RELIABILITY OF DIAGNOSIS ABNORM – NORMS AND DIAGNOSIS #2 – LESSON #2.
Förlossningsdepression- Studier på mammor och barn i
Uppsala
Alkistis SkalkidouDocent, Överläkare
Institutionen förKvinnors och Barns Hälsa

INCIDENCE OF DEPRESSION • 15%-20% of adults experience a major
depressive episode each year• The incidence among women is twice that of
men and peaks between 18 to 44 years of age - the childbearing years

DEPRESSION IN WOMEN
Women are at increased risk of mood disorders during periods of hormonal fluctuation
premenstrualpostpartumperimenopausal

Kendell et al, Br J Psychiatry, 1987
Admission of women to PSYCHIATRIC CLINICS perinatally

SPECTRUM OF POSTPARTUM MOOD DISORDERS

POSTPARTUM DEPRESSION
• As high as 19.2% of women experience depression (PPD) over the first year postpartum
• Onset can be as early as 24 hours or as late as several months following delivery
• Higher incidence by lower socioeconomic status
Gavin et al, Obstet Gynecol, 2005

SYMPTOMS OF POSTPARTUM DEPRESSION
Hopelessness Loss of pleasure in activities
Helplessness Mood changes
Persistent sadness Inability to adjust to role ofmotherhood
Irritability Inability to concentrate
Low self-esteem Sleep /appetite disturbances
Not different from non-postpartum depression
Williamson et al, Assessment, 2012

Mild Severe
• Severe Symptoms:– Thoughts of death– Thoughts of suicide– Wanting to flee or get away– Being unable to feel love for the baby– Thoughts of harming the baby– Thoughts of not being able to protect the
infant– Hopelessness

THE ETIOLOGY OF POSTPARTUM DEPRESSION
Hormonal factors
Psychosocial factors
Genetic vulnerability
POSTPARTUM DEPRESSION

THE hormonal hypothesis
Chroussos et al, Ann Intern Med, 1998
THE hormonal basis
After childbirth: Dramatic decreases in estradiol, progesterone, cortisol, thyroid hormones
HPA axis hyporesponsiveness for the first week postpartum
Vulnerability of with previous history of PPD
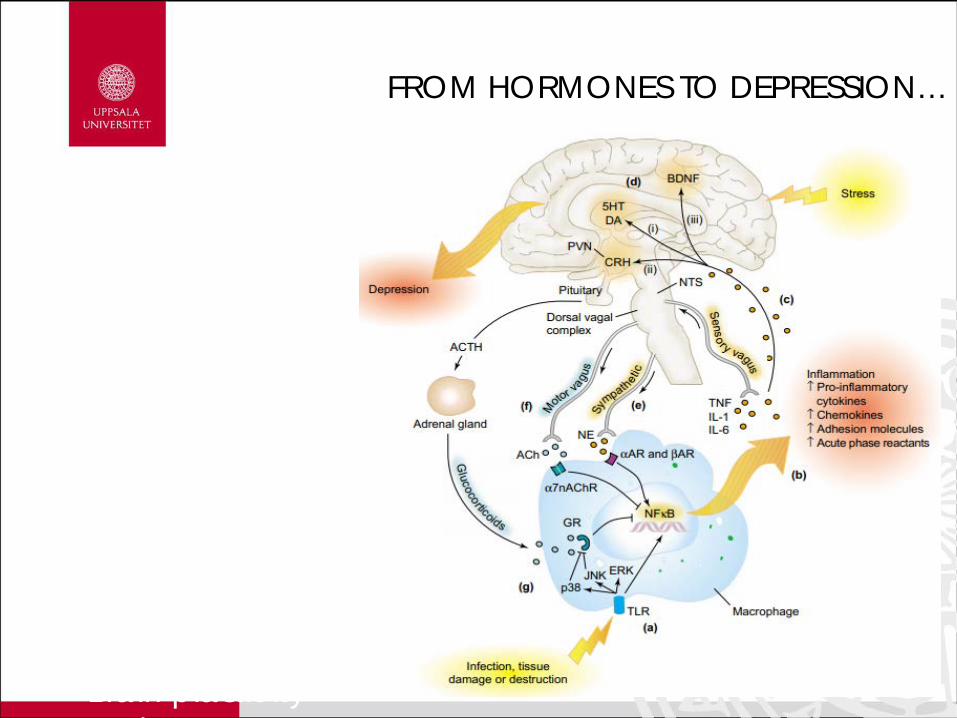
FROM HORMONES TO DEPRESSION…
– Serotoninergic system
– Dopaminergic system
– Inflammatory response
– BDNF system
– Brain plasticity d

