Frameworks for Internal Medicinedownloads.lww.com/.../samples/Frontmatter.pdf · and residency...
14
Frameworks for Internal Medicine
Transcript of Frameworks for Internal Medicinedownloads.lww.com/.../samples/Frontmatter.pdf · and residency...

Frameworks for Internal Medicine


Frameworks for Internal MedicineAndré M. Mansoor, MDAssistant Professor of Medicine
Division of Hospital Medicine
Director, Procedure Service
Oregon Health & Science University
Portland, Oregon

Acquisitions Editor: Matt HauberFreelance Development Editor: Tom ConvilleDevelopment Editor: Andrea VosburghEditorial Coordinator: Lindsay RiesMarketing Manager: Mike McMahonProduction Project Manager: Kim CoxDesign Coordinator: Teresa MallonManufacturing Coordinator: Margie OrzechPrepress Vendor: TNQ Technologies
Copyright © 2019 Wolters Kluwer.
All rights reserved. This book is protected by copyright. No part of this book may be reproduced or transmitted in any form or by any means, including as photocopies or scanned-in or other electronic copies, or utilized by any information storage and retrieval system without written permission from the copyright owner, except for brief quotations embodied in critical articles and reviews. Materials appearing in this book prepared by individuals as part of their official duties as U.S. government employees are not covered by the above-mentioned copyright. To request permission, please contact Wolters Kluwer at Two Commerce Square, 2001 Market Street, Philadelphia, PA 19103, via email at [email protected], or via our website at shop.lww.com (products and services).
9 8 7 6 5 4 3 2 1
Printed in China
Library of Congress Cataloging-in-Publication Data
Names: Mansoor, André M., author.Title: Frameworks for internal medicine / André M. Mansoor.Description: Philadelphia : Wolters Kluwer, [2019] | Includes bibliographical references and index.Identifiers: LCCN 2018041461 | ISBN 9781496359308 (pbk.)Subjects: | MESH: Internal Medicine | Diagnosis, Differential | Case Reports | Problems and ExercisesClassification: LCC RC71.5 | NLM WB 18.2 | DDC 616.07/5–dc23LC record available at https://lccn.loc.gov/2018041461
This work is provided “as is,” and the publisher disclaims any and all warranties, express or implied, including any warranties as to accuracy, comprehensiveness, or currency of the content of this work. This work is no substitute for individual patient assessment based upon health care professionals’ examination of each patient and con-sideration of, among other things, age, weight, gender, current or prior medical conditions, medication history, laboratory data and other factors unique to the patient. The publisher does not provide medical advice or guidance and this work is merely a reference tool. Healthcare pro-fessionals, and not the publisher, are solely responsible for the use of this work including all medical judgments and for any resulting diagnosis and treatments. Given continuous, rapid advances in medical science and health information, independent professional verification of medical diagnoses, indications, appropriate pharmaceutical selections and dosages, and treatment options should be made and healthcare professionals should consult a variety of sources. When prescribing medication, healthcare professionals are advised to consult the product information sheet (the manufacturer’s package insert) accompanying each drug to verify, among other things, conditions of use, warnings and side effects and identify any changes in dosage schedule or contraindications, particularly if the medication to be administered is new, infrequently used or has a narrow therapeutic range. To the maximum extent permitted under applicable law, no responsibility is assumed by the publisher for any injury and/or damage to persons or property, as a matter of products liability, negligence law or otherwise, or from any reference to or use by any person of this work.
Cover image:Antony GormleyBUILDING 1-5, 2013Cast iron5 elements; dimensions variablePhotograph by Stephen White, London© the artist
shop.lww.com

v
DEDICATION
For my mother Salma, and my father Edward. All that I have ever hoped to be, I owe to you.

