GENERAL SET
21
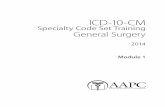
GENERAL SET Figure 23 : General Set BIL ITEM QUANTITY 1. Instrument Tray 1 2. Kidney Dish 3 3. Gallipot 4 4. Backhaus towel clip 8 5. Sponge holder 4 6. Scssor’s:- Mayo’s straight 14cm and 17cm Mayo’s curved 15cm Metzenbaum curved 2 1 1 7. B/P Handle - size 4 - size 5 2 1 8. 1 st Mayo’ pin:- Halstead Delicate Artery Forceps Crile Artery Forceps 8 8 9. 2 nd Mayo’ pin:- Babcock tissue forceps Allis tissue forceps Littlewood tissue forceps Duvals tissue forceps Spencer well artery forceps,straight Needle holder Yaunker sucker Pool sucker Sucker tubing – long 2 2 2 2 2 3 1 1 1 10. Dissecting forceps:- Mc Indoe Gillies Medium toothed 1 1 1
-
Upload
mageclairesky -
Category
Documents
-
view
246 -
download
0
Transcript of GENERAL SET

GENERAL SET
Figure 23 : General Set
BIL ITEM QUANTITY1. Instrument Tray 12. Kidney Dish 33. Gallipot 44. Backhaus towel clip 85. Sponge holder 46. Scssor’s:-
Mayo’s straight 14cm and 17cm Mayo’s curved 15cm Metzenbaum curved
211
7. B/P Handle - size 4- size 5
21
8. 1st Mayo’ pin:- Halstead Delicate Artery Forceps Crile Artery Forceps
88
9. 2nd Mayo’ pin:- Babcock tissue forceps Allis tissue forceps Littlewood tissue forceps Duvals tissue forceps Spencer well artery forceps,straight Needle holder Yaunker sucker Pool sucker Sucker tubing – long
222223111
10. Dissecting forceps:- Mc Indoe Gillies Medium toothed Medium non toothed Waugh toothed Waugh non toothed
111111
11. Retractor:- Small Langenback Medium Langenback
1 Pair1 Pair

Morris 1Pair12. Mc Donald Dissector 113. Dennis Brown 114. Raytex gauze – 10 pieces per bundle 2 bundles

TOTAL ABDOMINAL HYSTERECTOMY EXTRAS SET
Figure 24 : TAH extra
BIL ITEMS QUANTITY1. Instruments tray 12. Deavers retractor 23. Scissors :-
Mayo uterine Straight 9”
11
4. Dissecting forceps:- Toothed Non toothed
11
5. Mayo’ pin :- Kocher curved tissue forceps Kocher straight tissue Littlewood tissue forceps Teale vulsellum forceps
6662
6. Balfour Abdominal Retractor with centre blade 17. Gynae pad 1

LAYOUT OF THE INTRUMENT The scrub nurse arrange the instruments and accessory items on mayo stand and instrument
trolley. The circulating nurse open the packages of sterile supplies such as diathermy flex with pin, light handle, sutures and blade.
She flip the blade packet from over wrap into the kidney dish, then she opened the light handle packages and diathermy pin. Scrub nurse take contents from wrapped open and avoid touch the unsterile outer wrapper.
Figure 25 : Layout instrument on the instrument trolley
The scrub nurse put the blades on the bard parker handle using spencer well never use finger alone. Holding the cutting edge down and away from eyes or anybody. Grasp the blade at its widest, strongest part, and slip the blade into groove on the knife handle.
Figure 26 : Layout the instrument on the Mayo stand

A click indicates the blade is in the place. To prevent damage the blade, the instrument must not touch the cutting edge. The scrub nurse fix the diathermy pin.
The circulating nurse pour the povidone iodine 10% into the gallipot for skin preparation. The scrub nurse put 3 pieces of the gauze into the gallipot without touching the solution because the solution is not sterile and the glove can be contaminate.the scrub nurse ready for arrival of the surgeon.
The surgeon request for a catheter to insert the CBD to Mdm Aini. The circulating nurse prepare the set for the catheterization.
The circulating nurse open the outer layer of the catheterization set, then the scrub nurse open the inner layer of the set.
Circulating nurse pour the Hibitine in Aques, water and K-Y jelley. She also gives the catheter size 18FR and syringe 10cc for syringe out the water. Then, she assist in any way possible.
After catheterization is over, Mdm Aini was put back on supine position.
The scrub nurse put the inactive plate at the Right thigh muscle. It should be as closed as possible to site of incision to minimize current through the body.
The plate should cover as large of patient’s skin as possible in an area free of hair, scar tissue, which tend to act as insulation.

