
Geriatric Services in Manitoba - Long Term & Continuing ... PHIL ST JOHN... · GERIATRIC SERVICES...
79
GERIATRIC SERVICES IN MANITOBA PHIL ST JOHN LTCAM MAY, 2014
Transcript of Geriatric Services in Manitoba - Long Term & Continuing ... PHIL ST JOHN... · GERIATRIC SERVICES...

GERIATRIC SERVICES IN MANITOBA
PHIL ST JOHN
LTCAM
MAY, 2014

CONFLICT OF INTEREST DISCLOSURE
•Consultant for: None
•Speaker for: None
•Received grant/research support from: CIHR, MHRC, SIRP, Riverview Foundation
•Received honoraria from: None

KEY POINTS
• Comprehensive Geriatric Assessment (CGA) can be performed in any health care setting
• CGA has been shown to have better functional outcomes and lower rates of long term care
• In the community
• In post-acute settings
• In Acute care settings
• In spite of this evidence, it has proven difficult to attract physicians into the specialty of geriatric medicine










PERCENT OF POPULATION OVER 80

DEMOGRAPHY -SUMMARY
• There are a lot of really old people
• There likely be more



Copyright ©2005 CMA Media Inc. or its licensors
Rockwood, K. et al. CMAJ 2005;173:489-495
Fig. 1: Kaplan-Meier curves, adjusted for age and sex, for study participants (n) over the medium term (5-6 years), according to their scores on the CSHA Clinical Frailty Scale

PREVALENCE OF DEMENTIA CANADA 1991-92
Rate per 1,000
Source: Can Med Assoc J 1994;150:899-913

EPIDEMIOLOGY SUMMARY
We are amongst the healthiest people anywhere, ever
BUT – also the amongst the oldest
• Multimorbidity
• Dementia
• Frailty
• Disability

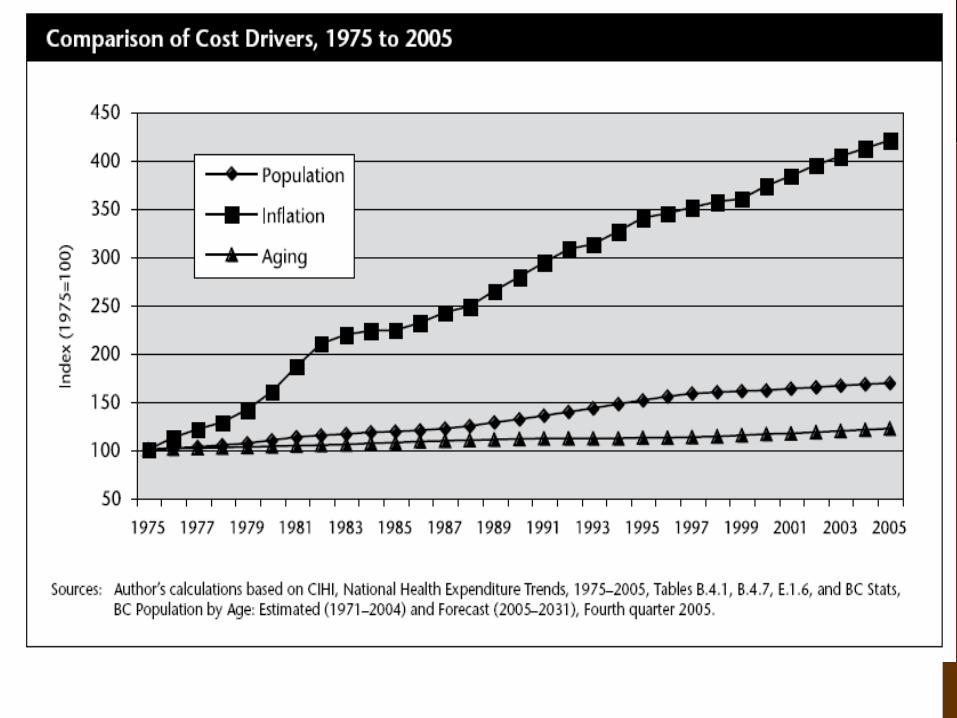
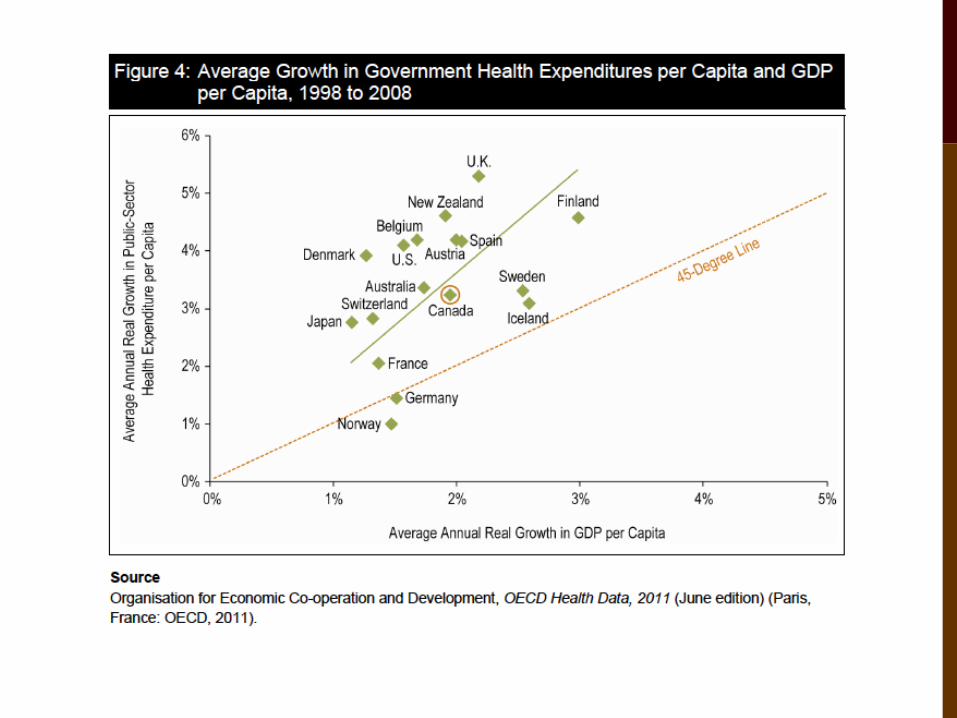
An ageing population is not the cause of health care inflation



