GAIT ABNORMALITIES IN FUNCTIONAL PROBLEMS OF THE …bsphs.org › wp-content › uploads › 2017...
5
48 Medical University- Plovdiv, Medical College, Bulgaria, 120Buxton Bros. 4004 Plovdiv Introduction Gait is a complex stereotyped and auto- mated motor activity, which allows for move- ment of the body in an upright position. It consists of several components: 1. Keeping the body upright. It is imple- mented by antigravity reflexes that keep body and head upright and limbs in extension [1]. These reflexes depend on proprioreception, which gives information about the position of the limbs, a sense of stepping down and so on. Anti-gravity reflexes may be increased patho- logically in the so called decerebration - increased muscle tone of the body and limbs extensors. It occurs when the brainstem is blocked at the level of the mesencephalon and bulbar nucleus [2]. 2. Stereotypical, automated sequential motor acts related to the movement of the body. This is a complex reflex activity that is activated by the consistent contact of the foot with the ground and allows the body to move forward. Gait is a conscious and volitional motor activity [3]. 3. A complex coordination action during body movements, to maintain the center of grav- ity by adjusting muscle tone of the extensors and flexors. Vestibular-cerebral reflexes, proprio receptive reflexes and neocerebral activities are important for the realization of a normal gait [4]. 4. Auxiliary motor actions (synkinesis). These are reflex motor acts which are not direct- ly related, but only assist motor activity for its better coordination, stability and keeping the body balance. The visual function is also import- ant to gait [5]. Types of abnormal gaits The investigation of gait is an integral part of the pathokinesiological study of the func- tional problems in any of the segments of the lower limbs. Review articles GAIT ABNORMALITIES IN FUNCTIONAL PROBLEMS OF THE LOWER EXTREMITIES AND IN NEUROLOGICAL DISEASES M. Becheva, PhD Abstract: Gait is a complex, automated and stereotyped motor activity that allows for movement of the body in an upright position. The investigation of gait is an integral part of the pathokinesiological study of the functional problems in any of the segments of the lower limbs. As the stereotype of walking changes at departure, stopping, turning, walking alongside another one, gait should be examined in different situations. In functional problems of the lower limbs and in some neurological diseases, the follow- ing abnormal gaits are detected: arthrogenic gait in extensional contractures of the hip or knee, walking in flexion contractures, "Gluteus maximus" gait, "Gluteus medius"gait, ataxic gait, hemiparetic (hemiplegic) gait, gait in parkinsonism, gait in paresis of plantar flexor, lameness in spasm of m. psoas major, gait in insufficiency of m. quadriceps femo- ris, gait in shortening of a lower limb, steppage gait and scissor gait. Adjusting abnormal gait is especially important to improve the functional condition of the patients in view of procuring a better quality of life. Keywords: abnormal gait, functional problems, neurological diseases.
Transcript of GAIT ABNORMALITIES IN FUNCTIONAL PROBLEMS OF THE …bsphs.org › wp-content › uploads › 2017...

48
Medical University- Plovdiv, Medical College, Bulgaria, 120Buxton Bros.4004 Plovdiv
Introduction Gait is a complex stereotyped and auto-mated motor activity, which allows for move-ment of the body in an upright position. It consists of several components: 1. Keeping the body upright. It is imple-mented by antigravity reflexes that keep body and head upright and limbs in extension [1]. These reflexes depend on proprioreception, which gives information about the position of the limbs, a sense of stepping down and so on. Anti-gravity reflexes may be increased patho-logically in the so called decerebration - increased muscle tone of the body and limbs extensors. It occurs when the brainstem is blocked at the level of the mesencephalon and bulbar nucleus [2]. 2. Stereotypical, automated sequential motor acts related to the movement of the body. This is a complex reflex activity that is activated by the consistent contact of the foot with the
ground and allows the body to move forward. Gait is a conscious and volitional motor activity [3]. 3. A complex coordination action during body movements, to maintain the center of grav-ity by adjusting muscle tone of the extensors and flexors. Vestibular-cerebral reflexes, proprio receptive reflexes and neocerebral activities are important for the realization of a normal gait [4]. 4. Auxiliary motor actions (synkinesis). These are reflex motor acts which are not direct-ly related, but only assist motor activity for its better coordination, stability and keeping the body balance. The visual function is also import-ant to gait [5].
Types of abnormal gaits The investigation of gait is an integral part of the pathokinesiological study of the func-tional problems in any of the segments of the lower limbs.