Role of psychiatric background
O’Hara et al, j Abnorm Psychol, 1984

established risk factors
• history of depression• depression and anxiety during pregnancy • neuroticism • low self-esteem • postpartum blues • stressful life events (including childcare-related stressors) • poor marital relationship• poor social support• low socioeconomic status (SES)• being single• unwanted pregnancy• obstetrical stressors• difficult infant temperament
O’Hara & McCabe, Annu Rev Clin Psychol, 2013
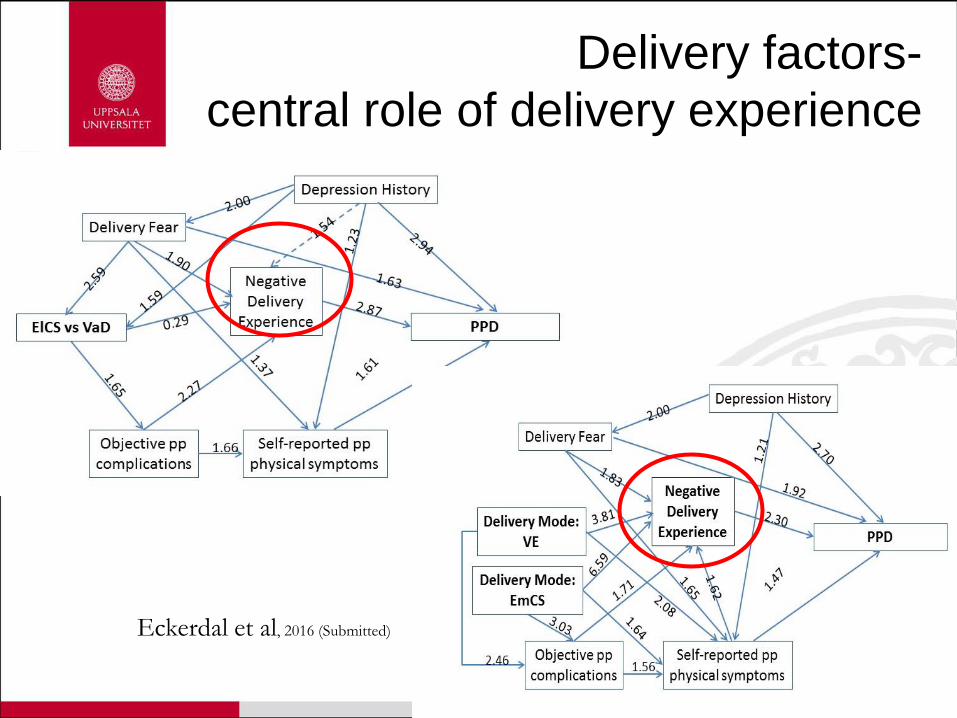
Delivery factors-central role of delivery experience
Eckerdal et al, 2016 (Submitted)

GENETICS
Associations of PPD risk with the following genetic polymorphisms in 5-HTTPLR (serotonin receptor)MAO-ACOMT
Associations only with early-onset PPD (8 weeks)Figuiredo et al, J Affect Disord, 2015

CONSEQUENCES OF PPD
Maternal impact
Recurrent depressive episodes
Negative emotionality
Increased risk of subsequent somatic morbidity
Negative effects on parenting
CONSEQUENCES OF PPD
Impact on breastfeeding
Negative feeding outcomes
Decreased breastfeeding duration
Increased difficulties during breastfeeding
Decreased levels of breastfeeding self-efficacyDennis & McQueen, Pediatrics,
2009

