Glycolate and 2-phosphoglycolate content of tissues measured by ion chromatography coupled to mass...
4
Glycolate and 2-phosphoglycolate content of tissues measured by ion chromatography coupled to mass spectrometry John Knight ⇑ , Mark Hinsdale, Ross Holmes Department of Urology, Wake Forest University Medical Center, Medical Center Boulevard, Winston-Salem, NC 27157, USA article info Article history: Received 5 July 2011 Received in revised form 18 October 2011 Accepted 24 October 2011 Available online 29 October 2011 Keywords: Glycolate Phosphoglycolate Mass spectrometry Ion chromatography abstract Glycolate and 2-phosphoglycolate (PG) are 2-carbon monocarboxylic acids with ill-defined metabolic roles. Their concentrations have not yet been described in tissues apart from body fluids and erythro- cytes. We describe the use of ion chromatography coupled with mass spectrometry (IC-MS) to quantify levels of glycolate and PG in tissue. Sample preparation and analysis can be performed within an hour. Low concentrations of glycolate (12–48 nmol/g) and PG (4–17 nmol/g) were detected in all tissues. The availability of this IC-MS assay will facilitate investigations of the origin, function, and metabolism of glycolate and PG in tissues. Ó 2011 Elsevier Inc. All rights reserved. An understanding of the origin, metabolism, and biological function of glycolate and 2-phosphoglycolate (PG) 1 is lacking as suitable methods for determining their concentrations are not avail- able. All cells most likely contain glycolate as a result of the metab- olism of glyoxal by the glyoxalase system and the reduction of glyoxylate by glyoxylate reductase as these activities are present in all cells. Glyoxal arises from glucose autooxidation, the break- down of glycation products, and lipid peroxidation [1–3]. Liver and kidney hydroxyproline metabolism is likely to be the major source of glyoxylate synthesis [4]. The origin of PG in mammalian cells is not known with certainty. In plants and some bacteria, it is synthesized during photorespiration following the oxygenation of ribulose-1,5,-bis- phosphate [5–7]. In all cells PG is generated as a result of DNA repair of 3 0 -PG ends that are generated following strand breaks [8,9]. The amount of PG formed during these processes has yet to be determined. Erythrocytes have been reported to contain a low concentration (2–5 lM) of PG [10], although earlier research was unable to identify the presence of PG in these cells [11,12]. The method used to measure PG was not direct and relied on its ability to activate the 2,3-diphosphoglycerate (DPG) phosphatase activity of bisphosphoglycerate mutase (BPGM). The reliability of this pro- cedure at such low concentrations of 2-PG has been questioned [13]. The biological role of PG, if any, is not known. It has attracted attention because low levels of PG stimulate the activity of DPG phosphatase and it is the most potent modifier yet identified [14]. This activity is potentially important as the concentration of DPG influences the binding of oxygen to hemoglobin. PG is dephos- phorylated by phosphoglycolate phosphatase, an apparent ubiqui- tous enzyme in cells of eukaryotes and prokaryotes, and in plants this activity is required to maintain a functional Calvin cycle [8,12,15,16]. In this report, we show that IC-MS reliably measures the con- centration of both PG and glycolate and have used this method to measure their concentrations in a variety of tissues. This method does not require extensive sample preparation, and total assay time, including tissue preparation, can be completed in an hour. Materials and methods Materials Reagent grade chemicals were obtained from either Sigma– Aldrich Chemicals (St. Louis, MO) or Fisher Scientific (Pittsburgh, PA). Sodium glycolate, 97%, and 2-phosphoglycolic acid as a tri-(monocyclohexylammonium) salt, 98%, were purchased from Sigma–Aldrich. Tissue preparation Freeze-clamped tissue was extracted with 10% ice-cold trichlo- roacetic acid (TCA). This preparation was vortexed continuously for 0003-2697/$ - see front matter Ó 2011 Elsevier Inc. All rights reserved. doi:10.1016/j.ab.2011.10.041 ⇑ Corresponding author. Fax: +1 336 716 0174. E-mail address: [email protected] (J. Knight). 1 Abbreviations used: BPGM, bisphosphoglycerate mutase; DPG, 2,3-diphosphogly- cerate; IC-MS, ion chromatography coupled with mass spectrometry; LOD, limit of detection; LOQ, limit of quantification; PG, 2-phosphoglycolate; TCA, trichloroacetic acid. Analytical Biochemistry 421 (2012) 121–124 Contents lists available at SciVerse ScienceDirect Analytical Biochemistry journal homepage: www.elsevier.com/locate/yabio
-
Upload
john-knight -
Category
Documents
-
view
213 -
download
0
Transcript of Glycolate and 2-phosphoglycolate content of tissues measured by ion chromatography coupled to mass...