Review articles
GAIT ABNORMALITIES IN FUNCTIONAL PROBLEMS OF THE LOWER EXTREMITIES AND IN NEUROLOGICAL DISEASES
M. Becheva, PhD
Abstract: Gait is a complex, automated and stereotyped motor activity that allows for movement of the body in an upright position. The investigation of gait is an integral part of the pathokinesiological study of the functional problems in any of the segments of the lower limbs. As the stereotype of walking changes at departure, stopping, turning, walking alongside another one, gait should be examined in different situations. In functional problems of the lower limbs and in some neurological diseases, the follow-ing abnormal gaits are detected: arthrogenic gait in extensional contractures of the hip or knee, walking in flexion contractures, "Gluteus maximus" gait, "Gluteus medius"gait, ataxic gait, hemiparetic (hemiplegic) gait, gait in parkinsonism, gait in paresis of plantar flexor, lameness in spasm of m. psoas major, gait in insufficiency of m. quadriceps femo-ris, gait in shortening of a lower limb, steppage gait and scissor gait. Adjusting abnormal gait is especially important to improve the functional condition of the patients in view of procuring a better quality of life.
Keywords: abnormal gait, functional problems, neurological diseases.

The examiner, however, should be aware that the irregularities in the posture of the head, neck, chest and lumbar spine can also lead to pathological changes in the gait without affect-ing the lower limbs [6]. We need to investigate the movement of each motor segment of the trunk and lower extremities and report any deviation from the normal stereotype of walking [7]. First, a comprehensive view of the posture of asymmetries need to be made and then gait should be analyzed taking into account the length and frequency of steps, duration of indi-vidual phases of the servomotor cycle, the speed of movement [8]. A normal walking stereotype in a patient is usually established after the third step. After the overall view, the study is direct-ed to separate motor moments of the kinetic chain. Because the stereotype of walking chang-es at departure, stopping, turning, walking alongside another one, the gait should be exam-ined in different situations. We need to seek ways to make the patient walk, not realizing that they are being observed- be sent to a device, bring some object, etc. During walking the patient should be viewed from all sides [9, 10]
Arthrogenic gait in extensional contractures in the hip or knee. Arthrogenic gait, caused by contracture or deformity, may be or may be not accompanied by pain. If until recently the knee was in immo-bilization and can be folded to the extent neces-sary to carry out normal swing, the pelvis will be compensatorily raised through increased plantar flexion of the opposite leg over his/her support phase [4]. On the other hand, the affected leg will not be moved ahead in a straight trajectory, but will strikean outer trajectory (mowing or circumduction)[11]. The pelvis on the affected part will carry out compensatory elevation. Irrespective of the joint (s) where the contracture is, in general there will be a different length of the steps between the affected and unaffected leg. Usually, the step of the unaffected leg is
shortened (the support phase of the affected foot is shortened) [12].
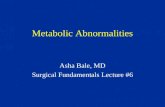
Gait in flexion contractures. Such contractures develop most often from prolonged immobilization, prolonged mode and improperly conducted conservative treatment. Arthrogenic gait in extensor contracture in the left knee or hip.A) increased plantar flexion during the support phase of the unaffected limb.B) circumduction in the swinging motion of the affected leg Flexion contracture in the hip is mostly offset by increased lumbar lordosis (increased inclination of the pelvis) and extension of the body, combined with flexion in the knee with a view to achieve foot contact with the floor [13]. In flexion contracture in the knee, the patient compensates by increased dorsal flexion in the ultimate swing phase and in meeting the support with the unaffected limb, as in the early phase of the push with the affected limb [11]. Plantar-flexion contracture in the knees offset by hyperextension in the knee in the monosupportphase of the affected limb and flex-ion of the corpse forward in the hip in the second part of the same phase. Lifting the heel at the end of the support phase of the affected limb occurrs earlier [14].
"Gluteus maximus" gait Such a gait is manifested in weakness of m.gluteus maximus, which is considered the main extensor hip. The offset is achieved with a rear swing of the corpse in the phase of meeting the support with the injured limb to keep the extension in hip joint [4].
"Gluteus medius" (Trendelenburg) gait Such a gait occurs in weakness in the hip abductor (m. gluteus medius and minimus). This violates the stabilization of the pelvis in the monosupport phase and it lowers in the direction of swing foot – the Trendelenburg symptom. In a more pronounced deficit the patient tilts
49PHARMACIA, vol. 64, No. 1/2017Gait abnormalities in functional problems...

the shoulder belt in the direction of the injured leg to shorten the arm of the Support Center of Gravityaction and thus alleviate the hip abductor (symptom of Duchenne). This type of gait is called by some Duchenne – Trendelenburg[12]. If the insufficiency of the abductor in the hip is bilaterally pronounced, the gait is associat-ed with a significant deviation in the frontal plane (duck walking). This type of gait is most frequently found in patients with bilateral congenital dislocation of hip joint [9].