CHILD CONSEQUENCES
• Cognitive development
• Poor development of language and IQ
• More profound the effect on boys
• Linear associations with chronicity of depression
Child CONSEQUENCES• Behavior
• higher levels of internalizing
• externalizing • general
psychopathology • negative
affect/behavior • lower levels of positive
affect/behavior
Goodman et al, Clin Child Fam Psychol Rev, 2013
Brand & Brennan, Clin Obstet Gynecol, 2009
Important is the role of epigenetic modifications!!!
• Physical health• Primarily infections• Maladaptive parenting of
depressed mothers
SCREENING FOR POSTPARTUM DEPRESSION
The USPSTF recommends screening for depression in the general adult population, including pregnant and postpartum women. Screening should be implemented with adequate systems in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.

SCREEN ALL POSTPARTUM WOMEN FOR PPD BECAUSE A WOMAN MAY:
• Be unable to recognize she is depressed• Believe her symptoms are “normal” for new
moms• Fear being labeled a “bad mother” if she admits
her maternal experience does not meet society’s picture of bliss
• Feel she is going crazy and fears her baby will be taken from her
Who Could Screen?
• Clinicians & service providers who work with pregnant & postpartum women– Advance Practice Nurses–CNMs, and NPs– Physicians–OB/GYN, Family Practice, Pediatrics– NICU staff– Public health, hospital, and parish nurses– Prenatal care coordinators– WIC dietitians– Lactation consultants & home visitors (PH nurse, etc.)– Social workers– Midwives at delivery ward– Others?

WHEN TO SCREEN FOR PMD
• At preconception visit• During prenatal intake & subsequent visits• During postpartum exams• During infant’s WCC & WIC visits• When infant is seen for sick care or in ER• At early intervention home visits• At family planning visits during the first year
postpartum• At mother’s visits for routine episodic care

Identification of women at risk-Stratification of risk

SCREENING TOOLS
• There are several tools available:– Edinburgh Postnatal Depression Scale
(EPDS)– The Mills Depression & Anxiety
Checklist– The Center for Epidemiological
Studies Depression Scale (CES-D)– Others, often on various websites for
mental health

EDINBURGH POSTNATAL DEPRESSION SCALE (EPDS)
• Designed for home or outpatient use• Consists of 10 questions• Can be completed in approx. 5 minutes• Reviews feelings the previous 7 days• Scored 0-3 depending on symptom severity • Depending on study, cut off is 13 - 9 points

EPDS

treatment
• Pharmacological intervention
• Counseling, individual and/or group
• Support groups

PSYCHOTHERAPY
O’ Hara et al, Arch Gen Psych, 2000Studart et al, Psychother Pract Res, 1995
Appleby et al, BMJ, 1997Wickberg & Hwang, J Affect Dosord, 1996
IPT: Interpersonal Psychotherapy, CBT: Cognitive Behavioral Therapy, RCT: Randomized Controlled Trial

Antidepressants• Fluoxetine: only drug proven as effective as
cognitive-behavioral counseling and more effective than placebo; transmits through breast milk
• Nortriptyline• Sertraline *• Paroxetine
-use for >6 months, data lacking in regards to optimal duration
-use in combination with adjunctive anxiolytics (lorazepam, clonazepam)
Wisner et al, J Clin Psychopharmacol, 2006Misrir al, J Clin Psych, 2004
Appleby et al, BMJ, 1997

Other Considerations
• If the woman chooses to breastfeed while on antidepressants, she should work collaboratively with a psychiatrist and her pediatrician
• If the infant experiences insomnia or other behavior changes, his serum should be assayed for the presence of medication
• In sufficient data for potential neurodevelopmental deficits of the baby

Hormonal Therapy
• Transdermal estrogen: effective in severe postpartum depression - women treated for 6 months
- estrogen patch more effective than placebo for treating postpartum depression, effect occurred by 1st
month and remained statistically significant- for last 3 months, women given progesterone
12days/month to reduce risks of unopposed estrogen• Sublingual 17-beta estradiol
- effective in 2 case reports and uncontrolled series of 23 cases
• Monotherapy or adjunctive to antidepressants• BREASTFEEDING
Gregoire et al, Lancet, 1996Ahokas er al, J Clin Psych, 2001