Analytical Biochemistry 421 (2012) 121–124
Contents lists available at SciVerse ScienceDirect
Analytical Biochemistry
journal homepage: www.elsevier .com/locate /yabio
Glycolate and 2-phosphoglycolate content of tissues measuredby ion chromatography coupled to mass spectrometry
John Knight ⇑, Mark Hinsdale, Ross HolmesDepartment of Urology, Wake Forest University Medical Center, Medical Center Boulevard, Winston-Salem, NC 27157, USA
a r t i c l e i n f o a b s t r a c t
Article history:Received 5 July 2011Received in revised form 18 October 2011Accepted 24 October 2011Available online 29 October 2011
Keywords:GlycolatePhosphoglycolateMass spectrometryIon chromatography
0003-2697/$ - see front matter � 2011 Elsevier Inc. Adoi:10.1016/j.ab.2011.10.041
⇑ Corresponding author. Fax: +1 336 716 0174.E-mail address: [email protected] (J. Knight).
1 Abbreviations used: BPGM, bisphosphoglycerate mucerate; IC-MS, ion chromatography coupled with masdetection; LOQ, limit of quantification; PG, 2-phosphoacid.
Glycolate and 2-phosphoglycolate (PG) are 2-carbon monocarboxylic acids with ill-defined metabolicroles. Their concentrations have not yet been described in tissues apart from body fluids and erythro-cytes. We describe the use of ion chromatography coupled with mass spectrometry (IC-MS) to quantifylevels of glycolate and PG in tissue. Sample preparation and analysis can be performed within an hour.Low concentrations of glycolate (12–48 nmol/g) and PG (4–17 nmol/g) were detected in all tissues. Theavailability of this IC-MS assay will facilitate investigations of the origin, function, and metabolism ofglycolate and PG in tissues.
� 2011 Elsevier Inc. All rights reserved.
An understanding of the origin, metabolism, and biologicalfunction of glycolate and 2-phosphoglycolate (PG)1 is lacking assuitable methods for determining their concentrations are not avail-able. All cells most likely contain glycolate as a result of the metab-olism of glyoxal by the glyoxalase system and the reduction ofglyoxylate by glyoxylate reductase as these activities are presentin all cells. Glyoxal arises from glucose autooxidation, the break-down of glycation products, and lipid peroxidation [1–3]. Liver andkidney hydroxyproline metabolism is likely to be the major sourceof glyoxylate synthesis [4].
The origin of PG in mammalian cells is not known withcertainty. In plants and some bacteria, it is synthesized duringphotorespiration following the oxygenation of ribulose-1,5,-bis-phosphate [5–7]. In all cells PG is generated as a result of DNArepair of 30-PG ends that are generated following strand breaks[8,9]. The amount of PG formed during these processes has yet tobe determined. Erythrocytes have been reported to contain a lowconcentration (2–5 lM) of PG [10], although earlier research wasunable to identify the presence of PG in these cells [11,12]. Themethod used to measure PG was not direct and relied on its abilityto activate the 2,3-diphosphoglycerate (DPG) phosphatase activityof bisphosphoglycerate mutase (BPGM). The reliability of this pro-cedure at such low concentrations of 2-PG has been questioned
ll rights reserved.
tase; DPG, 2,3-diphosphogly-s spectrometry; LOD, limit ofglycolate; TCA, trichloroacetic
[13]. The biological role of PG, if any, is not known. It has attractedattention because low levels of PG stimulate the activity of DPGphosphatase and it is the most potent modifier yet identified[14]. This activity is potentially important as the concentration ofDPG influences the binding of oxygen to hemoglobin. PG is dephos-phorylated by phosphoglycolate phosphatase, an apparent ubiqui-tous enzyme in cells of eukaryotes and prokaryotes, and in plantsthis activity is required to maintain a functional Calvin cycle[8,12,15,16].