Ataxic gait. If the patient has impaired propriorecep-tion or impaired muscle control, there is a tendency of disturbing the balance and diver-gence of legs. The feet are dragged on the floor because of the impaired sensation. The patient looks at his feet while walking. In patients with cerebellar ataxia, the gait characterized by stag-gering and rolling, shredded, interrupted, while the movements are irregular [14, 15].
Hemiparetic (hemiplegic) gait. Patients with hemiparesis and hemiparal-ysis move the affected foot with a swinging motion (mowing gait), while simultaneously folding more hip joint and the knee to separate the fingers of the sagging in plantar flexion foot from the floor. The affected upper limb is close to the body [16]. At expressed hemiparesis and hemiparal-ysis, the pelvis is rotated forward on the affected part. Thus the unaffected lower limb is located further back. In walking, the passing in opposite direction of either leg becomes almost impossi-ble. There is no back support with the affected leg and front support with the unaffected leg [14, 16].
Gait in Parkinsonism. In patients suffering from parkinsonism, the neck, trunk, hip joint and knees are flex-ioned. Gait is characterized by small quick steps (Japanese gait). The upper limbs are stiff and do not carry out normal counterswinging motions – there is a
lack of dissociation of the belly muscles. When walking the patient leans forward and walks faster, unable to stop propulsio [16].
Gait in paresis of plantar flexor In plantar flex dysfunction the stabiliza-tion of the knee and TBS is significantly affect-ed. The insufficiency of plantar flexors leads to loss of the thrust. The support phase with the affected limb is shortened, respectively the final swing is shortened (ie, length of step) with the unaffected leg [17, 18].
Lameness in spasm of m. psoas major. This type of claudication occurs in diseases and damage to the hip joint (eg. in Prethes). The patient has difficulties with performing the swing and limps, while manifest-ing compensatory increased mobility of the pelvis and trunk. The limping can be caused by weakness or painful inhibition of m. psoas major [18]. In the classic version of expression the affected hip is in external rotation, flexion and adduction. The patient increases the amplitude of motion of the trunk and pelvis so that to cause flexion moment in the during the swing [6].
Gait in insufficiency of m. quadriceps femoris In quadriceps insufficiency the patient includes proximal and distal compensatory mechanisms. Most often in the support phase, the knee is locked in hyperextension. In meeting the support, the body leans forward and while the ankle is flexed inaplantar fashion. If the body flexors, hip joint and the foot can not implement this compensatory mechanism, the patient extends the knee with a hand [15].
Gait in shortening of one lower limb In shortening of one lower limb, the patient limps, while in the support phase with the shorter leg tilts the body towards him/her and the pelvis leans towards the same part. The patient may supinate the foot on the truncated side in their attempt to extend the limb [19].
50 M. Becheva, PhDPHARMACIA, vol. 64, No. 1/2017

On the side of the longer limb there can be observed increased flexion in the knee and pelvic elevation during the swing phase, to enable the foot to be transferred forward without touching the floor The support phase for both limbs can be the same. By using appropriate orthopedic shoes with different height (to adjust shortening) a normal gait can be achieve. This gait is called by some authors osteogenic painless gait [20, 21].
Scissor gait. Such a gait can be observed in elastic adductor paralysis in hip joint, wherein knees adhere to one another and can not be separated. The divergence of the legs when walking in this case requires great effort. Spastic paraplegia is the reason for this most often, so some authors call this type of gait spastic gait [22, 23].
Steppage gait Such gait occurs in paresis and paralysis of the dorsal flexors of the foot, resulting in the foot hanging down when carrying it forward in swing phase. This causes an extension of the affected leg and therefore compensatorily the knee is raised higher than normal (greater flex-ion in TBS and knee). The meeting of the support occurs not with the heel but with the foot, which "splashes" in contact because of the lack of control by the dorsal flexors [19, 24].
Conclusion Musculoskeletal pathologies leading to the development of muscle weakness, pain or limited range of motion lead to changes in gait. Some patients develop effective compensatory and replacement mechanisms allowing them to keep their locomotor abilities. Patients with damage to the central motor neuron develop adequate compensation and replacement mecha-nisms harder because they have impaired propri-oreception, equilibrium abilities and prominent muscle spasticity [25]. Human gait changes with age. In adults it gradually becomes slower, steps smaller, the coordination of gait deteriorates, normal synki-
nesis are reduced. The reasons for this are com-plex and are associated with discrete functional disturbances of the entire central nervous system, in the wake of degenerative and vascular atherosclerotic processes [26]. Adjusting the parameters of abnormal gaits is especially important to improve the func-tional status of patients in view of a achieving higher quality of life.