vi
FOREWORD
In the end, after the “large group learning studios” have fallen silent, the “breakout” rooms are in disarray, and nobody knows that the remotes for the massive TV sets no longer work, medical students will still know 90% of the expected core knowledge. How can this be? It is because these handpicked students are surrounded by handpicked residents, fellows, and junior faculty, all of whom believe it is a fundamental obligation of the profession to teach. They teach all who thirst and most of those who should thirst. It has been this way since the “breakthrough” at Kos. More amazing, the best of these people do not expect any remuneration other than the satisfaction of doing the job well. Education is still the first of the professional expectations at most academic medical centers. These teachers bring the stringent and austere life of physicians-in-training to the task. They can be counted on to teach students what they need to know and, sometimes, what they ought to know.
This task, for which most academic centers pay nothing, is in peril. RVUs, EMRs, “rooming efficiency,” and grading scales for “patient satisfaction” all take a toll. These faculty members are expected to recognize “kaizen events” and alert the managers. Some of the managers want to teach the “silver spoon” doctors a lesson or 2 about “hard times.” Controversy abides, but the teachers persevere. They are, however, in dire need of help.
Where to start? More than anything else, they need blackboards. Blackboards have disappeared. The boards that fill the old blackboard gaps are white and can be written on only with special order pens. When the pens disappear, “informative flyers” begin to fill the space on the whiteboards. “Quiet please. No one can get well in a noisy place!” Are you sure? Sit and listen to an intensive care unit for an hour. “Wash your hands!” The sinks have all disappeared, too, and the wall “hand wash stations” deliver a foul-smelling liquid that fails to dis-patch C-diff spores. It has been labeled toxic for human beings by the FDA. Other messages of importance are
an invitation to a potluck lunch. There is an invitation to attend the next art committee meeting. The boards are covered with ephemerata. Doctors need a sacro-sanct clean board in every corridor of every ward service in every specialty. What will happen at these boards, should they appear, is an ongoing unscripted discussion of the clinical problems at hand for all to see and hear. Approaches to all of the “slings and arrows that life is heir to” show up on these boards. These challenges to health and happiness are ever-present and countless in number. More appear every day. Doctors learn much of what they know at these vestigial boards. Give them real boards and get out of the way!
This book preserves the art of Socratic teaching, a method that reaches back 2500 years. Not only does the process reveal what is known but, even more clearly, it reveals what is not known. Everybody learns. Students, teachers, and nurses learn. Laboratory per-sonnel and patients learn. All will evolve and grow. It is a powerful thing to witness.
Fifty of the most common clinical problems are illustrated in this book. The cache of questions will evolve as the anatomy of erudition points the way. This book contains frameworks that guide the discus-sion of the “chosen fifty.” The 60-year-old man with hematocrit of 32. The 29-year-old pregnant woman with pitting edema to the axillae. The acutely dyspneic long haul truck driver. The young person with fever of unknown origin. The framework prepares the teacher and the learners. It creates the environment most con-ducive to high-impact learning efficiency. In the end, it is the process rather than the framework. The process becomes generalized. Academia is back on track.
Now that we have the book, the boards will appear, hopefully!
Lynn Loriaux, MD, PhDProfessor of Medicine
Oregon Health & Science UniversityPortland, Oregon