What should we do?

GERIATRICS
Charcot first (modern) physician to describe conditions associated with old age
Term introduced in 1909 by Nascher
MARJORY WARREN
• Established the first inpatient geriatric units in the UK in 1935-48
• Attention to functional status
• Ambulation
• Physical Environment
• Team approach


Warren IOM
Advocacy/Oversight Annual report to congress
Physician Training Mandatory training
Inpatient Geriatrics
Ward
Increase in training
Emphasis on outpatient
Specialisation Should form a specialty Increase in numbers
Allied health Mandatory for nurses All Allied health
Standards Specialty certification States should set standards
Models of Care Inpatient only Should fund programmes with
proven benefit
Role expansion Encouraged
Funding Private and public sources
Income Support Should be increased
Research Urgently needed Urgently funded
Technology Low tech Should encourage new
technologies

Warren ACE HELP
Prepared Environment X X X
Specialized equipment X X X
Patient Centered Care X X X
Team Members X X X
Discharge Planning X X
Specialised ward X X
Activities X X
Early Ambulation X X X
Nutrition/Feeding X X


IN THE UK
• NHS did not take over long term care – remained under local administration
• Geriatric model of care not extended to cottages, although more LTC spots opened
• Recently, highly privatized
IN THE US
• Strong representation in some academic centres
• Strong presence in some VA systems
• Administrative roles in LTC settings
• Less widely disseminated
• Often primary care
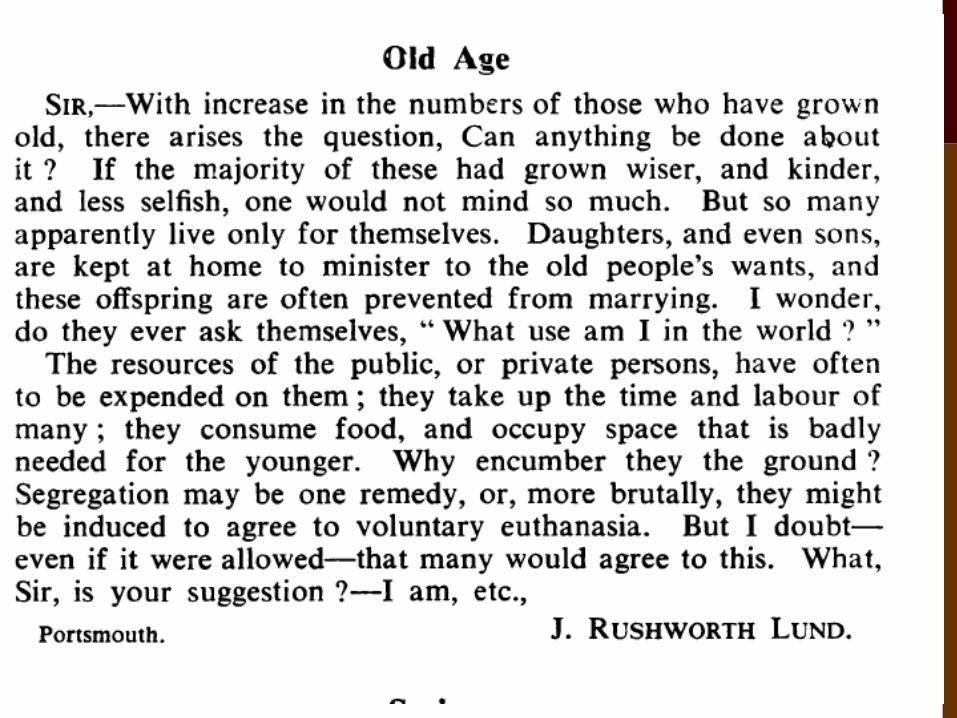
REACTION TO GERIATRICS
Other physicians “treated hear as a joke” (Tepper, 1975)
“the physicians even in her own hospital saw little value in what she was doing. It was not technical or scientific in their terms, nor did they see the importance of providing high quality care for the common but serious illnesses of this largely neglected group. Their main interest was in her ability to ‘clear their beds of chronics” (Bayne, 1977)
SINCE THEN……
The notion of Comprehensive Geriatric Assessment
A large literature to support CGA in a variety of settings


COMPREHENSIVE GERIATRIC ASSESSMENT (CGA)
A multidimensional interdisciplinary diagnostic process focused on determining a frail elderly person’s medical, psychological and functional capability in order to develop a coordinated and integrated plan for treatment and long-term follow-up.

THE GERIATRIC PROCESS Assessment
Health (diagnoses, prognosis)
Function (physical, mental)
Resources (culture, education, social, economic)
Objectives of care
What does the patient want? What is feasible?
Specify the management plan
Close the ecological gap between what the patient can do and what the environment requires
Therapeutic changes—improve the patient
Prosthetic changes—reduce environmental demands
Regular review
Is progress as expected?
Does the plan need changing?

GERIATRIC ASSESSMENT
• Evaluation and care planning by more than one professional
• Function, physical health, mental health, socioenvironmental assessment
• Performed in a wide variety of settings
• Predictors of better outcomes: targetting, intensiveness, setting