Alternative options• Enhanced professional and social
support
• Massage therapy (reduced anxiety)
• Behavioral sleep intervention
• Electroconvulsive therapy

Mother-baby units
När mamman drabbas av:
• Psykos• Bipolär sjukdom• Svår ångest eller depression• Annan sjukdom som kräver
inläggning
Och har en bebis upp till 12 månader gammal


Treatment and activities
PPD studier in Uppsala

UPPSAT-studien

UPPSAT – resultat
Risk of postpartum depression in association with serum leptin and interleukin-6 levels at delivery: a nested case-control study within the UPPSAT cohort(Skalkidou et al., Psychoneuroendocrinology 2009)
• Negative association between Leptin levels and depressive symptoms 6 weeks and 6 months postpartum
• Leptin – possible biomarker for postpartum depression?

UPPSAT – resultat
Seasonality patterns in postpartum depression (Sylvén et al., American Journal of Obstetrics and Gynecology, 2010)
• Seasons vary greatly in Sweden…
• Women giving birth during autumn/winter higher risk for postpartum depression

Seasonality
UPPSAT – resultat
Thyroid function tests at delivery and risk for postpartum depressive symptoms (Sylvén et al., Psychoneuroendocrinology 2012)
• Postpartum depression and thyroid disturbances common complications after delivery
• TSH taken at delivery could predict depressive symptoms at 6 months postpartum

Pappan- partner

Pappan- partner

BASIC
Biology, Affect, Stress, Imaging and Cognition in Pregnancy and the
Puerperium
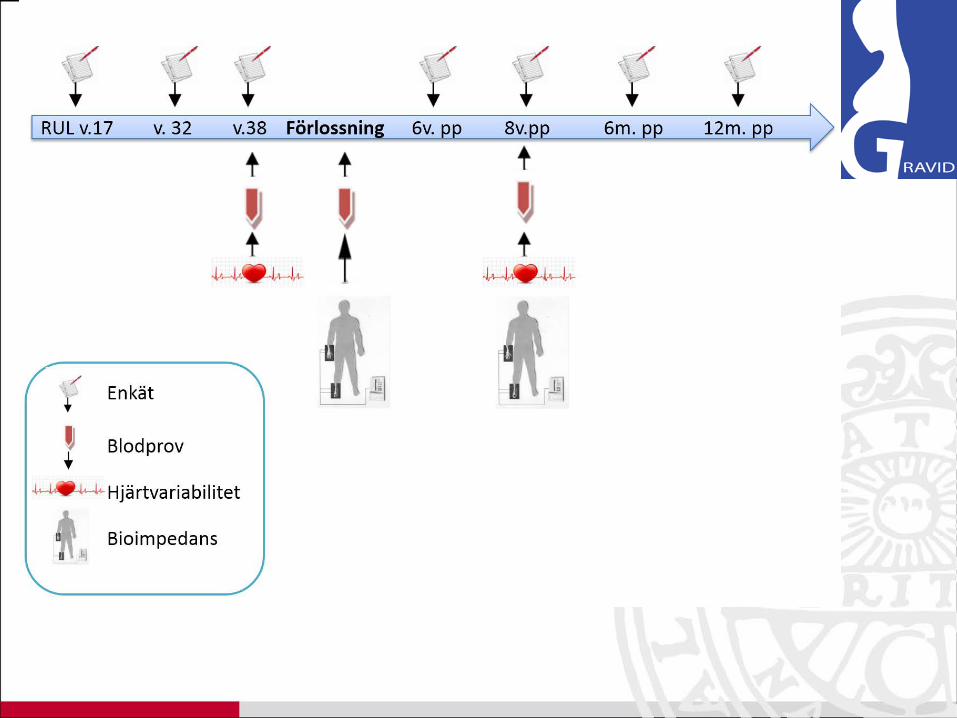
BASIC
• Autumn 2009• Longitudinal study• Web-based questionnaires• BIOLOGICAL focus