vii
PREFACE
Twenty: The number of years the average American physician spends as a student before a degree is earned and residency training begins. Experienced physicians would respond to this notion with a grin; medicine is a dynamic field that requires ongoing refinement of those who practice it. For the physician, learning is a lifelong endeavor. It does not end after 20 years. However, 20 years does mark an important inflection point in the life of an academic physician: there begins the transi-tion from full-time student to part-time student and part-time educator. For most young doctors, this evo-lution does not happen naturally. It must be sought.
Weakness
Brain/spinal cord Anteriorhorn cell
Peripheralnerve
Neuromuscularjunction
Muscle
When I was a third-year medical student on the internal medicine clerkship, I was introduced to the “morning report” case conference, usually led by the chief residents. It was the aspect of the rotation I most enjoyed. I was drawn to the chal-lenge of solving the cases, eventually turning it into a game: I would silently record how long it took for me to guess the correct diagnosis. My record was the time needed for the presenter to finish her open-ing words, “shortness of breath, facial plethora, and upper extremity swelling” (which I immediately recognized as superior vena cava syndrome). Often I was wrong. However, no one else knew about those mistakes. Then, I became an intern and sat in the same room as before, but my role had changed. As an intern, I was obligated to share my thoughts with the group. Still, it remained simple. I would speak up only when I thought I had a pretty good idea of the correct answer. When I did not, some-one else would, and eventually we would get on the right path. On some occasions, however, no one spoke up.
One such occasion involved the case of a mid-dle-aged man with weakness. After time was spent clarifying additional history from the presenter, the chief resident advised that we begin to construct a
differential diagnosis. “Stroke,” offered a resident in the audience. “Is that all?” asked the chief. The room was quiet. My mind was scrambling to come up with more diagnoses, as it often had when confronted with a problem associated with a broad differential diagnosis. “Does anyone have an approach to weak-ness?” Meeting more silence, he offered his own method. Breaking it down anatomically, he began to write several headings on the board, including “brain/spinal cord,” “anterior horn cell,” “peripheral nerve,” “neuromuscular junction,” and “muscle.”
It was as if a light had suddenly turned on in the room. Using this structural format, new possibilities were uncovered. Below the heading “brain/spinal cord,” the chief began listing the diagnoses that were now flow-ing from the audience, including brain tumor, multiple sclerosis, and epidural abscess. Next were lesions of the anterior horn cell. Prompting the group, the chief asked, “Does anyone remember what disease Lou Gehrig had?” Of course, within seconds, ALS appeared on the list. In a similar way, the audience identified diseases of the peripheral nerve, neuromuscular junction, and mus-cle. With this framework for approaching weakness, we had achieved what seemed impossible moments before.
I left that session with an appreciation of the chal-lenges of leading case conference. When the audience is quiet, the leader must not only determine the direc-tion of the conference but also guide the audience forward. The following year, I was offered one of the future chief resident positions. With joy came some trepidation. One of the concerns on my mind was the idea of leading the case conferences that I always enjoyed as a member of the audience.
I began to strategize. During ensuing conferences, I made note of each case. I soon recognized that certain problems were often at the center of discussion. This list included entities such as dyspnea, acute kidney

viii PREFACE
injury, anemia, hypoxemia, diarrhea, fever of unknown origin, and syncope. Given the frequency with which these entities seemed to appear during case confer-ence, I reasoned that developing an approach to each of them would prove valuable, particularly in moving conference along in front of a reticent audience.
As I began to work toward this goal, I realized that having an approach to a problem in many cases is as simple as constructing a framework that divides the long differential diagnosis into shorter sublists, which are easier for our brains to store and process. Rather than memorize a long list of diagnoses, it is sufficient to remember the headings of a framework, from which many of the diagnoses can then be generated.
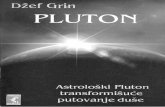
I began to build frameworks for all of the common clinical problems in internal medicine. I used various resources, from pages of notes I scribbled at one point or another during residency to textbooks and primary literature. Some frameworks are time-honored and commonly taught, such as those used for acute kidney injury (prerenal, intrarenal, postrenal) and vasculitis (small vessel, medium vessel, large vessel). After a few months, I had accumulated a healthy amount of mate-rial. Here is 1 example of the frameworks that I was beginning to assemble:
Arthritis
• Crystal arthropathy• Infectious (acute)• Infectious (chronic)• Early oligoarthritis
• Disseminated gonorrhea• Spondyloarthritis• Spirochetal infection• Löfgren’s syndrome• Henoch-Schönlein purpura• Cryoglobulinemia• Behçet’s disease• Early polyarthritis
Inflammatory
• Rheumatoid arthritis• Systemic lupus erythematosus• Viral infection• Polymyositis/ dermatomyositis• Still’s disease• Rheumatic fever• Serum sickness• Sarcoidosis
• Osteoarthritis• Trauma• Hemarthrosis• Charcot joint• Osteonecrosis• Hypertrophic osteoarthropathy• Episodic arthritis of cystic fibrosis• Acromegaly• Hemochromatosis
Noninflammatory
Monoarticular Oligoarticular Polyarticular
These frameworks would become the “tip of the spear” when I was faced with silence during case con-ference. I had accomplished my objective. However, I discovered something much more valuable. I had developed a collection of tools that could be used to teach learners how to approach the clinical problems of internal medicine, beyond the boundaries of case conference.
I spent the rest of my time as a resident using these tools to teach, taking advantage of every opportunity. On the inpatient medical ward, the members of my team were the audience of frequent talks. I discov-ered that the guidance from the framework alone was enough to result in a meaningful teaching session, but I began to expand the outlines with additional learn-ing points, making each talk healthier and more robust. With each passing month, I sharpened my skills as a resident-teacher. By the end of residency, I had become a nascent teacher. I hope this work can help others reach this point.