References. 1. Bouisset S. Biomécanique et physiolo-gie du movement. Médecine de rééduca-tion2002; 248-320. 2. Pérennou D. Contrôle postural, espace, locomotion, édition Solal, Paris, 2013. 3. Paysant J, Beyaert C, Datie A, Marti-net N. Évaluation des capacités et des perfor-mances: contribution des monitorages de la loco-motion en situation d'exercice et de vie réelle. Annales de Réadaptation et de Médecine Phy-sique 2007; 3(50):156–164. 4. Barbier F. Modélisationbiomécanique du corps humain et analyse de la marchenormale et pathologique- Application à la rééducation. Paris 1994:5. 5. Lacour M. Controle Postural, Espace, Locomotion. Posture, Equilibre&Mouvement 2013:45-62. 6. Bieuzen F. Influence des propriétésmusculaires sur un exercice de loco-motion humaine; de l'efficience à la déficience-motrice. Edilivre-a Paris Universitaire. 2008. 7. Valerius K.-P. Les muscles: Anato-miefonctionnelle de l'appareillocomoteur, édition De BoeckUniversité, Paris 2013. 8. Dimitrovа, Popov N. Manual function-al diagnosis of musculoskeletal system. Sofia: NSA-Press, 2003. 9. Lacour M. Posture Et Locomotion. 16emes JourneesFrancaises De Posturologie Clinique Posture, Equilibre&Mouvement 2011:18-42. 10. Pennecot G. Marché pathologique de l'enfant paralysécérébral. Sauramps Medical 2006. 11. Viton Dr. Pr. J M,.Bensoussan L Dr.,
51PHARMACIA, vol. 64, No. 1/2017Gait abnormalities in functional problems...

Corresponding author:Maria Vakrilova BechevaMedical College of Medical University-PlovdivPlovdiv 4004 “Buxton Brh 120”Tel: +359 32641882E-mail: [email protected]
Milhe V.de Bovis, Collado, Dr. H. Marche normale et marchepathologique. Delarque. Faculté de Médecine 2011. 12. Fusco N. Analyse, modélisation et simulation de la marchepathologiqueq. Maloin, 2008 13. Demenÿ G, Quinn L. Etude de la locomotion humainedans les cas pathologiques- Comptes Rendus des Séances de l'Académie, 2005. 14. Chantraine A. Rééducationneu-rologique, éditionArnette, Paris, 2013. 15. Popov N. Clinical pathokinesiologi-cal diagnostics. Sofia: NSA-Press, 2008 16. Perfetti С. L'exercicethérapeutiquec-ognitif pour la rééducation du patient hémi-plégique. 2001, Masson, 89-123. 17. Rivière J. Locomotion autonome et cognition spatiale: le paradoxe de l'amyotro-phiespinale infantile. Archives de Pédiatrie 2007;14(3): 279-284. 18. Auvinet B, Barrey E, Deguillard D. Quantification ambulatoire des claudicationshu-maines. Annales de Réadaptation et de Méde-cine Physique 1998;41:105-112. 19. De La Tourette G. Étudescliniqueset-physiologiques sur la marche: la marchedans les maladies du systèmenerveux: étudiéepar la
méthode des empreintes. 2001, Bureaux du Progrès. 20. Gasq D, Molinier F, Lafoss JM. Physiologie, methodesd'explorations et troubles de la marche2009. 21. MegrotF, Goulette A. Analyse du mouvement et handicap : application à la marchepathologique. : Des pratiques. Le mouve-ment., Paris : Editions Revue EPS, collection Pour l'action, 2009: 85-100. 22. Fraix V Dr. Orientation diagnos-tiquedevant un trouble de la marche et de l’équilibre . 2005: 340. 23. Maupas E, Martinet N, André JM. Miseenévidenced'uneasymétried'activité des membresinférieurslors de la marche chez le sujetsain par monitorageélectrogo-niométrique.Annales de Réadaptation et de Médecine Physique1998; 41(6): 334-339. 24. Thoumie P. Actualitésenrééducation des maladies neuro-musculaires de l'adulte. Paris: Springer, 2010 25. David A. Effet du contexte social sur la locomotion chez la personneâgée. Paris 2004 26. Viel É. La marchehumaine, la course et le saut. Biomécanique, explorations et move-ment. Paris Maloine 2008.
52 M. Becheva, PhDPHARMACIA, vol. 64, No. 1/2017