MS - Gastroesophageal Reflux Disease
15
Princess Celmea S. Aspuria
-
Upload
phantasm-darkstar -
Category
Documents
-
view
85 -
download
1
Transcript of MS - Gastroesophageal Reflux Disease

Princess Celmea S. Aspuria

Gastroesophageal reflux disease (GERD), gastro-oesophageal reflux disease (GORD), gastric reflux disease, or acid reflux disease is chronic symptoms or mucosal damage caused by stomach acid coming up from the stomach into the esophagus


CLINICAL MANIFESTATIONS• Pyrosis (burning sensation in the esophagus)• Dyspepsia (indigestion)• Regurgitation• Dysphagia or odynophagia (pain on swallowing)• Hypersalivation• Esophagitis


ASSESSMENT AND DIAGNOSTIC FINDINGS• Endoscopy or barium swallow : used to evaluate
damage to the esophageal mucosa• Ambulatory 12 to 36-hour esophageal pH monitoring :
used to evaluate the degree of acid reflux• Bilirubin monitoring (Bilitec) : used to measure bile
reflux patterns Exposure to bile can cause mucosal damage


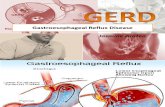
GERD is caused by a failure of the cardia. In healthy patients, the "Angle of His"—the angle at which the esophagus enters the stomach—creates a valve that prevents duodenal bile, enzymes, and stomach acid from traveling back into the esophagus where they can cause burning and inflammation of sensitive esophageal tissue.

Factors that can contribute to GERD:• Hiatal hernia, which increases the likelihood of GERD
due to mechanical and motility factors.• Obesity: increasing body mass index is associated with
more severe GERD• Zollinger-Ellison syndrome, which can be present with
increased gastric acidity due to gastrin production• Hypercalcemia, which can increase gastrin production,
leading to increased acidity

• Scleroderma and systemic sclerosis, which can feature esophageal dysmotility
• Visceroptosis or Glénard syndrome, in which the stomach has sunk in the abdomen upsetting the motility and acid secretion of the stomach.


MANAGEMENT• Teach patient to avoid situations that decrease lower
esophageal sphincter or cause esophageal irritation• Instruct patient to eat a low fat diet, avoid caffeine,
tobacco, beer, milk , foods containing peppermint or spearmint, and carbonated beverages
• Avoid eating or drinking 2 hours before bedtime• Maintain normal body weight• Avoid tight-fitting clothes

MANAGEMENT• Elevate head of the bed 6-8inches and elevate upper
body on pillows• If reflux persists, antacids or H2 receptor antagonists
such as famotidine (Pepcid), nizatidine (Axid), or ranitidine (Zantac), may be prescribed
• Proton pump inhibitors (medications that decrease the release of gastric acid, such as lansoprazole (Prevacid) or rabeprazole (Aciphex) may be used

MANAGEMENT• The patient may receive prokinetic agents, which
accelerate gastric emptying. These agents include bethanechol (Urecholine), domperidone (Motilium), and metoclopramide (Reglan). Metoclopramide has central nervous system complications
with long-term use.

MANAGEMENT• If medical management is unsuccessful, surgical
intervention may be necessary. Surgical management involves a fundoplication (wrapping of a portion of the gastric fundus around the sphincter area of the esophagus). Fundoplication may be performed by laparoscopy.