ix
REVIEWERS
The author would like to thank the following individ-uals for their time and expertise:
SECTION 3: Cardiology
Edward S. Murphy, MDProfessor of MedicineKnight Cardiovascular InstituteOregon Health & Science UniversityPortland, Oregon
Khidir Dalouk, MDAssistant Professor of MedicineClinical Cardiac ElectrophysiologistKnight Cardiovascular InstituteOregon Health & Science UniversityPortland, Oregon
SECTION 4: Endocrinology
D. Lynn Loriaux, MD, PhDProfessor of MedicineHead, Division of Endocrinology, Diabetes, and
Clinical NutritionOregon Health & Science UniversityPortland, Oregon
SECTION 5: Gastroenterology and Hepatology
Janice Jou, MD, MHSAssistant Professor of MedicineDivision of Gastroenterology and HepatologyDirector, Gastroenterology and Hepatology
FellowshipOregon Health & Science UniversityPortland, Oregon
SECTION 6: General Internal Medicine
D. Lynn Loriaux, MD, PhDProfessor of MedicineHead, Division of Endocrinology, Diabetes, and
Clinical NutritionOregon Health & Science UniversityPortland, Oregon
David Mansoor, MDAssociate Professor of PsychiatryOregon Health & Science UniversityPortland, Oregon
SECTION 7: Hematology
Thomas DeLoughery, MD, MACP, FAWMProfessor of Medicine, Pathology, and PediatricsDivision of Hematology and OncologyOregon Health & Science UniversityPortland, Oregon
SECTION 8: Infectious Diseases
Thomas Ward, MDProfessor Emeritus of MedicineDivision of Infectious DiseasesOregon Health & Science UniversityPortland, Oregon
SECTION 9: Nephrology
Pavan Chopra, MD, MSAssistant Professor of MedicineDivision of Nephrology and HypertensionDirector, Dialysis ServicesOregon Health & Science UniversityPortland, Oregon
SECTION 10: Neurology
Faheem Sheriff, MDFellow of Neurocritical CareMassachusetts General HospitalBrigham and Women’s HospitalBoston, Massachusetts
SECTION 11: Pulmonology
Alan F. Barker, MDProfessor of MedicineDivision of Pulmonary and Critical CareOregon Health & Science UniversityPortland, Oregon
SECTION 12: Rheumatology
Atul Deodhar, MD, MRCP, FACP, FACRProfessor of MedicineDivision of Arthritis & Rheumatic DiseasesDirector, Rheumatology ClinicsDirector, Immunology Infusion CenterOregon Health & Science UniversityPortland, Oregon

x REVIEWERS
Medical Editor
Margot E. Chase, MPAS, PA-CInstructor of MedicineDivision of Hospital MedicineOregon Health & Science UniversityPortland, Oregon
Additional Faculty Reviewers
Stephanie A.C. Halvorson, MD, FACPAssociate Professor of MedicineDivision of Hospital MedicineOregon Health & Science UniversityPortland, Oregon
Mary Ann Kuzma, MDAssociate Professor of MedicineClerkship Director, Internal MedicineDrexel University College of MedicinePhiladelphia, Pennsylvania
Octavian Calin Lucaciu, MD, PhDAssociate Professor of AnatomyCanadian Memorial Chiropractic CollegeToronto, Ontario, Canada
Gregory J. Magarian, MDProfessor of MedicineDivision of Hospital MedicineOregon Health & Science UniversityPortland, Oregon
Additional Student and Resident ReviewersShelby BadaniCassandra Betts, MDKaren BieraugelChristina B. CherryMichael-Hunter ClementAlexander ConnellySpencer Degerstedt, MDChristine GreippSameer Hirji, MDArthur KehasWhitney KingRebecca Levin-EpsteinAisha MohammedChristine MotzkusJennifer E. MustardAndrew Oehler, MDJayoma PereraNekeyua N. RichardsonBranden TarlowRachna UnnithanCara Varley

