Gastroesophageal Reflux Disease: The Burn that …...•Gastroesophageal reflux disease is a common...
59
Gastroesophageal Reflux Disease: The Burn that Burns Geoff S Williams, MD, FRCPC Associate Professor of Medicine Division of Gastroenterology Dalhousie University
Transcript of Gastroesophageal Reflux Disease: The Burn that …...•Gastroesophageal reflux disease is a common...

Gastroesophageal Reflux Disease: The Burn that Burns
Geoff S Williams, MD, FRCPC
Associate Professor of Medicine
Division of Gastroenterology
Dalhousie University

Disclosures
• I was paid an honoraria by pharmaceutical company Takeda to develop educational materials for family doctors
• The educational materials were accredited

Objectives
• At the end of this session the learner should:• Be able to explain the difference between physiologic and pathologic reflux
• Be able to describe the appropriate treatment strategy for GERD
• Be able to describe the ‘red flags’ that may suggest a need for endoscopy
• Appreciate the complexities in diagnosing reflux that does not respond to typical therapies.

The case of Jonathan Milsap
• 56 year old lawyer
• PMH: Dyslipidemia and hypertension
• He has been suffering retrosternal burning 3 – 4 times per week, and regurgitates food into his mouth once per week on average
• He has had these symptoms for over 10 years, but they seem to be getting worse
• His BMI is 35
• He does not smoke
• His father died of a heart attack

Questions about Jonathan Milsap’s case
• Is this GERD?
• Could this be a heart attack???????
• How would we investigate?
• If it is GERD, how do we treat him?
• Is he at risk for complications?

GERD vs Myocardial Infarction
• GERD
• Burning quality
• No shortness of breath
• Radiates up to neck
• Often occurs after eating
• Relieved with antacids
• Myocardial infarction
• Chest pressure
• Shortness of breath
• Can radiate into jaw and down left arm
• Often occurs after exertion
• Relieved with nitroglycerin

Let’s start with definitions: heartburn and regurgitation• Heartburn is the sensation of
burning in the retrosternal area, typically manifested after eating
• The burning sensation is thought to be secondary to acid exposure to esophageal mucosa
• Regurgitation is the perception of acid or food products into the mouth

Gastric acid
• Plays a role in absorption of • Proteins
• Iron
• B12
• Calcium
• Role in killing ingested microorganisms

Physiologic reflux vs GERD
• PHYSIOLOGIC
• Post prandial
• Short lived
• No symptoms
• Rarely have nocturnal symptoms
• PATHOLOGIC
• May occur anytime
• Mucosal injury
• Symptomatic
• Nocturnal symptoms common

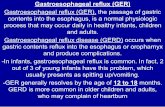
Upper digestive tract anatomy

Causes of GERD
• Most people believe heartburn is related to foods they eat
• Pathophysiologic factors:• Reduced saliva production• Transient lower esophageal sphincter relaxations• Decreased LES tone• Decreased gastric emptying (eg. Gastroparesis)• Hiatal hernia
• Conditions that predispose:• Certain foods: Fat, caffeine, peppermint, alcohol• Smoking• Pregnancy• Obesity

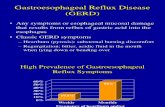
Hiatal hernia

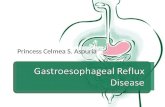
How common is GERD?
• 10 – 20 % of people in ‘western world’ suffer GERD
• Likely an underestimate, as only typical symptoms of GERD considered in most studies
• Significant impact on quality of life
• Prevalence of GERD and its complications increasing over time (despite improvements in medical therapies)

Symptom profile: typical vs atypical
• Classic symptoms
• Retrosternal burning
• Regurgitation of food
• Atypical symptoms
• Coughing
• Sore throat
• Laryngitis
• Throat clearing
• Waterbrash

Challenges with diagnosis

Diagnosing the problem
• Uncomplicated GERD is diagnosed with treatment!
• In setting of standard symptoms, Canadian Association of Gastroenterology recommends 8 week trial of once daily proton pump inhibitor once daily, 30 minutes before breakfast
• Resolution of symptoms ‘confirms’ diagnosis and treatment is then tapered to minimal treatment required to control symptoms

Other diagnostic tests
• Barium swallow
• Upper endoscopy
• 24 hour pH study
• Esophageal manometry

Barium swallow
• Barium is radiopaque and easily seen with x-ray technology
• slurry swallowed by the patient and video recording obtained
• Reflux is determined if barium is seen entering stomach and then reentering the esophagus
• Limited usefulness

24 hour pH testing – the gold standard

Esophageal manometry
• Small probe inserted through the nose and advanced into the stomach
• Measures pressures within the esophagus
• Patient given water to swallow and pressure recordings are taken

Endoscopy

Endoscopy benefits and risks
• Benefits
• Direct visualization of the mucosa
• Allows for tissue sampling
• Allows for therapeutic intervention (eg. Dilating a stricture)
• Risks
• Sedation required
• Bleeding (1/1000)
• Perforation of hollow organ (1/1000)
• Infection (1/1000000)
• Expensive
• Long wait lists

Who needs endoscopy?
• Weight loss
• Difficulty swallowing (dysphagia)
• Painful swallowing (odynophagia_
• Upper GI bleeding
• Iron deficiency anemia
• Vomiting
• First degree relative with esophageal cancer

What do we find at endoscopy for heartburn?