SETTINGS
• Home visits
• Clinics – referral, primary care
• Day Hospitals
• Long term care
• Acute Care of the Elderly Units (ACE)
• Geriatric Assessment (GAU or GEM)
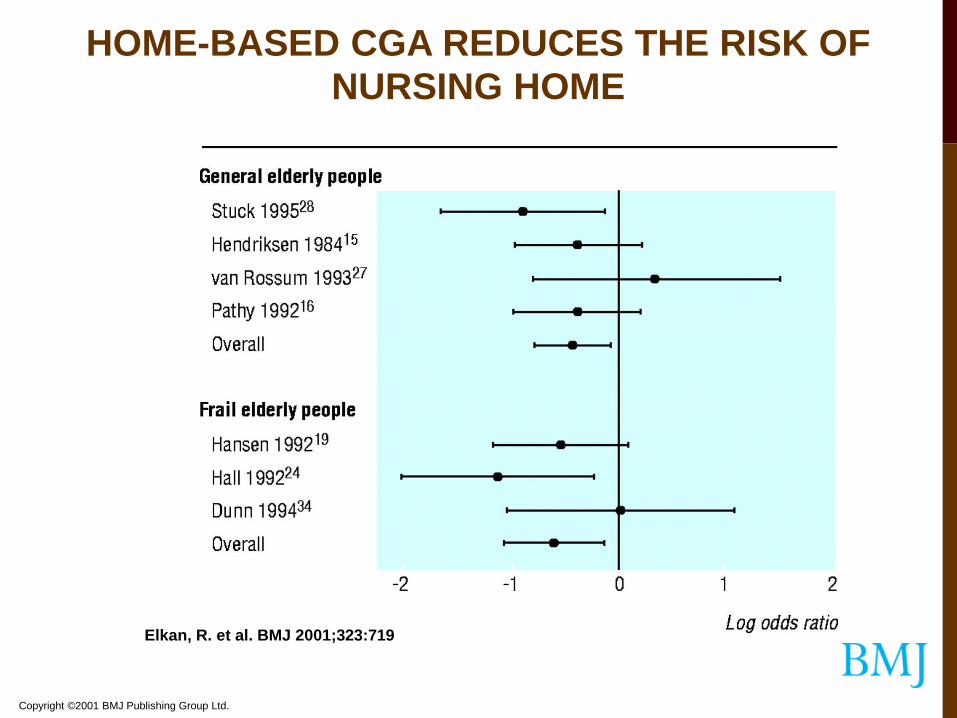
Copyright ©2001 BMJ Publishing Group Ltd.
Elkan, R. et al. BMJ 2001;323:719
HOME-BASED CGA REDUCES THE RISK OF NURSING HOME
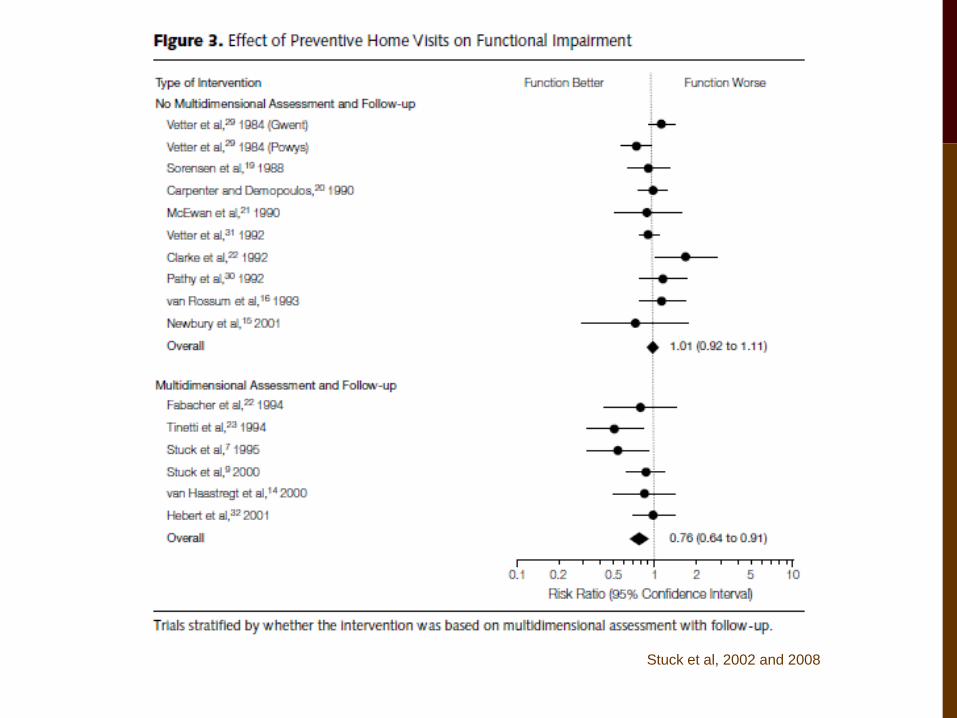
Stuck et al, 2002 and 2008

OUTPATIENT CGA HAS BETTER OUTCOMES THAN USUAL CARE
Beswick et al, Lancet, 2008

FALL PREVENTION CLINICS PREVENT FALLS

ACUTE CARE UNITS HAVE BETTER OUTCOMES THAN USUAL CARE
Baztan, BMJ, 2008


Fig 2 Odds ratios for living at home at end of follow-up (median 12 months) in elderly patients
according to comprehensive geriatric assessment after emergency admission.
Ellis G et al. BMJ 2011;343:bmj.d6553
©2011 by British Medical Journal Publishing Group

Fig 3 Odds ratios for death or deterioration at the end of follow-up (median 12 months) in
elderly patients according to comprehensive geriatric assessment after emergency
admission at baseline.
Ellis G et al. BMJ 2011;343:bmj.d6553
©2011 by British Medical Journal Publishing Group


GERIATRICS IN CANADA
• Evolved differently in different provinces
• Generally, established by itinerant geriatricians from the UK or Canadians who trained in UK
• First training programmes in the 1980s

Hogan et al, CGJ, 2012

MANITOBA
• First University section of Geriatrics in Canada (MacDonell)
• Second and third inpatient units in Canada
• First Geriatric Day Hospital

SERVICES OFFERED (HOSPITAL BASED):
Rehabilitation (Inpatient):
• Acquired Brain Injury, Stroke
• Amputee, Neuro-Musculoskeletal (NMSK; <65 y.o.) Spinal Cord Injury
• Geriatric
• General Rehab: Orthopedic
Chronic Care:
• General
• Specialized: Neuro, Respiratory, Peritoneal Dialysis
Ack: M Graceffo, D Strang