xi
ACKNOWLEDGEMENTS
I received an incredible amount of support over the 6 years it took me to complete this book. Above all, I am thankful for my mother Salma. I am grateful to my father Edward, siblings Sherri, Steve, Dave, Aimee, and Lori, as well as Sito (grandmother) Margareet Barhoum for encouraging me from the beginning until the end. It is amazing the impact of such a sim-ple question, “How is the book coming along?” My cousins Jamil Mansoor and Joseph Barhoum, and my friend Josh Hughes were always interested in the progress, no matter how fast or how slow.
When I first came to OHSU in 2005, I was intro-duced to the legend of Lynn Loriaux. So astute a clini-cian, it was said he needed only a handshake to make a diagnosis. Behind every legend there is a man. Often, they are nothing alike. Sometimes, the man is equal to the legend. Only seldom does he exceed it. When I met the man himself, it was clear just how rare he is. His guidance throughout this process cannot be over-stated. And we could not have done it without Julie Walvatne.
I received immeasurable support from Shangar Meman, from the earliest stages of writing until the end (she is a superb agent). The advice of my friend and
colleague Christopher “Kwonsult” Kwock was always as effective as it was sarcastic. He was available any time I needed him. This book benefited from excep-tional proofreading by Jennifer Mustard and Spencer “274” Degerstedt. Joseph Mabe provided valuable expertise in matters that are beyond me. Christopher Neck always took time to answer questions. Summer Steele contributed countless reference articles. I thank my friends and colleagues Gregory Magarian, Peter Sullivan, Sima Desai, Brian Chan, Elly Karamooz, and Margot Chase for their interest and advice over the years.
I am appreciative of the outstanding team at Wolters Kluwer, in particular Matt Hauber, Tom Conville, Andrea Vosburgh, and Lindsay Ries, first for their patience and second for their innovative ideas that enriched every facet of this book. I would also like to recognize Tari Broderick who first received my proposal and believed in this book from day one.
Finally, and most importantly, I would like to thank all of the patients I have ever had the privilege of caring for, with special attention to those presented in this book. I hope the telling of their stories will serve as a benefit to others.

xii
CONTENTS
FOREWORD VI
PREFACE VII
REVIEWERS IX
ACKNOWLEDGEMENTS XI
LIST OF COMPLETED FRAMEWORKS XIV
SECTION 1 How to Use This Book
FOR LEARNERS 1
FOR EDUCATORS 1
Internal Medicine Residents and Faculty 1
Internal Medicine Chief Residents 1
SECTION 2 The Framework System
SECTION 3 Cardiology
Chapter 1 BRADYCARDIA 5
Chapter 2 CHEST PAIN 15
Chapter 3 HEART BLOCK 29
Chapter 4 HEART FAILURE 37
Chapter 5 PERICARDITIS 55
Chapter 6 TACHYCARDIA 67
SECTION 4 Endocrinology
Chapter 7 ADRENAL INSUFFICIENCY 78
Chapter 8 CUSHING’S SYNDROME 91
Chapter 9 HYPERCALCEMIA 100
Chapter 10 HYPOCALCEMIA 112
Chapter 11 HYPOTHYROIDISM 125
Chapter 12 THYROTOXICOSIS 137
SECTION 5 Gastroenterology and Hepatology
Chapter 13 ASCITES 147
Chapter 14 CHOLESTATIC LIVER INJURY 162
Chapter 15 DIARRHEA 176
Chapter 16 GASTROINTESTINAL BLEEDING 198
Chapter 17 HEPATOCELLULAR LIVER INJURY 212
Chapter 18 INTESTINAL ISCHEMIA 223
SECTION 6 General Internal Medicine
Chapter 19 DELIRIUM 235
Chapter 20 DYSPNEA 248
Chapter 21 FEVER OF UNKNOWN ORIGIN 263
Chapter 22 HYPOTENSION 276
Chapter 23 PERIPHERAL EDEMA 288
Chapter 24 SYNCOPE 300
SECTION 7 Hematology
Chapter 25 ANEMIA 310
Chapter 26 HEMOLYTIC ANEMIA 326
Chapter 27 PANCYTOPENIA 342
Chapter 28 PLATELET DISORDERS 353
SECTION 8 Infectious Diseases
Chapter 29 ENDOCARDITIS 365
Chapter 30 MENINGITIS 382
Chapter 31 PNEUMONIA 398