In this report, we show that IC-MS reliably measures the con-centration of both PG and glycolate and have used this methodto measure their concentrations in a variety of tissues. This methoddoes not require extensive sample preparation, and total assaytime, including tissue preparation, can be completed in an hour.
Materials and methods
Materials
Reagent grade chemicals were obtained from either Sigma–Aldrich Chemicals (St. Louis, MO) or Fisher Scientific (Pittsburgh,PA). Sodium glycolate, 97%, and 2-phosphoglycolic acid as atri-(monocyclohexylammonium) salt, 98%, were purchased fromSigma–Aldrich.
Tissue preparation
Freeze-clamped tissue was extracted with 10% ice-cold trichlo-roacetic acid (TCA). This preparation was vortexed continuously for

Table 1IC-MS conditions used to measure glycolate and phosphoglycolate in tissue.
Glycolate 2-Phosphoglycolate
Column AS15, 2 � 250 mm,with AG15 guard
AS11-HC, 2 � 250 mmwith AG11 guard
Eluent 3 mM KOH 32 mM KOHIC flow rate (ml/min) 0.3 0.3Injection volume (ll) 10 10Cone voltage (V) 30 40Needle voltage (kV) 1.5 3.0Probe temperature (�C) 450 450
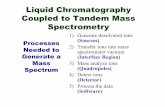
Fig.2. Phosphoglycolate SIM 155 calibration curve showing a linear SIM responsebetween 0.016 and 5 lM. Tissue levels of phosphoglycolate after TCA extraction andpreparation fall within this concentration range. Each data point representsmean ± SD, n = 4.
Table 2Glycolate and phosphoglycolate content of mouse tissues.
Tissue Glycolate(nmol/g wet wt)
Phosphoglycolate(nmol/g wet wt)
Liver 48.3 ± 4.5 12.6 ± 3.5Kidney 48.1 ± 5.6 4.3 ± 0.5Heart 23.8 ± 1.9 16.9 ± 3.9Brain 25.2 ± 2.5 5.4 ± 0.6Muscle 12.3 ± 1.1 5.9 ± 0.5Erythrocytesa 12.3 ± 2.2 10.0 ± 0.2Plasmaa 12.5 ± 2.9 0.17 ± 0.11
a The plasma levels above are presented as nmol/ml. Erythrocyte concentration ispresented as nmol/ml packed red cell lysate.
122 Glycolate and phosphoglycolate in tissues / J. Knight et al. / Anal. Biochem. 421 (2012) 121–124
1 min at 4 �C, frozen at �80 �C for 10 min to promote protein pre-cipitation, thawed, and vortexed again continuously for 1 min at4 �C. Precipitate was removed by centrifugation and TCA in thesupernatant removed by vigorously vortexing with 3 vol of 1,1,2-trichlorotrifluoroethane (FREON)-trioctylamine (3:1, vol/vol;Aldrich, Milwaukee, WI), centrifuging at 4 �C to promote phaseseparation, and collecting the upper aqueous layer for analysis.Samples were typically further diluted 2- to 10-fold in water priorto IC-MS analysis.
Ion chromatography/mass spectrometry
Glycolate and PG were quantified in tissue by ion chromatogra-phy coupled with negative electrospray mass spectrometry(IC-MS) (Dionex Corporation, Sunnyvale, CA). The IC portion ofthe IC-MS consisted of an ED50 conductivity detector, a GS50 gra-dient pump, an AS50 refrigerated autosampler, an EG50 potassiumhydroxide gradient generator, a continuously regenerated aniontrap column, an AS50 thermal compartment containing the col-umns controlled at a temperature of 30 �C, and a 2-mm ASRS 300suppressor operating with external water at 0.5 ml/min to providesuperior suppressed conductivity detection. The columns used forthe analysis of glycolate and PG are described in Table 1. The MSis a Thermo-Finnigan MSQ ELMO single quadrupole mass spec-trometer that is specifically designed for the analysis of low molec-ular weight ions (less than Mw 1000). Acetonitrile (50%), deliveredby an auxiliary pump at 0.3 ml/min, was mixed with column elu-ent via a zero dead volume mixing Tee (Upchurch Scientific, OakHarbor, WA) to improve electrospray ionization. A nitrogen gener-ator (18LA, Peak Scientific) was used to deliver nitrogen nebulizergas at 80 psi. Glycolate and PG were determined by selected-ionmonitoring (SIM) at the following mass/charge ratios, glycolate(SIM 75) and PG (SIM 155). Detailed running conditions for glyco-late and PG analysis are provided in Table 1.