OPERATION PROCEDURE
Figure
When the scrub nurse ready for assisting the surgery, the scrub nurse give the surgeon one gauze to wipe off the povidone iodine from incision site and surgeon will discard the gauze into the clinical waste receptacle.
The scrub nurse passed the blade size 23 in the kidney dish to surgeon to make skin incision to avoid accidentally cut. The blade were put at the edge of the trolley because the skin is not sterile and the blade consider contaminated. Then the scrub nurse give two gauze one for the surgeon, one for the assistant.
The surgeon made a Pfeannenstiel skin incision. The first cut should extent well into the subcutaneous layer, these were then separated with the knife down to the rectus sheath.

Figure 35
At the same time, the circulator documented the operating time start into the Swab Count Form.
Figure 36
Small vessel in the subcutaneous layer bleed and surgeon diathermized using dissecting forcep.
Figure 37

The full depth of the fat was incised down to rectus sheath but only in about the central 3 or 4 cm of the skin wound this is done with one stroke of the scaple with the left hand steadying in the wound area so that there is no sideways slip.
Figure 38
The rectus sheath is cut transversely, exposing the rectus and the paramidalis muscle.
Figure 39
Freeing anterior rectus sheath from underlying muscles. The sheath is release in an upwards direction with mayo scissor cuts as shown and the recti muscles fall back from the raise sheath.

Figure 40
The rectus muscles are cut transversely. The deep epigastric vessels are ligated and cut. Transversalis fascia is exposed. The assistant use the 1/2 “ langenback to exposed it.
The transversalis and peritoneum are cut transversely. Care was taken at the lower end of the wound to be sure that the gut or bladder was not injuired.
The taut fold was palpated between forefinger and thumb before incision to exclude the presence of underlying structures.
Figure 41
When the peritoneal cavity was opened, scrub nurse take all the loose gauze away and removed from the operation site. Swab on stick and abdominal pack was used instead.
Once the uterus was identified, the Balfour Retractor was used to ensure adequate exposure and scrub nurse gave 2 warm saline abdominal pack to surgeon to pack of the guts thus gave better exposure to work on the uterus. The abdominal pack were marked with crile artery forceps that clamped at the tape attached. This is to ensure the correct count.

Then the surgeon ask the anesthetist and inform the circulator to put the patient in trendelenburg position to provide better visualization of the pelvic cavity. At the same time circulating nurse and scrub nurse make sure that Mayo tray not touch patient’s leg and patient in good body alignment.
The scrub nurse watch operation field and try to anticipate the surgeon’s needs. She must be one step a head of the surgeon in passing the instrument, sutures and sponges. The scrub nurse passes the instrument in a decisive and positive manner. The tip is visible, hands is free. Handle was placed directly into surgeon palm.
Figure 42
Figure 43 Kocher Curved and Straight
The surgeon elevate the uterus, then the scrub nurse gave 2 curved kocker artery forceps one by one with handle placed firmly and directly into surgeon hand. The kocker forcep is to clamp the round ligament near uterine cornu and followed by the mayo curved scissor to cut . The scrub nurse passed the safil 1 Taper Cut Needle to ligate a short distal lateral to the clamp. Assistant

ready to cut suture with suture cutting scissors. One end of the suture was held with the crile artery forceps while the other strand was cut. This was done one side at a time. Curved kocker artery forceps was then handed to assistant, thus opening up the anterior leaf of the broad ligament. While passing the instrument scrub nurse hold the instrument by hinge.
Figure 44
The forcep on the uterine remnant of the ligament were left there which allow a means of traction to exposure. The posterior leaf of the broad ligament was pushed forward through the opening of the anterior leaf with the surgeon. It was then incised with metzenbaum scissors to create opening.
To removed the tube and ovary the infundibulo pelvic ligament was clamp with curved kocker artery forcep on the ovarian side and lateral side with one more curve kocker artery forcep. Then the scrub nurse give curved mayo scissor to cut the ligament. The same was done to the other side. The ligament were transfixed with Safil 1 suture.
Figure 45
While assisting, the scrub nurse still do the same thing such as give the instrument to the surgeon with the handle was placed into surgeon palm firmly, maintain the aseptic technique and keep talking to a minimum to avoid contamination.

Figure 46
The anterior utero vesical fold was incised using the metzenbaum scissor aided by waught non toothed dissecting forceps. Holding the peritoneum covering the bladder with the dissecting forceps the curved scissor are used to separate the bladder off the front of the lower uterus and cervix in direction of the arrow. Surgeon do not favour the method of using a gauze on finger or swab on the stick to push the bladder down, because it is liable to result in tearing of weak bladder wall.
The uterine arteries running close to the uterus along its lateral wall was clamp with curved kocker forceps, then cut with Mayo scissor and transfixed with Safil 1 suture.
The circulating nurse give the suture and the scrub nurse take the suture pocket opened and held by circulating nurse. The scrub nurse clips the neelde – needle holder and gives to surgeon. The surgeon suturing the stump using suture and tie technique.