GERIATRIC REHABILITATION INPATIENT UNITS
• Central Waiting List Coordination (access)
• Consultation Services:
• Clinicians &/or Physicians at all 6 acute care sites
• Clinical Nurse Specialists ( Geriatrics)
• Deer Lodge Centre, St Boniface General Hospital, Health Sciences Centre

SITES AND VOLUMES – INPATIENT UNITS 2010/11
Sites
Deer Lodge Centre - 64 beds
Riverview Health Centre - 29 beds
St. Boniface General Hospital - 40 beds
Seven Oaks General Hospital- 76 beds

SERVICES OFFERED:
Outpatient:
• Day Hospitals:
• Deer Lodge
• Riverview
• St Boniface (SBGH)
• Seven Oaks (7OGH)
• Health Sciences Centre (HSC – primarily Amputee/SCI)

DAY HOSPITALS:
•Multiple disciplines available to assess and treat patient specific issues
•Core programs (Fall Prevention/CGA/Transition/non-specific)
•Clients attend for the day- 1-2 X/ week
•Transportation cost/round trip
•Education and Counseling
•Link with resources to remain in community

DAY HOSPITAL REFERRALS:
•Family physician referral
•Require two or more disciplines’ service
•Refer to the individual Day Hospitals- future plans for Central Coordinated Entry database

PRIME
•PRIME: A Health Centre for Seniors
•opened Deer Lodge Site March 2009
•For seniors with very complex needs to avoid hospital & personal care home placement
•Second site at Misericordia has been announced and building commenced

SERVICES OFFERED:
Outreach:
• Geriatric Program Assessment Teams:
• Community/ ER based
• Geriatric Mental Health Teams:
• Community/ Personal Care Home based

COMMUNITY OUTREACH: VOLUMES – 2010/11
Service Outreach Referrals/yr
Geriatric Program
Assessment Teams
2288
Geriatric Mental
Health Teams
1413
Rehab & Geriatric
Clinicians
1921

GPAT CRITERIA:
• The frailest, at-risk elderly, 65+ years.
• Complex health concerns affecting their ability to function.
• Geriatric Issues including: Mobility/falls, functional/ADL problems, Continence issues, Confusion, Depression, Social Support issues, Medication problems

GERIATRIC MENTAL HEALTH ELIGIBILITY:
• 65 or older with 1st onset Mental Illness
• 65 or older with history of Mental Illness-disease and aging process- GMH service
• 65 with behaviour/MH symptoms or cognitive issues related to aging
• Dementia with behavioural issues, mood disorders, Anxiety, Psychotic disorders or Personality disorders

ED- 807 (35%)
Physician- 480 (21%)
Home Care- 359 (16%)
Community Professional-
34 (6%)
Lay Person- 353 (15%)
Inpatient- 155 (7%)
GPAT Referral Sources

ED- 89 (6%)
Physician- 251 (18%)
Home Care- 355 (26%)
Community Prof- 136
(10%)
Lay Person- 188 (14%)
PCH- 362 (26%)
GMHT Referral Sources

HOW TO COORDINATE THIS THEN?
• R&G Centralized Wait List (W/L):
• Appropriate screening is completed by program consultants and teams prior to placement on W/L
• Facilitates access and movement of all Geriatric Rehabilitation inpatients and Day Hospital patients to 1st available service/bed
• Rehab Geriatrics Intake Tracking System
• Web-based application provides “read only” access for many stakeholders
and manages outreach referrals
• Referrals are received at a single place for the outreach services (GPAT and
GMH)

GAPS IN SERVICE
• ACE units
• Proven superior to usual hospital care
• Not enough geriatricians to develop
• Sub-acute care
• No formal service in WRHA for this patient population
• Under-use of Geriatric Rehab Units/GEMU model
• Problems with interface with ER, Medicine, also Geriatrician staffing
• Rural Regions
• PCHs

GAPS IN SERVICE
Formal community dementia care
• Provincial Alzheimer Strategy in ~2000
• Limited uptake with recommendations until recently
• PIECES training for LTC staff needs to be extended to acute care hospitals as well
• 1st Link Alzheimer Society funding recently announced

CONCLUSIONS
• There is an increasing number of older adults
• Most older adults are well, BUT the very old have an increased risk of multimorbidity, frailty, and cognitive decline
• CGA has been shown to be a superior model of care than usual care for these people
• It is has proven difficult to deliver this model of care