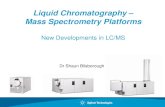
Fig.1. Phosphoglycolate conductivity (A) and mass spectrometry single ion monitorinconductivity chromatogram overlays of a 10 lM phosphoglycolate standard (dotted linSeparation of anions was done using an AS11-HC column. Panel B shows the SIM 155 reswas removed prior to IC-MS using TOA/FREON.
Results and discussion
On an AS11-HC column, PG does not coelute with other anionsin tissue extracts (Fig. 1). SIM responses at various PG concentra-tions are shown in Fig. 2. Limit of detection (LOD), defined as meanblank signal plus 3XSD blank signal, and limit of quantification(LOQ), defined as mean blank signal plus 10XSD blank signal, forPG are 6 and 25 nM, respectively. Recovery of PG in the tissuesshown in Table 2 spiked with PG at a concentration equivalent toLOQ ranged from 97% to 102%. The determination of the phospho-glycolate concentration in tissues by an independent methodwould help substantiate the validity of this method, but none arecurrently available. The incubation of PG in 32 mM potassiumhydroxide for 1 h prior to IC showed no change in PG signal, or
g (B) chromatograms of red blood cells extracted with 10% TCA. Panel A showse), and TCA-extracted red blood cells (solid line) diluted 30-fold prior to analysis.ponse of phosphoglycolate in the TCA-extracted red blood cells. The majority of TCA

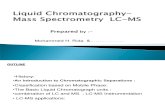
Fig.3. Separation of glycolate (2) from other major anions, including, glycerate (1), lactate (3), and formate (4) in red blood cells extracted with 10% TCA using an AS15 column(A), and quantification of glycolate by single ion monitoring in the TCA-extracted red blood cells (B). Panel A shows conductivity chromatogram overlays of a 10 lM standard(dotted line), and TCA-extracted red blood cells (solid line). Formate seen in Panel A is a product of the TCA extraction process.
Glycolate and phosphoglycolate in tissues / J. Knight et al. / Anal. Biochem. 421 (2012) 121–124 123
the presence of glycolate or phosphate, compared to a nonincubat-ed preparation, indicating that PG is not degraded in the presenceof the potassium hydroxide eluent.
In many biological matrices, including plasma and tissue, theelution of lactate on an AS11HC column suppresses the glycolatepeak which elutes just after it. On an AS15 column, glycolate elutesbefore lactate, freeing it from lactate suppression (Fig. 3). SIM re-sponses at various glycolate concentrations are shown in Fig. 4.LOD and LOQ for glycolate are 0.25 and 0.48 lM, respectively.Recovery of glycolate in the tissues shown in Table 2 spiked withglycolate at a concentration equivalent to LOQ ranged from 92%to 98%.
The PG and glycolate levels in several mouse tissues are shownin Table 2. PG was found in all tissues examined with mean con-centrations ranging from 4.3 to16.9 nmol/g wet wt. The PG levelsin human red blood cells were also measured and found to be10.0 ± 0.2 nmol/ml, similar to levels measured in mouse red bloodcells. PG was measurable in mouse and human plasma, but levelswere <0.25 nmol/ml. Glycolate was detected in all tissues at meanconcentrations ranging from 12.3 to 48.3 nmol/g wet wt. Mouseplasma glycolate levels are similar to those measured in humanplasma [17]. The results obtained assaying urinary glycolate by thismethod agree well with its determination by the more tedious pro-cedure of converting it to glyoxylate and quantifying the glyoxylateby HPLC after derivatization with phenylhydrazine [18].
