health and reduces service use.
8

Royal Borough of Greenwich (RBG) is one of the first London boroughs to move towards integration between Health and Social Care. Since April 2011, RBG has implemented an integrated structure across its Community Assessment and Rehabilitation Teams, Hospital Discharge Team and Joint Emergency Team. The feedback which RBG staff have given around this integrated structure has been very positive so far with many benefits to the people using the services. These include admission avoidance, increased joint working and decreased duplication of assessments. RBG has also recently been awarded Council of the Year by the Local Government Chronicle (LGC) in recognition of their “innovation, inspiration and hard work” resulting in an improvement in services across the local area. As an organisation, RBG has a high level of stability and a workforce which is committed, motivated and already has first hand knowledge of the challenges and benefits of integration. Public Health are now part of RBG and are fully committed to this project.
NHS Greenwich Clinical Commissioning Group (CCG) is responsible for commissioning most of the healthcare services for the people of Greenwich. It is responsible for planning which services need to be in place and ensuring that there are a range of healthcare providers able to deliver care high quality care to patients when they need it. They are led by local GPs who understand the needs of their patients and the healthcare of their local population. As a membership organisation comprising of all the 44 GP practices in Greenwich, the CCG is dedicated to planning, commissioning and monitoring the best possible health services for Greenwich residents that are integrated to improve health and wellbeing and reduce health inequalities.
Greenwich primary care services are formed by 44 GP practices which are commited to working with patients and their families and other healthcare providers to improve the health of the local population. Through Greenwich CCG, there are well-established GP leads who are an integral part of the Greenwich Coordinated Care initiative.
Oxleas NHS Foundation Trust delivers:• integrated mental health and social care services in
Bexley, Bromley and Greenwich• integrated adult community health and social care
services in Greenwich and Bexley• specialist children’s services in Greenwich and soon
in Bexley (due to be transferred in July 2013)• forensic services to Bexley, Bromley, Greenwich,
Lewisham and Kent• prison healthcare services in Kent• adult learning disability services in Bexley, Bromley
and Greenwich
Oxleas has consistently been amongst the top performing FTs and, critical to this bid, has a highly-
motivated and stable workforce. In the last two years, Oxleas has been rated the top trust to work for in London and the whole of the South; similarly excellent results are achieved in the mental health National Patient Survey. Oxleas thus has the capacity and focus to drive through the transformation. In addition, Oxleas membership and the Council of Governors will be a prime mechanism for wide ranging engagement of local stakeholders in this work. The trust has been delivering integrated mental health services through a S75 with the local authority for over a decade.
Greenwich Action for Voluntary Service (GAVS) is the local Council for Voluntary Services for Royal Borough Greenwich. Its role is to support and represent voluntary and community organisations working across the royal borough in all their forms. The organisation’s representation work has been recognised by NAVCA accreditation-the nationally recognised quality mark for infrastructure organisations which specifically mentioned the quality of support provided to voluntary and community sector representatives. Other support includes facilitating quarterly forums for the sector, including a forum for voluntary and community organisations working with adults and older people. The Health and Well Being Forum ensures regular communication amongst voluntary sector organisations providing health & well-being services and activities in Greenwich as well as creating opportunities to link GAVS member organisations with local projects.
Healthwatch Greenwich is the new consumer champion aiming to give citizens and communities a stronger voice to influence and challenge how health and social care services are provided locally.Healthwatch Greenwich is pleased to build on its close relationship with Oxleas established by the LINk. As well as bi-annual liaison meetings, the LINk facilitated Statutory Sector Liaison Group Meetings (attended by Oxleas) where statutory partners from services across health and social care shared updates and allowed LINk to raise concerns highlighted from its engagement with the local people; this will continue in Healthwatch. South London Healthcare Trust (SLHT) currently is the acute secondary provider. Following the work of the Trust Special Administrator, acute services in Greenwich will transfer into Lewisham and Greenwich NHS Trust on October 2013. This will give the stability with which secondary acute care fully can engage with the integration work. A number of senior clinicians are already engaged in better coordination with community services. For example, in cardiology, Oxleas and SLHT have moved services from a hospital to community setting and reconfigured the skill mix and there has been good joint working in relation to hospital discharge. Lewisham and Greenwich NHS Trust is fully committed to working with partners on implementing the integrated model of service.
Appendix 1: Partners involved in the initiative
9
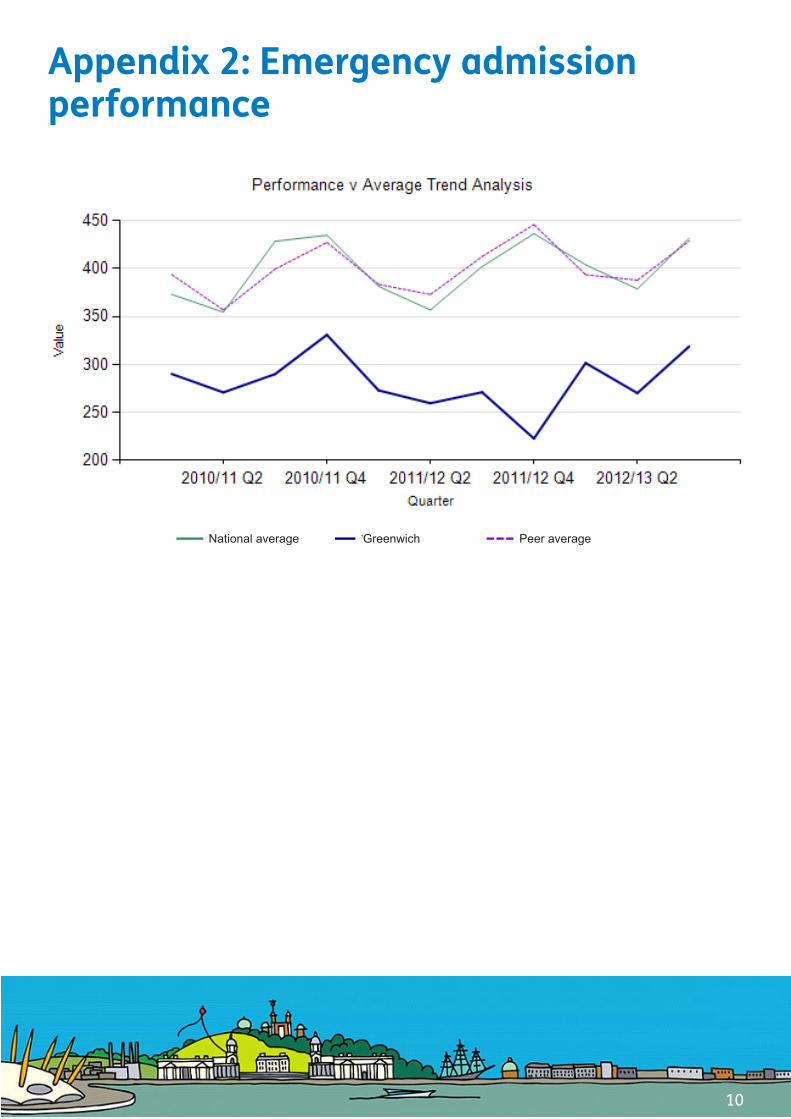
National average Greenwich Peer average
Appendix 2: Emergency admission performance
10


