www.basicstudie.se

BASIC
• 22 % of pregnant women in Uppsala
• Goal: inclusion of 5000 women
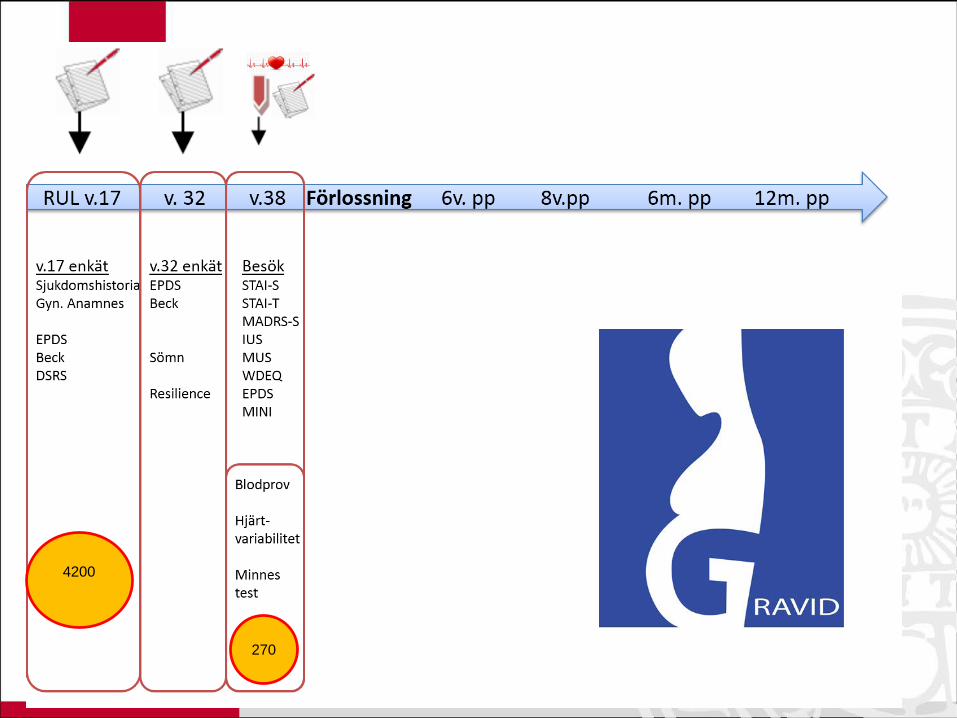
4200
270

Förlossning
BlodprovNavelsträngsblodNavelsträngsbiopsi
Bioimpedans
Vid ES:Ryggmärgsvätska
(Placentabiopsi)(Fostervatten)
FormulärMUS
3800
148

6v. pp
6v.pp enkätAllmänna frågorAmningLiv just nuSömnTobakAlkoholEPDSBeckLivshändelserDSRS IBQPartner
6m. pp
12m. pp
6m.pp enkätAllmänna frågorAmningLiv just nuSömnTobakAlkoholEPDSBeckLivshändelserBondingPTSD Partner
12m.pp enkätJust nuLITESLEIBQVPSQ
8v.pp
BesökSTAI-SSTAI-TMADRS-SIUSMUSWDEQEPDS
Blodprov
HjärtvariabilitetBioimpedans

Vilka är med?
Not participatingn = 3097
Participatingn = 661
Age 30,6 ±5,2*** 31,9 ±4,6
Nulliparous 42,6% 43,1%
Any pregnancycomplication
20,6%* 16,8%
Gestational length, days
276** 278
Premature birth 6,9% 5,4%
AURORA 2,2% 1,7%
SSRI use ?? 4,0%
All Uppsala women giving birth 2011


Current PhD projects• Do women with prior depression have an altered cortisol awakening
response during pregnancy?– Charlotte Hellgren
• Endocrinology of antenatal depression– Anna-Karin Hannefors
• The HPA axis system in PPD– Stavros Iliadis
• Attachment styles and perinatal depression– Cathrine Axfors
• Perinatal complications and depressive symptoms– Patricia Eckerdal
• Placental mRNA expression in depressed mothers– Åsa Edvinsson, Helena Kaihola
• In search of protein-level biomarkers in perinatal depression
• Epigenetic studies within the U-BIRTH cohort