xiiiCONTENTS
SECTION 9 Nephrology
Chapter 32 ACID-BASE DISORDERS 414
Chapter 33 ACUTE KIDNEY INJURY 430
Chapter 34 GLOMERULAR DISEASE 445
Chapter 35 HYPERKALEMIA 460
Chapter 36 HYPERNATREMIA 469
Chapter 37 HYPOKALEMIA 479
Chapter 38 HYPONATREMIA 487
Chapter 39 SECONDARY HYPERTENSION 501
SECTION 10 Neurology
Chapter 40 HEADACHE 510
Chapter 41 POLYNEUROPATHY 525
Chapter 42 SEIZURE 540
Chapter 43 STROKE 557
Chapter 44 WEAKNESS 578
SECTION 11 Pulmonology
Chapter 45 HEMOPTYSIS 603
Chapter 46 HYPOXEMIA 612
Chapter 47 INTERSTITIAL LUNG DISEASE 631
Chapter 48 PLEURAL EFFUSION 645
SECTION 12 Rheumatology
Chapter 49 ARTHRITIS 658
Chapter 50 SYSTEMIC VASCULITIS 673
SECTION 13 Educator’s Appendix
A Brief History of Medical Education and Introduction to the Chalk Talk 684The Seven Tenets of The Chalk Talk 687Chalk Talks and The Framework System 690
INDEX 693

xiv
LIST OF COMPLETED FRAMEWORKS
SECTION 3: CardiologyBRADYCARDIA 12
CHEST PAIN 22
HEART BLOCK 33
HEART FAILURE 51
PERICARDITIS 64
TACHYCARDIA 75
SECTION 4: EndocrinologyADRENAL INSUFFICIENCY 87
CUSHING’S SYNDROME 97
HYPERCALCEMIA 108
HYPOCALCEMIA 122
HYPOTHYROIDISM 133
THYROTOXICOSIS 143
SECTION 5: Gastroenterology and HepatologyASCITES 157
CHOLESTATIC LIVER INJURY 172
DIARRHEA 193
GASTROINTESTINAL BLEEDING 208
HEPATOCELLULAR LIVER INJURY 219
INTESTINAL ISCHEMIA 232
SECTION 6: General Internal MedicineDELIRIUM 244
DYSPNEA 259
FEVER OF UNKNOWN ORIGIN 272
HYPOTENSION 285
PERIPHERAL EDEMA 296
SYNCOPE 306
SECTION 7: HematologyANEMIA 322
HEMOLYTIC ANEMIA 338
PANCYTOPENIA 350
PLATELET DISORDERS 361
SECTION 8: Infectious DiseasesENDOCARDITIS 378
MENINGITIS 394
PNEUMONIA 410
SECTION 9: NephrologyACID/BASE DISORDERS 427
ACUTE KIDNEY INJURY 442
GLOMERULAR DISEASE 456
HYPERKALEMIA 466
HYPERNATREMIA 476
HYPOKALEMIA 484
HYPONATREMIA 497
SECONDARY HYPERTENSION 507
SECTION 10: NeurologyHEADACHE 521
POLYNEUROPATHY 535
SEIZURE 553
STROKE 574
WEAKNESS 598
SECTION 11: PulmonologyHEMOPTYSIS 609
HYPOXEMIA 627
INTERSTITIAL LUNG DISEASE 641
PLEURAL EFFUSION 654
SECTION 12: RheumatologyARTHRITIS 668
SYSTEMIC VASCULITIS 680