Complications of GERD
• Esophagitis
• Esophageal strictures
• Barrett’s esophagus
• Esophageal adenocarcinoma

The LA Classification

LA Class A

LA Class B

LA Class C

LA Class D

Esophageal strictures

Hurst
Maloney
Savary
Endoscopic Dilation
Balloon dilators





Barrett’s esophagus
• Longstanding exposure of the esophageal mucosa to acid results in a compensatory change in the cells (termed metaplasia)
• They esophageal mucosa which is normally ‘squamous’ cells becomes specialized intestinal cells
• Barrett’s esophagus increases risk of esophageal adenocarcinoma 30 fold
• Risk is up to 3 % per year

Endscopic findings in Barrett’s esophagus

Risk factors for Barrett’s esophagus
• Age 50 years or older
• ●Male sex
• ●White race
• ●Chronic GERD
• ●Hiatal hernia
• ●Elevated body mass index
• ●Intra-abdominal distribution of body fat

Concern with Barrett’s esophagus

Esophageal adenocarcinoma

Esophageal adenocarcinoma
• Most patients develop difficulty swallowing (dysphagia)
• Can also have weight loss, GI bleeding
• Prognosis depends on stage of the disease


Treating GERD
• Lifestyle
• Medications
• Endoscopic therapies
• Surgery

Treatment begins with lifestyle
• Evidence supports these recommendations:• Weight loss in those with GERD who are overweight or recently gained weight
• Raising the head of bed 6 – 8 inches with wooden blocks under head of bed or foam insert (for nocturnal symptoms)
• Avoid eating 4 hours before bedtime, and lying down after eating
• Evidence lacking, but physiologically makes sense:• Avoid foods that weaken the lower esophageal sphincter pressure (caffeine,
peppermint, fatty food, carbonated beverages, smoking and alcohol)
• Abdominal breathing exercises to strengthen the anti-reflux barrier
• Avoid tight fitting garments

Antacids: the cornerstone of therapy
• Calcium antacids
• Alginates
• Pepto bismol
• Histamine receptor blockers
• Proton pump inhibitors

The proton pump inhibitor: mechanism of action

The PPIs you know
Drug name Marketing name Dose Duration of action
Omeprazole Losec 20 mg , 40 mg Less than 24 h
Esomeprazole Nexium 40 mg Less than 24 h
Pantoprazole Pantoloc 20 mg , 40 mg Less than 24 h
Rabeprazole Pariet 10 mg, 20 mg Less than 24 h
Lansoprazole Prevacid 15 mg, 30 mg Less than 24 h
Pantoprazole sodium Tecta 40 mg 24 hours
Dexlansoprazole Dexilant 30 mg, 60 mg 24 hours

Are PPIs safe?
• Microscopic colitis
• Clostridium difficile colitis
• Osteoporosis
• Malabsorption of magnesium, iron, B12, calcium
• Kidney disease
• Dementia
• Pneumonia
• Drug induced lupus
• Mortality

Risk taken in context
• Most studies defining risk are Retrospective Cohort studies
• Suggest possible association but cannot conclude cause-effect relationship
• Risks may be real, therefore, PPIs should be prescribed:• 1. For appropriate indication
• 2. For appropriate period of time
• 3. Use lowest dose that controls symptoms
• 4. Can monitor calcium, Magnesium, B12, iron, renal function, etc.

PPIs and refractory GERD
• Term ‘refractory GERD’ refers to patients who do not have an adequate response to 8 week therapy with PPI medication
• Patient driven diagnosis
• 25% of patients will require twice daily PPI to control symptoms
• 90% of patients who do not respond to twice daily PPI have normal endoscopy

Putative mechanisms for failure of proton pump inhibitor (PPI) treatment• Compliance
• Improper dosing time
• Weak acidic reflux
• Duodenogastroesophageal/bile reflux
• Esophageal hypersensitivity
• Delayed gastric emptying
• Psychological comorbidity
• Concomitant functional bowel
disorder
• Reduced PPI bioavailability
• Rapid PPI metabolism
• PPI resistance
• Nocturnal reflux
• Helicobacter pylori infection status
• Eosinophilic esophagitis
• Functional heartburn
Fass R. Am J Gastroenterol 2009; 104:S33 -S38.

Algorithm for refractory GERD
Katz P et al. Am J Gastroenterol. 2013;108(3):308-328

Endoscopic therapies

Endoscopic therapies

Surgical options

Surgical options: Nissen fundoplication

Summary
• Gastroesophageal reflux disease is a common clinical modality and most patients can be diagnosed and managed by trial of proton pump inhibitor medication
• Complications are uncommon but can be serious (GI bleeding, stricture formation, Barrett’s esophagus and esophageal adenocarcinoma
• Important to recognize the ‘red flags’ which suggest need for endoscopy
• Endoscopic and surgical treatments are available but rarely required to manage GERD