This IC-MS assay should be useful in identifying the origin of PGin cells and tissues and factors that influence its concentration.Direct phosphorylation of glycolate is one possible origin of PG,but high, nonphysiological concentrations of glycolate are requiredin vitro and whether such a reaction occurs in vivo has been
Fig.4. Glycolate SIM 75 calibration curve showing a linear SIM response between0.31 and 5 lM. Tissue levels of glycolate after TCA extraction and preparation fallwithin this concentration range. Each data point represents mean ± SD, n = 4.
questioned [13,19,20]. It is possible that it is derived in animal cellsfrom the repair of DNA lesions, as Lindahl has estimated that up to10,000 purine bases are lost from DNA in every human cell dailyand subsequently repaired [21]. PG is often derived from 30-terminicreated with single-strand DNA breaks [22,23]. Thus, the measure-ment of PG may prove to be an indicator of increased damage toDNA and its associated repair. It is possible that the concentrationof intracellular PG is maintained at low levels by PG phosphatase toensure that the activities of enzymes modified by PG, includingBPGM, triose phosphate isomerase, pyruvate kinase, phosphoenol-pyruvate carboxykinase, and enolase are not affected [14,24,25].The phenotype of a KO mouse lacking PG phosphatase activity, per-haps under conditions accelerating DNA damage and repair andphosphoglycolate formation, would be of interest. In erythrocytes,PG levels may represent that formed during hematopoiesis andretained in cells following enucleation.
A biological role for glycolate has not yet been identified.Known metabolic reactions involving glycolate are illustrated inFig. 5. A major source of glycolate in most cells appears to be thedetoxification of glyoxal by the glyoxalase system [2]. A smallamount of glyoxal is produced in cells from the peroxidation thatoccurs as a result of normal metabolism [3–5]. Some glycolatemay also be produced by the reduction of glyoxylate by glyoxylatereductase (GRHPR), particularly in tissues that metabolizehydroxyproline such as the liver and kidney [1]. Our results withcultured hepatocytes have shown that there is a metabolic path-way from fructose to glycolate that is believed to arise from glycol-aldehyde production, but in vivo studies with human subjectsindicated that ingesting fructose in amounts up to 21% of the cal-ories did not alter glycolate excretion, suggesting this pathway isminor [26].
Fig.5. Pathways associated with glycolate production. (1) Aldehyde dehydrogenase,(2) phosphoglycolate phosphatase, (3) glyoxalase system, (4) glycolate oxidase, (5)glyoxylate reductase, (6) 4-hydroxy-2-oxoglutarate aldolase, (7) alanine:glyoxylateaminotransferase, (8) D-amino acid oxidase. The thicker arrows denote reactionsbelieved to have the largest fluxes.

124 Glycolate and phosphoglycolate in tissues / J. Knight et al. / Anal. Biochem. 421 (2012) 121–124
The measurement of glycolate has clinical significance as itsmeasurement in a 24 h urine collection, together with that of oxa-late, is a reliable noninvasive method for determining whether pa-tients have the rare monogenetic disease, primary hyperoxaluriatype 1 [27]. These patients have a deficiency in peroxisomal ala-nine:glyoxylate transferase activity in the liver and cannot convertglyoxylate to glycine. As a result, glyoxylate is converted to exces-sive amounts of glycolate and oxalate [1].
Acknowledgment
This work was supported by NIH Grant RO1 DK54468.
References
[1] A. Dudda, G. Spiteller, F. Kobelt, Lipid oxidation products in ischemic porcineheart tissue, Chem. Phys. Lipids 82 (1996) 39–51.
[2] P.J. Thornalley, A. Langborg, H.S. Minhas, Formation of glyoxal, methylglyoxaland 3-deoxyglucosone in the glycation of proteins by glucose, Biochem. J. 344(1) (1999) 109–116.
[3] K.J. Wells-Knecht, D.V. Zyzak, J.E. Litchfield, S.R. Thorpe, J.W. Baynes,Mechanism of autooxidative glycosylation: identification of glyoxal andarabinose as intermediates in the autooxidative modification of proteins byglucose, Biochemistry 34 (1995) 3702–3709.
[4] J.M. Phang, C.A. Hu, D. Valle, Disorders of proline and hydroxyprolinemetabolism, in: C.R. Scriver, A.L. Beaudet, W.S. Sly, D. Vallee, B. Childs, K.W.Kinzler, B. Vogelstein (Eds.), The Metabolic and Molecular Bases of InheritedDisease, McGraw-Hill, New York, 2001, pp. 1821–1838.
[5] T.J. Andrews, G.H. Lorimer, N.E. Tolbert, Ribulose diphosphate oxygenase. I.Synthesis of phosphoglycolate by fraction-1 protein of leaves, Biochemistry 12(1973) 11–18.