Current PhD projects• Do women with prior depression have an altered cortisol awakening
response during pregnancy?– Charlotte Hellgren
• Endocrinology of antenatal depression– Anna-Karin Hannefors
• The stress response system in PPD– Stavros Iliadis
• Attachment styles and perinatal depression– Cathrine Axfors
• Perinatal complications and depressive symptoms– Patricia Eckerdal
• Placental mRNA expression in depressed mothers– Åsa Edvinsson, Helena Kaihola
• In search of protein-level biomarkers in perinatal depression
• Epigenetic studies within the U-BIRTH cohort
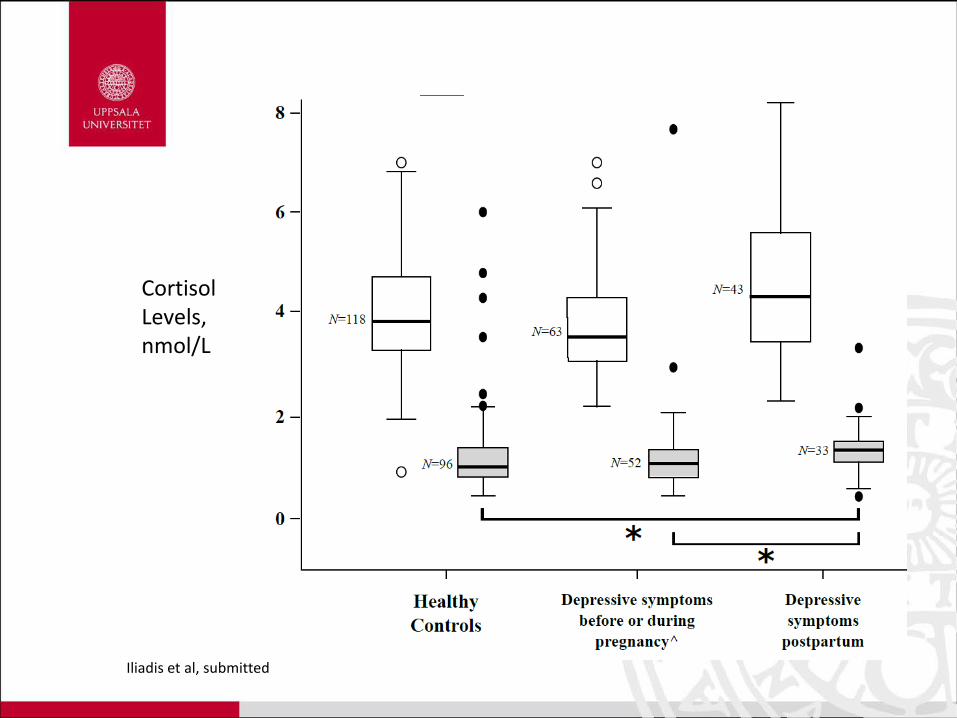
CortisolLevels,nmol/L
Iliadis et al, submitted

Iliadis et al, submitted
CSF vs serum/plasma


Exploratory metabolomics


MedverkandeUPPSALA UNIVERSITY
Dept of Women’s and Children’s Health/Obstetrics and Gynecology• Alkistis Skalkidou, Inger Sundström-Poromaa, Birgitta BirgisdottirDept of Neuroscience, Psychiatry• Lisa Ekselius, Fotios Papadopoulos Dept Physical and Analytical Chemistry • Jonas BergquistDept of Immunology, Genetics and Pathology• Masood Kamali-Moghaddam
Prof. Hasse Karlsson, Turku University, FinlandProf. Georgios Chrousos, Athens University, GreeceProf. Maria Klapa, Patras University, Greece
U-BIRTH studien
BASIC-child studien

Esscher et al., accepted

Esscher et al., accepted


” I decided to be happy because this improves my health”
Voltaire
Tack !