Figure 47
The cardinal ligaments or the transverse cervical ligament was now clamped, cut and sutured with Safil suture. This was done by placing the straight kocker artery forceps parallel to the cervix, squeezing the paracervical tissue off the cervix to give the most lateral room and protection to the uterus. Since the blood supply had been controlled a single clamp suffices and the incision was made. The same was done for the other side.
Once the opening of the vaginal vault was made, Septic Towel Technique was practiced. This was to prevent contamination of spillage to other surrounding tissue and organs in the peritoneal cavity and also soiling of sterile drapes and other instruments.
After the surgeon had identify the vagina and make sure the bladder was mobilized from the cervix and vagina, a knife was plunged into the anterior fornix. The vaginal vault was incised and

Figure 48 Uterine scissors
cut with uterine scissor. Littlewood tissue forceps were applied on the edges of the vaginal vault one at a time while the surgeon continued to cut the vaginal vault until the uterus was removed.
Figure 49

Figure 50 : Littlewood
Scrub nurse get ready to receive the specimen together with the forceps attached and put on top of sterile towel placed earlier. This is to avoid contamination to the sterile area.
The circulating nurse put on the glove and get ready to receive the specimen. The scrub nurse confirmed with the surgeon type of specimen gives it to the circulating nurse, avoiding from touching the circulating nurse’s glove hand.
Figure 51
Prior to the closure of the vaginal vault, blades, sutures and swab were counted by the scrub nurse with the circulating nurse to confirm the correct number.

Figure 52
The vaginal vault was sutured with Vicryl 1 suture. The corner of the vaginal vault were tied off with the cardinals and round ligaments to give support.
Figure 53
The instrument used on the vaginal vault were considered contaminated. They were littlewoods forcep, toothed dissecting forcep, uterine scissors, knife, needle holder, suture scissor, yaunker sucker and sutures.
They were all receive in the kidney dish and when the vaginal vault was closed, scrub nurse wrap the kidney dish with the towel that put earlier and gave to the circulating nurse who were ready to receive the things. The circulating nurse lay out the instrument on the floor for counting purpose.
The surgeon checked for bleeding points and diathermized using dissecting forcep. Before close the peritoneum, patient was put back in supine position.

Two abdominal pack put earlier in the peritoneum cavity was taken out. Balfour self retaining retractor also removed.
Then, the scrub nurse start to counting the sponges, atraumatics needles and instrument with the circulating nurse. All the sponges, needles and instrument count were found correct and the surgeon was noted and he acknowledged the scrub nurse.
The circulating nurse bring the swab count form during the counting and documented immediately.
The surgeon request for the drainage tube. The scrub nurse put the blade size 23 in the kidney dish and pass it to the surgeon to make the incision at the right abdomen to insert size D portex drain with 3 holes and put back the blade into the kidney dish to prevent injury during passing the blade either to the surgeon or scrub nurse. The surgeon used Fraser Kelly Artery Forcep to pull the drainage tube outside the abdomen. The drainage tube was anchored with Silk 2/0 Cutting Needle by assistant.
4 crile artery forcep were used to hold the rectus sheath during closing the peritoneum. The surgeon used Safil 1 Taper Cutting Needle to close the peritoneum and assistant wait with suture cutting scissor in the hand for cutting. Then, surgeon used the Safil 1 for closing the rectus sheath.
Figure 54
The scrub nurse start to count gauze, abdominal pack, needles, sharp instrument and all instruments that uses during operation side to mayo tray, instrument trolley and finally on the floor with the circulating nurse. The count must be tally with the Swab Count Form. It to avoid any of them left inside patient and injured her.
Before closed the skin, the scrub nurse perform the final count with the circulating nurse and documented in the Swab Count Form assure that swabs , needles and instrument used were correct.
The surgeon used the Monosyn 3/0 to closed the skin. During skin closure, key hole opsite dressing was prepared to put on the drain site. At the same time, scrub nurse dissemble blade from B/P handle. Discard the blade into adhesive pack, then put sharp instrument in the kidney dish.
After skin closure had finished, the scrub nurse get ready 2 pieces of gauze, 1 gauze soaked with normal saline and 1 gauze dry. The scrub nurse put the soaked gauze into the incision, roll it up from one side to a side. Then scrub nurse protect the wound with the dry gauze. The soaked gauze was used to clean the surrouding area around the incision and followed by dry gauze.

The scrub nurse applied the dressing at the wound and key hole at the drain site and plastered with hyperfix dressing. The portex drain was connected to a urine bag. After applying the dressing, the scrub nurse took the towel clips from the drapes. The nurse removed the drapes with roll it to prevent sparking and air borne contamination and put into the linen bag.
The circulating nurse switch off the operating light, suction apparatus and diathermy machine. She disconnected the sucker tubing and removed the inactive dispersive plate. The nurse checked the sign and symptom of burn at the skin where the inactive dispersive plate was placed and the skin looked normal.
The scrub nurse push away the Mayo stand and the instrument trolley from the operating table. The scrub nurse wet the extra gauze for removing the excess povidone iodine 10% from skin patient. The circulating nurse cover the patient with warmed blanket to provide hypothermia and avoid unnecessary expose the patient.