[6] G. Bowes, W.L. Ogren, R.H. Hageman, Phosphoglycolate production catalyzedby ribulose diphosphate carboxylase, Biochem. Biophys. Res. Commun. 45(1971) 716–722.
[7] G.H. Lorimer, T.J. Andrews, N.E. Tolbert, Ribulose diphosphate oxygenase. II.Further proof of reaction products and mechanism of action, Biochemistry 12(1973) 18–23.
[8] M.T. Pellicer, M.F. Nunez, J. Aguilar, J. Badia, L. Baldoma, Role of 2-phosphoglycolate phosphatase of Escherichia coli in metabolism of the 2-phosphoglycolate formed in DNA repair, J. Bacteriol. 185 (2003) 5815–5821.
[9] T.A. Winters, W.D. Henner, P.S. Russell, A. McCullough, T.J. Jorgensen, Removalof 30-phosphoglycolate from DNA strand-break damage in an oligonucleotidesubstrate by recombinant human apurinic/apyrimidinic endonuclease 1,Nucleic Acid Res. 22 (1994) 1866–1873.
[10] Z.B. Rose, J. Salon, The identification of glycolate-2-P as a constituent of normalred blood cells, Biochem. Biophys. Res. Commun. 87 (1979) 869–875.
[11] G.R. Bartlett, Human red cell glycolytic intermediates, J. Biol. Chem. 234 (1959)449–458.
[12] K.E. Richardson, N.E. Tolbert, Phosphoglycolic acid phosphatase, J. Biol. Chem.236 (1961) 1285–1290.
[13] S. Fujii, E. Beutler, Where does phosphoglycolate come from in red cells? ActaHaematol. 73 (1985) 26–30.
[14] Z.B. Rose, J. Liebowitz, 2,3-diphosphoglycerate phosphatase from humanerythrocytes. General properties and activation by anions, J. Biol. Chem. 245(1970) 3232–3241.
[15] J.A. Badwey, Phosphoglycolate phosphatase in human erythrocytes, J. Biol.Chem. 252 (1977) 2441–2443.
[16] S. Schwarte, H. Bauwe, Identification of the photorespiratory 2-phosphoglycolate phosphatase, PGLP1, in Arabidopsis, Plant Physiol. 144(2007) 1580–1586.
[17] J. Knight, J. Jiang, D.G. Assimos, R.P. Holmes, Hydroxyproline ingestion andurinary oxalate and glycolate excretion, Kidney Int. 70 (2006) 1929–1934.
[18] M. Petrarulo, S. Pellegrino, O. Bianco, M. Marangella, F. Linari, E. Mentasti,Derivatization and high-performance liquid chromatographic determinationof urinary glycolic acid, J. Chromatogr. 465 (1989) 87–93.
[19] S. Fujii, Glycolate kinase activity in human cells, Blood 65 (1985) 480–483.[20] H. Sasaki, S. Fujii, Y. Yoshizaki, K. Nakashima, T. Kaneko, Phosphoglycolate
synthesis by human erythrocyte pyruvate kinase, Acta Haematol. 77 (1987)83–86.
[21] T. Lindahl, Instability and decay of the primary structure of DNA, Nature 362(1993) 709–715.
[22] K.W. Caldecott, Single-strand break repair and genetic disease, Nat. Rev. Genet.9 (2008) 619–631.
[23] R. De Bont, N. van Larebeke, Endogenous DNA damage in humans: a review ofquantitative data, Mutagenesis 19 (2004) 169–185.
[24] T. Nowak, A.S. Mildvan, Stereoselective interactions of phosphoenolpyruvateanalogues with phosphoenolpyruvate-utilizing enzymes, J. Biol. Chem. 245(1970) 6057–6064.
[25] R. Wolfenden, Transition state analogues for enzyme catalysis, Nature 223(1969) 704–705.
[26] J. Knight, D.G. Assimos, L. Easter, R.P. Holmes, Metabolism of fructose tooxalate and glycolate, Horm. Metab. Res. 42 (2010) 868–873.
[27] B. Hoppe, B.B. Beck, D.S. Milliner, The primary hyperoxalurias, Kidney Int. 75(2009) 1264–1271.